Multimorbidity, Frailty and Diabetes in Older People–Identifying Interrelationships and Outcomes

Abstract
:1. Introduction
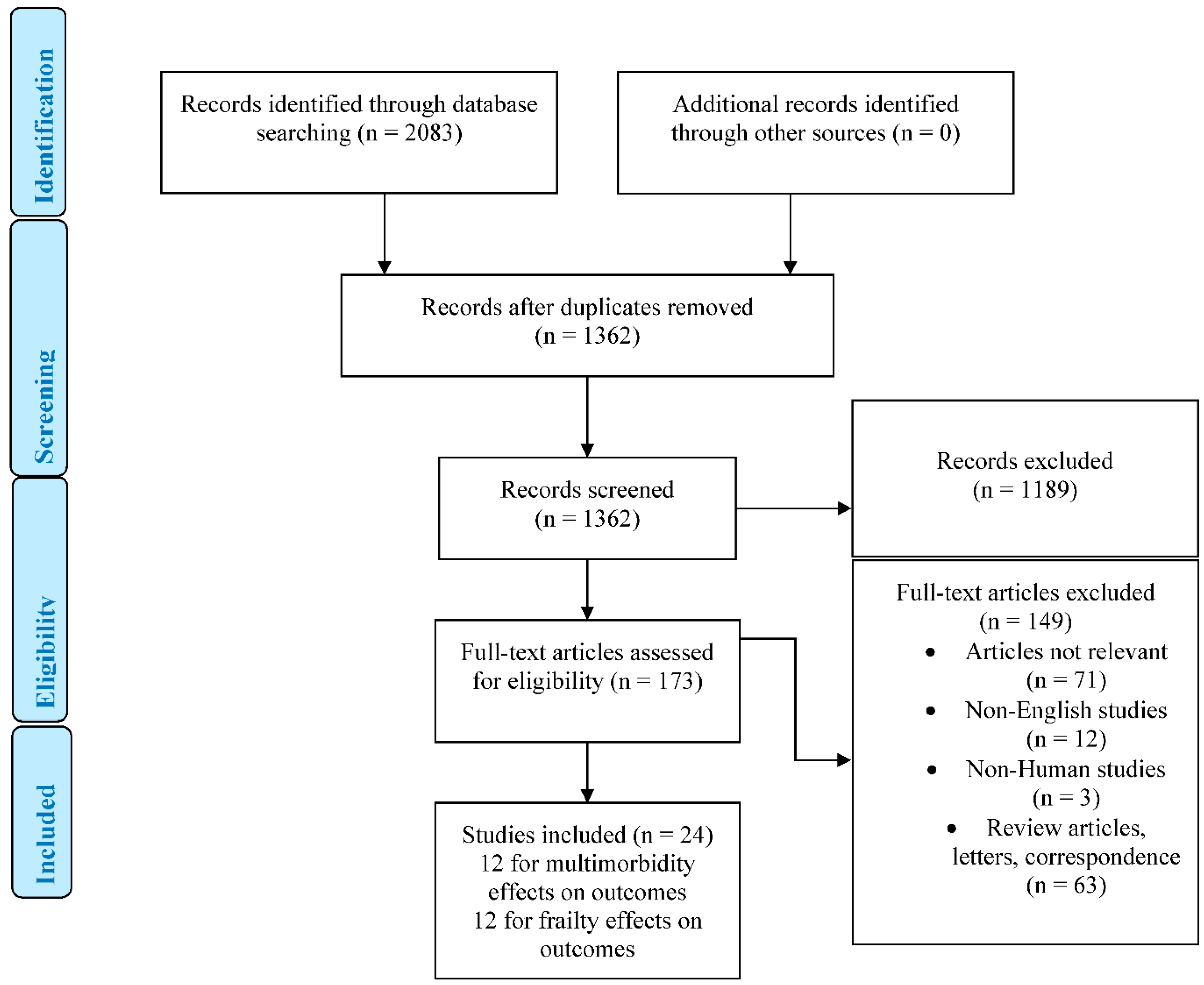
2. Methods
2.1. Data Sources
2.2. Study Selection
2.3. Data Extraction
3. Multimorbidity
4. Frailty
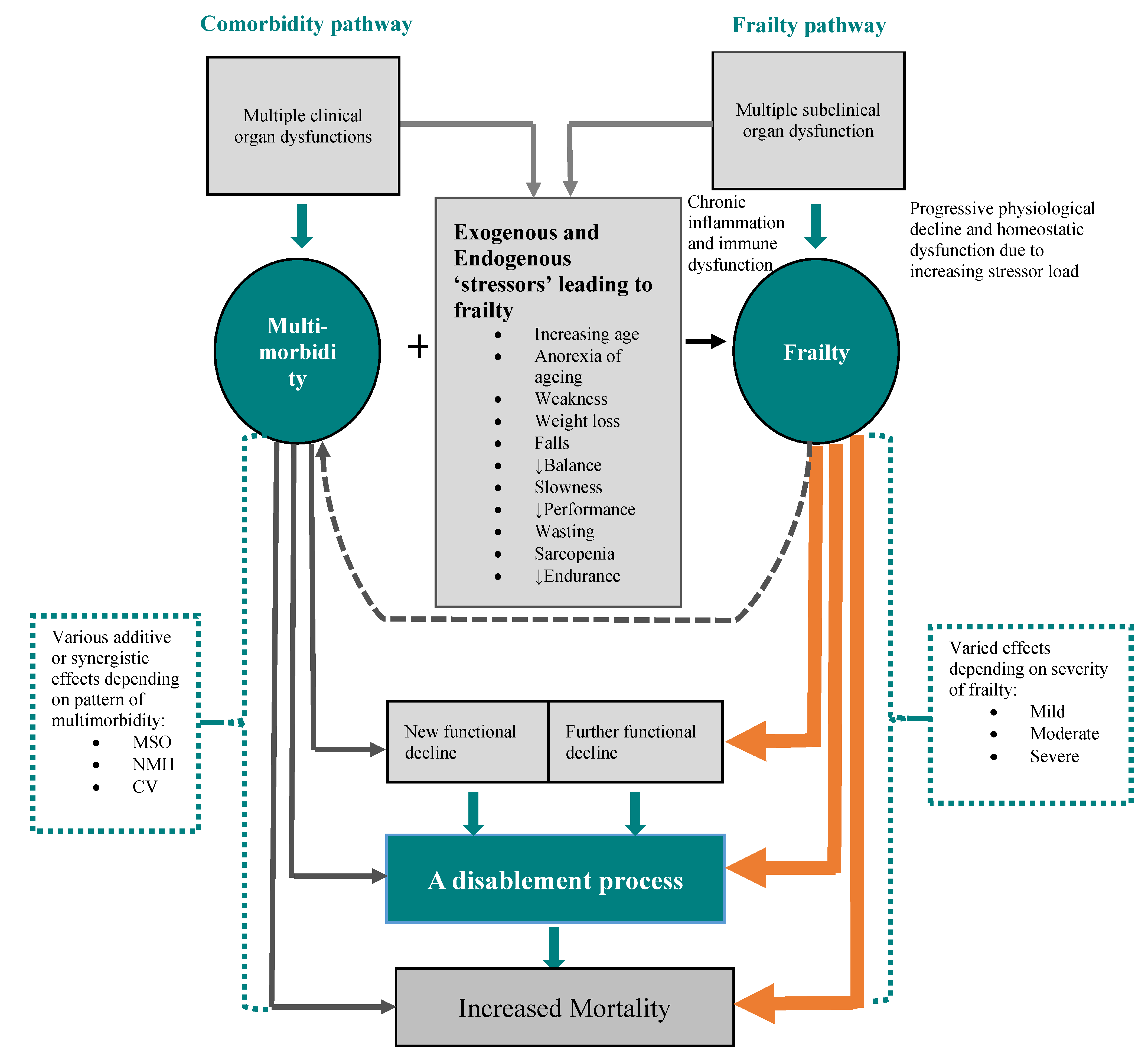
5. Multimorbidity and Frailty: Identifying Early Differences
6. Effects of Diabetes on Multimorbidity and Frailty
7. Effects of Multimorbidity and Frailty on Diabetes
7.1. Effects of Multimorbidity
7.2. Effects of Frailty
8. Discussion
8.1. Patterns of Multimorbidity
8.2. Multimorbidity-Frailty Overlap
8.3. Identifying Interventions to Target Multimorbidity and Frailty
9. Conclusions
10. Future Perspectives
11. Key Points
- Multimorbidity and frailty are predictors of adverse outcomes in older people with diabetes.
