
Effect of a NICU to Home Physical Therapy Intervention on White Matter Trajectories, Motor Skills, and Problem-Solving Skills of Infants Born Very Preterm: A Case Series
 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Intervention
2.3. MRI Administration & Protocol
2.4. Descriptive and Outcome Measures
2.5. Statistical Data Analysis
3. Results
3.1. Intervention Compliance
3.2. Case Descriptions: Developmental Assessments
3.2.1. Usual Care Group
3.2.2. SPEEDI2 Intervention Group
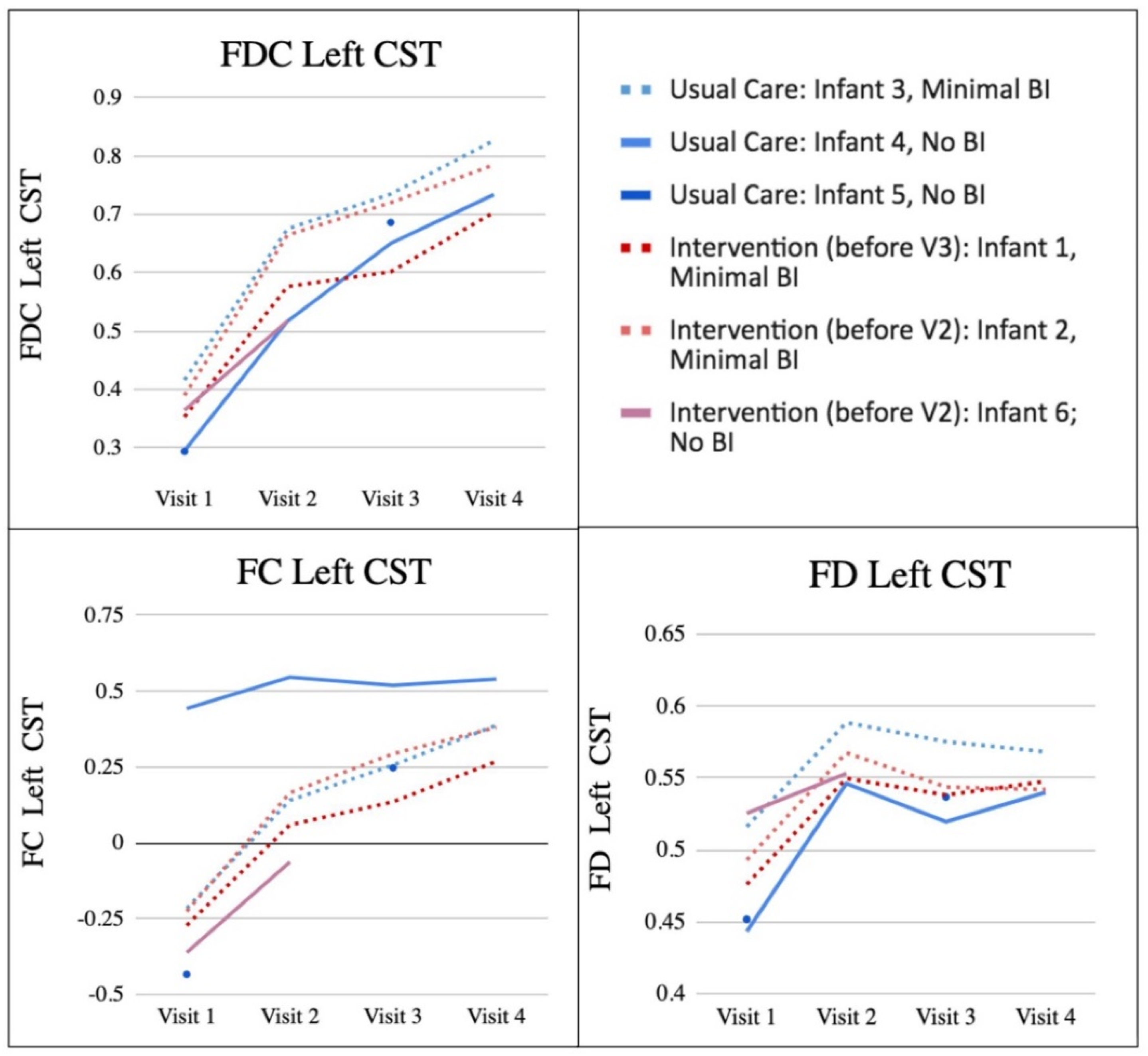
3.3. Case Descriptions: FD, FC, FDC
3.3.1. Usual Care Group
3.3.2. SPEEDI2 Intervention Group
3.4. Group Summary
4. Discussion
5. Limitations and Future Directions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lobo, M.A.; Galloway, J.C. Assessment and Stability of Early Learning Abilities in Preterm and Full-Term Infants across the First Two Years of Life. Res. Dev. Disabil. 2013, 34, 1721–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascal, A.; Govaert, P.; Oostra, A.; Naulaers, G.; Ortibus, E.; Van den Broeck, C. Neurodevelopmental Outcome in Very Preterm and Very-Low-Birthweight Infants Born over the Past Decade: A Meta-Analytic Review. Dev. Med. Child Neurol. 2018, 60, 342–355. [Google Scholar] [CrossRef] [Green Version]
- Brown, L.; Burns, Y.R.; Watter, P.; Gibbons, K.S.; Gray, P.H. Motor Performance, Postural Stability and Behaviour of Non-Disabled Extremely Preterm or Extremely Low Birth Weight Children at Four to Five Years of Age. Early Hum. Dev. 2015, 91, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Goyen, T.-A.; Lui, K. Developmental Coordination Disorder in “Apparently Normal” Schoolchildren Born Extremely Preterm. Arch. Dis. Child. 2009, 94, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Geldof, C.J.A.; van Wassenaer, A.G.; de Kieviet, J.F.; Kok, J.H.; Oosterlaan, J. Visual Perception and Visual-Motor Integration in Very Preterm and/or Very Low Birth Weight Children: A Meta-Analysis. Res. Dev. Disabil. 2012, 33, 726–736. [Google Scholar] [CrossRef]
- Strahle, J.M.; Triplett, R.L.; Alexopoulos, D.; Smyser, T.A.; Rogers, C.E.; Limbrick, D.D.; Smyser, C.D. Impaired Hippocampal Development and Outcomes in Very Preterm Infants with Perinatal Brain Injury. NeuroImag: Clin. 2019, 22, 101787. [Google Scholar] [CrossRef]
- de Vries, L.S.; van Haastert, I.C.; Benders, M.J.N.L.; Groenendaal, F. Myth: Cerebral Palsy Cannot Be Predicted by Neonatal Brain Imaging. Semin. Fetal Neonatal Med. 2011, 16, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Anjari, M.; Srinivasan, L.; Allsop, J.M.; Hajnal, J.V.; Rutherford, M.A.; Edwards, A.D.; Counsell, S.J. Diffusion Tensor Imaging with Tract-Based Spatial Statistics Reveals Local White Matter Abnormalities in Preterm Infants. NeuroImage 2007, 35, 1021–1027. [Google Scholar] [CrossRef]
