
Functional Profile of Older Adults Hospitalized in Rehabilitation Units of the National Network of Integrated Continuous Care of Portugal: A Longitudinal Study
 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Type and Sample
2.2. Instruments
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethical Procedures
3. Results
3.1. Socio-Demographic and Clinical Characteristics
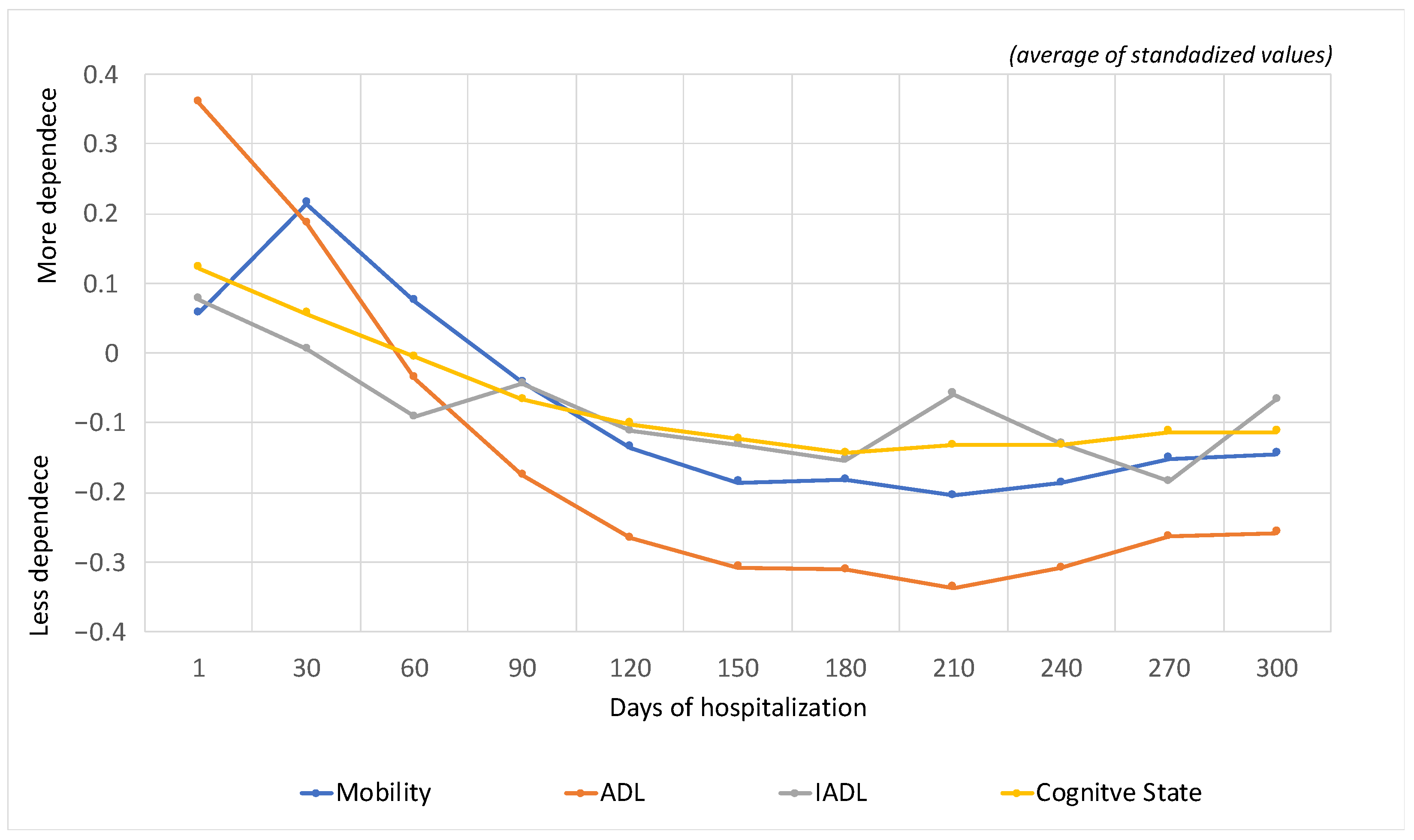
3.2. Evolution of the Functional during Hospitalization
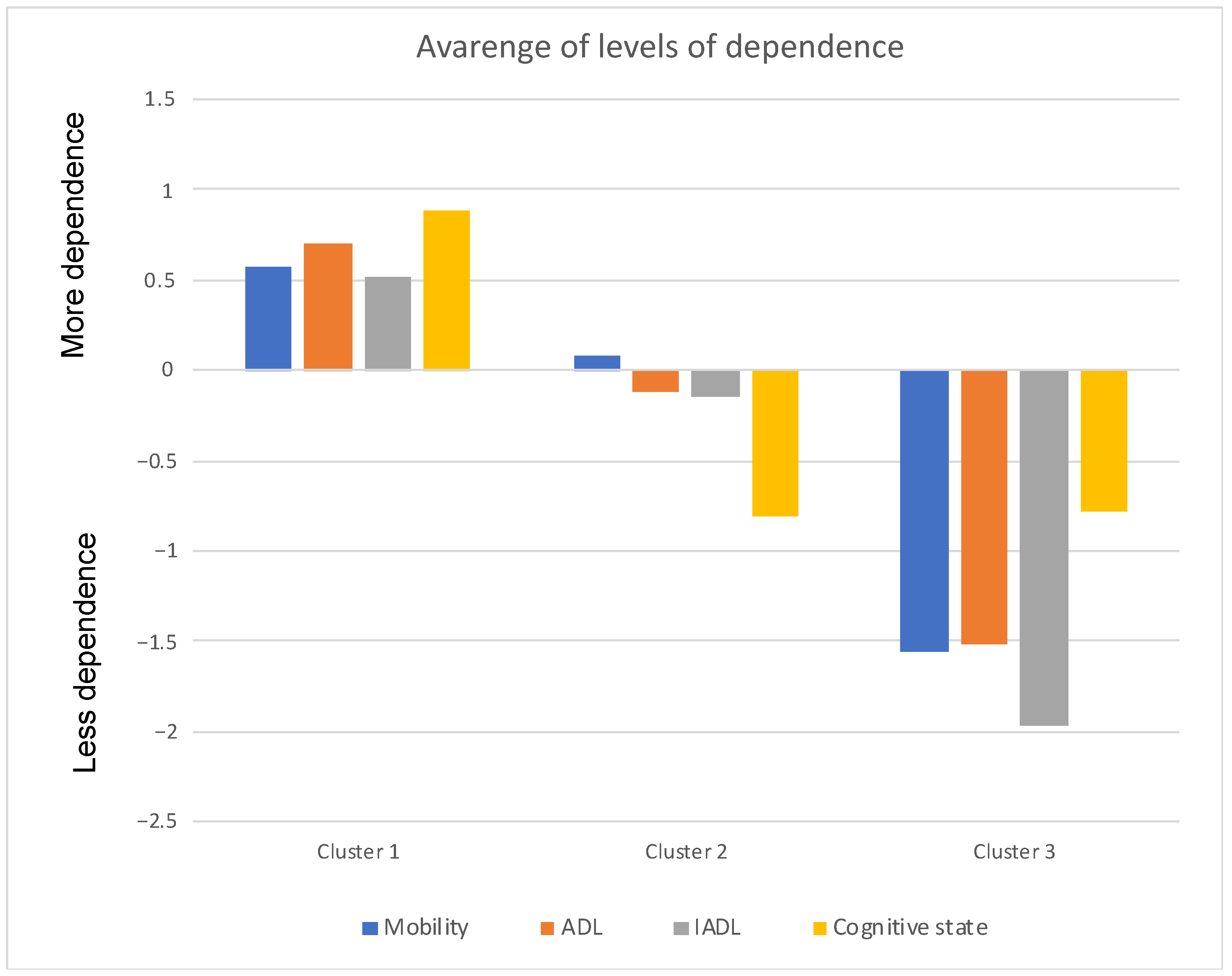
3.3. Dependence Clusters
- (a)
- Cluster 1: Older adults with a higher degree of dependence (severe/complete self-care deficit);
