
Predicting Intention to Participate in Community Physical Activities for Adults with Physical Disabilities
 ,
,
Abstract
:
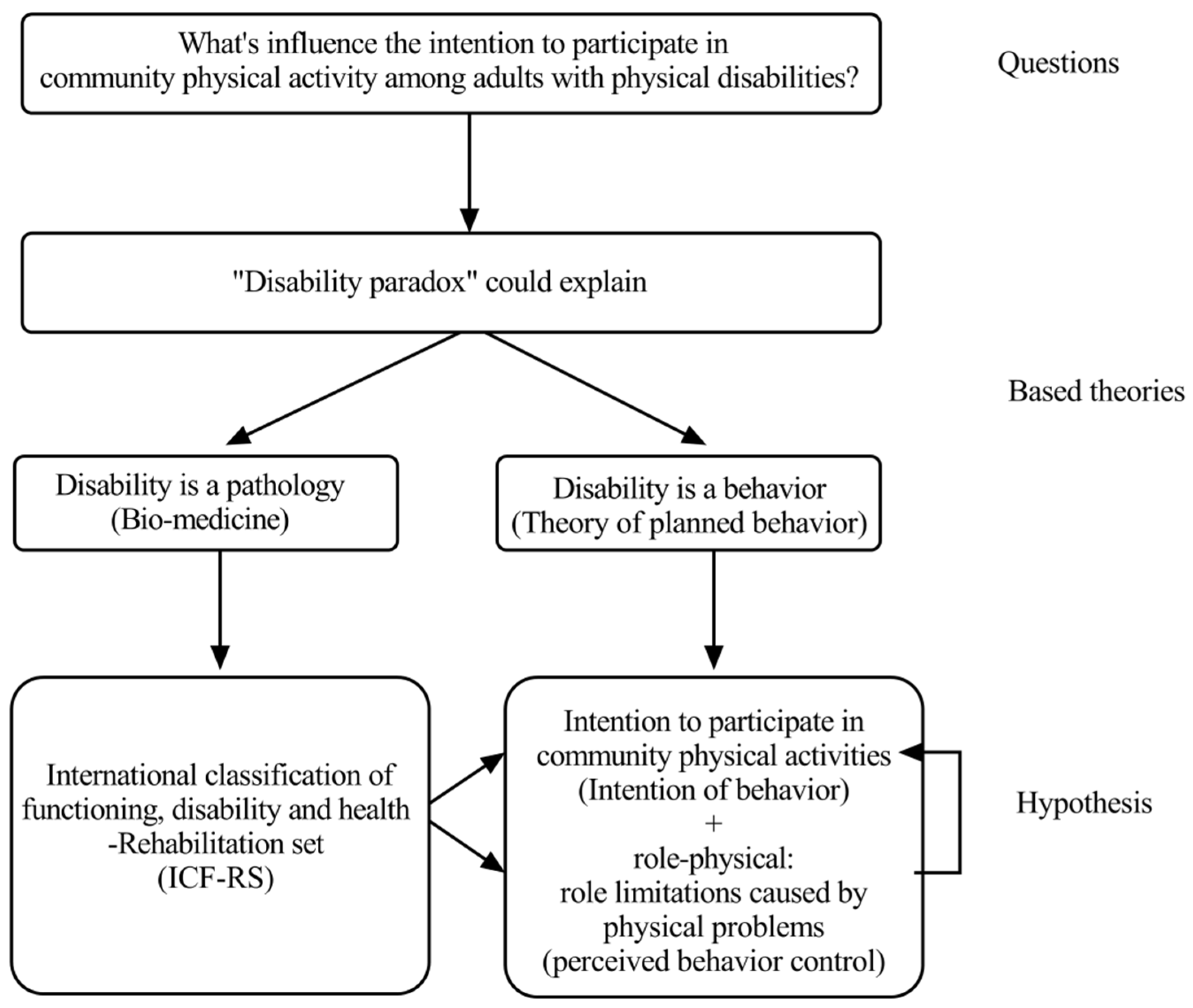
1. Introduction
2. Materials and Methods
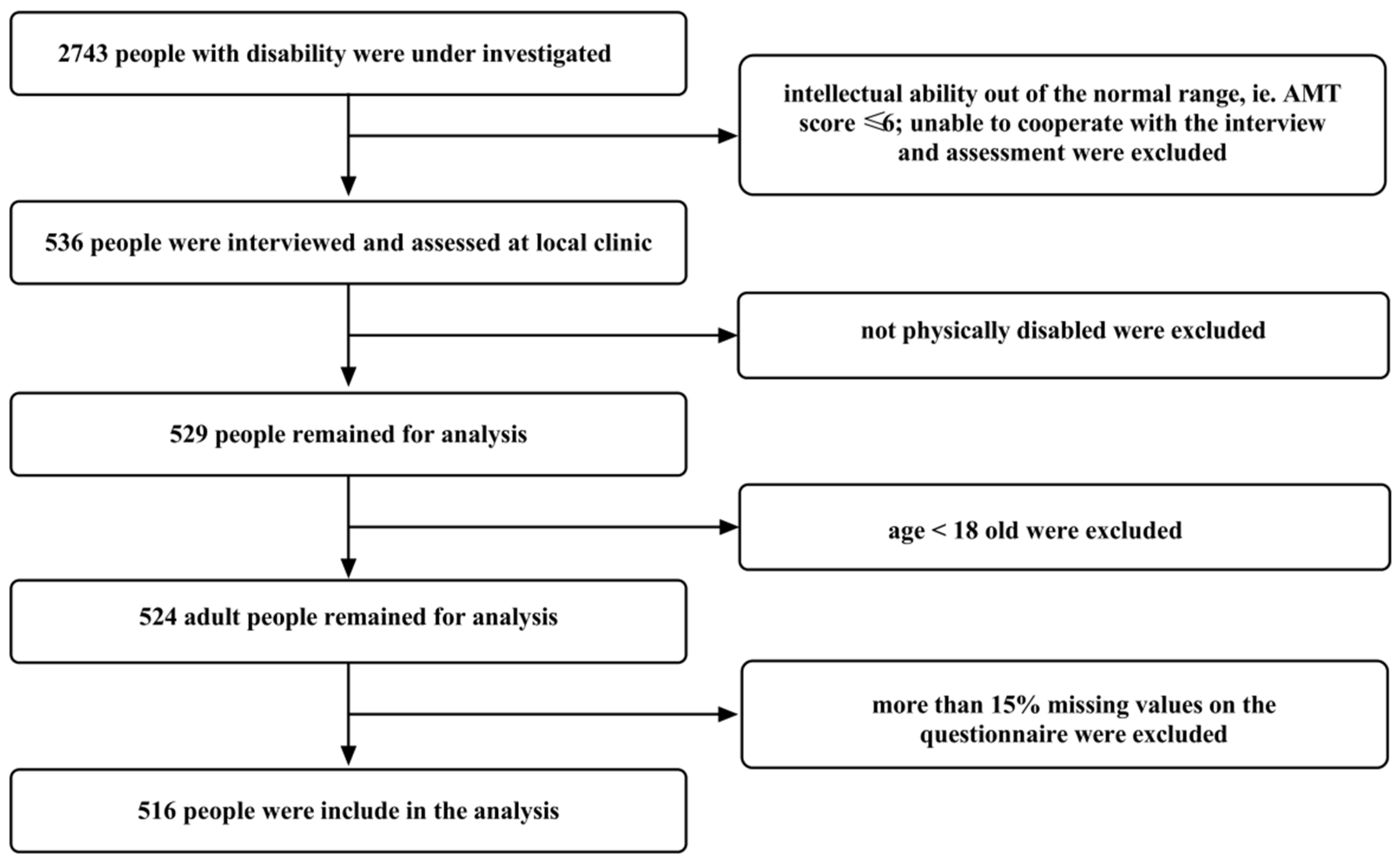
2.1. Participants
2.2. Instrument Scaling
2.3. Statistical Analyses
3. Results
3.1. Exploratory Factor Analysis
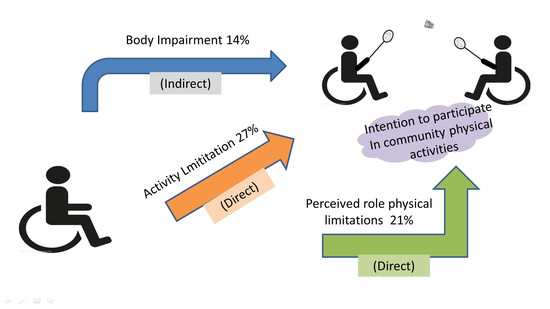
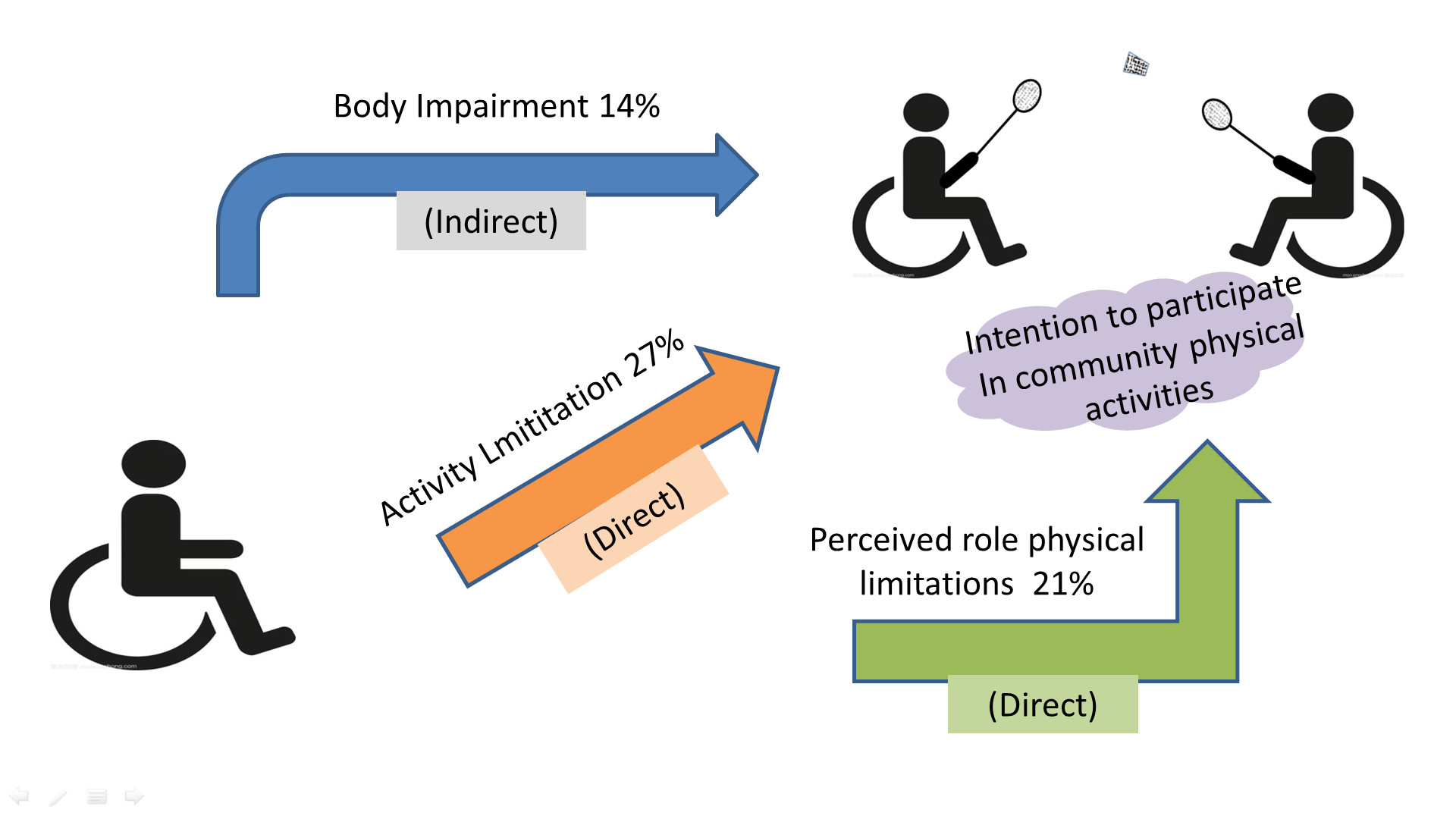
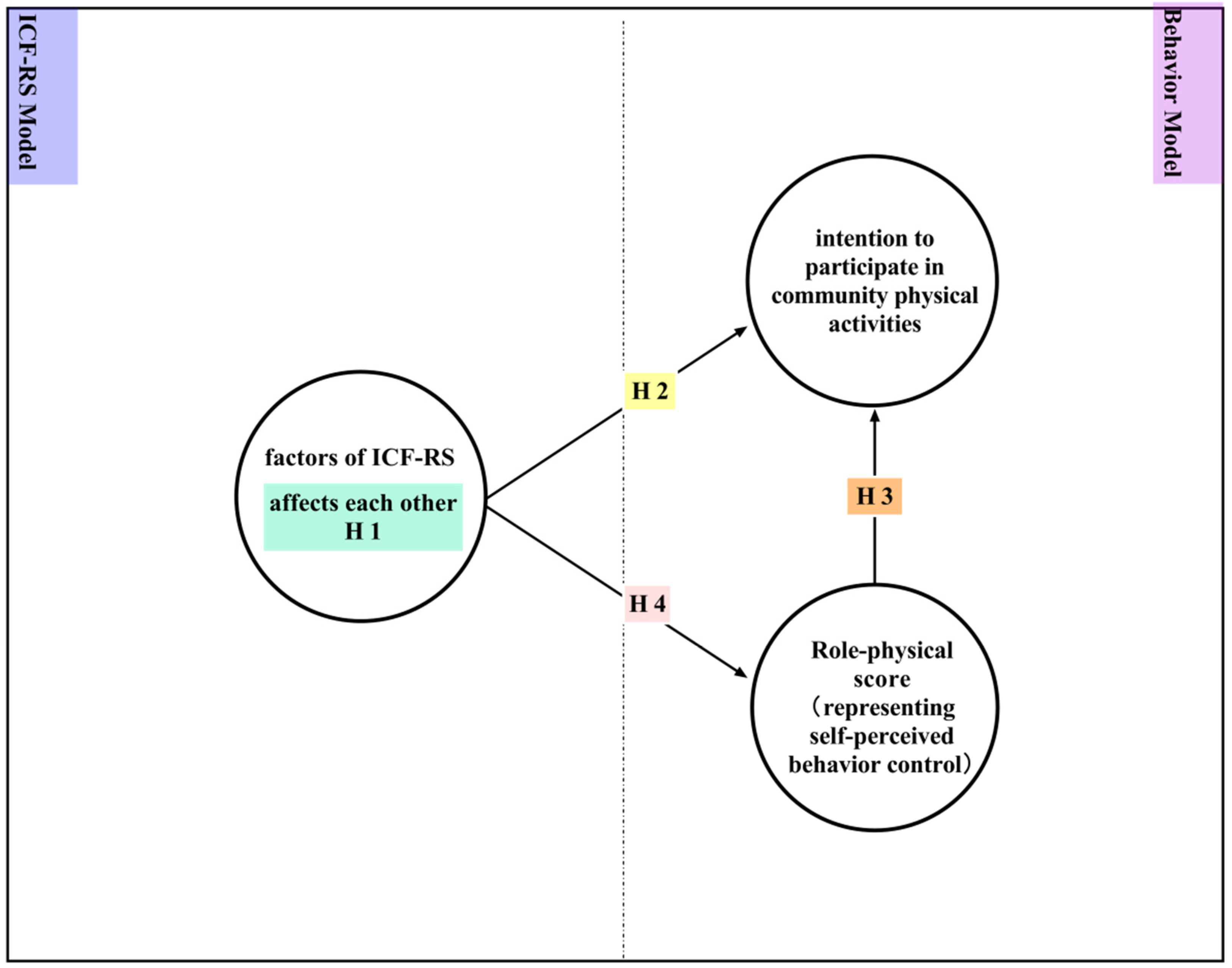
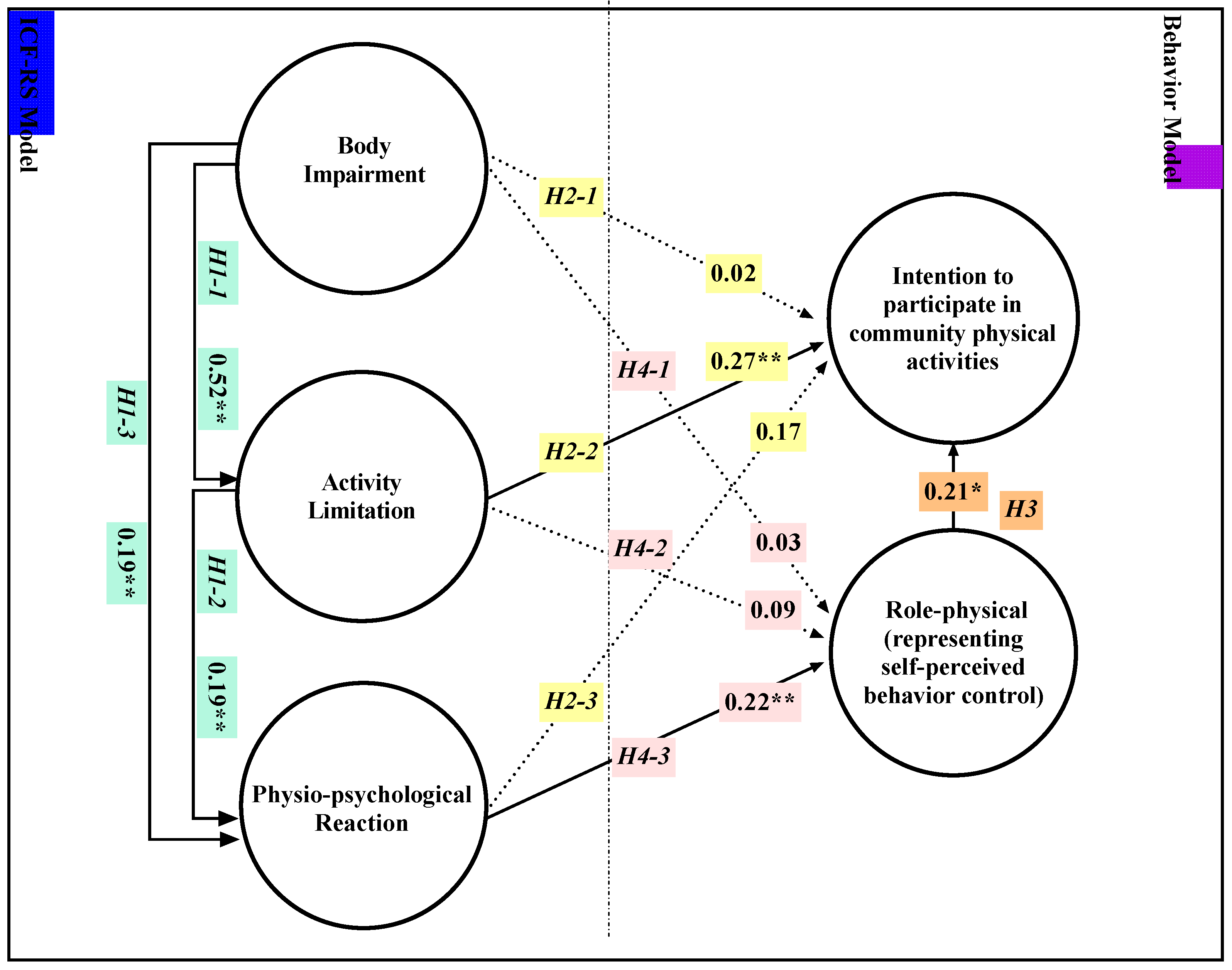
3.2. Structural Equation Modeling
4. Discussion
4.1. The ICF-RS and Planned Behavior Together Can Predict Participation Intentions
4.2. Cognition May Mediate between Impairment and Behavior
4.3. Body Impairment May Not Directly Affect Behavioral Intentions or Behavior
4.4. Potential Improvements to Aspects of the ICF
4.5. Clinical Implication of the Study
4.6. Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Body Impairment | Activity Limitation | Participation Limitation |
|---|---|---|
| b130 Energy and drive functions | d240 Handling stress and other psychological demands | d230 Carrying out daily routine |
| b134 Sleep functions | d410 Changing basic body position | d470 Using transportation |
| b152 Emotional functions | d415 Maintaining a body position | d660 Assisting others |
| b280 Sensation of pain | d420 Transferring oneself | d710 Basic interpersonal interactions |
| b455 Exercise tolerance functions | d455 Moving around | d770 Intimate relationships |
| b620 Urination functions | d450 Walking | d850 Remunerative employment |
| b640 Sexual functions | d465 Moving around using equipment | d920 Recreation and leisure |
| b710 Mobility of joint functions | d510 Washing oneself | |
| b730 Muscle power functions | d520 Caring for body parts | |
| d530 Toileting | ||
| d540 Dressing | ||
| d550 Eating | ||
