
Detecting the Effect Size of Weather Conditions on Patient-Reported Outcome Measures (PROMs)
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Statistical Analysis
3. Results
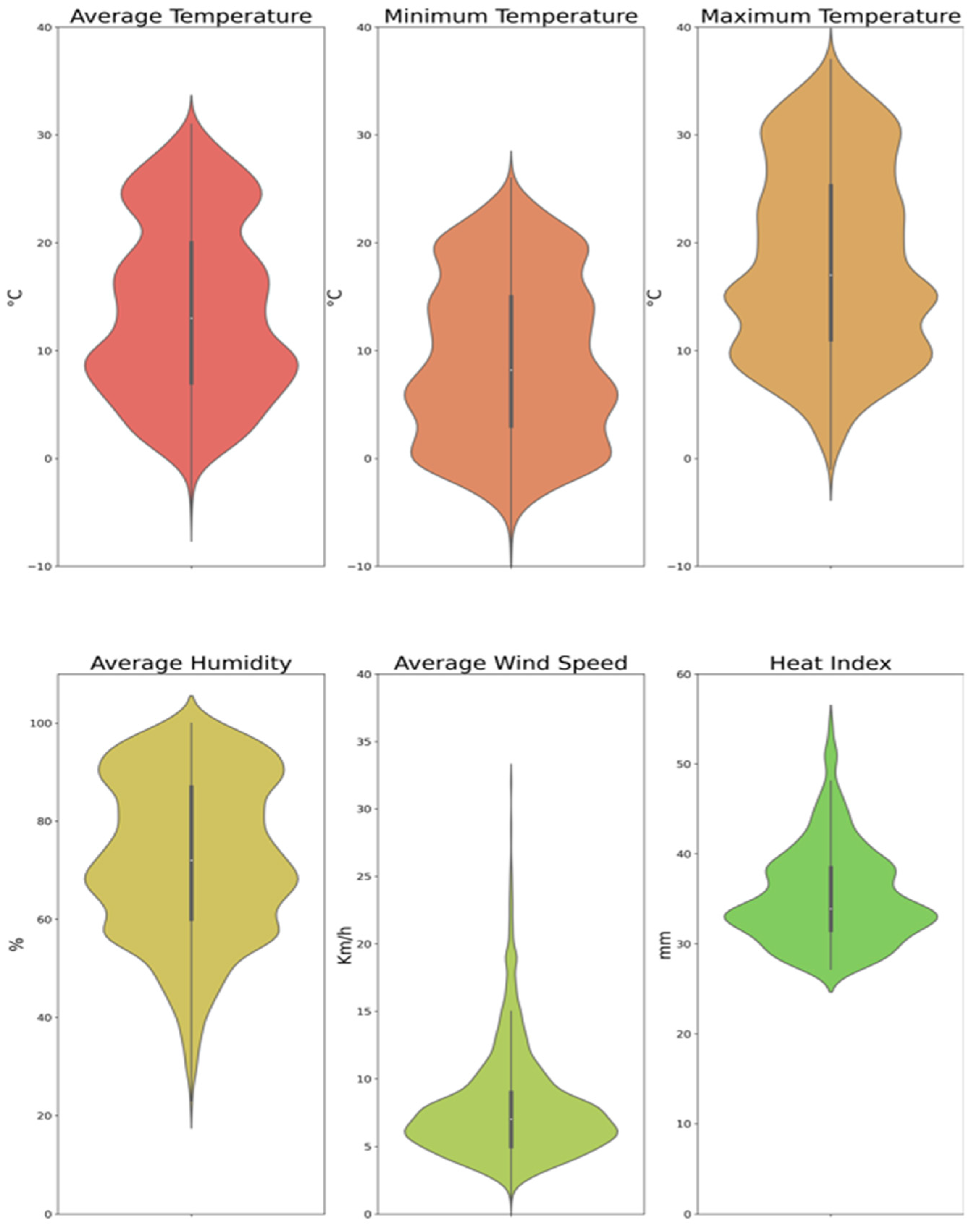
3.1. Descriptive Analysis
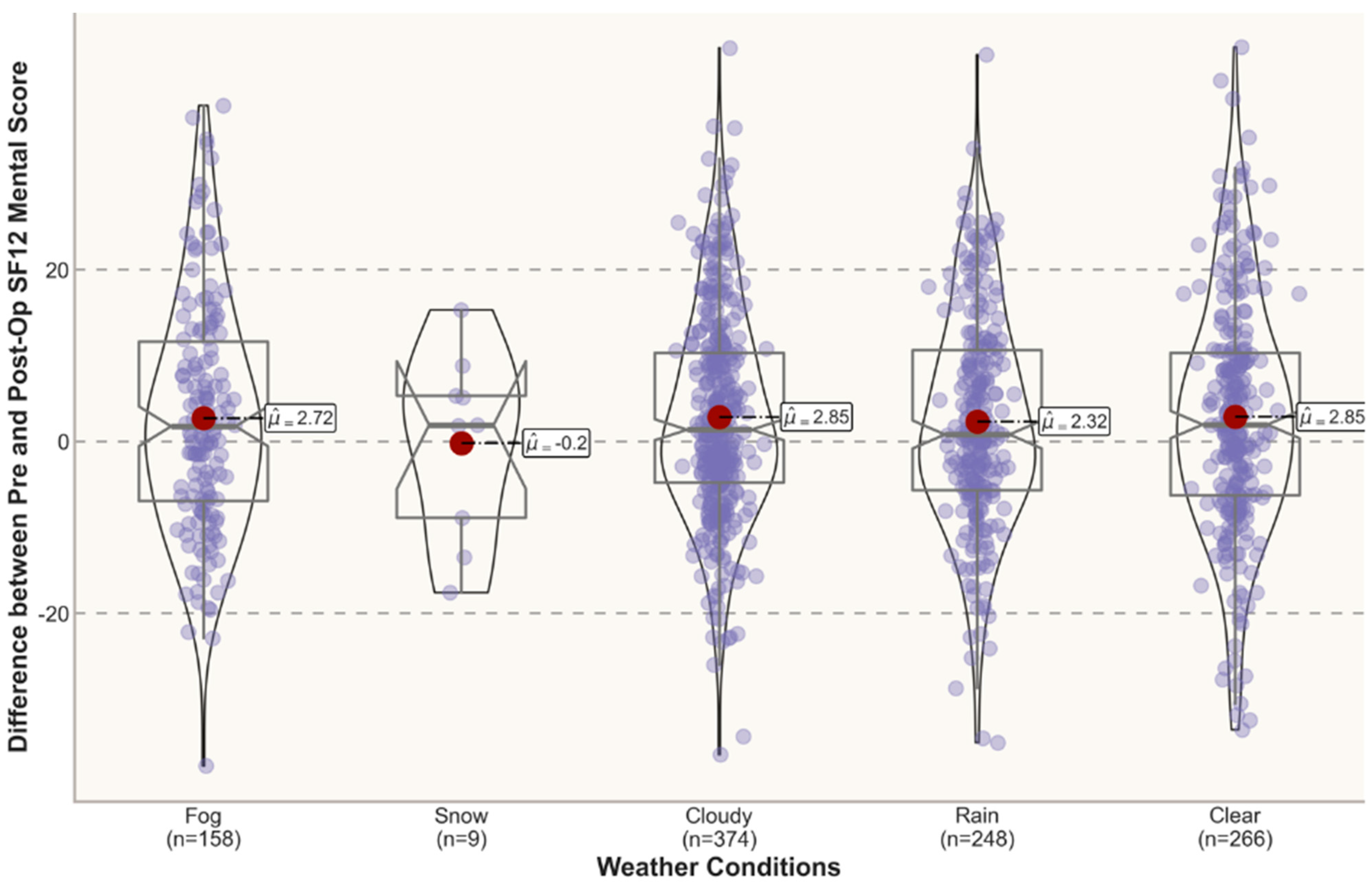
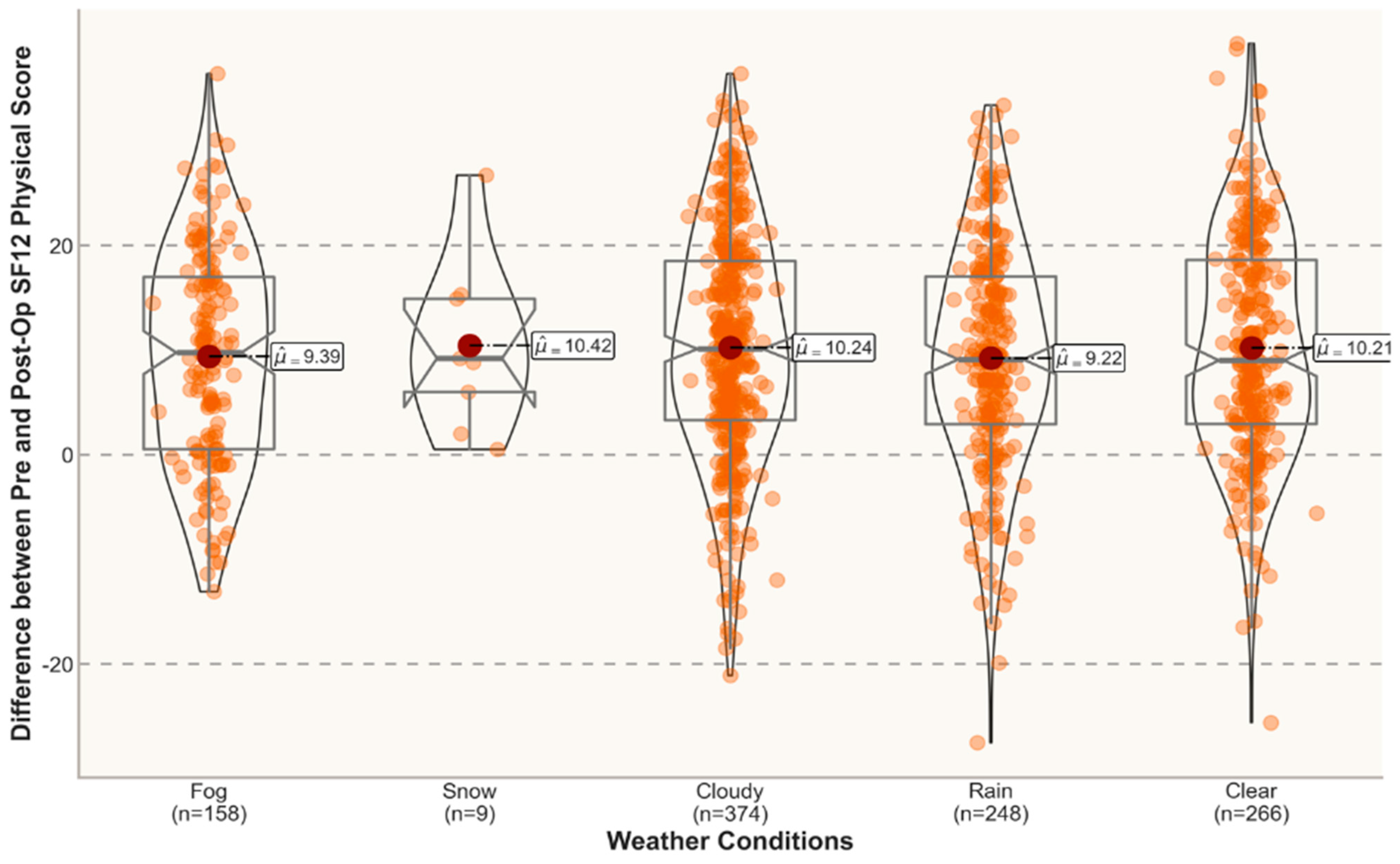
3.2. Hypothesis Testing
3.2.1. Humidity 3rd Quartile
3.2.2. Clear and Sunny Weather
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Domb, B.G.; Ouyang, V.W.; Go, C.C.; Gornbein, J.A.; Shapira, J.; Meghpara, M.B.; Maldonado, D.R.; Lall, A.C.; Rosinsky, P.J. Personalized Medicine Using Predictive Analytics: A Machine Learning-Based Prognostic Model for Patients Undergoing Hip Arthroscopy. Am. J. Sports Med. 2022, 50, 1900–1908. [Google Scholar] [CrossRef] [PubMed]
- Fox, R.J. Tissue Markers for Acute Multiple Sclerosis Treatment Response—A Step Toward Personalized Medicine. JAMA Neurol. 2018, 75, 406–407. [Google Scholar] [CrossRef] [PubMed]
- Chopra, S.S. Preparing for Personalized Medicine. JAMA 2004, 291, 1640. [Google Scholar] [CrossRef] [PubMed]
- Davidson, G.H.; Haukoos, J.S.; Feldman, L.S. Practical Guide to Assessment of Patient-Reported Outcomes. JAMA Surg. 2020, 155, 432–433. [Google Scholar] [CrossRef]
- Baldwin, M.; Spong, A.; Doward, L.; Gnanasakthy, A. Patient-reported outcomes, patient-reported information. Patient 2011, 4, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Damman, O.C.; Verbiest, M.E.A.; Vonk, S.I.; Berendse, H.W.; Bloem, B.R.; De Bruijne, M.C.; Faber, M.J. Using PROMs during routine medical consultations: The perspectives of people with Parkinson’s disease and their health professionals. Health Expect. 2019, 22, 939–951. [Google Scholar] [CrossRef] [Green Version]
- Weldring, T.; Smith, S.M. Article Commentary: Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health. Serv. Insights 2013, 6, HSI.S11093-68. [Google Scholar] [CrossRef]
- Whittal, A.; Meregaglia, M.; Nicod, E. The Use of Patient-Reported Outcome Measures in Rare Diseases and Implications for Health Technology Assessment. Patient 2021, 14, 485–503. [Google Scholar] [CrossRef]
- Black, N. Patient reported outcome measures could help transform healthcare. BMJ 2013, 346, f167. [Google Scholar] [CrossRef] [Green Version]
- Porter, M.E. What is value in health care. N. Engl. J. Med. 2010, 363, 2477–2481. [Google Scholar] [CrossRef]
- Tan, H.; Juan, L.Y. Finance transformation for healthcare: A structured model for planning and action. Int. J. Healthc. 2018, 5, 42. [Google Scholar] [CrossRef] [Green Version]
- Dias-Barbosa, C.; Matos, R.; Vernon, M.; Carney, C.E.; Krystal, A.; Puelles, J. Content validity of a sleep numerical rating scale and a sleep diary in adults and adolescents with moderate-to-severe atopic dermatitis. J. Patient Rep. 2020, 4, 100. [Google Scholar] [CrossRef] [PubMed]