- (b)
- Cluster 2: Older adults with an intermediate degree of dependence (moderate self-care deficit);
- (c)
- Cluster 3: Older adults with a lower degree of dependence (mild self-care deficit);
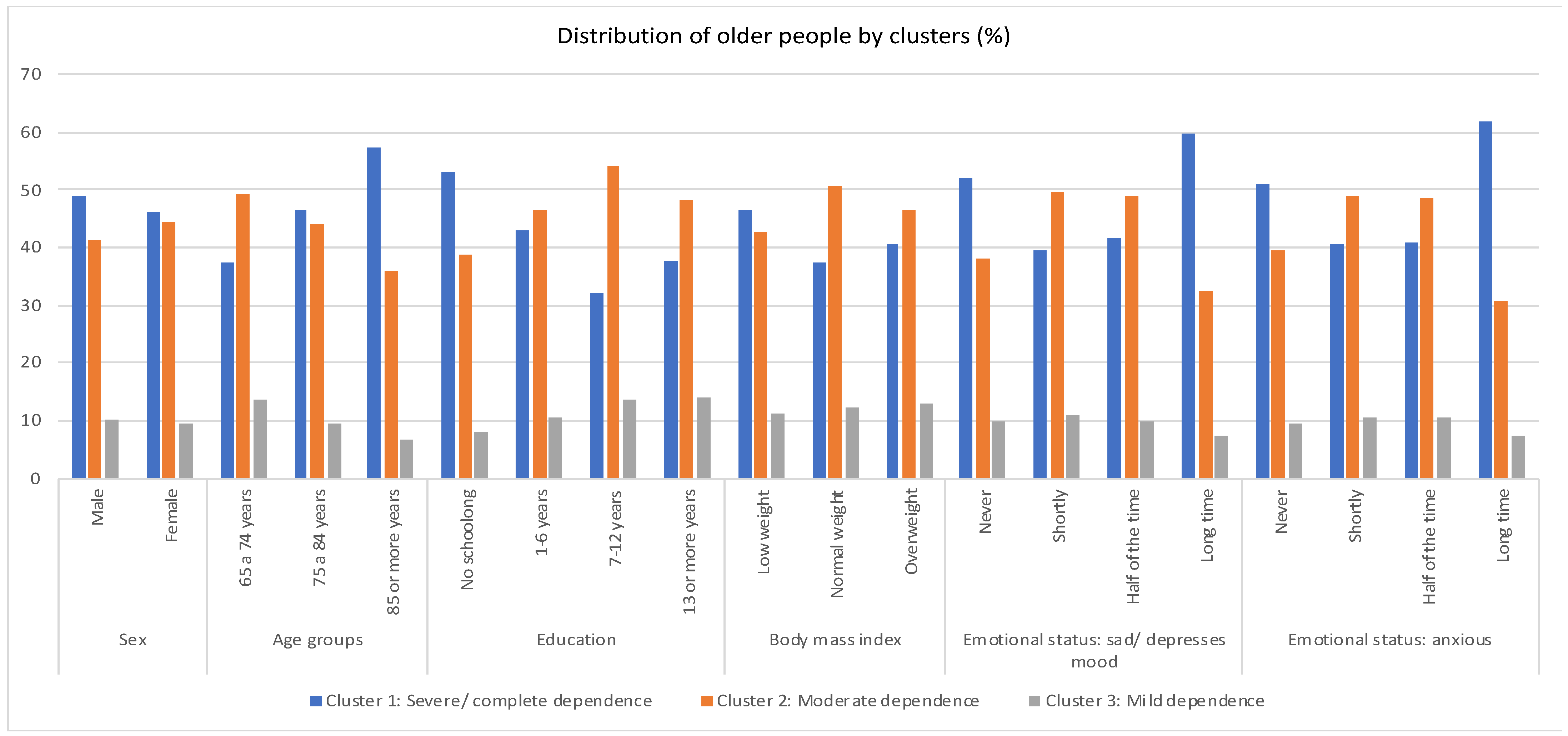
- Cluster 1 (severe dependence): a determinant of the need for totally compensatory nursing care is formed by a higher percentage of males aged 85 years or older. It is made up of people who have not attended school, are low-weight and feel depressed and anxious for a long time.
- Cluster 2 (moderate dependence): where partially compensatory nursing care is required includes females aged between 65 and 84 years old, with schooling from 7 to 12 years old, normal body mass index and feeling of sadness or anxiety little or half of the time.
- Cluster 3 (Mild dependence): who require nursing care at the psychoeducational level, predominantly male, aged 65 to 74, with 13 or more years of schooling. They are overweight, feel depressed a little of the time and feel anxious half of the time.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. World Population Ageing 2019: Highlights; Department of Economic and Social Affairs Population Division: New York, NY, USA, 2019; Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 1 November 2022).