- Whilst the pathogenesis and nature of multimorbidity and frailty may be diverse, the adverse outcomes predicted by multimorbidity and frailty are similar.
- Mental health disorders significantly augment adverse outcomes predicted by multimorbidity.
- The predictor effect of multimorbidity independent of frailty, and vice versa, still needs further clarification.
- Prospective clinical trials are required to investigate whether interventions to reduce multimorbidity and frailty would improve outcomes.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sinclair, A.; Saeedi, P.; Kaundal, A.; Karuranga, S.; Malanda, B.; Williams, R. Diabetes and global ageing among 65-99-year-old adults: Findings from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2020, 162, 108078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinclair, A.J.; Abdelhafiz, A.H.; Rodríguez-Mañas, L. Frailty and sarcopenia-newly emerging and high impact complications of diabetes. J. Diabetes Its Complicat. 2017, 31, 1465–1473. [Google Scholar] [CrossRef] [PubMed]
- Pearson-Stuttard, J.; Bennett, J.; Cheng, Y.J.; Vamos, E.P.; Cross, A.J.; Ezzati, M.; Gregg, E.W. Trends in predominant causes of death in individuals with and without diabetes in England from 2001 to 2018: An epidemiological analysis of linked primary care records. Lancet Diabetes Endocrinol. 2021, 9, 165–173. [Google Scholar] [CrossRef]
- Lascar, N.; Brown, J.; Pattison, H.; Barnett, A.H.; Bailey, C.J.; Bellary, S. Type 2 diabetes in adolescents and young adults. Lancet Diabetes Endocrinol. 2018, 6, 69–80. [Google Scholar] [CrossRef] [Green Version]
- Magnan, E.M.; Bolt, D.M.; Greenlee, R.T.; Fink, J.; Smith, M.A. Stratifying patients with diabetes into clinically relevant groups by combination of chronic conditions to identify gaps in quality of care. Health Serv. Res. 2018, 53, 450–468. [Google Scholar] [CrossRef]
- Iglay, K.; Hannachi, H.; Joseph Howie, P.; Xu, J.; Li, X.; Engel, S.S.; Moore, L.M.; Rajpathak, S. Prevalence and co-prevalence of co- morbidities among patients with type 2 diabetes mellitus. Curr. Med. Res. Opin. 2016, 32, 1243–1252. [Google Scholar] [CrossRef]
- Turner, G.; British Geriatrics Society; Age, U.K.; Royal College of General Practioners. Best practice guidelines for the management of frailty: A British Geriatrics Society, Age UK and Royal College of General Practitioners report. Age Ageing 2014, 43, 7447. [Google Scholar] [CrossRef] [Green Version]
- Feinstein, A.R. The Pre-therapeutic classification of comorbidity in chronic disease. J. Chronic Dis. 1970, 23, 455–468. [Google Scholar] [CrossRef]
- Nguyen, H.; Manolova, G.; Daskalopoulou, C.; Vitoratou, S.; Prince, M.; Prina, A.M. Prevalence of multimorbidity in community settings: A systematic review and meta-analysis of observational studies. J. Comorb. 2019, 9, 2235042X19870934. [Google Scholar] [CrossRef] [Green Version]
- Salive, M.E. Multimorbidity in older adults. Epidemiol. Rev. 2013, 35, 75–83. [Google Scholar] [CrossRef]
- Valderas, J.M.; Starfield, B.; Sibbald, B.; Salisbury, C.; Roland, M. Defining comorbidity: Implications for understanding health and health services. Ann. Fam. Med. 2009, 7, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, C. Health care quality and multimorbidity: The jury is still out. Med. Care 2007, 45, 477–479. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Groot, V.; Beckerman, H.; Lankhorst, G.J.; Bouter, L.M. How to measure comorbidity. a critical review of available methods. J. Clin. Epidemiol. 2003, 56, 221–229. [Google Scholar] [CrossRef] [Green Version]
- Concato, J.; Horwitz, R.I.; Feinstein, A.R.; Elmore, J.G.; Schiff, S.F. Prob- lems of comorbidity in mortality after prostatectomy. JAMA 1992, 267, 1077–1082. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Roos, L.L.J.; Nicol, J.P.; Cageorge, S.M. Using administrative data for longitudinal research: Comparisons with primary data collection. J. Chronic Dis. 1987, 40, 41–49. [Google Scholar] [CrossRef]
- Newschaffer, C.J.; Bush, T.L.; Penberthy, L.E.; Bellantoni, M.; Helzlsour, K.; Diener-West, M. Does comorbid disease interact with cancer? An epidemiologic analysis of mortality in a cohort of elderly breast cancer patients. J. Gerontol. 1998, 53, M372-8. [Google Scholar] [CrossRef] [Green Version]
- Kieszak, S.M.; Flanders, W.D.; Kosinski, A.S.; Shipp, C.C.; Karp, H. A comparison of the Charlson comorbidity index derived from medical record data and administrative billing data. J. Clin. Epidemiol. 1999, 52, 137–142. [Google Scholar] [CrossRef]
- Extermann, M.; Overcash, J.; Lyman, G.H.; Parr, J.; Balducci, L. Comorbidity and functional status are independent in older cancer patients. J. Clin. Oncol. 1998, 16, 1582–1587. [Google Scholar] [CrossRef]
- Miller, M.D.; Paradis, C.F.; Houck, P.R.; Mazumdar, S.; Stack, J.A.; Rifai, A.H.; Mulsant, B.; Reynolds, C.F., III. Rating chronic medical illness burden in geropsychiatric practice and research: Application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992, 41, 237–248. [Google Scholar] [CrossRef]
- Parmelee, P.A.; Thuras, P.D.; Katz, I.R.; Lawton, M.P. Validation of the Cumulative Illness Rating Scale in a geriatric residential population. J. Am. Geriatr. Soc. 1995, 43, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, S.; Apolone, G.; McNeil, B.J.; Cleary, P.D. The importance of co-existent disease in the occurrence of postoperative complications and one-year recovery in patients undergoing total hip replacement. Comorbidity and outcomes after hip replacement. Med. Care 1993, 31, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, M.H.; Feinstein, A.R. The importance of classifying initial co- morbidity in evaluating the outcome of diabetes mellitus. J. Chronic Dis. 1974, 27, 387–404. [Google Scholar] [CrossRef]
- Incalzi, R.A.; Capparella, O.; Gemma, A.; Landi, F.; Bruno, E.; Di Meo, F.; Carbonin, P.U. The interaction between age and comorbidity contributes to predicting the mortality of geriatric patients in the acute-care hospital. J. Intern. Med. 1997, 242, 291–298. [Google Scholar] [CrossRef] [Green Version]