- Moeini, S.; Rasmussen, J.V.; Klausen, T.W.; Brorson, S. Rasch analysis of the Western Ontario Osteoarthritis of the Shoulder index—the Danish version. Patient Relat. Outcome Meas. 2016, 7, 173–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loth, F.; Liebensteiner, M.; Giesinger, J.; Giesinger, K.; Bliem, H.; Holzner, B. What makes patients aware of their artificial knee joint? BMC Musculoskelet. Disord. 2018, 19, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, M.K.; Saucier, C.; Bailey, M.; D’Alessio, D.; Foster, A.; Pierre, D.S.; Raymond, K. Content validation of a self-report daily diary in patients with sickle cell disease. J. Patient-Rep. 2021, 5, 63. [Google Scholar] [CrossRef] [PubMed]
- Symonds, T.; A Randall, J.; Hoffman, D.L.; Zakrzewska, J.M.; Gehringer, W.; Lee, J.Y. Measuring the impact of trigeminal neuralgia pain: The Penn Facial Pain Scale-Revised. J. Pain Res. 2018, 11, 1067–1073. [Google Scholar] [CrossRef] [Green Version]
- Panter, C.; Berry, P.; Chauhan, D.; Fernandes, S.; Gatsi, S.; Park, J.; Wells, J.R.; Arbuckle, R. A qualitative exploration of the patient experience of erosive and non-erosive hand osteoarthritis. J. Patient Rep. 2021, 5, 18. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Lei, D.; Yousaf, M.; Janmohamed, S.R.; Vakharia, P.P.; Chopra, R.; Chavda, R.; Gabriel, S.; Patel, K.R.; Singam, V. Association of itch triggers with atopic dermatitis severity and course in adults. Ann. Allergy Asthma Immunol. 2020, 125, 552–559.e552. [Google Scholar] [CrossRef]
- Saarensilta, I.A.; Edman, G.; Ackermann, P. Achilles tendon ruptures during summer show the lowest incidence, but exhibit an increased risk of re-rupture. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 3978–3986. [Google Scholar] [CrossRef]
- Bentley, S.; Findley, A.; Chiva-Razavi, S.; Naujoks, C.; Patalano, F.; Johnson, C.; Arbuckle, R.; Wolffsohn, J.S. Understanding the visual function symptoms and associated functional impacts of phakic presbyopia. J. Patient-Rep. 2021, 5, 114. [Google Scholar] [CrossRef]
- Schallhorn, S.; Brown, M.; Venter, J.; Hettinger, K.; Hannan, S. The Role of the Mesopic Pupil on Patient-Reported Outcomes in Young Patients with Myopia 1 Month After Wavefront-Guided LASIK. J. Refract. Surg. 2014, 30, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Innominato, P.F.; Komarzynski, S.; Palesh, O.G.; Dallmann, R.; Bjarnason, G.A.; Giacchetti, S.; Ulusakarya, A.; Bouchahda, M.; Haydar, M.; Ballesta, A.; et al. Circadian rest-activity rhythm as an objective biomarker of patient-reported outcomes in patients with advanced cancer. Cancer Med. 2018, 7, 4396–4405. [Google Scholar] [CrossRef] [PubMed]