- Counsell, S.J.; Shen, Y.; Boardman, J.P.; Larkman, D.J.; Kapellou, O.; Ward, P.; Allsop, J.M.; Cowan, F.M.; Hajnal, J.V.; Edwards, A.D.; et al. Axial and Radial Diffusivity in Preterm Infants Who Have Diffuse White Matter Changes on Magnetic Resonance Imaging at Term-Equivalent Age. Pediatrics 2006, 117, 376–386. [Google Scholar] [CrossRef]
- Hüppi, P.S.; Maier, S.E.; Peled, S.; Zientara, G.P.; Barnes, P.D.; Jolesz, F.A.; Volpe, J.J. Microstructural Development of Human Newborn Cerebral White Matter Assessed in Vivo by Diffusion Tensor Magnetic Resonance Imaging. Pediatr. Res. 1998, 44, 584–590. [Google Scholar] [CrossRef]
- Krishnan, M.L.; Dyet, L.E.; Boardman, J.P.; Kapellou, O.; Allsop, J.M.; Cowan, F.; Edwards, A.D.; Rutherford, M.A.; Counsell, S.J. Relationship Between White Matter Apparent Diffusion Coefficients in Preterm Infants at Term-Equivalent Age and Developmental Outcome at 2 Years. Pediatrics 2007, 120, e604–e609. [Google Scholar] [CrossRef]
- Neil, J.J.; Shiran, S.I.; McKinstry, R.C.; Schefft, G.L.; Snyder, A.Z.; Almli, C.R.; Akbudak, E.; Aronovitz, J.A.; Miller, J.P.; Lee, B.C.; et al. Normal Brain in Human Newborns: Apparent Diffusion Coefficient and Diffusion Anisotropy Measured by Using Diffusion Tensor MR Imaging. Radiology 1998, 209, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Pannek, K.; Fripp, J.; George, J.M.; Fiori, S.; Colditz, P.B.; Boyd, R.N.; Rose, S.E. Fixel-Based Analysis Reveals Alterations Is Brain Microstructure and Macrostructure of Preterm-Born Infants at Term Equivalent Age. NeuroImage Clin. 2018, 18, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Rose, S.E.; Hatzigeorgiou, X.; Strudwick, M.W.; Durbridge, G.; Davies, P.S.W.; Colditz, P.B. Altered White Matter Diffusion Anisotropy in Normal and Preterm Infants at Term-Equivalent Age. Magn. Reson. Med. 2008, 60, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.K.; Lee, K.J.; Egan, G.F.; Warfield, S.K.; Doyle, L.W.; Anderson, P.J.; Inder, T.E. Regional White Matter Microstructure in Very Preterm Infants: Predictors and 7 Year Outcomes. Cortex 2014, 52, 60–74. [Google Scholar] [CrossRef] [Green Version]
- Yung, A.; Poon, G.; Qiu, D.-Q.; Chu, J.; Lam, B.; Leung, C.; Goh, W.; Khong, P.-L. White Matter Volume and Anisotropy in Preterm Children: A Pilot Study of Neurocognitive Correlates. Pediatr. Res. 2007, 61, 732–736. [Google Scholar] [CrossRef] [Green Version]
- Balakrishnan, U.; Amboiram, P.; Ninan, B.; Chandrasekharan, A.; Rangaswamy, R.; Subramanian, L. MRI at Term Equivalent Age for Predicting Long-Term Neurodevelopmental Outcome in Preterm Infants-a Cohort Study. J. Matern. -Fetal Neonatal Med. 2020, 33, 1867–1873. [Google Scholar] [CrossRef]