| d570 Looking after one’s health | ||
| d640 Doing housework |
References
- Diaz, R.; Miller, E.K.; Kraus, E.; Fredericson, M. Impact of Adaptive Sports Participation on Quality of Life. Sports Med. Arthrosc. Rev. 2019, 27, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Quinn, F.; Johnston, M.; Dixon, D.; Johnston, D.W.; Pollard, B.; Rowley, D.I. Testing the integration of ICF and behavioral models of disability in orthopedic patients: Replication and extension. Rehabil. Psychol. 2012, 57, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Mavaddat, N.; Sadler, E.; Lim, L.; Williams, K.; Warburton, E.; Kinmonth, A.L.; Mckevitt, C.; Mant, J. What underlies the difference between self-reported health and disability after stroke? A qualitative study in the UK. BMC Neurol. 2021, 21, 315. [Google Scholar] [CrossRef] [PubMed]
- Dixon, D.; Johnston, M.; Elliott, A.; Hannaford, P. Testing integrated behavioural and biomedical models of activity and activity limitations in a population-based sample. Disabil. Rehabil. 2011, 34, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Health Promotion by Social Cognitive Means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behaviour: Reactions and reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar] [CrossRef]
- Sur, M.H.; Jung, J.; Shapiro, D.R. Theory of planned behavior to promote physical activity of adults with physical disabilities: Meta-analytic structural equation modeling. Disabil. Health J. 2021, 15, 101199. [Google Scholar] [CrossRef]
- Kostanjsek, N. Use of The International Classification of Functioning, Disability and Health (ICF) as a conceptual framework and common language for disability statistics and health information systems. BMC Public Health 2011, 11, S3. [Google Scholar] [CrossRef] [Green Version]