- Abdi, S.; Spann, A.; Borilovic, J.; De Witte, L.; Hawley, M. Understanding the care and support needs of older people: A scoping review and categorisation using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr. 2019, 19, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos, A.; Fonseca, C.; Henriques, A. Needs of fundamental care in elderly with dependence on self-care in context of long-term care: A scoping review. Int. J. Curr. Res. 2017, 9, 53970–53976. [Google Scholar]
- Dias, K.M.; Herdman, T.H.; Ferretti-Rebustini, R.; Lopes, C.T.; Santos, E. Relationships between nursing diagnoses and the level of dependence in activities of daily living of elderly residents. Einstein (Sao Paulo Braz.) 2020, 18, eAO5445. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Self Care for Health: A Handbook for Community Health Workers & Volunteers; WHO: Geneva, Switzerland, 2013.
- Ramos, A.; Fonseca, C.; Pinho, L.; Lopes, M.; Brites, R.; Henriques, A. Assessment of Functioning in Older Adults Hospitalized in Long-Term Care in Portugal: Analysis of a Big Data. Front. Med. 2022, 9, 780364. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.X.M.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 3–25. [Google Scholar] [CrossRef] [Green Version]
- Kitzman, W.D.; Whellan, J.D.; Duncan, P.; Pastva, M.A.; Mentz, J.R.; Reeves, R.G.; Nelson, B.M.; Chen, H.; Upadhya, B.; Reed, D.S.; et al. Physical Rehabilitation for Older Patients Hospitalized for Heart Failure. N. Engl. J. Med. 2021, 385, 203–216. [Google Scholar] [CrossRef]
- Goolkate, T. Self-Management in Older Adults Who Are Temporarily Admitted to a Nursing Home for Rehabilitation after a Lower Limb Fracture and How This Can Be Supported by Technology. Master’s Thesis, University of Twente, Enschede, The Netherlands, 2018. [Google Scholar]
- Pereira, C.; Fonseca, C.; Pinho, L. A Rede Nacional de Cuidados Continuados Integrados em Portugal. In Os Cuidados de Saúde Face Aos Desafios do Nosso Tempo: Contributos para a Gestão da Mudança; Lopes, M., Sakellarides, C., Eds.; Universidade de Évora: Évora, Portugal, 2021; pp. 36–47. [Google Scholar]
- Katz, S.; Ford, S.; Moskowitz, R.; Jackson, B.; Jaffe, M. Studies of Illness in the Aged: The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Lawton, M.; Brody, E. Assessment of Older People: Self-maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Folstein, M.; Folstein, S.; Mchugh, P. “Mini-mental state”: A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Botelho, M. Autonomia Funcional em Idosos: Caracterização Multidimensional em Idosos Utentes de um Centro de Saúde Urbano (Tese de Doutoramento). 1999. Available online: https://run.unl.pt/bitstream/10362/15165/1/Botelho%20Maria%20Amalia%20TD%201999.PDF (accessed on 10 October 2020).