- Palesh, O.; Haitz, K.; Lévi, F.; Bjarnason, G.A.; Deguzman, C.; Alizeh, I.; Ulusakarya, A.; Packer, M.M.; Innominato, P.F. Relationship between subjective and actigraphy-measured sleep in 237 patients with metastatic colorectal cancer. Qual. Life Res. 2017, 26, 2783–2791. [Google Scholar] [CrossRef]
- Yang, P.-L.; Ward, T.M.; Burr, R.L.; Kapur, V.K.; McCurry, S.M.; Vitiello, M.V.; Hough, C.L.; Parsons, E.C. Sleep and Circadian Rhythms in Survivors of Acute Respiratory Failure. Front. Neurol. 2020, 11, 94. [Google Scholar] [CrossRef] [PubMed]
- Cabitza, F.; Dui, L.G.; Banfi, G. PROs in the wild: Assessing the validity of patient reported outcomes in an electronic registry. Comput. Methods Programs Biomed. 2019, 181, 104837. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.B.; Bell, M.L.; Peng, R.D. Methods to calculate the heat index as an exposure metric in environmental health research. Environ. Health Perspect. 2013, 121, 1111–1119. [Google Scholar] [CrossRef]
- Blazejczyk, K.; Epstein, Y.; Jendritzky, G.; Staiger, H.; Tinz, B. Comparison of UTCI to selected thermal indices. Int. J. Biometeorol. 2011, 56, 515–535. [Google Scholar] [CrossRef] [Green Version]
- Awasthi, A.; Vishwakarma, K.; Pattnayak, K.C. Retrospection of heatwave and heat index. Arch. Meteorol. Geophys. Bioclimatol. Ser. B 2021, 147, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Arundel, A.V.; Sterling, E.M.; Biggin, J.H.; Sterling, T.D. Indirect health effects of relative humidity in indoor environments. Environ. Health Perspect. 1986, 65, 351–361. [Google Scholar] [CrossRef] [Green Version]
- Larson, R.B. Controlling social desirability bias. Int. J. Mark. Res. 2018, 61, 534–547. [Google Scholar] [CrossRef]
- Kline, A.; Luo, Y. PsmPy: A package for retrospective cohort matching in python. In Proceedings of the 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, UK, 11–15 July 2022; IEEE: New York, NY, USA; pp. 1354–1357. [Google Scholar]
- Jafari, M.; Ansari-Pour, N. Why, When and How to Adjust Your P Values? Cell J. 2019, 20, 604–607. [Google Scholar] [CrossRef]
- Lee, D.K. Alternatives to P value: Confidence interval and effect size. Korean J. Anesthesiol. 2016, 69, 555–562. [Google Scholar] [CrossRef] [Green Version]
- Webster, K.E.; Feller, J.A. Comparison of the short form-12 (SF-12) health status questionnaire with the SF-36 in patients with knee osteoarthritis who have replacement surgery. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2620–2626. [Google Scholar] [CrossRef]
- Diacon, A.; Kimmel, L.; Hau, R.; Gabbe, B.; Edwards, E. Outcomes of midfoot and hindfoot fractures in multitrauma patients. Injury 2018, 50, 558–563. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Mean | Std | 95% Mean CI | Median | IQR |
|---|---|---|---|---|---|
| Age | 67.84 | 11.34 | [67.63, 68.05] | 69.00 | 15.00 |
| VAS total score: | |||||
