
Combination of Radiomics Features and Functional Radiosensitivity Enhances Prediction of Acute Pulmonary Toxicity in a Prospective Validation Cohort of Patients with a Locally Advanced Lung Cancer Treated with VMAT-Radiotherapy
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Toxicities
2.3. Clinical and Dosimetric Features
2.4. Radiomics and Pmap Features
2.5. Statistical Analysis
- -
- Three without SMOTE: RadNonSmote, PmapNonSmote, and CombNonSmote
- -
- Three with SMOTE: RadSmote, PmapSmote, and CombSmote
3. Results
3.1. Population
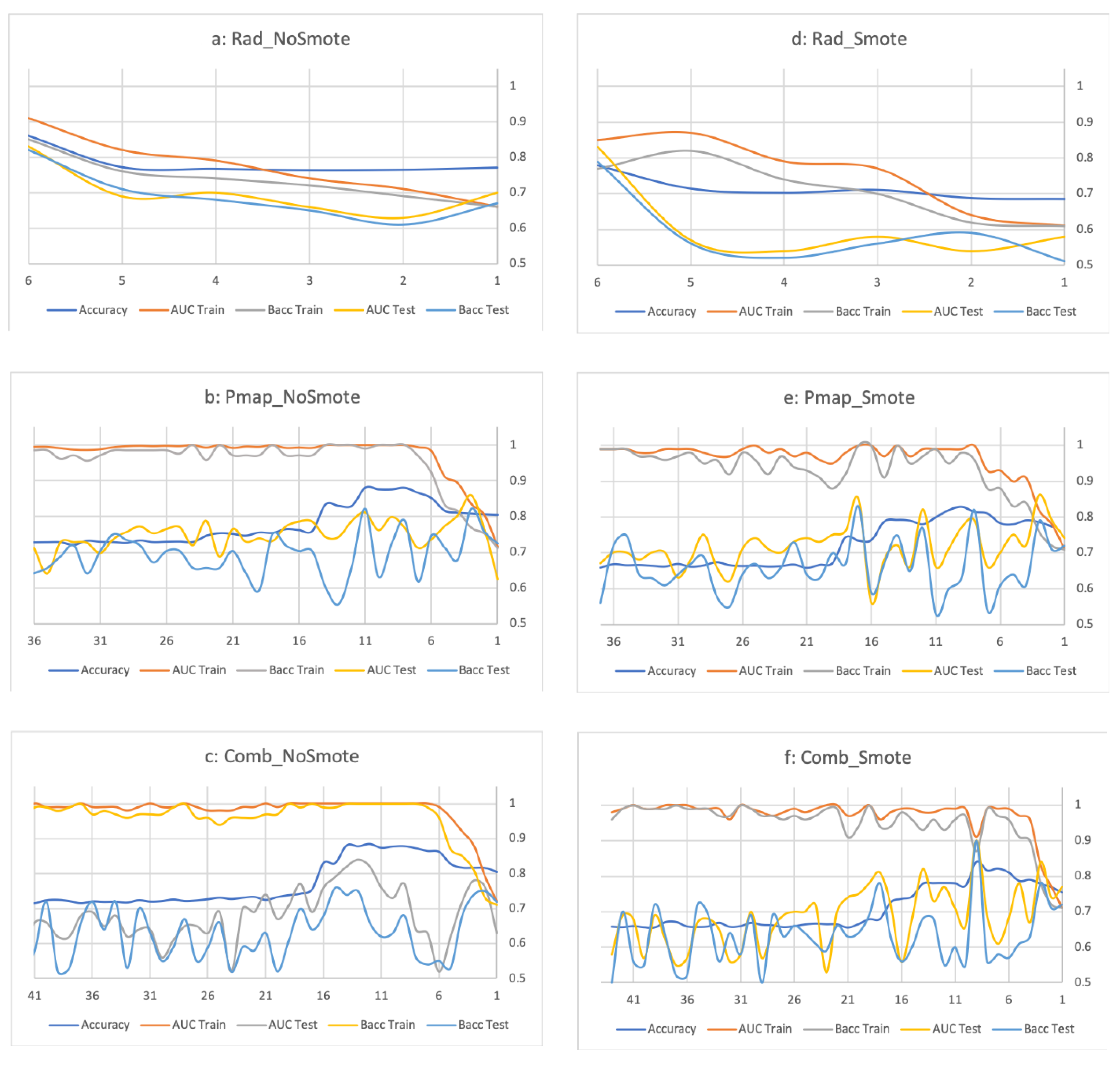
3.2. Radiomics and Pmap-Models
3.3. Combined Model
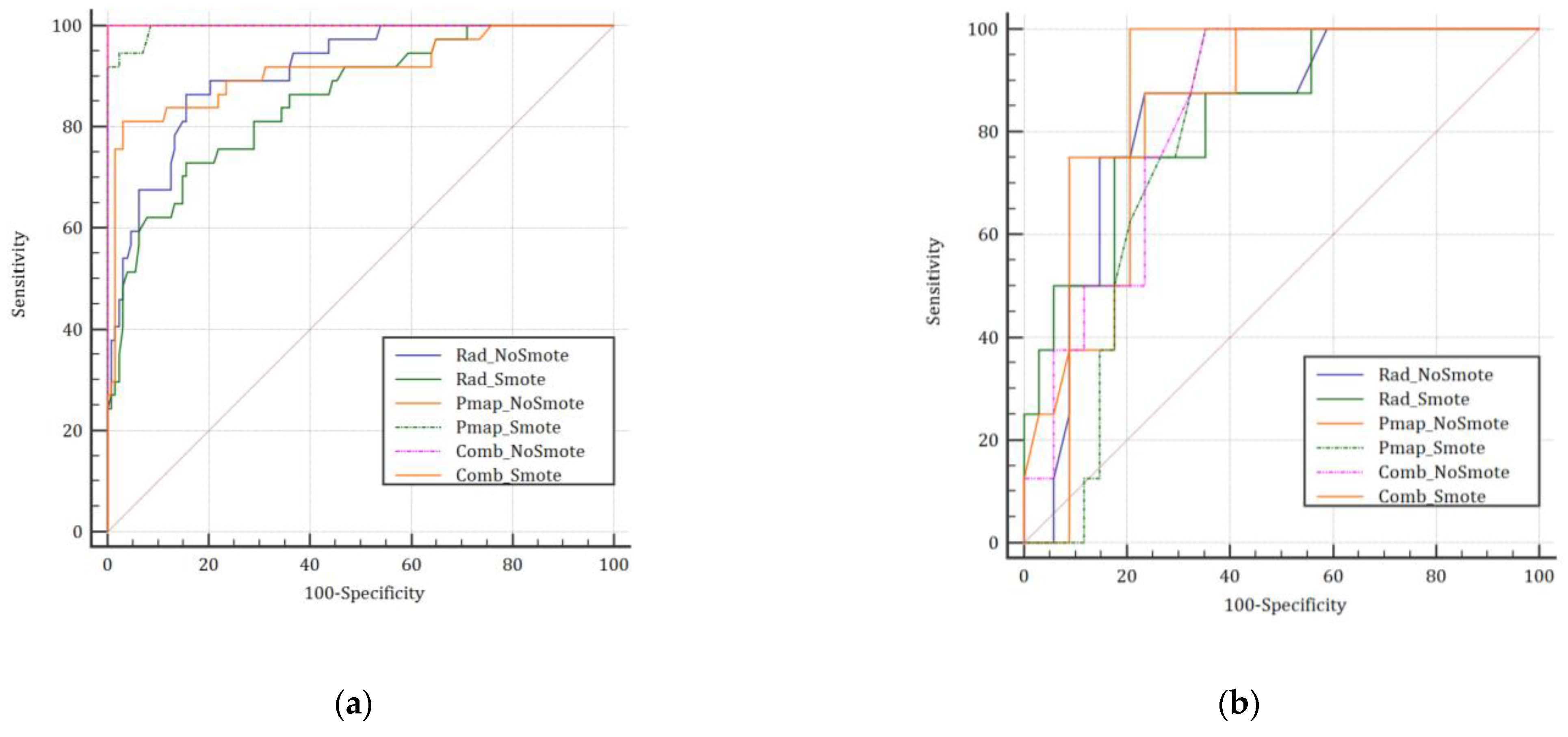
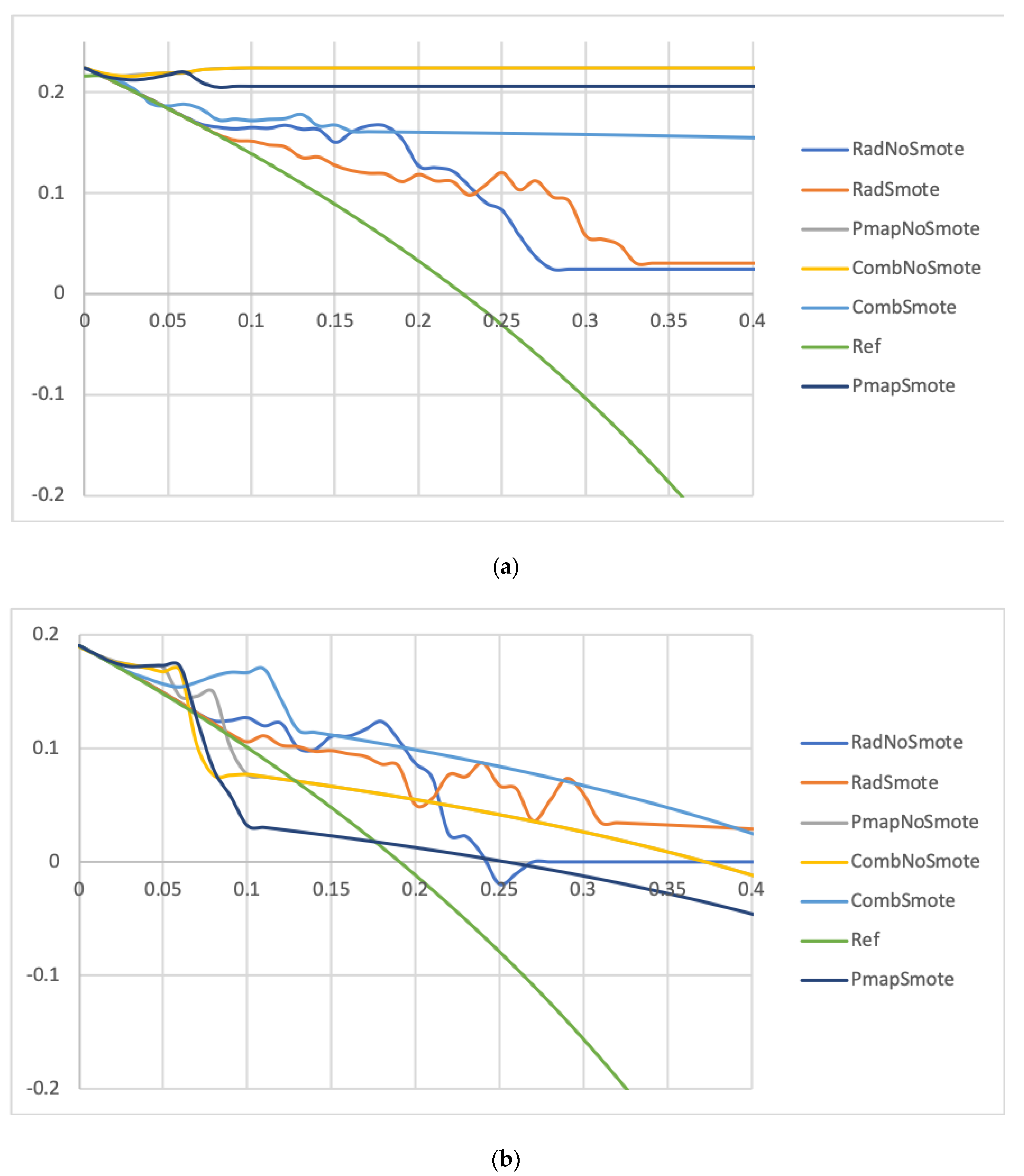
3.4. Model Comparison for the Prediction of APT ≥ Grade 2 and APT ≥ Grade 3
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized ” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. NCCN Guidelines Insights: Non-Small Cell Lung Cancer, Version 2.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [Green Version]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourbonne, V.; Da-Ano, R.; Jaouen, V.; Lucia, F.; Dissaux, G.; Bert, J.; Pradier, O.; Visvikis, D.; Hatt, M.; Schick, U. Radiomics analysis of 3D dose distributions to predict toxicity of radiotherapy for lung cancer. Radiother. Oncol. 2021, 155, 144–150. [Google Scholar] [CrossRef]
- Bucknell, N.; Hardcastle, N.; Jackson, P.; Hofman, M.; Callahan, J.; Eu, P.; Iravani, A.; Lawrence, R.; Martin, O.; Bressel, M.; et al. Single-arm prospective interventional study assessing feasibility of using gallium-68 ventilation and perfusion PET/CT to avoid functional lung in patients with stage III non-small cell lung cancer. BMJ Open 2020, 10, e042465. [Google Scholar] [CrossRef]
