
Postoperative Inpatient Rehabilitation Does Not Increase Knee Function after Primary Total Knee Arthroplasty
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
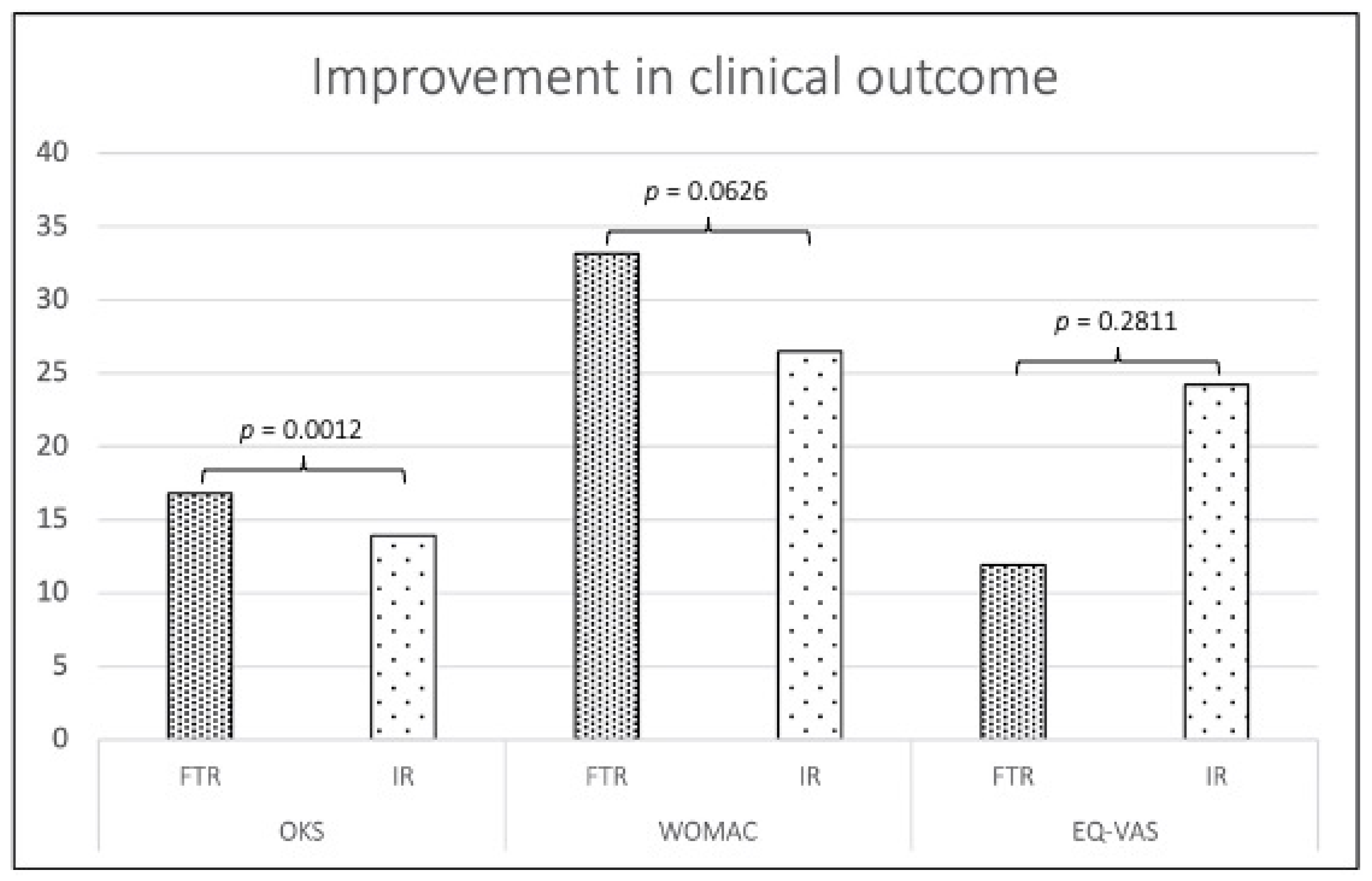
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jiang, L.; Rong, J.; Wang, Y.; Hu, F.; Bao, C.; Li, X.; Zhao, Y. The relationship between body mass index and hip osteoarthritis: A systematic review and meta-analysis. Jt. Bone Spine Rev. Du Rhum. 2011, 78, 150. [Google Scholar] [CrossRef] [PubMed]
- Mahomed, N.N.; Davis, A.M.; Hawker, G.; Badley, E.; Davey, J.R.; Syed, K.A.; Coyte, P.C.; Gandhi, R.; Wright, J.G. Inpatient compared with home-based rehabilitation following primary unilateral total hip or knee replacement: A randomized controlled trial. J. Bone Jt. Surg. Am. 2008, 90, 1673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett, R.A., III; Serino, J.; Yang, J.; Della Valle, C.J.; Courtney, P.M. National trends in post-acute care costs following total knee arthroplasty from 2007 to 2016. J. Arthroplast. 2021, 36, 2268. [Google Scholar] [CrossRef]
- Naylor, J.M.; Hart, A.; Mittal, R.; Harris, I.; Xuan, W. The value of inpatient rehabilitation after uncomplicated knee arthroplasty: A propensity score analysis. Med. J. Aust. 2017, 207, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Aarid, N. Effektivität von Stationärer und Ambulanter Rehabilitation bei Patienten Nach Knieendoprothesen-Implantation; Universität Rostock: Rostock, Germany, 2019. [Google Scholar]
- Fussenich, W.; Gerhardt, D.M.; Pauly, T.; Lorenz, F.; Olieslagers, M.; Braun, C.; van Susante, J.L. A comparative health care inventory for primary hip arthroplasty between Germany versus the Netherlands. Is there a downside effect to fast-track surgery with regard to patient satisfaction and functional outcome? Hip. Int. 2020, 30, 423. [Google Scholar] [CrossRef] [PubMed]
- Onggo, J.R.; Onggo, J.D.; De Steiger, R.; Hau, R. The Efficacy and Safety of Inpatient Rehabilitation Compared with Home Discharge After Hip or Knee Arthroplasty: A Meta-Analysis and Systematic Review. J. Arthroplast. 2019, 34, 1823. [Google Scholar] [CrossRef]
- Scott, C.E.H.; Bell, K.R.; Ng, R.T.; MacDonald, D.J.; Patton, J.T.; Burnett, R. Excellent 10-year patient-reported outcomes and survival in a single-radius, cruciate-retaining total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1106. [Google Scholar] [CrossRef] [Green Version]