| Pre-Op | 7.00 | 2.12 | [6.90, 7.10] | 7.00 | 2.00 |
| 3 months | 2.44 | 2.53 | [2.32, 2.55] | 2.00 | 4.00 |
| 6 months | 2.41 | 2.70 | [2.28, 2.55] | 1.00 | 4.00 |
| SF12 Physical Score: | |||||
| Pre-Op | 32.89 | 7.98 | [32.52, 33.26] | 31.80 | 10.90 |
| 3 months | 42.66 | 9.21 | [42.25, 43.06] | 42.60 | 15.20 |
| 6 months | 44.37 | 9.73 | [43.91, 44.84] | 46.25 | 16.40 |
| SF12 Mental Score: | |||||
| Pre-Op | 49.11 | 12.15 | [48.56, 49.67] | 50.30 | 18.27 |
| 3 months | 51.96 | 10.29 | [51.51, 52.41] | 54.80 | 14.80 |
| 6 months | 51.80 | 10.17 | [51.31, 52.28] | 54.70 | 14.10 |
| Avg Temperature (°C) | 13.78 | 8.01 | [13.63, 13.93] | 13.00 | 13.00 |
| Min Temperature (°C) | 9.19 | 7.15 | [9.04, 9.33] | 8.20 | 12.00 |
| Max Temperature (°C) | 18.29 | 8.67 | [18.13, 18.45] | 17.00 | 14.30 |
| Avg Humidity (%) | 72.27 | 16.05 | [71.93, 72.60] | 72.00 | 27.00 |
| Avg Wind Speed (km/h) | 7.86 | 3.89 | [7.78, 7.94] | 7.00 | 4.00 |
| Precipitations (mm) | 4.57 | 10.45 | [4.11, 5.03] | 0.00 | 4.00 |
| Heat Index | 35.25 | 5.27 | [35.01, 35.50] | 33.89 | 6.97 |
| Variable Groups | VAS Total Score | SF12 PhysicalScore | SF12 MentalScore | |||
|---|---|---|---|---|---|---|
| Score | Improvement | Score | Improvement | Score | Improvement | |
| Humidity 3rd quartile | 0.918 | 0.394 | 0.011 * | 0.003 * | 0.021 * | 0.001 * |
| Clear and sunny weather | 0.300 | 0.308 | 0.159 | 0.279 | 0.001 * | 0.037 * |
| Variable Groups | VAS Total Score | SF12 PhysicalScore | SF12 Mental Score | |||
|---|---|---|---|---|---|---|
| Score | Improvement | Score | Improvement | Score | Improvement | |
| Humidity 3rd quartile | 0.662 | 0.937 | 0.130 | 0.064 | 0.529 | 0.082 |
| Clear and sunny weather | 0.973 | 0.742 | 0.545 | 0.403 | 0.321 | 0.975 |
| Groups | Score | Time | Test | Stat | p-Value | p-Value adj | n | Group 1 (m ± SD [CI90\%]) | Group 2 (m ± SD [CI90\%]) | Cohen d |
|---|---|---|---|---|---|---|---|---|---|---|
| Clear vs. Other | VAS | Post-Op | Mann–Whitney | 111,064.5 | 0.300 | 0.837 | 487 | 2.00 ± 4.00 [1.00, 2.00] | 2.00 ± 4.00 [1.00, 2.00] | −0.06 |
| Improvement | Mann–Whitney | 111,053 | 0.308 | 0.837 | 487 | −5.00 ± 4.50 [−5.00, −5.00] | −5.00 ± 5.00 [−5.00, −4.00] | −0.06 | ||
| SF12-PS | Post-Op | Mann–Whitney | 152,717 | 0.159 | 0.636 | 546 | 43.80 ± 15.00 [42.40, 44.80] | 42.20 ± 14.20 [41.40, 43.60] | 0.09 | |
| Improvement | t-test | 1.1 | 0.279 | 0.837 | 546 | 10.30 ± 10.80 [9.57, 10.40] | 9.60 ± 10.20 [8.91, 10.40] | 0.07 | ||
| SF12-MS | Post-Op | Mann–Whitney | 160,453.5 | 0.001 | 0.006 | 552 | 56.00 ± 12.70 [55.30, 56.90] | 54.40 ± 16.70 [53.10, 55.20] | 0.16 | |
| Improvement | t-test | 2.1 | 0.037 | 0.185 | 552 | 3.90 ± 12.70 [3.05, 3.22] | 2.30 ± 12.90 [1.40, 3.24] | 0.13 | ||