- Bergman, H.; Ferrucci, L.; Guralnik, J.; Hogan, D.B.; Hummel, S.; Karunananthan, S.; Wolfson, C. Frailty: An emerging research and clinical paradigm-issues and controversies. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 62A, 731–737. [Google Scholar] [CrossRef] [Green Version]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Voshaar, R.O. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E. Diabetes, sarcopenia, and frailty. Clin. Geriatr. Med. 2008, 24, 455–469. [Google Scholar] [CrossRef]
- Kojima, G. Frailty as a predictor of future falls among community-dwelling older people: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2015, 16, 1027–1033. [Google Scholar] [CrossRef]
- Kojima, G. Frailty as a predictor of fractures among community-dwelling older people: A systematic review and meta-analysis. Bone 2016, 90, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G.; Taniguchi, Y.; Iliffe, S.; Walters, K. Frailty as a predictor of Alzheimer disease, vascular dementia, and all dementia among community-dwelling older people: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2016, 17, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G. Frailty as a predictor of disabilities among community-dwelling older people: A systematic review and meta-analysis. Disabil. Rehabil. 2017, 39, 1897–1908. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G.; Iliffe, S.; Jivraj, S.; Walters, K. Association between frailty and quality of life among community-dwelling older people: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 716–721. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Walters, K. Frailty index as a predictor of mortality: A systematic review and meta-analysis. Age Ageing 2018, 47, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Roe, L.; Normand, C.; Wren, M.-A.; Browne, J.; O’Halloran, A.M. The impact of frailty on healthcare utilisation in Ireland: Evidence from the Irish longitudinal study on ageing. BMC Geriatr. 2017, 17, 203. [Google Scholar] [CrossRef] [Green Version]
- Salinas, A.; Manrique-Espinoza, B.; Heredia-Pi, I.B.; Rivera-Almaraz, A.; Avila-Funes, J.A. Healthcare costs of frailty: Implications for long-term care. J. Am. Med. Dir. Assoc. 2019, 20, 102–103.e2. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146-56. [Google Scholar] [CrossRef]
- Kojima, G. Frailty Defined by FRAIL Scale as a Predictor of Mortality: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2018, 19, 480–483. [Google Scholar] [CrossRef]
- Rockwood, K.; Theou, O. Using the Clinical Frailty Scale in Allocating Scarce Health Care Resources. Can. Geriatr. J. 2020, 23, 254–259. [Google Scholar] [CrossRef]
- Clegg, A.; Bates, C.; Young, J.; Ryan, R.; Nichols, L.; Ann Teale, E.; Mohammed, M.A.; Parry, J.; Marshall, T. Development and validation of an electronic frailty index using routine primary care electronic health record data. Age Ageing 2016, 45, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulok, M.H.; Theou, O.; van der Valk, A.; Rockwood, K. The role of illness acuity on the association between frailty and mortality in emergency department patients referred to internal medicine. Age Ageing 2020, 49, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G. Quick and simple FRAIL scale predicts incident activities of daily living (ADL) and instrumental ADL (IADL) disabilities: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2018, 19, 1063–1068. [Google Scholar] [CrossRef]
- Church, S.; Rogers, E.; Rockwood, K.; Theou, O. A scoping review of the Clinical Frailty Scale. BMC Geriatr. 2020, 20, 393. [Google Scholar] [CrossRef]
- Rivera-Almaraz, A.; Manrique-Espinoza, B.; Ávila-Funes, J.A.; Chatterji, S.; Naidoo, N.; Kowal, P.; Salinas-Rodríguez, A. Disability, quality of life and all-cause mortality in older Mexican adults: Association with multimorbidity and frailty. BMC Geriatr. 2018, 18, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagi, S.Z. Disability concepts revisited: Implications for prevention. In Disability in America: Toward a National Agenda for Prevention; Pope AMT, A.R., Ed.; National Academy Press: Washington, DC, USA, 1991; pp. 309–327. [Google Scholar]
- Jackson, C.A.; Jones, M.; Tooth, L.; Mishra, G.D.; Byles, J.; Dobson, A. Multimorbidity patterns are differentially associated with functional ability and decline in a longitudinal cohort of older women. Age Ageing 2015, 44, 810–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, P.; Ding, H.; Zhang, W.; Duan, G.; Yang, Y.; Chen, R.; Duan, Z.; Du, L.; Xie, C.; Jin, C.; et al. The association of multimorbidity and disability in a community-based sample of elderly aged 80 or older in Shanghai, China. BMC Geriatr. 2016, 16, 178. [Google Scholar] [CrossRef] [Green Version]
- Lu, F.P.; Chang, W.C.; Wu, S.C. Geriatric conditions, rather than multimorbidity, as predictors of disability and mortality among octogenarians: A population-based cohort study. Geriatr. Gerontol. Int. 2016, 16, 345–351. [Google Scholar] [CrossRef]
- Stenholm, S.; Westerlund, H.; Head, J.; Hyde, M.; Kawachi, I.; Pentti, J.; Kivimäki, M.; Vahtera, J. Comorbidity and functional trajectories from midlife to old age: The Health and Retirement Study. J. Gerontol. A Biol. Sci. Med. Sci.. 2015, 70, 332–338. [Google Scholar] [CrossRef] [Green Version]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.S.; Kuller, L.H.; Broudeau, R.; Kammerer, C.; de Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; et al. Health, Aging, and Body Composition Study. Accelerated loss of skeletal muscle strength in older adults with type 2 diabetes: The health, aging, and body composition study. Diabetes Care 2007, 30, 1507–1512. [Google Scholar] [CrossRef]
