
Prevalence of Anal High-Risk Human Papilloma Virus Infection and Abnormal Anal Cytology among Women Living with HIV
 ,
,
Abstract
:1. Introduction
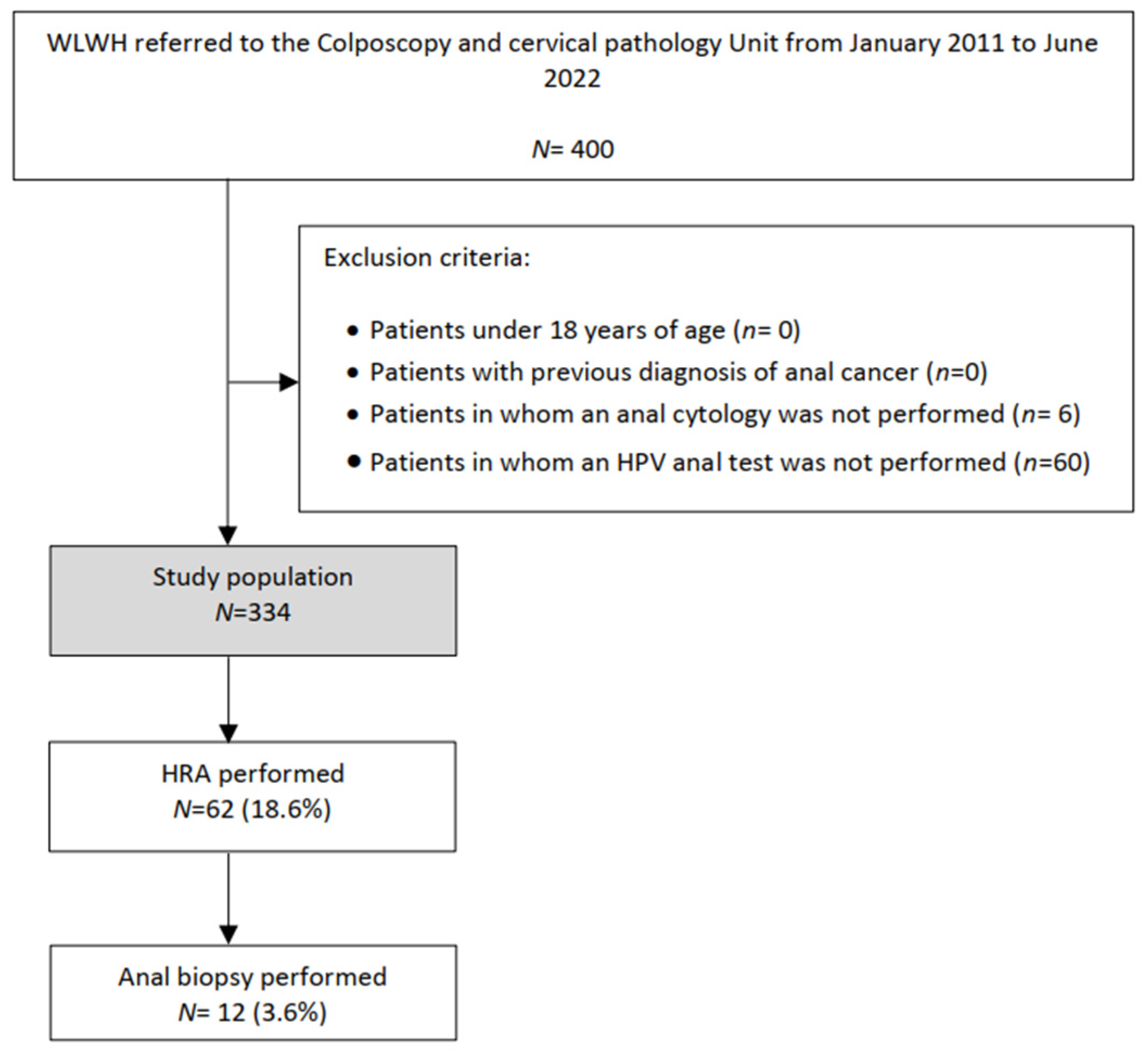
2. Materials and Methods
2.1. Sampling Procedures
2.2. Management of Abnormal Results
2.3. Statistical Analysis
3. Results

{kind=link}
| Characteristics | Values |
|---|---|
| Age, years | |
| Mean (SD) | 47.1 (8.6) |
| Median (IQR) | 48.0 (42.0; 53.0) |
| Age, years | |
| <35 | 38 (11.4) |
| 35–50 | 171 (51.2) |
| >50 | 125 (37.4) |
| Postmenopausal NR: 11 | 141 (43.7) |
| Parity | |
| NR: 41 | |
| Mean (SD) | 1.5 (1.1) |
| Median (IQR) | 1.0 (1.0; 2.0) |
| HIV infection time, years | |
| ≤2 | 34 (10.9) |
| 3–9 | 38 (12.3) |
| ≥10 NR: 24 | 238 (76.8) |
| HIV viral load level, copies/mL | |
| <50 | 287 (89.1) |
| 50–400 | 16 (5.0) |
| >400 NR:12 | 19 (5.9) |
| CD4+ level, cells/µL | |
| ≤200 | 21(6.8) |
| 201–500 | 74 (24.1) |
| >500 NR: 41 | 212 (69.1) |
| Currently taking antiretroviral therapy NR: 7 | 317 (96.4) |
| Time of antiretroviral therapy, years | |
| ≤2 | 40 (12.8) |
| 3–9 | 53 (17.0) |
| ≥10 NR:22 | 219 (70.2) |
| Characteristics | Values |
|---|---|
| Previous cervical cancer screening | 297 (89.0) |
| HPV vaccination NR: 15 | 14 (4.4) |
| Previous HSIL | 124 (37.1) |
| Vulvar | 16 (4.8) |
| Vaginal | 5 (1.4) |
| Cervical | 81 (24.3) |
| Smoking | |
| Current Smoker | 150 (46.7) |
| Former user | 59 (18.4) |
| Never used NR: 13 | 112 (34.9) |
| Age of first sexual intercourse, years | |
| NR: 72 | |
| Mean (SD) | 17.8 (10.1) |
| Median (IQR) | 17.0 (16.0;18.0) |
| Number of sexual partners in the last three years | |
| NR: 57 | |
| Mean (SD) | 1.1 (1.1) |
| Median (IQR) | 1.1 (1.0;1.0) |
| Stable partner NR: 36 | 186 (62.4) |
| Anal sex NR: 101 | 59 (25.3) |
| Hormonal contraceptives NR: 85 | |