| Humidity > 60 | VAS | Post-Op | Mann–Whitney | 87,722.5 | 0.293 | 1.000 | 403 | 2.00 ± 4.00 [1.00, 2.00] | 2.00 ± 4.00 [1.00, 2.00] | 0.08 |
| Improvement | Mann–Whitney | 88,234.5 | 0.236 | 1.000 | 403 | −5.00 ± 5.00 [−5.00, −4.00] | −5.00 ± 4.00 [−5.00, −5.00] | 0.09 | ||
| SF12-PS | Post-Op | Mann–Whitney | 100,346.5 | 0.823 | 1.000 | 418 | 43.10 ± 16.10 [41.40, 44.80] | 43.30 ± 14.20 [42.20, 44.20] | 0.01 | |
| Improvement | t-test | 0.9 | 0.365 | 1.000 | 418 | 10.20 ± 11.00 [9.28, 10.40] | 9.50 ± 10.30 [8.75, 10.30] | 0.06 | ||
| SF12-MS | Post-Op | Mann–Whitney | 102,844 | 0.910 | 1.000 | 434 | 54.20 ± 15.00 [53.20, 56.00] | 55.20 ± 14.20 [54.30, 55.90] | −0.01 | |
| Improvement | t-test | −0.1 | 0.911 | 1.000 | 434 | 2.20 ± 12.60 [1.20, 3.29] | 2.30 ± 12.50 [1.35, 3.24] | −0.01 | ||
| Humidity 3rd quartile | VAS | Post-Op | Mann–Whitney | 26,373.5 | 0.918 | 0.918 | 249 | 2.00 ± 4.00 [1.00, 2.00] | 2.00 ± 4.00 [1.00, 2.00] | −0.02 |
| Improvement | Mann–Whitney | 25,304.5 | 0.394 | 0.788 | 249 | −5.00 ± 5.00 [−6.00, −5.00] | −5.00 ± 5.00 [−5.00, −4.00] | −0.08 | ||
| SF12-PS | Post-Op | Mann–Whitney | 30,223.5 | 0.011 | 0.044 | 230 | 44.90 ± 15.60 [43.30, 46.20] | 41.50 ± 14.60 [39.40, 43.40] | 0.23 | |
| Improvement | t-test | 3 | 0.003 | 0.015 | 230 | 11.60 ± 9.80 [10.60, 9.84] | 8.80 ± 10.70 [7.62, 9.93] | 0.28 | ||
| SF12-MS | Post-Op | Mann–Whitney | 29,481 | 0.021 | 0.063 | 227 | 56.00 ± 12.70 [55.30, 57.50] | 52.80 ± 18.20 [51.30, 54.80] | 0.24 | |
| Improvement | t-test | 1.9 | 0.001 | 0.006 | 227 | 4.20 ± 12.70 [2.80, 3.31] | 1.90 ± 12.30 [0.57, 3.25] | 0.18 | ||
| Heat Index > 27 | VAS | Post-Op | Mann–Whitney | 13,302 | 0.723 | 1.000 | 154 | 1.00 ± 3.80 [1.00, 2.00] | 1.00 ± 3.00 [1.00, 2.00] | 0.00 |
| Improvement | Mann–Whitney | 14,114 | 0.187 | 0.935 | 154 | −5.00 ± 4.00 [−6.00, −5.00] | −6.00 ± 4.00 [−6.00, −5.00] | 0.15 | ||
| SF12-PS | Post-Op | Mann–Whitney | 13,400.5 | 0.895 | 1.000 | 151 | 43.00 ± 15.20 [40.10, 44.60] | 44.80 ± 14.80 [41.40, 46.50] | −0.02 | |
| Improvement | t-test | −1.7 | 0.086 | 0.516 | 151 | 10.20 ± 10.80 [8.74, 13.60] | 12.10 ± 9.40 [11.00, 13.30] | −0.19 | ||
| SF12-MS | Post-Op | Mann–Whitney | 12,355 | 0.295 | 1.000 | 148 | 54.70 ± 14.60 [53.20, 56.00] | 56.70 ± 15.20 [55.10, 58.30] | −0.07 | |
| Improvement | t-test | −0.6 | 0.539 | 1.000 | 148 | 2.30 ± 13.10 [0.52, 4.95] | 3.20 ± 12.90 [1.58, 4.77] | −0.07 | ||
| Heat Index > 32 | VAS | Post-Op | Mann–Whitney | 7695.5 | 0.718 | 1.000 | 135 | 1.00 ± 3.00 [1.00, 2.00] | 1.00 ± 4.00 [1.00, 2.00] | −0.06 |
| Improvement | Mann–Whitney | 8441 | 0.344 | 1.000 | 135 | −5.00 ± 4.50 [−6.00, −5.00] | −6.00 ± 4.00 [−6.00, −5.00] | 0.13 | ||
| SF12-PS | Post-Op | Mann–Whitney | 6688.5 | 0.952 | 1.000 | 105 | 43.50 ± 16.40 [40.90, 45.30] | 45.80 ± 13.70 [42.10, 47.60] | −0.02 | |