- Yoon, J.W.; Ha, Y.-C.; Kim, K.M.; Moon, J.H.; Choi, S.H.; Lim, S.; Park, Y.J.; Lim, J.Y.; Kim, K.W.; Park, K.S.; et al. Hyperglycemia is associated with impaired muscle quality in older men with diabetes: The Korean Longitudinal Study on Health and Aging. Diabetes Metab. J. 2016, 40, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, K.; Tabara, Y.; Ikegami, H.; Takata, Y.; Kamide, K.; Ikezoe, T.; Kiyoshige, E.; Makutani, Y.; Onuma, H.; Gondo, Y.; et al. Hyperglycemia in non-obese patients with type 2 diabetes is associated with low muscle mass: The Multicenter Study for Clarifying Evidence for Sarcopenia in Patients with Diabetes Mellitus. J. Diabetes Investig. 2019, 10, 1471–1479. [Google Scholar] [CrossRef] [Green Version]
- Park, S.W.; Goodpaster, B.H.; Lee, J.S.; Kuller, L.H.; Boudreau, R.; de Rekeneire, N.; Harris, T.B.; Kritchevsky, S.; Tylavsky, F.A.; Nevitt, M.; et al. Health, Aging, and Body Composition Study. Excessive loss of skeletal muscle mass in older adults with type 2 diabetes. Diabetes Care 2009, 32, 1993–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.-S.; Park, K.-S.; Kim, M.-J.; Kim, S.-K.; Cho, Y.-W.; Park, S.W. Type 2 diabetes is associated with low muscle mass in older adults. Geriatr. Gerontol. Int. 2014, 14 (Suppl. S1), 115–121. [Google Scholar] [CrossRef] [PubMed]
- Leenders, M.; Verdijk, L.; van der Hoeven, L.; Adam, J.J.; van Kranenburg, J.; Nilwik, R.; van Loon, L.J. Patients with type 2 diabetes show a greater decline in muscle mass, muscle strength, and functional capacity with aging. J. Am. Med. Dir. Assoc. 2013, 14, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Volpato, S.; Bianchi, L.; Lauretani, F.; Lauretani, F.; Bandinelli, S.; Guralnik, J.M.; Zuliani, G.; Ferrucci, L. Role of muscle mass and muscle quality in the association between diabetes and gait speed. Diabetes Care 2012, 35, 1672–1679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalyani, R.R.; Tra, Y.; Yeh, H.-C.; Egan, J.M.; Ferrucci, L.; Brancati, F.L. Quadriceps strength, quadriceps power, and gait speed in older U.S. adults with diabetes mellitus: Results from the National Health and Nutrition Examination Survey, 1999–2002. J. Am. Geriatr. Soc. 2013, 61, 769–775. [Google Scholar] [CrossRef]
- Chhetri, J.K.; Zheng, Z.; Xu, X.; Ma, C.; Chan, P. The prevalence and incidence of frailty in Pre-diabetic and diabetic community dwelling older population: Results from Beijing longitudinal study of aging II (BLSA-II). BMC Geriatr. 2017, 17, 47. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Freire, M.; de Cabo, R.; Studenski, S.A.; Eferrucci, L. The neuromuscular junction: Aging at the crossroad between nerves and muscle. Front Aging Neurosci. 2014, 6, 208. [Google Scholar] [CrossRef] [Green Version]
- Xie, W.; He, M.; Yu, D.; Wu, Y.; Wang, X.; Lv, S.; Xiao, W.; Li, Y. Mouse models of sarcopenia: Classification and evaluation. J. Cachexia Sarcopenia Muscle 2021, 12, 538–554. [Google Scholar] [CrossRef]
- Castrejón-Pérez, R.C.; Gutiérrez-Robledo, L.M.; Cesari, M.; Pérez-Zepeda, M.U. Diabetes mellitus, hypertension and frailty: A population-based, cross-sectional study of Mexican older adults. Geriatr. Gerontol. Int. 2017, 17, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lee, S.; Harada, K.; Bae, S.; Makizako, H.; Doi, T.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Park, H.; et al. Relationship between chronic kidney disease with diabetes or hypertension and frailty in community-dwelling Japanese older adults. Geriatr. Gerontol. Int. 2016, 17, 1527–1533. [Google Scholar] [CrossRef] [PubMed]
- Heikkala, E.; Mikkola, I.; Jokelainen, J.; Timonen, M.; Hagnäs, M. Multimorbidity and achievement of treatment goals among patients with type 2 diabetes: A primary care, real-world study. BMC Health Serv. Res. 2021, 21, 964. [Google Scholar] [CrossRef] [PubMed]
- Umeh, K. Self-rated health and multimorbidity in patients with type 2 diabetes. J. Health Psychol. 2021, 27, 1659–1678. [Google Scholar] [CrossRef] [PubMed]
- McClellan, S.P.; Haque, K.; García-Peña, C. Diabetes multimorbidity combinations and disability in the Mexican Health and Aging Study, 2012–2015. Arch. Gerontol. Geriatr. 2021, 93, 104292. [Google Scholar] [CrossRef]
- Coles, B.; Zaccardi, F.; Hvid, C.; Davies, M.J.; Khunti, K. Cardiovascular events and mortality in people with type 2 diabetes and multimorbidity: A real-world study of patients followed for up to 19 years. Diabetes Obes. Metab. 2021, 23, 218–227. [Google Scholar] [CrossRef]
- Chiang, J.I.; Hanlon, P.; Li, T.-C.; Jani, B.D.; Manski-Nankervis, J.-A.; Furler, J.; Lin, C.-C.; Yang, S.-Y.; Nicholl, B.I.; Thuraisingam, S.; et al. Multimorbidity, mortality, and HbA1c in type 2 diabetes: A cohort study with UK and Taiwanese cohorts. PLoS Med. 2020, 7, e1003094. [Google Scholar] [CrossRef]
- McCoy, R.G.; Lipska, K.J.; Van Houten, H.K.; Shah, N.D. Association of Cumulative Multimorbidity, Glycemic Control, and Medication Use With Hypoglycemia-Related Emergency Department Visits and Hospitalizations Among Adults With Diabetes. JAMA Netw. Open 2020, 3, e1919099. [Google Scholar] [CrossRef]
- McCoy, R.G.; Lipska, K.J.; Van Houten, H.K.; Shah, N.D. Paradox of glycemic management: Multimorbidity, glycemic control, and high-risk medication use among adults with diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001007. [Google Scholar] [CrossRef] [Green Version]
- Chiang, J.I.; Furler, J.; Mair, F.; Jani, B.D.; I Nicholl, B.; Thuraisingam, S.; Manski-Nankervis, J.-A. Associations between multimorbidity and glycaemia (HbA1c) in people with type 2 diabetes: Cross-sectional study in Australian general practice. BMJ Open 2020, 10, e039625. [Google Scholar] [CrossRef]