- Brites, R. Análise de Dados com IBM SPSS®: Mix Essencial para Relatórios Profissionais e Teses Académicas, Módulo I—Básico; ISEG, Ed.; ISEG: Lisboa, Portugal, 2015. [Google Scholar]
- Murteira, B.J.F. Probabilidades e Estatística; McGraw-Hill: New York, NY, USA, 1990; Volume I. [Google Scholar]
- Marôco, J. Análise Estatística com o SPSS Statistics v18–v27, 8th ed.; Pêro Pinheiro: Lisboa, Portugal, 2021. [Google Scholar]
- Zhu, Y.; Zhong, Q.; Ji, J.; Ma, J.; Wu, H.; Gao, Y.; Ali, N.; Wang, T. Effects of Aerobic Dance on Cognition in Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2020, 74, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Biazus-Sehn, L.F.; Schuch, F.B.; Firth, J.; Stigger, F.S. Effects of physical exercise on cognitive function of older adults with mild cognitive impairment: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2020, 89, 104048. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.; Fonseca, C.; Pinho, L.; Lopes, M.; Oliveira, H.; Henriques, A. Functional profile of older adults hospitalized in convalescence units of the national network of integrated continuous care of portugal: A longitudinal study. J. Pers. Med. 2021, 11, 1350. [Google Scholar] [CrossRef] [PubMed]
- Kosse, N.M.; Dutmer, A.L.; Dasenbrock, L.; Bauer, J.M.; Lamoth, C.J.C. Effectiveness and feasibility of early physical rehabilitation programs for geriatric hospitalized patients: A systematic review. BMC Geriatr. 2013, 13, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pils, K. Aspects of physical medicine and rehabilitation in geriatrics. Wien. Med. Wochenschr. 2016, 166, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Makino, K.; Lee, S.; Bae, S.; Shinkai, Y.; Chiba, I.; Shimada, H. Relationship between instrumental activities of daily living performance and incidence of mild cognitive impairment among older adults: A 48-month follow-up study. Arch. Gerontol. Geriatr. 2020, 88, 104034. [Google Scholar] [CrossRef]
- Read, S.; Comas-Herrera, A.; Grundy, E. Social Isolation and Memory Decline in Later-life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2020, 75, 367–376. [Google Scholar] [CrossRef] [Green Version]
- Koepsell, T.D.; Monsell, S.E. Reversion from mild cognitive impairment to normal or near-normal cognition: Risk factors and prognosis. Neurology 2012, 79, 1591–1598. [Google Scholar] [CrossRef] [Green Version]
- Fonseca, C.; De Pinho, L.G.; Lopes, M.J.; Marques, C.; Garcia-Alonso, J. The Elderly Nursing Core Set and the cognition of Portuguese older adults: A cross-sectional study. BMC Nurs. 2021, 20, 108. [Google Scholar] [CrossRef]
- Safak, E.D.; Kizilcay, H.D.; Arguvanli, S.; Mazicioglu, M.M.; Mucuk, S.; Ozturk, A.; Akin, S. The Relationship between Daily Living Activities and Cognitive Function in the Elderly: Cross-Sectional Study. Konuralp Med. J. 2019, 11, 30–35. [Google Scholar]
- Campos, A.C.V.; Ferreira, E.F.E.; Vargas, A.M.D. Determinantes do envelhecimento ativo segundo a qualidade de vida e gênero. Cien Saude Colet. 2015, 20, 2221–2237. [Google Scholar] [CrossRef] [Green Version]
- Gyasi, R.M.; Phillips, D.R. Gender, self-rated health and functional decline among community-dwelling older adults. Arch. Gerontol. Geriatr. 2018, 77, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Lopes, M.; De Pinho, L.G.; Fonseca, C.; Goes, M.; Oliveira, H.; Garcia-Alonso, J.; Afonso, A. Functioning and Cognition of Portuguese Older Adults Attending in Residential Homes and Day Centers: A Comparative Study. Int. J. Environ. Res. Public Health 2021, 18, 7030. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.; Topping, M.; Zheng, F.; Lu, Q. The effects of education on cognition in older age: Evidence from genotyped Siblings. Soc. Sci. Med. 2021, 280, 114044. [Google Scholar] [CrossRef] [PubMed]
- Sobral, R.; Sobral, M. Computer Education and Third Age Universities: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7390. [Google Scholar] [CrossRef]