| Improvement | t-test | −1 | 0.320 | 1.000 | 105 | 10.80 ± 11.00 [8.98, 13.90] | 12.10 ± 9.70 [10.70, 13.50] | −0.13 | ||
| SF12-MS | Post-Op | Mann–Whitney | 6721.5 | 0.798 | 1.000 | 103 | 56.00 ± 12.80 [53.90, 57.60] | 56.70 ± 13.10 [55.10, 58.30] | 0.06 | |
| Improvement | t-test | 0.7 | 0.504 | 1.000 | 103 | 3.80 ± 12.40 [1.79, 4.72] | 2.70 ± 12.70 [0.84, 4.56] | 0.09 | ||
| Heat Index > 41 | VAS | Post-Op | Mann–Whitney | 322 | 0.640 | 1.000 | 26 | 2.00 ± 5.00 [0.00, 5.00] | 1.00 ± 4.00 [0.00, 3.00] | 0.15 |
| Improvement | t-test | 1.6 | 0.114 | 0.684 | 26 | −3.60 ± 3.40 [−4.75, −3.95] | −5.10 ± 3.00 [−6.14, −4.03] | 0.46 | ||
| SF12-PS | Post-Op | t-test | 0.7 | 0.459 | 1.000 | 23 | 43.70 ± 9.70 [40.20, 45.20] | 41.70 ± 9.20 [38.50, 44.80] | 0.22 | |
| Improvement | t-test | −0.2 | 0.808 | 1.000 | 23 | 9.40 ± 8.70 [6.32, 13.20] | 10.00 ± 7.90 [7.34, 12.70] | −0.07 | ||
| SF12-MS | Post-Op | t-test | −0.6 | 0.542 | 1.000 | 29 | 51.40 ± 9.30 [48.50, 55.90] | 53.00 ± 9.10 [49.90, 56.10] | −0.17 | |
| Improvement | t-test | 0 | 0.987 | 1.000 | 29 | 3.30 ± 12.30 [−0.57, 7.26] | 3.40 ± 10.30 [−0.17, 6.91] | 0.00 | ||
| Day vs. Night | VAS | Post-Op | Mann–Whitney | 7277.5 | 0.807 | 1.000 | 130 | 2.00 ± 4.00 [1.00, 2.00] | 2.00 ± 4.00 [1.00, 3.00] | −0.02 |
| Improvement | Mann–Whitney | 7045.5 | 0.506 | 1.000 | 130 | −5.00 ± 4.00 [−5.00, −4.00] | −5.00 ± 5.00 [−5.00, −4.00] | −0.12 | ||
| SF12-PS | Post-Op | Mann–Whitney | 11,166.5 | 0.062 | 0.372 | 157 | 40.90 ± 16.50 [39.60, 43.30] | 39.80 ± 15.10 [37.30, 41.50] | 0.22 | |
| Improvement | t-test | 1.7 | 0.086 | 0.430 | 157 | 9.60 ± 10.80 [8.14, 8.83] | 7.40 ± 10.30 [5.88, 8.91] | 0.21 | ||
| SF12-MS | Post-Op | Mann–Whitney | 10,108.5 | 0.484 | 1.000 | 153 | 54.10 ± 15.70 [52.00, 56.30] | 52.80 ± 15.60 [50.70, 53.80] | 0.07 | |
| Improvement | t-test | −0.1 | 0.892 | 1.000 | 153 | 0.60 ± 13.00 [−1.17, 2.51] | 0.80 ± 12.90 [−1.13, 2.68] | −0.02 |
| Groups | Score | Time | Test | Stat | p-Value | p-Value adj | n | Group 1 (m ± SD [CI90\%]) | Group 2 (m ± SD [CI90\%]) | Cohen’s d |
|---|---|---|---|---|---|---|---|---|---|---|
| Clear vs. Other | VAS | Post-Op | Mann–Whitney | 62,723 | 0.973 | 1.000 | 348 | 1.00 ± 4.00 [1.00, 2.00] | 1.00 ± 4.00 [1.00, 1.00] | −0.04 |
| Improvement | Mann–Whitney | 637,065 | 0.742 | 1.000 | 348 | −5.00 ± 4.00 [−5.00, −5.00] | −5.00 ± 5.00 [−5.00, −5.00] | 0.01 | ||
| SF12-PS | Post-Op | Mann–Whitney | 83,183 | 0.545 | 1.000 | 406 | 46.80 ± 15.70 [45.20, 48.50] | 47.30 ± 15.70 [46.30, 48.50] | −0.02 | |
| Improvement | t-test | 82,391 | 0.403 | 1.000 | 406 | 12.40 ± 14.40 [11.20, 13.90] | 13.00 ± 16.00 [11.90, 14.10] | −0.05 | ||
| SF12-MS | Post-Op | Mann–Whitney | 865,015 | 0.321 | 1.000 | 396 | 55.90 ± 14.40 [54.90, 56.80] | 54.70 ± 12.90 [53.70, 55.70] | 0.02 | |