- Wong, E.L.Y.; Xu, R.H.; Cheung, A.W.L. Measurement of health-related quality of life in patients with diabetes mellitus using EQ-5D-5L in Hong Kong, China. Qual. Life Res. 2020, 29, 1913–1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerrero Fernández de Alba, I.; Gimeno-Miguel, A.; Poblador-Plou, B.; Gimeno-Feliu, L.A.; Ioakeim-Skoufa, I.; Rojo-Martínez, G.; Forjaz, M.J.; Prados-Torres, A. Association between mental health comorbidity and health outcomes in type 2 diabetes mellitus patients. Sci. Rep. 2020, 10, 19583. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.I.; Manski-Nankervis, J.-A.; Thuraisingam, S.; Jenkins, A.; O’Neal, D.; Mair, F.S.; Jani, B.D.; Nicholl, B.I.; Furler, J. Multimorbidity, glycaemic variability and time in target range in people with type 2 diabetes: A baseline analysis of the GP-OSMOTIC trial. Diabetes Res. Clin. Pract. 2020, 169, 108451. [Google Scholar] [CrossRef] [PubMed]
- Quiñones, A.R.; Markwardt, S.; Botoseneanu, A. Diabetes-Multimorbidity Combinations and Disability Among Middle-aged and Older Adults. J. Gen. Intern. Med. 2019, 34, 944–951. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, P.; Jani, B.D.; Butterly, E.; Nicholl, B.; Lewsey, J.; McAllister, D.A.; Mair, F.S. An analysis of frailty and multimorbidity in 20,566 UK Biobank participants with type 2 diabetes. Commun Med. 2021, 1, 28. [Google Scholar] [CrossRef]
- Espeland, M.A.; Justice, J.N.; Bahnson, J.; Evans, J.K.; Munshi, M.; Hayden, K.M.; Simpson, F.R.; Johnson, K.C.; Johnston, C.; Kritchevsky, S.R. Look AHEAD Research Group. Eight Year Changes in Multimorbidity and Frailty in Adults with Type 2 Diabetes Mellitus: Associations with Cognitive and Physical Function and Mortality. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 77, glab342. [Google Scholar] [CrossRef]
- Nguyen, T.N.; Harris, K.; Woodward, M.; Chalmers, J.; Cooper, M.; Hamet, P.; Harrap, S.; Heller, S.; MacMahon, S.; Mancia, G.; et al. The Impact of Frailty on the Effectiveness and Safety of Intensive Glucose Control and Blood Pressure-Lowering Therapy for People With Type 2 Diabetes: Results From the ADVANCE Trial. Diabetes Care 2021, 44, 1622–1629. [Google Scholar] [CrossRef]
- Sable-Morita, S.; Tanikawa, T.; Satake, S.; Okura, M.; Tokuda, H.; Arai, H. Microvascular complications and frailty can predict adverse outcomes in older patients with diabetes. Geriatr. Gerontol. Int. 2021, 21, 359–363. [Google Scholar] [CrossRef]
- Ferri-Guerra, J.; Aparicio-Ugarriza, R.; Salguero, D.; Baskaran, D.; Mohammed, Y.N.; Florez, H.; Ruiz, J.G. The Association of Frailty with Hospitalizations and Mortality among Community Dwelling Older Adults with Diabetes. J. Frailty Aging 2020, 9, 94–100. [Google Scholar] [CrossRef]
- Gual, M.; Formiga, F.; Ariza-Solé, A.; López-Palop, R.; Sanchís, J.; Marín, F.; Vidán, M.T.; Martínez-Sellés, M.; Sionis, A.; Lorente, V.; et al. LONGEVO-SCA registry investigators. Diabetes mellitus, frailty and prognosis in very elderly patients with acute coronary syndromes. Aging Clin. Exp. Res. 2019, 31, 1635–1643. [Google Scholar] [CrossRef]
- Chao, C.-T.; Wang, J.; Huang, J.-W.; Chan, D.-C.; Chien, K.-L. Frailty Predicts an Increased Risk of End-Stage Renal Disease with Risk Competition by Mortality among 165,461 Diabetic Kidney Disease Patients. Aging Dis. 2019, 10, 1270–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitamura, A.; Taniguchi, Y.; Seino, S.; Yokoyama, Y.; Amano, H.; Fujiwara, Y.; Shinkai, S. Combined effect of diabetes and frailty on mortality and incident disability in older Japanese adults. Geriatr. Gerontol. Int. 2019, 19, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Perez, S.I.A.; Senior, P.A.; Field, C.J.; Jindal, K.; Mager, D.R. Frailty, Health-Related Quality of Life, Cognition, Depression, Vitamin D and Health-Care Utilization in an Ambulatory Adult Population With Type 1 or Type 2 Diabetes Mellitus and Chronic Kidney Disease: A Cross-Sectional Analysis. Can. J. Diabetes 2019, 43, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.T.; Wang, J.; Chien, K.L.; COhort of GEriatric Nephrology in NTUH (COGENT) study group. Both pre-frailty and frailty increase healthcare utilization and adverse health outcomes in patients with type 2 diabetes mellitus. Cardiovasc. Diabetol. 2018, 17, 130. [Google Scholar] [CrossRef] [PubMed]
- Thein, F.S.; Li, Y.; Nyunt, M.S.Z.; Gao, Q.; Wee, S.L.; Ng, T.P. Physical frailty and cognitive impairment is associated with diabetes and adversely impact functional status and mortality. Postgrad. Med. 2018, 130, 561–567. [Google Scholar] [CrossRef]
- Li, C.L.; Stanaway, F.F.; Lin, J.D.; Chang, H.-Y. Frailty and health care use among community-dwelling older adults with diabetes: A population-based study. Clin. Interv. Aging 2018, 13, 2295–2300. [Google Scholar] [CrossRef] [Green Version]
- Cicek, M.; Buckley, J.; Pearson-Stuttard, J.; Gregg, E.W. Characterizing Multimorbidity from Type 2 Diabetes: Insights from Clustering Approaches. Endocrinol. Metab. Clin. N. Am. 2021, 50, 531–558. [Google Scholar] [CrossRef]
- Gao, F.; Chen, J.; Liu, X.; Wang, X.; Zhao, H.; Han, D.; Jing, X.; Liu, Y.; Cui, Z.; Li, C.; et al. Latent class analysis suggests four classes of persons with type 2 diabetes mellitus based on complications and comorbidities in Tian- jin, China: A cross-sectional analysis. Endocr. J. 2017, 64, 1007–1016. [Google Scholar] [CrossRef] [Green Version]
- Nowakowska, M.; Zghebi, S.S.; Ashcroft, D.M.; Buchan, I.; Chew-Graham, C.; Holt, T.; Mallen, C.; Van Marwijk, H.; Peek, N.; Perera-Salazar, R.; et al. The comorbidity burden of type 2 diabetes mellitus: Patterns, clusters and predictions from a large English primary care cohort. BMC Med. 2019, 17, 145. [Google Scholar] [CrossRef] [Green Version]
- Seng, J.J.B.; Kwan, Y.H.; Lee, V.S.Y.; Tan, C.S.; Zainudin, S.B.; Thumboo, J.; Low, L.L. Differential health care use, diabetes-related complications, and mortality among five unique classes of patients with type 2 diabetes in Singapore: A latent class analysis of 71,125 patients. Diabetes Care 2020, 43, 1048–1056. [Google Scholar] [CrossRef]
- Stirland, L.E.; González-Saavedra, L.; Mullin, D.S.; Ritchie, C.W.; Muniz-Terrera, G.; Russ, T.C. Measuring multimorbidity beyond counting diseases: Systematic review of community and population studies and guide to index choice. BMJ 2020, 368, m160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, J.I.; Jani, B.D.; Mair, F.S.; Nicholl, B.I.; Furler, J.; O’Neal, D.; Jenkins, A.; Condron, P.; Manski-Nankervis, J.-A. Associations between multimorbidity, all-cause mortality and glycaemia in people with type 2 diabetes: A systematic review. PLoS ONE. 2018, 13, e0209585. [Google Scholar] [CrossRef] [PubMed]