- George, J.M.; Fiori, S.; Fripp, J.; Pannek, K.; Bursle, J.; Moldrich, R.X.; Guzzetta, A.; Coulthard, A.; Ware, R.S.; Rose, S.E.; et al. Validation of an MRI Brain Injury and Growth Scoring System in Very Preterm Infants Scanned at 29- to 35-Week Postmenstrual Age. Am. J. Neuroradiol. 2017, 38, 1435–1442. [Google Scholar] [CrossRef] [Green Version]
- Melbourne, L.; Murnick, J.; Chang, T.; Glass, P.; Massaro, A.N. Regional Brain Biometrics at Term-Equivalent Age and Developmental Outcome in Extremely Low-Birth-Weight Infants. Am. J. Perinatol. 2015, 32, 1177–1184. [Google Scholar] [CrossRef]
- Pannek, K.; George, J.M.; Boyd, R.N.; Colditz, P.B.; Rose, S.E.; Fripp, J. Brain Microstructure and Morphology of Very Preterm-Born Infants at Term Equivalent Age: Associations with Motor and Cognitive Outcomes at 1 and 2 Years. NeuroImage 2020, 221, 117163. [Google Scholar] [CrossRef]
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Eliasson, A.-C.; et al. Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA Pediatr. 2017, 171, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.J.; Morgan, C.; Olsen, J.E.; Novak, I.; Cheong, J.L.Y. Early Diagnosis and Treatment of Cerebral Palsy in Children with a History of Preterm Birth. Clin. Perinatol. 2018, 45, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Dusing, S.C.; Brown, S.E.; Van Drew, C.M.; Thacker, L.R.; Hendricks-Muñoz, K.D. Supporting Play Exploration and Early Development Intervention From NICU to Home: A Feasibility Study. Pediatr. Phys. Ther. 2015, 27, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, F.; Olsen, J.; Dusing, S.C.; Guzzetta, A.; Eeles, A.; Spittle, A. Supporting Play, Exploration, and Early Development Intervention (SPEEDI) for Preterm Infants: A Feasibility Randomised Controlled Trial in an Australian Context. Early Hum. Dev. 2020, 151, 105172. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.-Y.; Chang, W.H.; Chang, H.J.; Yi, S.-H.; Kim, M.-Y.; Kim, E.-H.; Kim, Y.-H. Changes in Diffusion Tensor Tractographic Findings Associated with Constraint-Induced Movement Therapy in Young Children with Cerebral Palsy. Clin. Neurophysiol. 2014, 125, 2397–2403. [Google Scholar] [CrossRef]
- Bleyenheuft, Y.; Dricot, L.; Gilis, N.; Kuo, H.-C.; Grandin, C.; Bleyenheuft, C.; Gordon, A.M.; Friel, K.M. Capturing Neuroplastic Changes after Bimanual Intensive Rehabilitation in Children with Unilateral Spastic Cerebral Palsy: A Combined DTI, TMS and FMRI Pilot Study. Res. Dev. Disabil. 2015, 43–44, 136–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullman, H.; Spencer-Smith, M.; Thompson, D.K.; Doyle, L.W.; Inder, T.E.; Anderson, P.J.; Klingberg, T. Neonatal MRI Is Associated with Future Cognition and Academic Achievement in Preterm Children. Brain 2015, 138, 3251–3262. [Google Scholar] [CrossRef]
