
High-Risk Siblings without Autism: Insights from a Clinical and Eye-Tracking Study
 , , and
, , and
Abstract
:1. Introduction
1.1. High-Risk Population for ASD
1.2. Eye-Tracking Studies Exploring Joint Attention
2. Methods
2.1. Study Population
2.2. Clinical Assessment
2.3. Stimuli and Procedure
- -
- No looking at the model’s face during the interactive segment, which could be considered a prerequisite for JA behavior;
- -
- Looking away from the computer screen for the entire JA phase.
2.4. Measures
2.5. Statistical Analyses
3. Results
3.1. Overall Looking Time on Screen
3.2. Initiating Joint Attention

{kind=link}
{kind=link}
{kind=link}
| Groups | Groups Comparison | Post-Hoc Comparisons | ||||||
|---|---|---|---|---|---|---|---|---|
| HR-noASD (N = 19) | ASD (N = 17) | TD (N = 16) | F | p Value | η2 | HR-noASD vs. ASD (p Value) | HR-noASD vs. TYP (p Value) | |
| IJA1 | ||||||||
| FD F (%) | 30.52 ± 31.18 | 29.65 ± 23.14 | 22.71 ± 17.76 | 0.059 | 0.94 | 0.003 | 0.74 | 0.85 |
| FD TO (%) | 22.73 ± 17.47 | 20.64 ± 11.91 | 27.72 ± 24.86 | 0.176 | 0.83 | 0.008 | 0.84 | 0.67 |
| FD NTO (%) | 9.03 ± 10.58 | 5.60 ± 5.30 | 6.76 ± 6.65 | 0.794 | 0.45 | 0.047 | 0.23 | 0.39 |
| Transitions TO → F | 2.37 ± 2.09 | 4.82 ± 2.74 | 3.06 ± 1.61 | 6.261 | 0.004 * | 0.218 | 0.002 * | 0.72 |
| Transitions F → TO | 2.72 ± 2.32 | 4.88 ± 2.78 | 4.31 ± 1.40 | 3.270 | 0.048 * | 0.140 | 0.016 * | 0.11 |
| Transitions NTO → F | 0.17 ± 0.39 | 0.75 ± 0.77 | 1.12 ± 1.25 | 4.210 | 0.02 * | 0.158 | 0.07 | 0.008 * |
| Transitions F → NTO | 0.08 ± 0.28 | 0.37 ± 0.61 | 0.62 ± 0.95 | 1.469 | 0.24 | 0.068 | 0.18 | 0.12 |
| Transitions TO → NTO | 1.09 ± 1.70 | 1.64 ± 1.53 | 2.93 ± 1.91 | 3.260 | 0.049 * | 0.140 | 0.10 | 0.015 * |
| Normalized Transition Score | 0.80 (0.38) | 0.56 ± 0.56 | 0.52 ± 0.45 | 2.289 | 0.11 | 0.096 | 0.17 | 0.04 * |
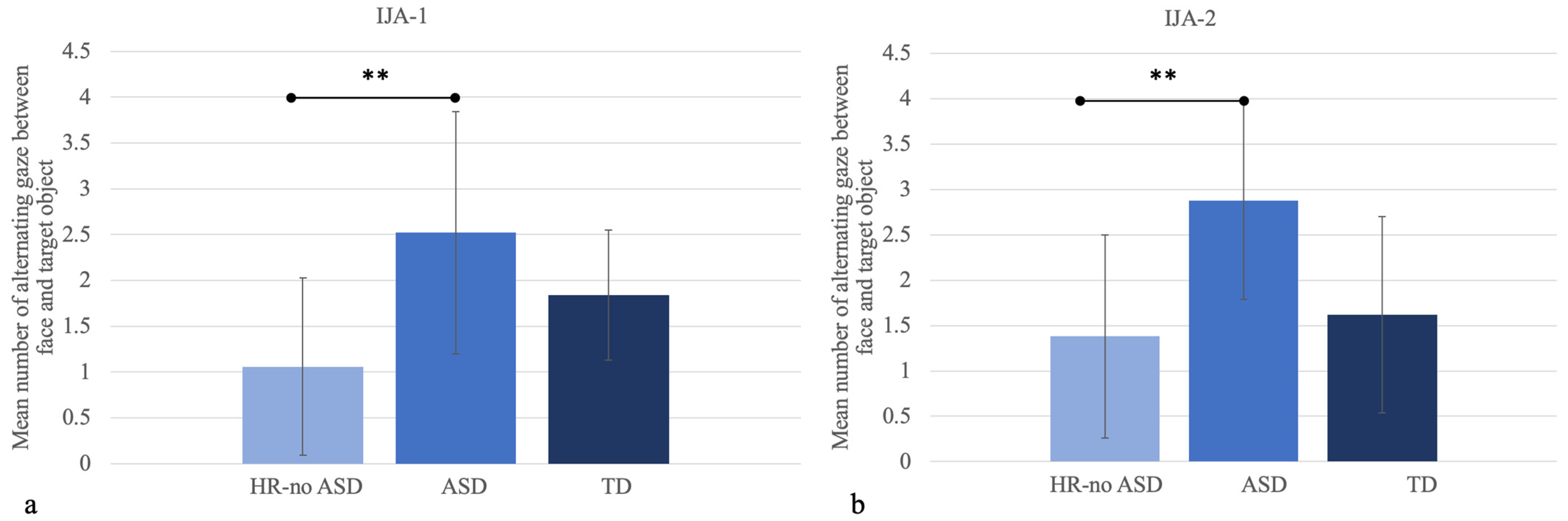
| Alternating gaze F ↔ TO | 1.06 ± 0.97 | 2.52 ± 1.32 | 1.84 ± 0.71 | 8.554 | 0.01 * | 0.800 | <0.001 ** | 0.13 |
| Alternating gaze F ↔ NTO | 0.05 ± 0.10 | 0.28 ± 0.30 | 0.43 ± 0.52 | 3.878 | 0.028 * | 0.150 | 0.06 | 0.012 * |
| Alternating gaze NTO ↔ TO | 0.19 ± 0.37 | 0.41 ± 0.38 | 0.73 ± 0.48 | 4.888 | 0.012 * | 0.178 | 0.10 | 0.003 * |
| Groups | Groups Comparison | Post-Hoc Comparisons | ||||||
|---|---|---|---|---|---|---|---|---|
| HR-noASD (N = 19) | ASD (N = 17) | TD (N = 16) | F | p Value | η2 | HR-noASD vs. ASD (p Value) | HR-noASD vs. TYP (p Value) | |
| IJA2 | ||||||||
| FD F (%) | 21.77 ± 18.62 | 24.28 ± 18.52 | 15.02 ± 11.25 | 0.202 | 0.82 | 0.009 | 0.76 | 0.69 |
| FD TO (%) | 22.60 ± 16.03 | 32.53 ± 17.61 | 36.07 ± 18.09 | 1.513 | 0.23 | 0.074 | 0.12 | 0.21 |
| Transitions TO → F | 2.82 ± 2.18 | 6.11 ± 2.17 | 3.71 ± 2.19 | 9.837 | <0.001 ** | 0.309 | <0.001 ** | 0.34 |
| Transitions F → TO | 3.83 ± 1.89 | 5.41 ± 2.37 | 3.71 ± 1.77 | 1.944 | 0.15 | 0.091 | 0.08 | 0.91 |
| Alternating gaze F ↔ TO | 1.38 ± 1.12 | 2.88 ± 1.09 | 1.62 ± 1.08 | 8.57 | 0.001 * | 0.272 | <0.001 ** | 0.62 |
3.3. Correlations between Eye-Tracking and Clinical Measures in HR-noASD and ASD
4. Discussion
Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maenner, M.J.; Shaw, K.A.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Esler, A.; Furnier, S.M.; Hallas, L.; Hall-Lande, J.; Hudson, A.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2018. MMWR Surveill. Summ. 2021, 70, 1–16. [Google Scholar] [CrossRef]