- Prodinger, B.; Cieza, A.; Oberhauser, C.; Bickenbach, J.; Üstün, T.B.; Chatterji, S.; Stucki, G. Toward the International Classification of Functioning, Disability and Health (ICF) Rehabilitation Set: A Minimal Generic Set of Domains for Rehabilitation as a Health Strategy. Arch. Phys. Med. Rehabil. 2016, 97, 875–884. [Google Scholar] [CrossRef] [Green Version]
- Prodinger, B.; Reinhardt, J.D.; Selb, M.; Stucki, G.; Yan, T.; Zhang, X.; Li, J. Towards system-wide implementation of the International Classification of Functioning, Disability and Health (ICF) in routine practice: Developing simple, intuitive descriptions of ICF categories in the ICF generic and rehabilitation set. J. Rehabil. Med. 2016, 48, 508–514. [Google Scholar] [CrossRef]
- Yan, T.; Zhang, M.; Yu, J.; Gao, Y.; Li, K.; Zhang, L.; Jin, D.; Sui, M.; Shen, W.; Li, T.; et al. Expert consensus on the International Classification of Functioning, Disability and Health (ICF). China J. Rehabil. Med. 2021, 36, 4–9. [Google Scholar]
- Gao, Y.; Yan, T.; You, L.; Liming, Y. Developing operational items for the International Classification of Functioning, Disability and Health Rehabilitation Set: The experience from China. Int. J. Rehabil. Res. 2018, 41, 20–27. [Google Scholar] [CrossRef]
- Gao, Y.; Yan, T.; You, L.; Li, K.; Zhang, L. The reliability and validity analysis of the International Classification of Functioning, Disability and Health Rehabilitation Set in non-acute patients. China J. Rehabil. Med. 2019, 34, 1193–1198. [Google Scholar]
- Zhang, M.; Zhang, Y.; Xiang, Y.; Lin, Z.; Shen, W.; Wang, Y.; Wang, L.; Yu, J.; Yan, T. A team approach to applying the International Classification of Functioning, Disability and Health Rehabilitation set in clinical evaluation. J. Rehabil. Med. 2021, 53, jrm00147. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.; Dixon, D. Developing an integrated biomedical and behavioural theory of functioning and disability: Adding models of behaviour to the ICF framework. Health Psychol. Rev. 2013, 8, 381–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajzen, I. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. J. Appl. Soc. Psychol. 2002, 32, 665–683. [Google Scholar] [CrossRef]
- Godin, G.; Kok, G. The Theory of Planned Behavior: A Review of its Applications to Health-Related Behaviors. Am. J. Health Promot. 1996, 11, 87–98. [Google Scholar] [CrossRef]
- Kirk, T.N.; Haegele, J.A. Theory of Planned Behavior in Research Examining Physical Activity Factors Among Individuals with Disabilities: A Review. Adapt. Phys. Act. Q. 2019, 36, 164–182. [Google Scholar] [CrossRef]
- Hausenblas, H.A.; Carron, A.V.; Mack, D.E. Application of the theories of reasoned action and planned behavior to exercise be-havior: A meta-analysis. J. Sport Exerc. Psych. 1997, 19, 36–51. [Google Scholar] [CrossRef]
- Hagger, M.; Chatzisarantis, N.; Biddle, S. A Meta-Analytic Review of the Theories of Reasoned Action and Planned Behavior in Physical Activity: Predictive Validity and the Contribution of Additional Variables. J. Sport Exerc. Psychol. 2002, 24, 3–32. [Google Scholar] [CrossRef]
- Downs, D.S.; Hausenblas, H.A. The Theories of Reasoned Action and Planned Behavior Applied to Exercise: A Meta-analytic Update. J. Phys. Act. Health 2005, 2, 76–97. [Google Scholar] [CrossRef]
- Johnston, M.; Bonetti, D.; Pollard, B. Disability as behaviour: Models of measurement and explanation. In Psychology at the Turn of the Millennium; Backman, I.L., von Hofston, C., Eds.; Psychology Press: Hove, UK, 2002; pp. 319–334. [Google Scholar]
- Dixon, D.; Johnston, M.; Rowley, D.; Pollard, B. Using the ICF and psychological models of behavior to predict mobility limitations. Rehabil. Psychol. 2008, 53, 191–200. [Google Scholar] [CrossRef]