- Aeby, A.; De Tiège, X.; Creuzil, M.; David, P.; Balériaux, D.; Van Overmeire, B.; Metens, T.; Van Bogaert, P. Language Development at 2years Is Correlated to Brain Microstructure in the Left Superior Temporal Gyrus at Term Equivalent Age: A Diffusion Tensor Imaging Study. NeuroImage 2013, 78, 145–151. [Google Scholar] [CrossRef]
- Barnett, M.L.; Tusor, N.; Ball, G.; Chew, A.; Falconer, S.; Aljabar, P.; Kimpton, J.A.; Kennea, N.; Rutherford, M.; David Edwards, A.; et al. Exploring the Multiple-Hit Hypothesis of Preterm White Matter Damage Using Diffusion MRI. NeuroImage Clin. 2018, 17, 596–606. [Google Scholar] [CrossRef] [Green Version]
- de Bruïne, F.T.; van den Berg-Huysmans, A.A.; Leijser, L.M.; Rijken, M.; Steggerda, S.J.; van der Grond, J.; van Wezel-Meijler, G. Clinical Implications of MR Imaging Findings in the White Matter in Very Preterm Infants: A 2-Year Follow-up Study. Radiology 2011, 261, 899–906. [Google Scholar] [CrossRef]
- Duerden, E.G.; Foong, J.; Chau, V.; Branson, H.; Poskitt, K.J.; Grunau, R.E.; Synnes, A.; Zwicker, J.G.; Miller, S.P. Tract-Based Spatial Statistics in Preterm-Born Neonates Predicts Cognitive and Motor Outcomes at 18 Months. Am. J. Neuroradiol. 2015, 36, 1565–1571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khurana, S.; Evans, M.E.; Kelly, C.E.; Thompson, D.K.; Burnsed, J.C.; Harper, A.D.; Hendricks-Muñoz, K.D.; Shall, M.S.; Stevenson, R.D.; Inamdar, K.; et al. Longitudinal Changes in the Sensorimotor Pathways of Very Preterm Infants During the First Year of Life With and Without Intervention: A Pilot Study. Dev. Neurorehabilit. 2021, 24, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Peyton, C.; Yang, E.; Msall, M.E.; Adde, L.; Støen, R.; Fjørtoft, T.; Bos, A.F.; Einspieler, C.; Zhou, Y.; Schreiber, M.D.; et al. White Matter Injury and General Movements in High-Risk Preterm Infants. Am. J. Neuroradiol. 2017, 38, 162–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Kooij, B.J.M.; de Vries, L.S.; Ball, G.; van Haastert, I.C.; Benders, M.J.N.L.; Groenendaal, F.; Counsell, S.J. Neonatal Tract-Based Spatial Statistics Findings and Outcome in Preterm Infants. Am. J. Neuroradiol. 2012, 33, 188–194. [Google Scholar] [CrossRef] [Green Version]
- Woodward, L.J.; Clark, C.A.C.; Bora, S.; Inder, T.E. Neonatal White Matter Abnormalities an Important Predictor of Neurocognitive Outcome for Very Preterm Children. PLoS ONE 2012, 7, e51879. [Google Scholar] [CrossRef] [Green Version]