- Narzisi, A.; Posada, M.; Barbieri, F.; Chericoni, N.; Ciuffolini, D.; Pinzino, M.; Romano, R.; Scattoni, M.L.; Tancredi, R.; Calderoni, S.; et al. Prevalence of Autism Spectrum Disorder in a large Italian catchment area: A school-based population study within the ASDEU project. Epidemiol. Psychiatr. Sci. 2018, 29, e5. [Google Scholar] [CrossRef] [PubMed]
- Ozonoff, S.; Young, G.S.; Carter, A.; Messinger, D.; Yirmiya, N.; Zwaigenbaum, L.; Bryson, S.; Carver, L.J.; Constantino, J.N.; Dobkins, K. Recurrence risk for autism spectrum disorders: A Baby Siblings Research Consortium study. Pediatrics 2011, 128, e488–e495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grønborg, T.K.; Schendel, D.E.; Parner, E.T. Recurrence of autism spectrum disorders in fulland half-siblings and trends over time: A population-based cohort study. JAMA Pediatr. 2013, 167, 947–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, N.; Beam, A.; Agniel, D.; Eran, A.; Manrai, A.; Spettell, C.; Steinberg, G.; Mandl, K.; Fox, K.; Nelson, S.F.; et al. Association of Sex With Recurrence of Autism Spectrum Disorder Among Siblings. JAMA Pediatr. 2017, 171, 1107–1112. [Google Scholar] [CrossRef] [PubMed]
- Hansen, S.N.; Schendel, D.E.; Francis, R.W.; Windham, G.C.; Bresnahan, M.; Levine, S.Z.; Parner, E.T. Recurrence risk of autism in siblings and cousins: A multinational, population-based study. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 866–875. [Google Scholar] [CrossRef]
- Rogers, S.J. What are infant siblings teaching us about autism in infancy? Autism Res. 2009, 2, 125–137. [Google Scholar] [CrossRef] [Green Version]
- Libertus, K.; Sheperd, K.A.; Ross, S.W.; Landa, R.J. Limited fine motor and grasping skills in 6-month-old infants at high risk for autism. Child Dev. 2014, 85, 2218–2231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, E.J.; Gliga, T.; Bedford, R.; Charman, T.; Johnson, M.H. Developmental pathways to autism: A review of prospective studies of infants at risk. Neurosci. Biobehav. Rev. 2014, 39, 1–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salomone, E.; Shephard, E.; Milosavljevic, B.; Johnson, M.H.; Charman, T.; BASIS Team. Adaptive behaviour and cognitive skills: Stability and change from 7 months to 7 years in siblings at high familial risk of Autism Spectrum Disorder. J. Autism Dev. Disord. 2018, 48, 2901–2911. [Google Scholar] [CrossRef] [PubMed]
- Sucksmith, E.; Roth, I.; Hoekstra, R.A. Autistic traits below the clinical threshold: Re-examining the broader autism phenotype in the 21st century. Neuropsychol. Rev. 2011, 21, 360–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozonoff, S.; Young, G.S.; Belding, A.; Hill, M.; Hill, A.; Hutman, T.; Johnson, S.; Miller, M.; Rogers, S.J.; Schwichtenberg, A.J. The broader autism phenotype in infancy: When does it emerge? J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 398–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgiades, S.; Szatmari, P.; Zwaigenbaum, L.; Bryson, S.; Brian, J.; Roberts, W.; Smith, I.; Vaillancourt, T.; Roncadin, C.; Garon, N. A prospective study of autistic-like traits in unaffected siblings of probands with autism spectrum disorder. JAMA Psychiatry 2013, 70, 42–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messinger, D.; Young, G.S.; Ozonoff, S.; Dobkins, K.; Carter, A.; Zwaigenbaum, L.; Landa, R.J.; Charman, T.; Stone, W.L.; Constantino, J.N. Beyond autism: A baby siblings research consortium study of high-risk children at three years of age. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 300–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.; Young, G.S.; Hutman, T.; Johnson, S.; Schwichtenberg, A.J.; Ozonoff, S. Early pragmatic language difficulties in siblings of children with autism: Implications for DSM-5 social communication disorder? J. Child Psychol. Psychiatry 2015, 56, 774–781. [Google Scholar] [CrossRef] [Green Version]
- Shephard, E.; Milosavljevic, B.; Pasco, G.; Jones, E.J.; Gliga, T.; Happé, F.; Johnson, M.H.; Charman, T.; BASIS Team. Mid-childhood outcomes of infant siblings at familial high-risk of autism spectrum disorder. Autism Res. 2017, 10, 546–557. [Google Scholar] [CrossRef] [Green Version]
- Wagner, J.B.; Luyster, R.J.; Moustapha, H.; Tager-Flusberg, H.; Nelson, C.A. Differential attention to faces in infant siblings of children with autism spectrum disorder and associations with later social and language ability. Int. J. Behav. Dev. 2018, 42, 83–92. [Google Scholar] [CrossRef]
- Webb, S.J.; Jones, E.J.; Merkle, K.; Namkung, J.; Toth, K.; Greenson, J.; Dawson, G. Toddlers with elevated autism symptoms show slowed habituation to faces. Child Neuropsychol. 2010, 16, 255–278. [Google Scholar] [CrossRef] [Green Version]
- Rankin, J.A.; Tomeny, T.S. Screening of Broader Autism Phenotype Symptoms in Siblings: Support for a Distinct Model of Symptomatology. J. Autism Dev. Disord. 2019, 49, 4686–4690. [Google Scholar] [CrossRef]
- Loth, E.; Charman, T.; Mason, L.; Tillmann, J.; Jones, E.J.; Wooldridge, C.; Buitelaar, J.K. The EU-AIMS Longitudinal European Autism Project (LEAP): Design and methodologies to identify and validate stratification biomarkers for autism spectrum disorders. Mol. Autism 2017, 8, 24. [Google Scholar] [CrossRef]
- Tang, W.Y.F. Application of Eye Tracker to Detect Visual Processing of Children with Autism Spectrum Disorders. Curr. Dev. Disord. Rep. 2022. [Google Scholar] [CrossRef]
- Bölte, S.; Marschik, P.B.; Falck-Ytter, T.; Charman, T.; Roeyers, H.; Elsabbagh, M. Infants at risk for autism: A European perspective on current status, challenges and opportunities. Eur. Child Adolesc. Psychiatry 2013, 22, 341–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gredebäck, G.; Johnson, S.; von Hofsten, C. Eye tracking in infancy research. Dev. Neuropsychol. 2009, 35, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Falck-Ytter, T.; Bölte, S.; Gredebäck, G. Eye tracking in early autism research. J. Neurodev. Disord. 2013, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, J.; Dissanayake, C. Autism spectrum disorders in infancy and toddlerhood: A review of the evidence on early signs, early identification tools, and early diagnosis. J. Dev. Behav. Pediatr. 2009, 30, 447–459. [Google Scholar] [CrossRef]
- Bedford, R.; Elsabbagh, M.; Gliga, T.; Pickles, A.; Senju, A.; Charman, T.; Johnson, M.H. Precursors to social and communication difficulties in infants at-risk for autism: Gaze following and attentional engagement. J. Autism Dev. Disord. 2012, 42, 2208–2218. [Google Scholar] [CrossRef]
- Falck-Ytter, T.; Fernell, E.; Hedvall, Å.L.; von Hofsten, C.; Gillberg, C. Gaze performance in children with autism spectrum disorder when observing communicative actions. J. Autism Dev. Disord. 2012, 42, 2236–2245. [Google Scholar] [CrossRef]