- Le Roux, P.Y.; Hicks, R.J.; Siva, S.; Hofman, M.S. PET/CT Lung Ventilation and Perfusion Scanning Using Galligas and Gallium-68-MAA. Semin. Nucl. Med. 2019, 49, 71–81. [Google Scholar] [CrossRef]
- Siva, S.; Thomas, R.; Callahan, J.; Hardcastle, N.; Pham, D.; Kron, T.; Hicks, R.; MacManus, M.; Ball, D.L.; Hofman, M.S. High-resolution pulmonary ventilation and perfusion PET/CT allows for functionally adapted intensity modulated radiotherapy in lung cancer. Radiother. Oncol. 2015, 115, 157–162. [Google Scholar] [CrossRef]
- Westergaard, S.A.; Castillo, R.; Rupji, M.; Bell, J.; Castro, R.; Harms, J.; Kayode, O.; Nguyen, T.; Wolf, J.; Higgins, K.; et al. Sparing Functional Lung Using Optimized Volumetric Modulated Arc Therapy in Thoracic Radiation for Locally Advanced Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, e456–e457. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; Cella, L. Voxel-based analysis in radiation oncology: A methodological cookbook. Phys. Med. 2020, 69, 192–204. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; Xu, T.; Scifoni, E.; Yang, P.; Hahn, S.M.; Durante, M.; Mohan, R.; Liao, Z.; Cella, L. Spatial Dose Patterns Associated with Radiation Pneumonitis in a Randomized Trial Comparing Intensity-Modulated Photon Therapy with Passive Scattering Proton Therapy for Locally Advanced Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1124–1132. [Google Scholar] [CrossRef]
- Bourbonne, V.; Lucia, F.; Jaouen, V.; Bert, J.; Rehn, M.; Pradier, O.; Visvikis, D.; Schick, U. Development and prospective validation of a spatial dose pattern based model predicting acute pulmonary toxicity in patients treated with volumetric arc-therapy for locally advanced lung cancer. Radiother. Oncol. 