- Abdelhafiz, A.H.; Sinclair, A.J. Metabolic phenotypes explain the relationship between dysglycaemia and frailty in older people with type 2 diabetes. J. Diabetes Complicat. 2022, 36, 108144. [Google Scholar] [CrossRef]
- Zghebi, S.S.; Steinke, D.T.; Rutter, M.K.; Ashcroft, D.M. Eleven-year multimorbidity burden among 637 255 people with and without type 2 diabetes: A population-based study using primary care and linked hospitalisation data. BMJ Open 2020, 10, e033866. [Google Scholar] [CrossRef] [PubMed]
- Roland, M.; Paddison, C. Better management of patients with multimorbidity. BMJ 2013, 346, f2510. [Google Scholar] [CrossRef]
- Aga, F.; Dunbar, S.B.; Kebede, T.; A Gary, R. The role of concordant and discordant comorbidities on performance of self-care behaviors in adults with type 2 diabetes: A systematic review. Diabetes Metab. Syndr. Obes. 2019, 12, 333–356. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.S.; Weiss, C.O.; Xue, Q.-L.; Fried, L.P. Association between inflammatory-related disease burden and frailty: Results from the Women’s Health and Aging Studies (WHAS) I and II. Arch. Gerontol. Geriatr. 2012, 54, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Hadley, E.C.; Walston, J.D.; Newman, A.B.; Guralnik, J.M.; Studenski, S.; Harris, T.B.; Ershler, W.B.; Ferrucci, L. From bedside to bench: Research agenda for frailty. Sci. Aging Knowl. Env. 2005, 2005, pe24. [Google Scholar] [CrossRef]
- Andreadi, A.; Bellia, A.; Di Daniele, N.; Meloni, M.; Lauro, R.; Della-Morte, D.; Lauro, D. The molecular link between oxidative stress, insulin resistance, and type 2 diabetes: A target for new therapies against cardiovascular diseases. Curr. Opin. Pharmacol. 2022, 62, 85–96. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Multimorbidity | ||||
| Index | Items | Weights | Score | Population and Advantages |
| CCI | 19 conditions. | Range: RR 1.2–1.5 for 0 conditions to RR > 6.0 for 6 conditions. | Sum of weights. | Mixed populations including elderly, care home residents and cancer patients. Correlates with mortality, disability, readmissions and length of hospital stay. |
| CIRS | 13 body systems | Ranges from 0 for no impairment to 4 for life threatening impairment. | Sum of weights. | Mixed populations including elderly, care home residents and cancer patients. Correlates with ADL, IADL and age. |
| ICED | ICED-DS 14 disease categories ICED-FS 10 functional categories. | ICED-DS 1–5. ICED-FS 1–3. | 1–4 | Care home residents and those with hip replacement. Predicts mortality and disability. |
| KI | Vascular or non-vascular diseases. | Ranges from 0 for no or easy to control to 3 for full decompensated disease. | According to the most severe condition. | Diabetes mellitus and breast cancer. Has a mortality predictive validity. |
| Incalzi | 52 conditions. | Based on RR of mortality. | Sum of weights, adding points for every decade above age of 75 years. | Mixed populations including elderly. Has predictive validity for mortality. |
| Frailty | ||||
| Tool | Criteria | Advantages | ||
| Fried criteria | 5-point scale: weight loss, exhaustion, weakness assessed by grip strength, reduced physical activity and slowness measured by gait speed. | Identifies robust (score 0), pre-frail (score 1–2) and frail (score >3) individuals but requires two practical measurements. | ||
| FRAIL scale | 5-point scale: fatigue, resistance, ambulation, illness and loss of weight. | Can be self-assessed and does not require measurements by healthcare professionals. | ||
| CFS | 9-point scale that describes patient’s functional characteristics and categorise them from very fit to severely frail. | Uses clinical descriptors and pictographs to stratify older people according to level of function to predict mortality or institutionalisation. | ||
| eFI | Uses the cumulative deficit model to identify and score frailty based on routine interactions of patients with their general practitioner. | Can be used to screen for the whole practice population who are >65 years old. | ||
| 35-Items Rockwood frailty index | 35 items, based on data from chronic diseases, disabilities in activities of daily living, cognition, nutrition, visual and hearing impairment. | Includes comprehensive data as a part of comprehensive geriatric assessment. | ||
| Study | Patients | Aim to | Main Findings |
|---|---|---|---|
| Heikkala E et al., cross-sectional, Finland, 2021 [64]. | 4545 subjects with type 2 DM, mean (SD) age 70.9 (12.3) Y. | Investigate associations of multimorbidity and treatment goals, HbA1c, LDL cholesterol and SBP. | A. 93% of subjects had general, 21% concordant, 8 % discordant and 64% both multimorbidities, respectively. B. General multimorbidity, concordant multimorbidity and discordant multimorbidity significantly associated with achievement of HbA1c target (OR 1.32, 95% CI 1.01 to 1.70, 1.47, 1.10 to 1.95 and 1.32, 1.01 to 1.72, respectively). C. Similar findings with attainment of LDL target (1.34, 1.03 to 1.74, 1.33, 1.00 to 1.78 and 1.36, 1.05 to 1.78, respectively). |
| Umeh K, cross sectional, UK, 2021 [65]. | 280 subjects with type 2 DM, median age 65–74 Y. | Examine self-rated health related to multimorbidity, glycaemia and BMI. | Odds of ‘fair/bad/very bad’ increased 10-fold in patients with 3 conditions (OR 10.11, 95% CI 3.36 to 30.40) and 4 conditions (10.58, 2.9 to 38.25) irrespective of glycaemic control (p < 0.001). |
| McClellan SP et al., prospective cohort, Mexico, 2021 [66]. | Total 2558 subjects with DM, 1997 with and 561 without morbidities. | Investigate relationship of combinations of morbidities and disability. | A. Top 3 combinations were diabetes-hypertension (31.9%), diabetes-hypertension-depression (19.4%) and diabetes-depression (10.6%). B. DM-hypertension-depression (IRR 2.44, CI 1.65 to 3.60), DM-depression (2.37, 1.34 to 4.21) and DM-hypertension-arthritis-depression (3.74, 2.08 to 6.73) associated with higher ADL-IADL scores. |