- Billeci, L.; Narzisi, A.; Campatelli, G.; Crifaci, G.; Calderoni, S.; Gagliano, A.; Calzone, C.; Colombi, C.; Pioggia, G.; Muratori, F.; et al. Disentangling the initiation from the response in joint attention: An eye-tracking study in toddlers with autism spectrum disorders. Transl. Psychiatry 2016, 6, e808. [Google Scholar] [CrossRef] [Green Version]
- Thorup, E.; Nyström, P.; Gredebäck, G.; Bölte, S.; Falck-Ytter, T. Altered gaze following during live interaction in infants at risk for autism: An eye tracking study. Mol. Autism 2016, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Thorup, E.; Nyström, P.; Gredebäck, G.; Bölte, S.; Falck-Ytter, T.; EASE Team. Reduced Alternating Gaze During Social Interaction in Infancy is Associated with Elevated Symptoms of Autism in Toddlerhood. J. Abnorm. Child Psychol. 2018, 46, 1547–1561. [Google Scholar] [CrossRef]
- Gammer, I.; Bedford, R.; Elsabbagh, M.; Garwood, H.; Pasco, G.; Tucker, L.; Volein, A.; Johnson, M.H.; Charman, T.; BASIS Team. Behavioural markers for autism in infancy: Scores on the Autism Observational Scale for Infants in a prospective study of at-risk siblings. Infant Behav. Dev. 2015, 38, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Ruzich, E.; Allison, C.; Smith, P.; Watson, P.; Auyeung, B.; Ring, H.; Baron-Cohen, S. Subgrouping siblings of people with autism: Identifying the broader autism phenotype. Autism Res. 2016, 9, 658–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule Second Edition (ADOS-2) Manual (Part 1): Modules 1–4; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Huntley, M. The Griffiths Mental Developmental Scales from Birth to 2 Years, Manual; The 1996 Revision, Revised; The Test Agency Ltd.: Oxford, UK, 1996. [Google Scholar]
- Luiz, D.; Barnard, A.; Knoesen, N.; Kotras, N.; Horrocks, S.; McAlinden, P.; Challis, D.; O’Connell, R. GMDS-ER 2–8—Griffiths Mental Development Scales—Extended Revised: 2 to 8 Years; Cianchetti, C., Fancello, G.S., Eds.; Giunti: Firenze, Italy, 2006. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule-WPS Edition; Western & Psychological Services: Los Angeles, CA, USA, 2002. [Google Scholar]
- Gotham, K.; Risi, S.; Dawson, G.; Tager-Flusberg, H.; Joseph, R.; Carter, A.; Hepburn, S.; McMahon, W.; Rodier, P.; Hyman, S.L. Replication of the Autism Diagnostic Observation Schedule (ADOS) Revised Algorithms. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 642–651. [Google Scholar] [CrossRef] [Green Version]
- Gotham, K.; Pickles, A.; Lord, C. Standardizing ADOS Scores for a Measure of Severity in Autism Spectrum Disorders. J. Autism. Dev. Disord. 2009, 39, 693–705. [Google Scholar] [CrossRef] [Green Version]
- Luyster, R.; Gotham, K.; Guthrie, W.; Coffing, M.; Petrak, R.; Pierce, K.; Bishop, S.; Esler, A.; Hus, V.; Oti, R. The Autism Diagnostic Observation Schedule—Toddler Module: A new module of a standardized diagnostic measure for autism spectrum disorders. J. Autism. Dev. Disord. 2009, 39, 1305–1320. [Google Scholar] [CrossRef] [Green Version]
- Esler, A.N.; Bal, V.H.; Guthrie, W.; Wetherby, A.; Ellis Weismer, S.; Lord, C. The Autism Diagnostic Observation Schedule, Toddler Module: Standardized Severity Scores. J. Autism. Dev. Disord. 2015, 45, 2704–2720. [Google Scholar] [CrossRef] [Green Version]