2021, 164, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lema, G.; Nogueira, F.; Aridas, C.K. Imbalanced-Learn: A Python Toolbox to Tackle the Curse of Imbalanced Datasets in Machine Learning. J. Mach. Learn. Res. 2017, 18, 1–5. [Google Scholar]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Bourbonne, V.; Delafoy, A.; Lucia, F.; Quéré, G.; Pradier, O.; Schick, U. Toxicity after volumetric modulated arc therapy for lung cancer: A monocentric retrospective study. Transl. Lung Cancer Res. 2021, 10, 156–166. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef]
- Jabbour, S.K.; Lee, K.H.; Frost, N.; Breder, V.; Kowalski, D.; Alawin, I.; Levchenko, E.; Reguart, N.; Martinez-Marti, A.; Houghton, B.; et al. Pembrolizumab Plus Platinum Chemotherapy and Radiotherapy for Unresectable, Locally Advanced, Stage 3 NSCLC: KEYNOTE-799. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, S9–S10. [Google Scholar] [CrossRef]
- Weber, D.C.; Hurkmans, C.W.; Melidis, C.; Budach, W.; Langendijk, J.H.; Peters, L.J.; Gregoire, V.; Maingon, P.; Combescure, C. Outcome impact and cost-effectiveness of quality assurance for radiotherapy planned for the EORTC 22071–24071 prospective study for head and neck cancer. Radiother. Oncol. 2014, 111, 393–399. [Google Scholar] [CrossRef]
- Ohri, N.; Shen, X.; Dicker, A.; Doyle, L.A.; Harrison, A.S.; Showalter, T. Radiotherapy Protocol Deviations and Clinical Outcomes: A Meta-analysis of Cooperative Group Clinical Trials. J. Natl. Cancer Inst. 2013, 105, 387–393. [Google Scholar] [CrossRef]
- Peters, S.; Felip, E.; Dafni, U.; Belka, C.; Guckenberger, M.; Irigoyen, A.; Nadal, E.; Becker, A.; Vees, H.; Pless, M.; et al. Safety evaluation of nivolumab added concurrently to radiotherapy in a standard first line chemo-radiotherapy regimen in stage III non-small cell lung cancer—The ETOP NICOLAS trial. Lung Cancer 2019, 133, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.H.; Lin, Y.; Yao, L.; Kalhor, N.; Carter, B.W.; Altan, M.; Blumenschein, G.; Byers, L.A.; Fossela, F.; Gibbons, D.L.; et al. Phase II Trial of Concurrent Atezolizumab with Chemoradiation for Unresectable NSCLC. J. Thorac. Oncol. 