- Raffelt, D.A.; Tournier, J.-D.; Smith, R.E.; Vaughan, D.N.; Jackson, G.; Ridgway, G.R.; Connelly, A. Investigating White Matter Fibre Density and Morphology Using Fixel-Based Analysis. NeuroImage 2017, 144, 58–73. [Google Scholar] [CrossRef] [Green Version]
- Dhollander, T.; Clemente, A.; Singh, M.; Boonstra, F.; Civier, O.; Duque, J.D.; Egorova, N.; Enticott, P.; Fuelscher, I.; Gajamange, S.; et al. Fixel-Based Analysis of Diffusion MRI: Methods, Applications, Challenges and Opportunities. NeuroImage 2021, 241, 118417. [Google Scholar] [CrossRef]
- Tournier, J.-D.; Calamante, F.; Connelly, A. Robust Determination of the Fibre Orientation Distribution in Diffusion MRI: Non-Negativity Constrained Super-Resolved Spherical Deconvolution. NeuroImage 2007, 35, 1459–1472. [Google Scholar] [CrossRef]
- Jeurissen, B.; Tournier, J.-D.; Dhollander, T.; Connelly, A.; Sijbers, J. Multi-Tissue Constrained Spherical Deconvolution for Improved Analysis of Multi-Shell Diffusion MRI Data. NeuroImage 2014, 103, 411–426. [Google Scholar] [CrossRef]
- Dhollander, T.; Connelly, A. A Novel Iterative Approach to Reap the Benefits of Multi-Tissue CSD from Just Single-Shell (+b = 0) Diffusion MRI Data. Proc. Intl. Soc. Mag. Reson. Med. 2016, 24, 3010. [Google Scholar]
- Chandwani, R.; Kline, J.E.; Harpster, K.; Tkach, J.; Parikh, N.A.; Cincinnati Infant Neurodevelopment Early Prediction Study (CINEPS) Group. Early Micro- and Macrostructure of Sensorimotor Tracts and Development of Cerebral Palsy in High Risk Infants. Hum. Brain Mapp. 2021, 42, 4708–4721. [Google Scholar] [CrossRef]
- Dusing, S.C.; Burnsed, J.C.; Brown, S.E.; Harper, A.D.; Hendricks-Munoz, K.D.; Stevenson, R.D.; Thacker, L.R., II.; Molinini, R.M. Efficacy of Supporting Play Exploration and Early Development Intervention in the First Months of Life for Infants Born Very Preterm: 3-Arm Randomized Clinical Trial Protocol. Phys. Ther. 2020, 100, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Einspieler, C.; Marschik, P.B.; Bos, A.F.; Ferrari, F.; Cioni, G.; Prechtl, H.F. Early Markers for Cerebral Palsy: Insights from the Assessment of General Movements. Future Neurol. 2012, 7, 709–717. [Google Scholar] [CrossRef] [Green Version]
- Prechtl, H.F.; Einspieler, C.; Cioni, G.; Bos, A.F.; Ferrari, F.; Sontheimer, D. An Early Marker for Neurological Deficits after Perinatal Brain Lesions. Lancet 1997, 349, 1361–1363. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S. Test of Infant Motor Performance: Test User’s Manual, 3rd ed.; Infant Motor Performance Scales, LLC: Chicago, IL, USA, 2012. [Google Scholar]
- Common Data Elements Cerebral Palsy. Available online: https://www.commondataelements.ninds.nih.gov/cerebral%20palsy (accessed on 21 March 2022).