- Hus, V.; Gotham, K.; Lord, C. Standardizing ADOS Domain Scores: Separating Severity of Social Affect and Restricted and Repetitive Behaviors. J. Autism. Dev. Disord. 2014, 44, 2400–2412. [Google Scholar] [CrossRef] [Green Version]
- Sparrow, S.S.; Balla, D.A.; Cicchetti, D.V. Vineland-II: Vineland Adaptive Behavior Scales; [VABS]; Survey Forms Manual; A revision of the Vineland Social Maturity Scale; Pearson Assessments: San Antonio, TX, USA, 2005. [Google Scholar]
- Rutter, M.; Bailey, A.; Lord, C. The Social Communication Questionnaire: Manual; Western Psychological Services: Torrance, CA, USA, 2003. [Google Scholar]
- Marvin, A.R.; Marvin, D.J.; Lipkin, P.H.; Law, J.K. Analysis of Social Communication Questionnaire (SCQ) Screening for Children Less Than Age 4. Curr. Dev. Disord. Rep. 2017, 4, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Fenson, L. The MacArthur Communicative Development Inventories: User’s Guide and Technical Manual (Brookes, Baltimore, MD), 2nd ed.; Brookes Publishing: Baltimore, MA, USA, 1993. [Google Scholar]
- Charman, T. Why is joint attention a pivotal skill in autism? Philosophical Trans. R. Soc. Lond. B Biol. Sci. 2003, 358, 315–324. [Google Scholar] [CrossRef]
- Dawson, G.; Toth, K.; Abbott, R.; Osterling, J.; Munson, J.; Estes, A.; Liaw, J. Early social attention impairments in autism: Social orienting, joint attention, and attention in autism. Dev. Psychol. 2004, 40, 271–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobson, J.; Hobson, R.P. Identification: The missing link between joint attention and imitation. Dev. Psychopathol. 2007, 19, 411–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyström, P.; Thorup, E.; Bölte, S.; Falck-Ytter, T. Joint attention in infancy and the emergence of autism. Biol. Psychiatry 2019, 86, 631–638. [Google Scholar] [CrossRef] [Green Version]
- Falck-Ytter, T.; Thorup, E.; Bölte, S. Brief report: Lack of processing bias for the objects other people attend to in 3-year-olds with autism. J. Autism Dev. Disord. 2015, 45, 1897–1904. [Google Scholar] [CrossRef] [Green Version]
- Messinger, D.S.; Young, G.S.; Webb, S.J.; Ozonoff, S.; Bryson, S.E.; Carter, A.; Carver, L.; Charman, T.; Chawarska, K.; Curtin, S. Early sex differences are not autism-specific: A Baby Siblings Research Consortium (BSRC) study. Mol. Autism 2015, 6, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charman, T.; Young, G.S.; Brian, J.; Carter, A.; Carver, L.J.; Chawarska, K.; Curtin, S.; Dobkins, K.; Elsabbagh, E.; Georgiades, S.; et al. Non-ASD outcomes at 36 months in siblings at familial risk for autism spectrum disorder (ASD): A baby siblings research consortium (BSRC) study. Autism Res. 2017, 10, 169–178. [Google Scholar] [CrossRef] [Green Version]
- Girault, J.B.; Swanson, M.R.; Meera, S.S.; Grzadzinski, R.L.; Shen, M.D.; Burrows, C.A.; Wolff, J.J.; Pandey, J.; St John, T.; Estes, A.; et al. Quantitative trait variation in ASD probands and toddler sibling outcomes at 24 months. J. Neurodev. Disord. 2020, 12, 5. [Google Scholar] [CrossRef] [Green Version]
- Ozonoff, S.; Young, G.S.; Brian, J.; Charman, T.; Shephard, E.; Solish, A.; Zwaigenbaum, L. Diagnosis of Autism Spectrum Disorder after Age 5 in Children Evaluated Longitudinally Since Infancy. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 849–857. [Google Scholar] [CrossRef]