- Johnston, M. Models of disability. Physiother. Theory Pract. 1996, 12, 131–141. [Google Scholar] [CrossRef]
- Pinhal, K.C.; Figueiredo, P.S.; De Oliveira, V.C.; Gomes, W.F.; Pernambuco, A.P.; Alcantara, M.A. Functional decline in people with diabetes: Bidirectional relationships between body function and activity–participation components in a two-wave longitudinal structural equation modeling. Physiother. Theory Pract. 2022, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kongwattanakul, K.; Hiengkaew, V.; Jalayondeja, C.; Sawangdee, Y. A structural equation model of falls at home in individuals with chronic stroke, based on the international classification of function, disability, and health. PLoS ONE 2020, 15, e0231491. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.Y.; Wu, C.-E. Predict the exercise behavior intention of the older adults in Taipei City to promote exercise behavior. Sci. Prog. 2021, 104, 1–13. [Google Scholar] [CrossRef]
- Stehr, P.; Rossmann, C.; Kremer, T.; Geppert, J. Determinants of Physical Activity in Older Adults: Integrating Self-Concordance into the Theory of Planned Behavior. Int. J. Environ. Res. Public Health 2021, 18, 5759. [Google Scholar] [CrossRef]
- Raggi, A.; Leonardi, M.; Ajovalasit, D.; Carella, F.; Soliveri, P.; Albanese, A.; Romito, L. Disability and profiles of functioning of patients with Parkinson’s disease described with ICF classification. Int. J. Rehabil. Res. 2011, 34, 141–150. [Google Scholar] [CrossRef]
- Chen, T.; Li, L.; Single, J.M.; Kochen, M.M. Comparison on the first version and the second version of SF-36. Chin. J. Soc. Med. 2006, 23, 111–114. [Google Scholar]
- Ware, J.E., Jr.; Kosinski, M.; Bayliss, M.S.; McHorney, C.A.; Rogers, W.H.; Raczek, A. Comparison of methods for the scoring and statis-tical analysis of SF-36 health profile and summary measures: Summary of results from the Medical Outcomes Study. Med. Care 1995, 33, AS264–AS279. [Google Scholar]