2020, 15, 248–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jabbour, S.K.; Cho, B.C.; Bria, E.; Kato, T.; Bhosle, J.; Gainor, J.; Reguart, N.; Wang, L.; Morgensztern, D.; Gurary, E.; et al. KEYLYNK-012: A Phase 3 Study of Pembrolizumab with Concurrent Chemoradiation Therapy (CCRT) Followed by Pembrolizumab with or without Olaparib vs. CCRT Followed by Durvalumab in Unresectable, Locally Advanced, Stage III Non-Small-Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, e440–e441. [Google Scholar] [CrossRef]
- Bradley, J.D.; Nishio, M.; Okamoto, I.; Newton, M.D.; Trani, L.; Shire, N.J.; Gu, Y.; Dennis, P.A.; Lee, K.H. PACIFIC-2: Phase 3 study of concurrent durvalumab and platinum-based chemoradiotherapy in patients with unresectable, stage III NSCLC. J. Clin. Oncol. 2019, 37, TPS8573. [Google Scholar] [CrossRef]
- Leal, T.; Wang, Y.; Dowlati, A.; Lewis, D.A.; Chen, Y.; Mohindra, A.R.; Razaq, M.; Ahuja, H.G.; Liu, J.; King, D.M.; et al. Randomized phase II clinical trial of cisplatin/carboplatin and etoposide (CE) alone or in combination with nivolumab as frontline therapy for extensive-stage small cell lung cancer (ES-SCLC): ECOG-ACRIN EA5161. J. Clin. Oncol. 2020, 38, 9000. [Google Scholar] [CrossRef]
- Varlotto, J.M.; Sun, Z.; Ky, B.; Upshaw, J.; Katz, S.I.; Fitzgerald, T.J.; Wakelee, H.; Diehn, M.; Mankoff, D.A.; Lovely, C.; et al. A Review of Immunotherapy for Stage III and Metastatic Non-Small Cell Lung Cancer and the Rationale for the ECOG-ACRIN EA5181 Study. Oncologist 2021, 26, 523–532. [Google Scholar] [CrossRef]