- Spittle, A.J.; Doyle, L.W.; Boyd, R.N. A Systematic Review of the Clinimetric Properties of Neuromotor Assessments for Preterm Infants during the First Year of Life. Dev. Med. Child Neurol. 2008, 50, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Bayley, N. Bayley Scales of Infant and Toddler Development Measurement Instrument, 3rd ed.; PsychCorp: San Antonio, TX, USA, 2006. [Google Scholar]
- Schiariti, V.; Fowler, E.; Brandenburg, J.E.; Levey, E.; Mcintyre, S.; Sukal-Moulton, T.; Ramey, S.L.; Rose, J.; Sienko, S.; Stashinko, E.; et al. A Common Data Language for Clinical Research Studies: The National Institute of Neurological Disorders and Stroke and American Academy for Cerebral Palsy and Developmental Medicine Cerebral Palsy Common Data Elements Version 1.0 Recommendations. Dev. Med. Child Neurol. 2018, 60, 976–986. [Google Scholar] [CrossRef] [Green Version]
- Veraart, J.; Novikov, D.S.; Christiaens, D.; Ades-aron, B.; Sijbers, J.; Fieremans, E. Denoising of Diffusion MRI Using Random Matrix Theory. NeuroImage 2016, 142, 394–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellner, E.; Dhital, B.; Kiselev, V.G.; Reisert, M. Gibbs-Ringing Artifact Removal Based on Local Subvoxel-Shifts. Magn. Reson. Med. 2016, 76, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, J.L.R.; Sotiropoulos, S.N. An Integrated Approach to Correction for Off-Resonance Effects and Subject Movement in Diffusion MR Imaging. NeuroImage 2016, 125, 1063–1078. [Google Scholar] [CrossRef] [Green Version]
- Dhollander, T.; Mito, R.; Raffelt, D.; Connelly, A. Improved White Matter Response Function Estimation for 3-Tissue Constrained Spherical Deconvolution. Proc. Intl. Soc. Mag. Reson. Med. 2019, 555, 10. [Google Scholar]
- Smith, S.M. Fast Robust Automated Brain Extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Dhollander, T.; Tabbara, R.; Rosnarho-Tornstrand, J.; Tournier, J.-D.; Raffelt, D.; Connelly, A. Multi-Tissue Log-Domain Intensity and Inhomogeneity Normalisation for Quantitative Apparent Fibre Density. Proc. ISMRM 2021, 29, 2472. [Google Scholar]
- Raffelt, D.; Tournier, J.-D.; Fripp, J.; Crozier, S.; Connelly, A.; Salvado, O. Symmetric Diffeomorphic Registration of Fibre Orientation Distributions. NeuroImage 2011, 56, 1171–1180. [Google Scholar] [CrossRef] [PubMed]
- Wasserthal, J.; Neher, P.; Maier-Hein, K.H. TractSeg-Fast and Accurate White Matter Tract Segmentation. NeuroImage 2018, 183, 239–253. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Gao, F.; Zheng, W.; You, Y.; Zhao, Z.; Lv, Y.; Chen, W.; Zhang, H.; Ji, C.; Wu, D. Diffusion MRI of the Infant Brain Reveals Unique Asymmetry Patterns during the First-Half-Year of Development. NeuroImage 2021, 242, 118465. [Google Scholar] [CrossRef] [PubMed]