- Cosendey, K.; Eudier, A.; Fleury, N.; Pereira, L.C.; Favre, J.; Jolles, B.M. Ten-year follow-up of a total knee prosthesis combining multi-radius, ultra-congruency, posterior-stabilization and mobile-bearing insert shows long-lasting clinically relevant improvements in pain, stiffness, function and stability. Knee Surg. Sports Traumatol. Arthrosc. 2022; online ahead of print. [Google Scholar]
- Fransen, B.L.; Hoozemans, M.J.; Argelo, K.D.; Keijser, L.; Burger, B.J. Fast-track total knee arthroplasty improved clinical and functional outcome in the first 7 days after surgery: A randomized controlled pilot study with 5-year follow-up. Arch. Orthop. Trauma Surg. 2018, 138, 1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seetharam, A.; Deckard, E.R.; Ziemba-Davis, M.; Meneghini, R.M. The AAHKS clinical research award: Are minimum two-year patient-reported outcome measures necessary for accurate assessment of patient outcomes after primary total knee arthroplasty? J. Arthroplast. 2022, 37, S716–S720. [Google Scholar] [CrossRef] [PubMed]
- Clement, N.; MacDonald, D.; Simpson, A. The minimal clinically important difference in the Oxford knee score and Short Form 12 score after total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1933. [Google Scholar] [CrossRef] [PubMed]
- Clement, N.D.; Bardgett, M.; Weir, D.; Holland, J.; Gerrand, C.; Deehan, D.J. What is the Minimum Clinically Important Difference for the WOMAC Index After TKA? Clin. Orthop. Relat. Res. 2018, 476, 2005. [Google Scholar] [CrossRef] [PubMed]
- Tsai, A.P.Y.; Hur, S.A.; Wong, A.; Safavi, M.; Assayag, D.; Johannson, K.A.; Morisset, J.; Fell, C.; Fisher, J.H.; Manganas, H.; et al. Minimum important difference of the EQ-5D-5L and EQ-VAS in fibrotic interstitial lung disease. Thorax 2021, 76, 37. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Buhagiar, M.A.; Naylor, J.M.; Harris, I.A.; Xuan, W.; Kohler, F.; Wright, R.; Fortunato, R. Effect of Inpatient Rehabilitation vs a Monitored Home-Based Program on Mobility in Patients With Total Knee Arthroplasty: The HIHO Randomized Clinical Trial. JAMA 2017, 317, 1037. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.Y.; Sultana, R.; Yeo, S.J.; Chia, S.L.; Pang, H.N.; Lo, N.N. Comparison of outcome measures from different pathways following total knee arthroplasty. Singap. Med. J. 2018, 59, 476. [Google Scholar]
- Jorgenson, E.S.; Richardson, D.M.; Thomasson, A.M.; Nelson, C.L.; Ibrahim, S.A. Race, Rehabilitation, and 30-Day Readmission After Elective Total Knee Arthroplasty. Geriatr. Orthop. Surg. Rehabil. 2015, 6, 303. [Google Scholar] [CrossRef] [PubMed]