- Anonymous. Scientific Platform Serving for Statistics Professionals. Suzhou Zhongyan Network Technology. Available online: https://www.spsspro.com (accessed on 5 June 2022).
- Ferrando, P.J.; Lorenzo-Seva, U. Assessing the quality and appropriateness of factor solutions and factor score estimates in ex-ploratory item factor analysis. Educ. Psychol. Meas. 2018, 78, 762–780. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.T. Confirmatory Factor Analysis for Applied Research; Guilford Publication: New York, NY, USA, 2015. [Google Scholar]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Whibley, D.; AlKandari, N.; Kristensen, K.; Barnish, M.; Rzewuska, M.; Druce, K.L.; Tang, N.K.Y. Sleep and pain: A systematic review of studies of mediation. Clin. J. Pain. 2019, 35, 544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eiser, A.S. Physiology and Psychology of Dreams. Skull Base 2005, 25, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Knittle, K.; Nurmi, J.; Crutzen, R.; Hankonen, N.; Beattie, M.; Dombrowski, S.U. How can interventions increase motivation for physical activity? A systematic review and meta-analysis. Health Psychol. Rev. 2018, 12, 211–230. [Google Scholar] [CrossRef]
- Reedman, S.E.; Jayan, L.; Boyd, R.N.; Ziviani, J.; Elliott, C.; Sakzewski, L. Descriptive contents analysis of ParticiPAte CP: A participation-focused intervention to promote physical activity participation in children with cerebral palsy. Disabil. Rehabil. 2021, 1–11. [Google Scholar] [CrossRef]
- Sykes, C.R.; Maribo, T.; Stallinga, H.A.; Heerkens, Y. Remodeling of the ICF: A commentary. Disabil. Health J. 2020, 14, 100978. [Google Scholar] [CrossRef]