- Dusing, S.C.; Tripathi, T.; Marcinowski, E.C.; Thacker, L.R.; Brown, L.F.; Hendricks-Muñoz, K.D. Supporting Play Exploration and Early Developmental Intervention versus Usual Care to Enhance Development Outcomes during the Transition from the Neonatal Intensive Care Unit to Home: A Pilot Randomized Controlled Trial. BMC Pediatr. 2018, 18, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khurana, S.; Kane, A.E.; Brown, S.E.; Tarver, T.; Dusing, S.C. Effect of Neonatal Therapy on the Motor, Cognitive, and Behavioral Development of Infants Born Preterm: A Systematic Review. Dev. Med. Child Neurol. 2020, 62, 684–692. [Google Scholar] [CrossRef]
- Øberg, G.K.; Handegård, B.H.; Campbell, S.K.; Ustad, T.; Fjørtoft, T.; Kaaresen, P.I.; Girolami, G.L. Two-Year Motor Outcomes Associated with the Dose of NICU Based Physical Therapy: The Noppi RCT. Early Hum. Dev. 2022, 174, 105680. [Google Scholar] [CrossRef]
- Barfield, W.D.; Clements, K.M.; Lee, K.G.; Kotelchuck, M.; Wilber, N.; Wise, P.H. Using Linked Data to Assess Patterns of Early Intervention (EI) Referral among Very Low Birth Weight Infants. Matern. Child Health J. 2008, 12, 24–33. [Google Scholar] [CrossRef]
- Rosenberg, S.A.; Zhang, D.; Robinson, C.C. Prevalence of Developmental Delays and Participation in Early Intervention Services for Young Children. Pediatrics 2008, 121, e1503–e1509. [Google Scholar] [CrossRef]
- Feinberg, E.; Silverstein, M.; Donahue, S.; Bliss, R. The Impact of Race on Participation in Part C Early Intervention Services. J. Dev. Behav. Pediatr. 2011, 32, 284–291. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Group | Brain Injury | PVH-IVH | Sepsis | Baseline GMA | TIMP Z-Score | Gestational Age | Birth Weight | Gender | Race; Ethnicity | Annual Income |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Infant 1 | SPEEDI | Minimal | No | No | Normal | −0.88 | 23 weeks | 580 gm | M | Black; Non-Hispanic | USD 15K–USD 25K |
| Infant 2 | SPEEDI | Minimal | No | No | Normal | −1.36 | 27 weeks | 840 gm | F | White; Non-Hispanic | ≥USD 100K |
| Infant 3 | Usual Care | Minimal | No | Yes | Normal | −0.08 | 27 weeks | 1030 gm | M | White; Non-Hispanic | ≥USD 100K |
| Infant 4 | Usual Care | Normal | No | No | Normal | 0.15 | 27 weeks | 970 gm | F | Black; Non-Hispanic | USD 35K–USD 49K |
| Infant 5 | Usual Care | Normal | No | No | Normal | 0.8 | 27 weeks | 1000 gm | F | Not Reported | Not Reported |
| Infant 6 | SPEEDI | Normal | Grade I or II | No | Abnormal | −1.07 | 27 weeks | 1038 gm | F | Not Reported | Not Reported |
| Variable | Age * | TIMP Z-Score | GMA | Bayley-III MC | Bayley-III MC | Bayley-III MC | Bayley-III CC | Bayley-III CC | Bayley-III CC |
|---|---|---|---|---|---|---|---|---|---|
| Visit 1; Visit 2; Visit 3; Visit 4 | Visit 2 | Visit 2 | Visit 2 | Visit 3 | Visit 4 | Visit 2 | Visit 3 | Visit 4 | |
| Infant 1 | 4m 7d; 7m 14d; 10m 6d;17m 25d | −0.59 | Normal | 121 | 94 | 79 | 110 | 85 | 80 |
| Infant 2 | 2m 17d; 6m 1d; 10m 2d; 16m 11d | −0.77 | Normal | 103 | 82 | 88 | 105 | 100 | 90 |
| Infant 3 | 2m 9d; 5m 26d; 8m 26d; 16m 14d | −0.73 | Normal | 85 | 97 | 91 | 95 | 105 | 115 |
| Infant 4 | 2m 4d; 5m 14d; 13m 12d; 15m 22d | 0.38 | Normal | 121 | 76 | 76 | 95 | 70 | 85 |
| Infant 5 | 1m 26d; 5m 22d; 9m 5d; 20m 23d | −0.36 | Normal | 107 | 103 | 94 | 90 | 105 | 85 |
| Infant 6 | 3m; 6m 23d | −1.38 | Normal | 103 | N/A | N/A | 105 | N/A | N/A |