- Loh, A.; Soman, T.; Brian, J.; Bryson, S.E.; Roberts, W.; Szatmari, P.; Smith, I.M.; Zwaigenbaum, L. Stereotyped motor behaviors associated with autism in high-risk infants: A pilot videotape analysis of a sibling sample. J. Autism Dev. Disord. 2007, 37, 25–36. [Google Scholar] [CrossRef]
- Christensen, L.; Hutman, T.; Rozga, A.; Young, G.S.; Ozonoff, S.; Rogers, S.J.; Baker, B.; Sigman, M. Play and developmental outcomes in infant siblings of children with autism. J. Autism Dev. Disord. 2010, 40, 946–957. [Google Scholar] [CrossRef]
- Damiano, C.R.; Nahmias, A.; Hogan-Brown, A.L.; Stone, W.L. What do repetitive and stereotyped movements mean for infant siblings of children with autism spectrum disorders? J. Autism Dev. Disord. 2013, 43, 1326–1335. [Google Scholar] [CrossRef] [Green Version]
- Elison, J.T.; Wolff, J.J.; Reznick, J.S.; Botteron, K.N.; Estes, A.M.; Gu, H.; Hazlett, H.C.; Meadows, A.J.; Paterson, S.J.; Zwaigenbaum, L.; et al. Repetitive behavior in 12-month-olds later classified with autism spectrum disorder. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 1216–1224. [Google Scholar] [CrossRef] [Green Version]
- Zwaigenbaum, L.; Bryson, S.; Rogers, T.; Roberts, W.; Brian, J.; Szatmari, P. Behavioral manifestations of autism in the first year of life. Int. J. Dev. Neurosci. 2005, 23, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Rozga, A.; Hutman, T.; Young, G.S.; Rogers, S.J.; Ozonoff, S.; Dapretto, M.; Sigman, M. Behavioral profiles of affected and unaffected siblings of children with autism: Contribution of measures of mother–infant interaction and nonverbal communication. J. Autism Dev. Disord. 2011, 41, 287–301. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, W.A.; Jarvis, K.L.; Osann, K.; Laulhere, T.M.; Straub, C.; Thomas, E.; Filipek, P.; Spence, M.A. Brief report: Early social communication behaviors in the younger siblings of children with autism. J. Autism Dev. Disord. 2005, 35, 657–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrus, N.; Hall, L.P.; Paterson, S.J.; Elison, J.T.; Wolff, J.J.; Swanson, M.R.; Parish-Morris, J.; Eggebrecht, A.T.; Pruett, J.R., Jr.; Hazlett, H.C.; et al. IBIS Network. Language delay aggregates in toddler siblings of children with autism spectrum disorder. J. Neurodev. Disord. 2018, 10, 29. [Google Scholar] [CrossRef] [PubMed]
- Landa, R.J.; Gross, A.L.; Stuart, E.A.; Bauman, M. Latent class analysis of early developmental trajectory in baby siblings of children with autism. J. Child Psychol. Psychiatry 2012, 53, 986–996. [Google Scholar] [CrossRef] [Green Version]
- Garrido, D.; Petrova, D.; Watson, L.R.; Garcia-Retamero, R.; Carballo, G. Language and motor skills in siblings of children with autism spectrum disorder: A meta-analytic review. Autism Res. 2017, 10, 1737–1750. [Google Scholar] [CrossRef]
- Chita-Tegmark, M.; Arunachalam, S.; Nelson, C.A.; Tager-Flusberg, H. Eye-tracking measurements of language processing: Developmental differences in children at high risk for ASD. J. Autism Dev. Disord. 2015, 45, 3327–3338. [Google Scholar] [CrossRef] [Green Version]
- Iverson, J.M. Early Motor and Communicative Development in Infants With an Older Sibling With Autism Spectrum Disorder. J. Speech Lang. Hear. Res. 2018, 61, 2673–2684. [Google Scholar] [CrossRef]