| Coles B et al., retrospective, UK, 2021. [67] | Total 120,409 subjects with type 2 DM, mean (SD) age 63.5 (13.4) Y. | Quantify risk of CVD events, all-cause mortality and CV mortality in DM and multimorbidity. | A. Compared with DM only, ≥4 morbidities increased risk of CV events (HR 2.57, 95% CI 2.45 to 2.69), all-cause mortality (1.73, 1.68 to 1.78) and CV mortality (2.68, 2.52 to 2.85). B. Compared with no CVD morbidity, ≥2 morbidities increased risk of CV events (2.42, 2.35 to 2.49), all-cause mortality (1.44, 1.42 to 1.47) and CV mortality (2.44, 2.35 to 2.54). |
| Chiang JI et al., longitudinal cohort, UK-China, 2020 [68]. | UK Biobank, 20,569 subjects, mean (SD) age 60.2 (6.8) Y, Taiwan NDCMP 59,657 subjects, mean (SD) age 60.8 (11.3) Y. | Explore associations of multimorbidity with baseline HbA1c and all-cause mortality in type 2 DM. | Increasing total and discordant multimorbidity were associated with lower HbA1c and increased mortality in both datasets. A. In UK Biobank, HRs (95% CI) for all-cause mortality in people with 1, 2, 3 and 4 morbidities compared with no morbidities were 1.20 (0.91 to 1.56), 1.75 (1.35 to 2.27), 2.17 (1.67 to 2.81) and 3.14 (2.43 to 4.03), all p < 0.001. B. HRs for mortality in Taiwan NDCMP were similar. C. Largest effect size on mortality was CHD and HF in UK Biobank (HR 4.37, 95% CI 3.59 to 5.32) p < 0.001, and painful conditions and alcohol in Taiwan NDCMP (4.02, 3.08 to 5.23) p < 0.001. |
| McCoy RG et al., cohort, US, 2020 [69]. | 201,705 subjects with DM, mean (SD) age, 65.8 (12.1) Y. | Examine associations of multimorbidity and other factors with hypoglycaemia-related ED visits and hospitalisations. | Risk of hypoglycaemia-related ED visits and hospitalisations increased by number of comorbidities (IRR of 1.66, 95% CI 1.42 to 1.95) in the presence of 2 comorbidities to IRR of 4.12, 3.07 to 5.51 with ≥8 comorbidities compared with ≤1 morbidity. |
| McCoy RG et al., retrospective, US, 2020 [70]. | 194,157 patients with type 2 DM, mean (SD) age 66.2 (11.7) Y. | Examine impact of DM-concordant, discordant and advanced morbidities on HbA1c. | A. 45.2% patients had DM-concordant, 2.7% discordant, 30.6% both morbidities and 13.0% had ≥1 advanced morbidities. B. Mean (SD) HbA1c was highest in patients with no comorbidities, 7.4% (1.7), slightly lower in those with concordant, 7.3% (1.5), much lower in those with discordant, 7.1% (1.5), both, 7.1% (1.4) and advanced comorbidities, 7.0 (1.3). C. In patients with discordant comorbidities, HbA1c declined as number of comorbidities increased, 7.1% (1.6) with 1 to 6.6% (1.2) with ≥3 morbidities. |
| Chiang JI et al., cross sectional, Australia, 2020 [71]. | 69,718 subjects with type 2 DM, mean (SD) age 66.42 (12.70) Y. | Explore prevalence of multimorbidity and its association with HbA1c. | A. >90% of participants had multimorbidity, 83.4% discordant and 69.9% concordant conditions. B. Top 3 discordant were painful diseases (55.4%), dyspepsia (31.6%), depression (22.8%) and concordant were hypertension (61.4%), CHD (17.1%) and CKD (8.5%). C. No association of multimorbidity and HbA1c. |
| Wong FLY et al., cross sectional, China, 2020 [72]. | 2326 patients with DM, 60% aged ≥65 Y. | Estimate health scores by sociodemographics. | Patients with ≥3 morbidities are more likely to show a lower health-related quality of life scores than those with DM alone. |
| Guerrero Fernández de Alba I et al., retrospective, Spain, 2020 [73] | 63,365 subjects with type 2 DM, mean (SD) age 69.9 (12.1) Y. | Study mental health comorbidity prevalence and its association with outcomes. | Mental health multimorbidity prevalent in 19% of subjects and increased mortality risk (OR 1.24, 95% CI 1.16 to 1.31), all-cause hospitalisation (1.16, 1.10 to 1.23), DM-related hospitalisation (1.51, 1.18 to 1.93) and emergency room visits (1.26, 1.21 to 1.32). |
| Chiang JI et al., cross-sectional, Australia, 2020 [74]. | 279 subjects with type 2 DM, mean (SD) age 60.4 (9.9) Y. | Explore associations of multimorbidity and HbA1c, GV and TIR. | A. 89.2% of subjects had multimorbidity. B. Most prevalent was hypertension (57.4%), painful conditions (29.8%), CHD (22.6%) and depression (19.0%). C. Multimorbidity was not associated with HbA1c, GV or TIR. |
| Quiñones, AR et al., prospective cohort, US, 2019 [75]. | 3841 subjects with DM, mean (SD) age 68.1 (9.5) Y. | Identify multimorbidity combinations and their association with poor functional status. | Depressive symptoms or stroke, added to DM-multimorbidity combinations associated with higher ADL-IADL limitations: A. DM-arthritis-hypertension-depressive symptoms vs. DM-arthritis-hypertension: IRR 1.95, 95% CI 1.13 to 3.38). B. DM-arthritis-hypertension-stroke vs. DM-arthritis-hypertension: (2.09, 1.15 to 3.82). |
| Study | Patients | Aim to | Main Findings |
|---|---|---|---|
| Hanlon P et al., longitudinal cohort, UK, 2021 [76]. | UK Biobank, 20,566 with type 2 DM aged 40–72 Y. | Assess implications of frailty/multimorbidity in middle/older-aged people with type 2 DM using 2 morbidity and 2 frailty measures. | A. 42% of participants were frail or multimorbid by at least one measure, 2.2% by all four measures. B. Each measure was associated with mortality, MACE, hypoglycaemia, fall or fracture. C. Mortality risk was higher in older vs. younger participants with a given level of frailty (1.9%, and 9.9% in men aged 45 and 65, respectively or multimorbidity (1.3% and 7.8% in men with 4 morbidities aged 45 and 65, respectively). |
| Espeland MA et al., prospective, US, 2021 [77]. | 3842 subjects with type 2 DM aged 45–76 Y at baseline, F/U 8 Y. | Examine effect of multimorbidity and frailty on cognition, physical function and mortality. | Increases in both multimorbidity and frailty index were associated with poor composite cognitive function and 400 m walk speed and increased risk for death (all p < 0.001). |