- Lucia, F.; Rehn, M.; Blanc-Béguin, F.; Le Roux, P.-Y. Radiation Therapy Planning of Thoracic Tumors: A Review of Challenges Associated with Lung Toxicities and Potential Perspectives of Gallium-68 Lung PET/CT Imaging. Front. Med. 2021, 8, 723748. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Set | AUC | p | Cut-Off | C-Index | Se | Sp | BAcc | F1 | Number of Patients, n (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Below the Cutoff (Low Risk of APT ≥ Grade 2) | Above the Cutoff (High Risk of APT ≥ Grade 2) | |||||||||||||
| Total | Without APT | With APT | Total | Without APT | With APT | |||||||||
| RadNoSmote | 0.91 | <0.0001 | >18% | 0.85 | 86.5 | 84.4 | 85.5 | 0.72 | 113 (68.5%) | 108 (95.6%) | 5 (4.4%) | 52 (31.5%) | 20 (38.5%) | 32 (61.5%) |
| RadSmote | 0.85 | <0.0001 | >24% | 0.77 | 75.7 | 78.1 | 76.9 | 0.66 | 109 (66.1%) | 100 (91.7%) | 9 (8.3%) | 56 (33.9%) | 28 (50.0%) | 28 (50.0%) |
| PmapNoSmote | 0.99 | <0.0001 | >8% | 0.99 | 100.0 | 98.4 | 99.2 | 1.00 | 126 (76.4%) | 126 (100.0%) | 0 (0.0%) | 39 (23.6%) | 2 (5.1%) | 37 (94.9%) |
| PmapSmote | 0.99 | <0.0001 | >6% | 0.96 | 100.0 | 91.4 | 95.7 | 0.96 | 117 (70.9%) | 117 (100.0%) | 0 (0.0%) | 48 (29.1%) | 11 (22.9%) | 37 (77.1%) |
| CombNoSmote | 0.99 | <0.0001 | >8% | 0.99 | 100 | 98.4 | 99.2 | 1.00 | 126 (76.4%) | 126 (100.0%) | 0 (0.0%) | 39 (23.6%) | 2 (5.1%) | 37 (94.9%) |
| CombSmote | 0.91 | <0.0001 | >12% | 0.87 | 81.1 | 92.2 | 86.7 | 0.85 | 125 (75.8%) | 118 (94.4%) | 7 (5.6%) | 40 (24.2%) | 10 (25.0%) | 30 (75.0%) |
| Set | AUC | p | Cut-Off | C-Index | Se | Sp | BAcc | F1 | Number of Patients, n (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Below the Cutoff (Low Risk of APT ≥ Grade 2 | Above the Cutoff (High Risk of APT ≥ Grade 2) | |||||||||||||