| Participant | Variable | Bayley-III CR | Bayley-III CC | Bayley-III GMR | Bayley-III MC | APSP Global Score | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | r | p | ||
| Infant 1 (Intervention, minimal injury) | FD Left CST | −0.047 | 0.97 | 0.512 | 0.658 | 0.163 | 0.896 | 0.327 | 0.788 | 0.149 | 0.904 |
| FC Left CST | 0.999 * | 0.021 | −0.866 | 0.333 | 0.984 | 0.113 | −0.949 | 0.203 | 0.987 | 0.104 | |
| FDC Left CST | 0.978 | 0.135 | −0.763 | 0.447 | 1.00 ** | <0.001 | −0.878 | 0.317 | 1.00 ** | 0.01 | |
| Infant 2 (Intervention, minimal injury) | FD Left CST | −0.917 | 0.261 | 0.795 | 0.415 | −0.737 | 0.473 | 0.942 | 0.218 | −0.921 | 0.254 |
| FC Left CST | 0.99 * | 0.037 | −0.955 | 0.191 | 0.924 | 0.249 | −0.768 | 0.442 | 0.999 * | 0.030 | |
| FDC Left CST | 0.995 | 0.063 | −0.99 | 0.091 | 0.973 | 0.149 | −0.659 | 0.542 | 0.994 | 0.07 | |
| Infant 3 (Usual Care, minimal injury) | FD Left CST | −0.983 | 0.118 | −0.986 | 0.108 | −0.922 | 0.252 | −0.639 | 0.559 | −0.958 | 0.184 |
| FC Left CST | 1.00 * | 0.012 | 0.999 * | 0.02 * | 0.981 | 0.123 | 0.47 | 0.688 | 0.996 | 0.055 | |
| FDC Left CST | 0.994 | 0.067 | 0.993 | 0.077 | 0.994 | 0.067 | 0.392 | 0.744 | 1.00 ** | <0.001 | |
| Infant 4 (Usual Care, no injury) | FD Left CST | −0.388 | 0.747 | 0.982 | 0.12 | −0.584 | 0.603 | 0.678 | 0.526 | −0.582 | 0.685 |
| FC Left CST | 0.989 | 0.093 | −0.688 | 0.534 | 0.997 | 0.051 | −0.98 | 0.128 | 0.997 * | 0.049 | |
| FDC Left CST | 0.999 * | 0.02* | −0.515 | 0.656 | 0.964 | 0.172 | −0.924 | 0.249 | 0.964 | 0.17 | |
| Infant 5 (Usual Care, no injury) | FD Left CST | ||||||||||
| FC Left CST | |||||||||||
| FDC Left CST | |||||||||||
| Infant 6 (Intervention, no injury) | FD Left CST | ||||||||||
| FC Left CST | |||||||||||
| FDC Left CST | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butera, C.D.; Rhee, C.; Kelly, C.E.; Dhollander, T.; Thompson, D.K.; Wisnowski, J.; Molinini, R.M.; Sargent, B.; Lepore, N.; Vorona, G.; et al. Effect of a NICU to Home Physical Therapy Intervention on White Matter Trajectories, Motor Skills, and Problem-Solving Skills of Infants Born Very Preterm: A Case Series. J. Pers. Med. 2022, 12, 2024. https://doi.org/10.3390/jpm12122024
Butera CD, Rhee C, Kelly CE, Dhollander T, Thompson DK, Wisnowski J, Molinini RM, Sargent B, Lepore N, Vorona G, et al. Effect of a NICU to Home Physical Therapy Intervention on White Matter Trajectories, Motor Skills, and Problem-Solving Skills of Infants Born Very Preterm: A Case Series. Journal of Personalized Medicine. 2022; 12(12):2024. https://doi.org/10.3390/jpm12122024
Chicago/Turabian StyleButera, Christiana Dodd, Claire Rhee, Claire E. Kelly, Thijs Dhollander, Deanne K. Thompson, Jessica Wisnowski, Rebecca M. Molinini, Barbara Sargent, Natasha Lepore, Greg Vorona, and et al. 2022. "Effect of a NICU to Home Physical Therapy Intervention on White Matter Trajectories, Motor Skills, and Problem-Solving Skills of Infants Born Very Preterm: A Case Series" Journal of Personalized Medicine 12, no. 12: 2024. https://doi.org/10.3390/jpm12122024