- Hendry, A.; Jones, E.J.; Bedford, R.; Gliga, T.; Charman, T.; Johnson, M.H. Developmental change in look durations predicts later effortful control in toddlers at familial risk for ASD. J. Neurodev. Disord. 2018, 10, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyström, P.; Bölte, S.; Falck-Ytter, T.; EASE Team. Responding to Other People’s Direct Gaze: Alterations in Gaze Behavior in Infants at Risk for Autism Occur on Very Short Timescales. J. Autism Dev. Disord. 2017, 47, 3498–3509. [Google Scholar] [CrossRef] [PubMed]
- Falck-Ytter, T.; Rehnberg, E.; Bölte, S. Lack of visual orienting to biological motion and audiovisual synchrony in 3-year-olds with autism. PLoS ONE 2013, 8, e68816. [Google Scholar] [CrossRef] [PubMed]
- Falck-Ytter, T.; Nyström, P.; Gredebäck, G.; Gliga, T.; Bölte, S. Reduced orienting to audiovisual synchrony in infancy predicts autism diagnosis at three years of age. J. Child Psychol. Psychiatry 2018, 59, 872–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, C.E.; Baron-Cohen, S. Sensory perception in autism. Nat. Rev. Neurosci. 2017, 18, 671. [Google Scholar] [CrossRef]
- Donaldson, C.K.; Stauder, J.E.A.; Donkers, F.C.L. Increased sensory processing atypicalities in parents.of multiplex ASD families versus typically developing and simplex ASD families. J. Autism Dev. Disord. 2017, 47, 535–548. [Google Scholar] [CrossRef] [Green Version]
- Brian, J.; Bryson, S.E.; Garon, N.; Roberts, W.; Smith, I.M.; Szatmari, P.; Zwaigenbaum, L. Clinical assessment of autism in high-risk 18-month-olds. Autism 2008, 12, 433–456. [Google Scholar] [CrossRef]
- Shah, A.; Frith, U. An islet of ability in autistic children: A research note. J. Child Psychol. Psychiatry 1983, 24, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Gangi, D.N.; Schwichtenberg, A.; Iosif, A.-M.; Young, G.S.; Baguio, F.; Ozonoff, S. Gaze to faces across interactive contexts in infants at heightened risk for autism. Autism 2018, 22, 763–768. [Google Scholar] [CrossRef]
- Pellicano, E.; Burr, D. When the world becomes ‘too real’: A Bayesian explanation of autistic perception. Trends Cogn. Sci. 2012, 16, 504–510. [Google Scholar] [CrossRef]
- Schmitz, C.; Martineau, J.; Barthélémy, C.; Assaiante, C. Motor control and children with autism: Deficit of anticipatory function? Neurosci. Lett. 2003, 348, 17–20. [Google Scholar] [CrossRef]
- Cattaneo, L.; Fabbri-Destro, M.; Boria, S.; Pieraccini, C.; Monti, A.; Cossu, G.; Rizzolatti, G. Impairment of actions chains in autism and its possible role in intention understanding. Proc. Natl. Acad. Sci. USA 2007, 104, 17825–17830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boria, S.; Fabbri-Destro, M.; Cattaneo, L.; Sparaci, L.; Sinigaglia, C.; Santelli, E.; Cossu, G.; Rizzolatti, G. Intention understanding in autism. PLoS ONE 2009, 4, e5596. [Google Scholar] [CrossRef]
- Sinha, P.; Kjelgaard, M.M.; Gandhi, T.K.; Tsourides, K.; Cardinaux, A.L.; Pantazis, D.; Diamond, S.P.; Held, R.M. Autism as a disorder of prediction. Proc. Natl. Acad. Sci. USA 2014, 111, 15220–15225. [Google Scholar]
- Bradshaw, J.; Shic, F.; Holden, A.N.; Horowitz, E.J.; Barrett, A.C.; German, T.C.; Vernon, T.W. The use of eye tracking as a biomarker of treatment outcome in a pilot randomized clinical trial for young children with autism. Autism Res. 2019, 12, 779–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muratori, F.; Billeci, L.; Calderoni, S.; Boncoddo, M.; Lattarulo, C.; Costanzo, V.; Turi, M.; Colombi, C.; Narzisi, A. How attention to faces and objects changes over time in toddlers with autism spectrum disorders: Preliminary evidence from an eye tracking study. Brain Sci. 2019, 9, 344. [Google Scholar] [CrossRef]