- Dekker, J.; de Groot, V. Psychological adjustment to chronic disease and rehabilitation: An exploration. Disabil. Rehabil. 2018, 40, 116–120. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, N.; Philpott-Morgan, S.; Dixon, D. Using impairment and cognitions to predict walking in osteoarthritis: A series of n-of-1 studies with an individually tailored, data-driven intervention. Brit. J. Health Psychol. 2016, 21, 52–70. [Google Scholar] [CrossRef]
- Maribo, T.; Petersen, K.S.; Handberg, C.; Melchiorsen, H.; Momsen, H.A.; Nielsen, C.V.; Leonardi, M.; Labriola, M. Systematic literature review on ICF from 2001 to 2013 in the Nordic countries focusing on clinical and rehabilitation context. J. Clin. Med. Res. 2016, 8, 1327–1328. [Google Scholar] [CrossRef] [Green Version]
- Leonardi, M.; Sykes, C.R.; Madden, R.C.; Napel, H.T.; Hollenweger, J.; Snyman, S.; Madden, R.H.; de Camargo, O.K.; Raggi, A.; van Gool, C.H.; et al. Do we really need to open a classification box on personal factors in ICF? Disabil. Rehabil. 2015, 38, 1327–1328. [Google Scholar] [CrossRef] [PubMed]
- Heerkens, Y.F.; De Weerd, M.; Huber, M.; De Brouwer, C.P.M.; Van Der Veen, S.; Perenboom, R.J.M.; Van Gool, C.H.; Napel, H.T.; Van Bon-Martens, M.; Stallinga, H.A.; et al. Reconsideration of the scheme of the international classification of functioning, disability and health: Incentives from the Netherlands for a global debate. Disabil. Rehabil. 2017, 40, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Jette, A.M. The Utility of and Need for Improving the ICF. Phys. Ther. 2018, 98, 629–630. [Google Scholar] [CrossRef] [PubMed]




| Variable | N (%) | Missing Records (N) |
|---|---|---|
| Sex, Male | 368 (71.5%) | 1 |
| Age, years | 16 * | |
| ≤39 years | 81 (16.2%) | |
| 40–59 years | 241 (48.2%) | |
| ≥60 years | 178 (35.3%) | |
| Education | 6 | |
| None | 49 (9.6%) | |
| Elementary | 196 (38.4%) | |
| Secondary or over | 265 (52.0%) | |
| Marital status | 10 | |
| Married | 371 (73.3%) | |