- Coutinho, A.T.D.Q.; Vilela, M.B.R.; Lima, M.L.L.T.D.; Silva, V.D.L. Social communication and functional independence of the elderly in a community assisted by the family health strategy. Rev. CEFAC 2018, 20, 363–373. [Google Scholar] [CrossRef]
- Assis, A.; de Oliveira, B.; Gomes, A.L.; Soares, A.; Guimarães, N.S.; Gomes, J. The association between nutritional status, advanced activities of daily living, and cognitive function among Brazilian older adults living in care homes. Geriatr. Nurs. 2020, 41, 899–904. [Google Scholar] [CrossRef]
- Zoghbi, M.E.; Boulos, C.; Amal, A.H.; Saleh, N.; Awada, S.; Rachidi, S.; Bawab, W.; Salameh, P. Association between cognitive function and nutritional status in elderly: A cross-sectional study in three institutions of Beirut—Lebanon. Geriatr. Ment. Health Care 2013, 1, 73–81. [Google Scholar] [CrossRef]
- Luo, M.S.; Wing, E.; Chui, T.; Li, L.W. The Longitudinal Associations between Physical Health and Mental Health among Older Adults The Longitudinal Associations between Physical Health and Mental Health. Aging Ment. Health 2019, 24, 1990–1998. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Socio-Demographic Variables | n (%) |
|---|---|
| Age (years) 65–74 75–84 ≥85 | 14,498 (24.6) 28,414 (48.1) 16,101 (27.3) |
| Sex Female Male | 34,215 (58.0) 24,798 (42.0) |
| Marital status Married Widowed Single Divorced Union of Fact Unknown | 24,665 (46.6) 19,510 (36.9) 6332 (12.0) 2166 (4.1) 167 (0.3) 90 (0.2) |
| Education (years) No education 1 to 6 7 to 12 ≥13 | 10,933 (34.1) 18,564 (57.8) 1346 (4.2) 1248 (3.9) |
| Professional level Unqualified Qualified Intermediate Specialist | 22,568 (70.3) 7498 (23.4) 1443 (4.5) 571 (1.8) |
| Region of Portugal Alentejo Algarve Centro Lisboa e Vale do Tejo Norte | 4668 (8.3) 2761 (4.9) 15,233 (27.2) 18,663 (31.6) 14,778 (26.3) |
| Levels of Dependence (%) | ||||
|---|---|---|---|---|
| Cluster 1 Severe Dependence | Cluster 2 Moderate Dependence | Cluster 3 Mild Dependence | ||
| Sex | Male | 41.4 | 38.1 | 40.9 |
| Female | 58.6 | 61.9 | 59.1 | |
| TOTAL | 100.0 | 100.0 | 100.0 | |
| Age groups | 65–74 years | 19.4 | 27.9 | 33.8 |
| 75–84 years | 48.4 | 50.0 | 48.1 | |
| 85 or more years | 32.3 | 22.1 | 18.1 | |
| TOTAL | 100.0 | 100.0 | 100.0 | |
| Educational level | No schooling | 43.5 | 33.6 | 31.8 |
| 1–6 years | 51.6 | 58.7 | 59.0 | |
| 7–12 years | 2.3 | 4.0 | 4.5 | |
| 13 or more years | 2.7 | 3.6 | 4.7 | |
| TOTAL | 100.0 | 100.0 | 100.0 | |
| Body mass index | Low weight | 41.7 | 34.7 | 34.7 |
| Normal weight | 26.8 | 32.8 | 30.1 | |
| Overweight | 31.5 | 32.6 | 35.2 | |
| TOTAL | 100.0 | 100.0 | 100.0 | |
| Emotional state: sad/depressed | Never | 43.9 | 35.2 | 39.4 |
| Shortly | 28.3 | 38.8 | 36.8 | |
| Half of the time | 13.8 | 17.7 | 15.4 | |
| Long time | 14.0 | 8.3 | 8.3 | |
| TOTAL | 100.0 | 100.0 | 100.0 | |
| Emotional state: anxious | Never | 46.7 | 39.4 | 41.7 |
| Shortly | 29.6 | 38.9 | 36.7 | |
| Half of the time | 11.8 | 15.3 | 14.6 | |
| Long time | 11.9 | 6.4 | 6.9 | |
| TOTAL | 100.0 | 100.0 | 100.0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fonseca, C.; Ramos, A.; Pinho, L.G.; Morgado, B.; Oliveira, H.; Lopes, M. Functional Profile of Older Adults Hospitalized in Rehabilitation Units of the National Network of Integrated Continuous Care of Portugal: A Longitudinal Study. J. Pers. Med. 2022, 12, 1937. https://doi.org/10.3390/jpm12111937
Fonseca C, Ramos A, Pinho LG, Morgado B, Oliveira H, Lopes M. Functional Profile of Older Adults Hospitalized in Rehabilitation Units of the National Network of Integrated Continuous Care of Portugal: A Longitudinal Study. Journal of Personalized Medicine. 2022; 12(11):1937. https://doi.org/10.3390/jpm12111937
Chicago/Turabian StyleFonseca, César, Ana Ramos, Lara Guedes Pinho, Bruno Morgado, Henrique Oliveira, and Manuel Lopes. 2022. "Functional Profile of Older Adults Hospitalized in Rehabilitation Units of the National Network of Integrated Continuous Care of Portugal: A Longitudinal Study" Journal of Personalized Medicine 12, no. 11: 1937. https://doi.org/10.3390/jpm12111937