| Groups | Group Comparison | Post-Hoc Comparisons | ||||||
|---|---|---|---|---|---|---|---|---|
| HR-noASD (N = 19) | ASD (N = 17) | TD (N = 16) | Comparison Coefficient | p Value | HR-noASD vs. ASD (p Value) | HR-noASD vs. TD (p Value) | ASD vs. TD (p Value) | |
| Gender | ||||||||
| Boy:Girl | 12:7 | 13:4 | 10:6 | Χ2 = 0.965 | 0.617 | - | - | - |
| Age (Months) | ||||||||
| Mean Age ± SD | 22.63 ± 4.87 | 24.65 ± 4.24 | 24.88 ± 4.56 | F = 1.312 | 0.279 | 0.580 | 0.465 | 1.000 |
| Age Range | 18–33 | 18–30 | 18–30 | - | - | - | - | - |
| PQ (GMDS-ER) N = 17 N = 17 N = 16 | ||||||||
| Mean PQ ± SD | 88.59 ± 25.71 | 84.18 ± 22.08 | 110.75 ± 17.43 | F = 6.384 | 0.004 | 1.000 | 0.023 * | 0.005 * |
| Range PQ | 35–119 | 35–130 | 83–162 | - | - | - | - | - |
| SCQ (last 3 months) | N = 13 | N = 17 | - | |||||
| Raw Score ± SD (range) | 5.08 ± 3.84 (2–16) | 12.18 ± 4.42 (3–20) | - | t = 4.6 | 0.0002 ** | - | - | - |
| ADOS | N = 14 | N = 17 | ||||||
| Total CSS ± SD (range) | 1.71 ± 0.91 (1–4) | 6.59 ± 1.42 (4–9) | - | t = 11.1 | 0.0001 ** | - | - | - |
| SA-CSS ± SD (range) | 1.43 ± 0.65 (1–3) | 6.71 ± 1.53 (3–10) | - | t = 12.02 | 0.0001 ** | - | - | - |
| RRB-CSS ± SD (range) | 4.57 ± 2.79 (1–9) | 6.47 ± 2.87 (1–10) | - | t = 1.85 | 0.73 | - | - | - |
| VABS-II | N = 12 | N = 14 | ||||||
| ABC Score ± SD (range) | 95.50 ± 15.39 (58–115) | 79.54 ± 6.51 (70–95) | - | t = 3.42 | 0.02 * | - | - | - |
| Communication Score ± SD (range) | 93.75 ± 11.33 (71–115) | 70.36 ± 16.48 (21–90) | - | t = 4.14 | 0.0003 ** | - | - | - |
| Daily Living Skills Score ± SD (range) | 96.42 ± 21.07 (43–121) | 82.50 ± 16.5 (35–103) | - | t = 1.65 | 0.11 | - | - | - |
| Socialization Score ± SD (range) | 96.08 ± 18.74 (44–113) | 74.07 ± 15.69 (44–94) | - | t = 3.26 | 0.003 * | - | - | - |
| Motor Score ± SD (range) | 98.00 ± 11.42 (85–110) | 90.71 ± 15.12 (72–109) | - | t = 1.36 | 0.18 | - | - | - |
| MacArthur-CDI | N = 13 | N = 17 | ||||||
| Words Understood Raw Score ± SD (range) | 231.62 ± 94.6 (0–349) | 106.82 ± 92.16 (55–270) | - | t = 3.62 | 0.001 | - | - | - |
| Words Produced Raw Score ± SD (range) | 78.38 ± 89.80 (1–290) | 11.47 ± 19.65 (0–80) | - | t = 2.99 | p = 0.005 | - | - | - |
| Gestures Raw Score ± SD (range) | 52.23 ± 22.12 (22–115) | 26.06 ± 13.42 (7–47) | - | t = 4.01 | p = 0.0002 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costanzo, V.; Narzisi, A.; Cerullo, S.; Crifaci, G.; Boncoddo, M.; Turi, M.; Apicella, F.; Tancredi, R.; Muratori, F.; Calderoni, S.; et al. High-Risk Siblings without Autism: Insights from a Clinical and Eye-Tracking Study. J. Pers. Med. 2022, 12, 1789. https://doi.org/10.3390/jpm12111789
Costanzo V, Narzisi A, Cerullo S, Crifaci G, Boncoddo M, Turi M, Apicella F, Tancredi R, Muratori F, Calderoni S, et al. High-Risk Siblings without Autism: Insights from a Clinical and Eye-Tracking Study. Journal of Personalized Medicine. 2022; 12(11):1789. https://doi.org/10.3390/jpm12111789
Chicago/Turabian StyleCostanzo, Valeria, Antonio Narzisi, Sonia Cerullo, Giulia Crifaci, Maria Boncoddo, Marco Turi, Fabio Apicella, Raffaella Tancredi, Filippo Muratori, Sara Calderoni, and et al. 2022. "High-Risk Siblings without Autism: Insights from a Clinical and Eye-Tracking Study" Journal of Personalized Medicine 12, no. 11: 1789. https://doi.org/10.3390/jpm12111789