| Improvement | t-test | 83,054 | 0.975 | 1.000 | 396 | 1.40 ± 16.60 [0.40, 2.70] | 0.70 ± 17.70 [−0.30, 2.30] | 0.01 | ||
| Humidity > 60 | VAS | Post-Op | Mann–Whitney | 16,059 | 0.662 | 1.000 | 182 | 1.00 ± 4.00 [1.00, 2.00] | 1.00 ± 4.00 [1.00, 1.00] | −0.01 |
| Improvement | Mann–Whitney | 15,576 | 0.937 | 1.000 | 182 | −5.00 ± 4.00 [−6.00, −4.00] | −5.00 ± 5.00 [−6.00, −5.00] | −0.02 | ||
| SF12-PS | Post-Op | Mann–Whitney | 171,165 | 0.130 | 0.520 | 174 | 44.40 ± 15.50 [42.40, 46.60] | 48.00 ± 15.70 [46.70, 49.80] | −0.12 | |
| Improvement | t-test | −19 | 0.064 | 0.384 | 174 | 11.00 ± 9.80 [9.75, 14.10] | 12.90 ± 10.50 [11.70, 14.10] | −0.19 | ||
| SF12-MS | Post-Op | Mann–Whitney | 22,405 | 0.529 | 1.000 | 215 | 54.80 ± 15.10 [53.00, 56.40] | 55.50 ± 12.90 [53.60, 56.60] | −0.06 | |
| Improvement | t-test | −17 | 0.082 | 0.410 | 215 | 2.10 ± 13.60 [0.60, 5.86] | 4.30 ± 12.60 [2.92, 5.75] | −0.17 | ||
| Humidity 3rd quartile | VAS | Post-Op | Mann–Whitney | 42,734 | 0.275 | 1.000 | 306 | 1.00 ± 4.00 [1.00, 1.00] | 2.00 ± 4.00 [1.00, 2.00] | −0.04 |
| Improvement | Mann–Whitney | 417,585 | 0.127 | 0.762 | 306 | −5.00 ± 5.00 [−6.00, −5.00] | −5.00 ± 5.00 [−5.00, −4.00] | −0.09 | ||
| SF12-PS | Post-Op | Mann–Whitney | 60,616 | 0.320 | 1.000 | 364 | 48.00 ± 16.40 [46.80, 49.50] | 46.00 ± 14.90 [44.30, 47.90] | 0.04 | |
| Improvement | t-test | 1 | 0.882 | 1.000 | 364 | 12.00 ± 10.90 [11.10, 12.80] | 11.90 ± 9.60 [11.00, 12.80] | 0.01 | ||
| SF12-MS | Post-Op | Mann–Whitney | 54,983 | 0.934 | 1.000 | 346 | 55.70 ± 12.90 [54.40, 56.40] | 55.20 ± 13.50 [53.80, 56.00] | −0.03 | |
| Improvement | t-test | 14 | 0.178 | 0.890 | 346 | 3.20 ± 13.50 [1.98, 3.00] | 1.80 ± 12.50 [0.65, 2.96] | 0.10 | ||
| Heat Index > 27 | VAS | Post-Op | Mann–Whitney | 9150 | 0.378 | 1.000 | 138 | 1.00 ± 4.00 [1.00, 2.00] | 1.00 ± 3.00 [1.00, 1.00] | 0.14 |
| Improvement | Mann–Whitney | 82,925 | 0.588 | 1.000 | 138 | −5.50 ± 4.00 [−6.00, −5.00] | −5.00 ± 4.00 [−6.00, −5.00] | −0.04 | ||
| SF12-PS | Post-Op | Mann–Whitney | 100,825 | 0.413 | 1.000 | 163 | 48.40 ± 16.40 [44.20, 50.80] | 48.00 ± 12.40 [46.30, 50.10] | −0.13 | |
| Improvement | t-test | −9 | 0.375 | 1.000 | 163 | 12.60 ± 10.70 [11.20, 15.10] | 13.70 ± 10.00 [12.30, 15.20] | −0.10 | ||
| SF12-MS | Post-Op | Mann–Whitney | 9250 | 0.167 | 1.000 | 156 | 53.80 ± 13.50 [51.20, 55.80] | 55.90 ± 12.80 [54.70, 57.50] | −0.10 | |
| Improvement | t-test | 3 | 0.791 | 1.000 | 156 | 2.10 ± 14.00 [0.21, 3.51] | 1.70 ± 10.80 [0.09, 3.23] | 0.03 | ||
| Heat Index > 32 | VAS | Post-Op | Mann–Whitney | 3878 | 0.917 | 1.000 | 86 | 1.00 ± 3.80 [1.00, 2.00] | 1.00 ± 3.00 [1.00, 2.00] | 0.01 |
| Improvement | Mann–Whitney | 34,675 | 0.189 | 1.000 | 86 | −5.00 ± 5.00 [−6.00, −5.00] | −5.00 ± 4.50 [−6.00, −4.00] | −0.19 | ||