| Total | Without APT | With APT | Total | Without APT | With APT | |||||||||
| RadNoSmote | 0.83 | <0.0001 | >18% | 0.82 | 87.5 | 76.5 | 82.0 | 0.63 | 27 (64.3%) | 26 (96.3%) | 1 (3.7%) | 15 (35.7%) | 8 (53.3%) | 7 (46.7%) |
| RadSmote | 0.83 | <0.0001 | >24% | 0.79 | 75.0 | 82.4 | 78.7 | 0.60 | 30 (71.4%) | 28 (93.3%) | 2 (6.7%) | 12 (28.6%) | 6 (50.0%) | 6 (50.0%) |
| PmapNoSmote | 0.81 | <0.0001 | >8% | 0.82 | 87.5 | 76.5 | 82.0 | 0.61 | 27 (64.3%) | 26 (96.3%) | 1 (3.7%) | 15 (35.7%) | 8 (53.3%) | 7 (46.7%) |
| PmapSmote | 0.79 | <0.0001 | >6% | 0.82 | 100.0 | 64.7 | 82.4 | 0.57 | 22 (52.4%) | 22 (100.0%) | 0 (0.0%) | 20 (47.6%) | 12 (60.0%) | 8 (40.0%) |
| CombNoSmote | 0.83 | <0.0001 | > 8% | 0.70 | 62.5 | 76.5 | 69.5 | 0.57 | 29 (69.0%) | 26 (89.7%) | 3 (10.3%) | 13 (31.0%) | 8 (61.5%) | 5 (38.5%) |
| CombSmote | 0.90 | <0.0001 | >12% | 0.90 | 100.0 | 79.4 | 89.7 | 0.71 | 27 (64.3%) | 27 (100.0%) | 0 (0.0%) | 15 (35.7%) | 7 (46.7%) | 8 (53.3%) |
| RadNoSmote Model | RadSmote Model | PmapNoSmote Model | PmapSmote Model | CombNoSmote Model | CombSmote Model | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Feature | Importance | Feature | Importance | Feature | Importance | Feature | Importance | Feature | Importance | Feature | Importance |
| LungH_Variance | 0.1% | LungH_Entropy | 1.9% | V40Heart | 5.0% | Stage | 3.6% | V40Heart | 4.4% | V13LungH | 3.3% |
| LungH_DVAR | 1.5% | Lungs_Energy | 4.5% | DMeanLungH | 5.0% | V5LungH | 5.0% | DMeanLungH | 5.0% | V5LungH | 3.8% |
| LungH_Contrast | 3.2% | LungH_IC1 | 15.6% | V5LungH | 5.0% | MEVS | 5.4% | V5LungH | 5.0% | V10LungH | 4.4% |
| LungH_IC1 | 15.2% | LungH_DVAR | 16.9% | AJCC Stage | 5.0% | V10LungH | 6.1% | AJCC Stage | 5.1% | DMeanLungH | 4.8% |
| LungH_Entropy | 20.5% | LungH_Contrast | 18.1% | V10LungH | 6.0% | DMeanLungH | 6.6% | V10LungH | 5.5% | V302Lungs | 6.3% |