| Nguyen Tu N et al., retrospective, multicentre, 2021 [78]. | 11,140 subjects with type 2 DM, mean (SD) age, 65.78 (6.39) Y. | Explore effect of frailty on intensive glycaemic and blood pressure control. | A. Frailty increased risk of combined macro- and microvascular events (HR 1.03, 95% CI 0.90 to 1.19, p = 0.02) and all-cause mortality (1.11, 0.92 to 1.34). B. Severe hypoglycaemia was higher in frail, 8.39 (6.15 to 10.63) vs. 4.80 (3.84 to 5.76) in non-frail (p < 0.001). C. No significant difference in discontinuation of BP treatment due to hypotension/dizziness between frail and non-frail. |
| Sable-Morita S et al., retrospective, Japan, 2021 [79]. | 477 subjects with DM, mean (SD) age 74.2 (6.2) Y. | Assess whether frailty and DM-related factors could predict occurrence of adverse events. | Microvascular complications and frailty were significant predictors of adverse event incidence, respective OR (95% CI) 1.403 (1.11 to 1.78) per additional complication, 2.419 (1.33 to 4.40) for frailty; both p < 0.05). |
| Ferri-Guerra J et al., retrospective, US, 2020 [80]. | 763 subjects with DM, mean (SD) age 72.9 (6.8) Y. | Determine association of frailty with all-cause hospitalisations and mortality. | Frailty was associated with higher all-cause hospitalisations, HR 1.71 (95% CI 1.31 to 2.24), p < 0.0001 and greater mortality, 2.05, 1.16 to 3.64), p = 0.014. |
| Gual M et al., prospective, Spain, 2019 [81]. | Total 532 subjects with ACS, 212 with DM, mean (SD) age 83.7 (5.0) Y. | Evaluate impact of DM on mortality or 6-month readmission according to frailty status. | Association of DM and incidence of clinical outcomes was significant only in patients with established frailty (HR 1.72, 1.05 to 2.81) compared to non-frail patients. |
| Chao CT et al., retrospective, Taiwan, 2019 [82]. | 165,461subjects with DKD, aged >20 Y. | Examine effect of frailty on DKD progression to ESRD, mortality, and adverse episodes. | A. Subjects with 1, 2, and ≥3 on FRAIL scale had increased risks of ESRD and mortality HRs 1.13, 1.18, and 1.2 and 1.25, 1.41, and 1.34, respectively. B. frailty increased risk of CV events and ICU admission in a dose response-manner. |
| Kitamura A et al., prospective, Japan, 2019 [83]. | 1271 subjects, 174 with DM, mean (SD) age 71.0 (5.6) Y, F/U 8.1 Y. | Clarify risks of death and disability in diabetes, frailty, both or neither. | A. Compared with non-frail subjects without diabetes, those with diabetes and frailty had higher risks of mortality, HR 5.0, 95% CI 2.4 to 10.3) and incident disability (3.9, 2.1 to 7.3). B. Non-frail with diabetes did not have a significant increased risk of mortality, but a tendency for disability compared with non-frail without diabetes. |
| Adame Perez SI et al., cross-sectional, Canada, 2019 [84]. | 41 subjects with DM and CKD, median (range) age 70 (65–74) Y. | Compare differences in body composition, HRQoL, mental health, cognition and vitD status with health-care utilization by frail and non-frail. | Frail, compared with non-frail, subjects had lower lean body mass, lower HRQoL scores, more depression (p = <0.05) and higher numbers of health visits (p < 0.05). No differences in health-care visit types or vitD status were noted between frail and non-frail participants. |
| Chao CT et al., longitudinal cohort, Taiwan, 2018 [85]. | 560,795 subjects with type 2 DM, mean (SD) age 56.4 (13.8) Y, 3.14 Y F/U. | Examine frailty impact on long-term mortality, CV risk, all-cause hospitalisation, and ICU admission. | Pre-frailty (1, 2 FRAIL scale) and frailty (≥3) increased risk of: A. Mortality, HR 1.05, 1.13, and 1.25 (95% CI 1.02 to 1.07, 1.08 to 1.17 and 1.15 to 1.36, respectively). B. CV events, 1.05, 1.15, and 1.13 (1.02 to 1.07, 1.1 to 1.2 and 1.01 to 1.25, respectively). C. Hospitalisation, 1.06, 1.16, and 1.25 (1.05 to 1.07, 1.14 to 1.19, and 1.18 to 1.33, respectively). D. ICU admission, 1.05, 1.13, and 1.17 (1.03 to 1.07, 1.08 to 1.14, and 1.06 to 1.28, respectively) compared to non-frail. |
| Thein FS et al., prospective, Singapore, 2018 [86]. | 2696 subjects, 486 with DM, mean (SD) age 67.3 (7.5) Y. | Investigate effect of frailty and cognitive impairment on functional and mortality outcomes. | A. Frailty associated with higher prevalence of IADL disability, OR 6.72, 95% CI 1.84 to 24.5. B. Frailty and cognitive impairment associated with highest prevalence of IADL (17.8, 3.66 to 8.68) and ADL disabilities (93.8, 23.6 to 372.4). C. Cognitive impairment (HR 2.72, 95% CI 1.48 to 5.01), frailty (4.30, 1.88 to 9.82) and cognitive impairment with frailty (8.41, 3.95 to 17.9) associated with mortality. |
| Li CL et al., cross-sectional, Taiwan, 2018 [87]. | 3203 subjects, 719 with DM, aged ≥ 65 Y. | Investigate prevalence of frailty and its relationship with health care. | A. Frailty, but not pre-frailty, significantly associated with hospitalisation, OR 5.31, 95% CI 1.87 to 15.10). B. Pre-frail and frail significantly associated with emergency department visits (2.64, 1.35 to 5.17 and 4.05, 1.31 to 12.49, respectively). |
| Multimorbidity | Frailty |
|---|---|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinclair, A.J.; Abdelhafiz, A.H. Multimorbidity, Frailty and Diabetes in Older People–Identifying Interrelationships and Outcomes. J. Pers. Med. 2022, 12, 1911. https://doi.org/10.3390/jpm12111911
Sinclair AJ, Abdelhafiz AH. Multimorbidity, Frailty and Diabetes in Older People–Identifying Interrelationships and Outcomes. Journal of Personalized Medicine. 2022; 12(11):1911. https://doi.org/10.3390/jpm12111911
Chicago/Turabian StyleSinclair, Alan J., and Ahmed H. Abdelhafiz. 2022. "Multimorbidity, Frailty and Diabetes in Older People–Identifying Interrelationships and Outcomes" Journal of Personalized Medicine 12, no. 11: 1911. https://doi.org/10.3390/jpm12111911