| SF12-PS | Post-Op | Mann–Whitney | 56,315 | 0.973 | 1.000 | 117 | 46.80 ± 16.70 [44.00, 51.50] | 47.00 ± 13.60 [44.30, 49.90] | −0.03 | |
| Improvement | t-test | 3 | 0.746 | 1.000 | 117 | 13.10 ± 10.60 [11.50, 14.20] | 12.60 ± 10.50 [10.90, 14.40] | 0.04 | ||
| SF12-MS | Post-Op | Mann–Whitney | 5102 | 0.846 | 1.000 | 108 | 54.40 ± 13.00 [51.50, 56.20] | 55.20 ± 14.50 [53.70, 57.50] | 0.00 | |
| Improvement | t-test | 7 | 0.503 | 1.000 | 108 | 1.60 ± 11.70 [−0.23, 2.49] | 0.60 ± 10.20 [−1.13, 2.35] | 0.09 | ||
| Heat Index > 41 | VAS | Post-Op | Mann–Whitney | 239 | 0.258 | 1.000 | 18 | 2.50 ± 5.20 [1.00, 4.00] | 2.00 ± 2.80 [0.00, 2.00] | 0.44 |
| Improvement | t-test | 2 | 0.855 | 1.000 | 18 | −4.30 ± 3.10 [−5.53, −3.20] | −4.50 ± 3.00 [−5.55, −3.36] | 0.06 | ||
| SF12-PS | Post-Op | t-test | 2 | 0.826 | 1.000 | 23 | 46.10 ± 9.80 [42.60, 49.00] | 45.50 ± 9.60 [41.90, 49.00] | 0.07 | |
| Improvement | t-test | 17 | 0.103 | 0.618 | 23 | 14.80 ± 8.60 [11.70, 13.40] | 10.30 ± 9.70 [6.74, 13.8] | 0.50 | ||
| SF12-MS | Post-Op | t-test | 1 | 0.932 | 1.000 | 19 | 49.30 ± 11.10 [44.90, 53.40] | 49.00 ± 9.70 [45.50, 52.50] | 0.03 | |
| Improvement | t-test | 8 | 0.457 | 1.000 | 19 | 1.50 ± 10.30 [−2.65, 3.41] | −0.70 ± 8.10 [−3.67, 2.27] | 0.24 | ||
| Day vs. Night | VAS | Post-Op | Mann–Whitney | 5794 | 0.849 | 1.000 | 105 | 1.00 ± 3.00 [1.00, 2.00] | 1.50 ± 4.00 [1.00, 2.00] | −0.12 |
| Improvement | Mann–Whitney | 5932 | 0.911 | 1.000 | 105 | −5.00 ± 5.00 [−5.00, −4.00] | −5.00 ± 5.00 [−6.00, −4.00] | −0.02 | ||
| SF12-PS | Post-Op | Mann–Whitney | 71,195 | 0.879 | 1.000 | 102 | 47.00 ± 15.80 [43.90, 49.00] | 45.20 ± 18.60 [42.40, 49.10] | 0.08 | |
| Improvement | t-test | −7 | 0.467 | 1.000 | 102 | 11.20 ± 11.30 [9.35, 14.10] | 12.30 ± 10.70 [10.70, 13.80] | −0.10 | ||
| SF12-MS | Post-Op | Mann–Whitney | 7445 | 0.811 | 1.000 | 106 | 55.80 ± 9.80 [54.00, 56.70] | 55.60 ± 14.50 [53.90, 56.70] | 0.04 | |
| Improvement | t-test | −16 | 0.116 | 0.696 | 106 | −0.80 ± 11.60 [−2.73, 3.53] | 1.70 ± 12.90 [−0.16, 3.48] | −0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milella, F.; Seveso, A.; Famiglini, L.; Banfi, G.; Cabitza, F. Detecting the Effect Size of Weather Conditions on Patient-Reported Outcome Measures (PROMs). J. Pers. Med. 2022, 12, 1811. https://doi.org/10.3390/jpm12111811
Milella F, Seveso A, Famiglini L, Banfi G, Cabitza F. Detecting the Effect Size of Weather Conditions on Patient-Reported Outcome Measures (PROMs). Journal of Personalized Medicine. 2022; 12(11):1811. https://doi.org/10.3390/jpm12111811
Chicago/Turabian StyleMilella, Frida, Andrea Seveso, Lorenzo Famiglini, Giuseppe Banfi, and Federico Cabitza. 2022. "Detecting the Effect Size of Weather Conditions on Patient-Reported Outcome Measures (PROMs)" Journal of Personalized Medicine 12, no. 11: 1811. https://doi.org/10.3390/jpm12111811