- White, P.B.; Carli, A.V.; Meftah, M.; Ghazi, N.; Alexiades, M.M.; Windsor, R.E.; Ranawat, A.S. Patients Discharged to Inpatient Rehabilitation Facilities Undergo More Diagnostic Interventions with No Improvement in Outcomes. Orthopedics 2018, 41, E841. [Google Scholar] [CrossRef] [PubMed]
- Nöth, U.; Rackwitz, L.; Clarius, M. Herausforderungen der Fast-Track-Endoprothetik in Deutschland. Der Orthopäde 2020, 49, 334. [Google Scholar] [CrossRef] [PubMed]
- Lindström, B.; Eriksson, M. Salutogenesis. J. Epidemiol. Community Health 2005, 59, 440. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Rehabilitation Protocol | FTR-Canada (n = 101) | IR-Germany (n = 104) | p-Value | |
|---|---|---|---|---|
| Age (years) mean ± SD | 66 ± 8 | 67 ± 10 | 0.703 | |
| Sex | Female (n) (%) | 65 (64%) | 57 (55%) | 0.205 |
| Male (n) (%) | 36 (36%) | 47 (45%) | ||
| BMI mean ± SD | 30.1 ± 6.4 | 31.6 ± 6.0 | 0.029 | |
| ASA | 0.189 | |||
| I (n) (%) | 9 (9%) | 4 (4%) | ||
| II (n) (%) | 71 (70%) | 70 (67%) | ||
| III (n) (%) | 21 (21%) | 30 (29%) |
| Rehabilitation Protocol | Pre-Operative Mean ± SD | p-Value | 1-Year Follow-Up Mean ± SD | p-Value | Clinical Improvement ∆ Mean ± SD | p-Value | |
|---|---|---|---|---|---|---|---|
| OKS | FTR | 21.9 ± 8.4 | 0.111 | 38.7 ± 8.8 | <0.001 | 16.8 ± 10.6 | 0.001 |
| IR | 19.9 ± 6.6 | 33.9 ± 9.9 | 14.0 ± 10.7 | ||||
| WOMAC | FTR | 47.7 ± 20.1 | 0.177 | 14.7 ± 15.2 | 0.571 | 33.2 ± 20.6 | 0.063 |
| IR | 44.8 ± 19.8 | 18.3 ± 18.7 | 26.5 ± 25.5 | ||||
| EQ-VAS | FTR | 66.4 ± 19.6 | <0.001 | 78.6 ± 17.6 | 0.103 | 11.9 ± 24.2 | 0.281 |
| IR | 48.4 ± 17.3 | 72.6 ± 22.1 | 24.2 ±26.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rak, D.; Nedopil, A.J.; Sayre, E.C.; Masri, B.A.; Rudert, M. Postoperative Inpatient Rehabilitation Does Not Increase Knee Function after Primary Total Knee Arthroplasty. J. Pers. Med. 2022, 12, 1934. https://doi.org/10.3390/jpm12111934
Rak D, Nedopil AJ, Sayre EC, Masri BA, Rudert M. Postoperative Inpatient Rehabilitation Does Not Increase Knee Function after Primary Total Knee Arthroplasty. Journal of Personalized Medicine. 2022; 12(11):1934. https://doi.org/10.3390/jpm12111934
Chicago/Turabian StyleRak, Dominik, Alexander J. Nedopil, Eric C. Sayre, Bassam A. Masri, and Maximilian Rudert. 2022. "Postoperative Inpatient Rehabilitation Does Not Increase Knee Function after Primary Total Knee Arthroplasty" Journal of Personalized Medicine 12, no. 11: 1934. https://doi.org/10.3390/jpm12111934