| Unmarried | 135 (26.7%) |
| Latent Factors | Items/Variants | Standardized Factor Loading |
|---|---|---|
| Body Impairment | ||
| b730 Muscle power functions | 0.846 | |
| b710 Mobility of joint functions | 0.837 | |
| Activity Limitation | ||
| d420 Transferring oneself | 0.772 | |
| d450 Walking | 0.674 | |
| d520 Caring for body parts | 0.855 | |
| d530 Toileting | 0.891 | |
| d540 Dressing | 0.776 | |
| d550 Eating | 0.692 | |
| Physio-psychological Reaction | ||
| b134 Sleep functions | 0.711 | |
| b152 Emotional functions | 0.679 | |
| b280 Sensation of pain | 0.533 | |
| Role-physical (representing self-perceived behavior control) | ||
| Perceived limited by time taken in tasks | 0.872 | |
| Perceived to have accomplished less | 0.874 | |
| Perceived limit on types of tasks | 0.858 | |
| Perceived difficulty with tasks | 0.827 | |
| Intention to participate in community physical activities | ||
| whether willing to participate | 0.507 | |
| whether have a chance to participate | 0.454 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, Q.; Xie, H.; Zheng, D.; Wu, X.; Zhang, Y.; Li, T.; Yan, T. Predicting Intention to Participate in Community Physical Activities for Adults with Physical Disabilities. J. Pers. Med. 2022, 12, 1832. https://doi.org/10.3390/jpm12111832
Xu Q, Xie H, Zheng D, Wu X, Zhang Y, Li T, Yan T. Predicting Intention to Participate in Community Physical Activities for Adults with Physical Disabilities. Journal of Personalized Medicine. 2022; 12(11):1832. https://doi.org/10.3390/jpm12111832
Chicago/Turabian StyleXu, Qi, Hongwu Xie, Dingzhao Zheng, Xinhong Wu, Yun Zhang, Taibiao Li, and Tiebin Yan. 2022. "Predicting Intention to Participate in Community Physical Activities for Adults with Physical Disabilities" Journal of Personalized Medicine 12, no. 11: 1832. https://doi.org/10.3390/jpm12111832