| Lungs_Energy | 58.5% | LungH_Variance | 43.0% | COPD | 6.0% | V302Lungs | 10.2% | COPD | 6.1% | COPD | 10.4% |
| MEVS | 7.0% | DMean2Lungs | 15.5% | MEVS | 6.1% | DMean2Lungs | 10.5% | ||||
| Smoking Status | 7.0% | DMeanPmap | 47.7% | Smoking Status | 6.2% | LungH_Variance | 12.6% | ||||
| V302Lungs | 7.0% | V302Lungs | 6.7% | DMeanPmap | 44.1% | ||||||
| DMean2Lungs | 11.0% | LungH_Variance | 7.1% | ||||||||
| DMeanPmap | 36.0% | DMean2Lungs | 10.1% | ||||||||
| DMeanPmap | 32.7% | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bourbonne, V.; Lucia, F.; Jaouen, V.; Pradier, O.; Visvikis, D.; Schick, U. Combination of Radiomics Features and Functional Radiosensitivity Enhances Prediction of Acute Pulmonary Toxicity in a Prospective Validation Cohort of Patients with a Locally Advanced Lung Cancer Treated with VMAT-Radiotherapy. J. Pers. Med. 2022, 12, 1926. https://doi.org/10.3390/jpm12111926
Bourbonne V, Lucia F, Jaouen V, Pradier O, Visvikis D, Schick U. Combination of Radiomics Features and Functional Radiosensitivity Enhances Prediction of Acute Pulmonary Toxicity in a Prospective Validation Cohort of Patients with a Locally Advanced Lung Cancer Treated with VMAT-Radiotherapy. Journal of Personalized Medicine. 2022; 12(11):1926. https://doi.org/10.3390/jpm12111926
Chicago/Turabian StyleBourbonne, Vincent, François Lucia, Vincent Jaouen, Olivier Pradier, Dimitris Visvikis, and Ulrike Schick. 2022. "Combination of Radiomics Features and Functional Radiosensitivity Enhances Prediction of Acute Pulmonary Toxicity in a Prospective Validation Cohort of Patients with a Locally Advanced Lung Cancer Treated with VMAT-Radiotherapy" Journal of Personalized Medicine 12, no. 11: 1926. https://doi.org/10.3390/jpm12111926