| Current user | 10 (4.0) |
| Former user | 67 (26.9) |
| Never used | 172 (69.1) |
| Barrier contraceptive user NR: 65 | 140 (52.0) |
| IUD user NR: 15 | 15 (4.7) |
| Previous STD NR: 14 | 134 (41.9) |
| HCV co-infection | 102 (31.9) |
| Characteristics | Location | |
|---|---|---|
| Anal | Cervical | |
| Cytology | ||
| NILM, HPV not available | - | 19 (5.7) |
| NILM, HPV negative | 141 (42.2) | 167 (50.0) |
| NILM, HR-HPV positive | 61 (18.3) | 49 (14.7) |
| ASCUS | 107 (32.0) | 54 (16.2) |
| ACG | 0 (0.0) | 1 (0.3) |
| L-SIL | 17 (5.1) | 30 (9.0) |
| ASC-H | 3 (0.9) | 3 (0.9) |
| H-SIL | 4 (1.2) | 6 (1.8) |
| Carcinoma | 1 (0.3) | 0 (0.0) |
| Not available | - | 5 (1.5) |
| HPV test | ||
| Negative | 167 (50.0) | 186 (61.6) |
| Positive, low risk | 33 (9.9) | 22 (7.3) |
| Positive, high risk | 95 (28.4) | 68 (22.5) |
| Positive, Low and High risk | 39 (11.7) | 26 (8.6) |
| Not available | - | 32 |
| HPV 16 positive | 33 (9.9) | 23 (6.9) |
| HRA | 62 (18.6) | - |
| Negative | 52 (83.9) | |
| G1 | 7 (11.3) | |
| G2 | 3 (4.8) | |
| Biopsy a | 12 (3.6) | 34 (10.2) |
| Negative | 4 (33.3) | 9 (26.5) |
| LSIL | 6 (50.0) | 13 (38.2) |
| HSIL | 2 (16.7) | 12 (35.3) |
| Characteristics | Abnormal Cytology | High Risk HPV Infection | ||||
|---|---|---|---|---|---|---|
| No | Yes | p-Value | No | Yes | p-Value | |
| Age, years | 0.08 | 0.059 | ||||
| <35 | 29 (14.4) | 9 (6.8) | 16 (8.0) | 22 (16.4) | ||
| 35–50 | 97 (48.0) | 74 (56.1) | 107 (53.5) | 64 (47.8) | ||
| >50 | 76 (37.6) | 49 (37.1) | 77 (38.5) | 48 (35.8) | ||
| Postmenopausal | 84 (42.2) | 57 (46.0) | 0.5 | 83 (42.6) | 58 (45.3) | 0.626 |
| HIV infection time, years | 0.85 | <0.001 | ||||
| ≤2 | 19 (10.2) | 15 (12.2) | 12 (6.4) | 22 (17.9) | ||
| 3–9 | 23 (12.3) | 15 (12.2) | 29 (10.6) | 19 (15.5) | ||
| ≥10 | 145 (77.5) | 93 (75.6) | 156 (83.4) | 82 (66.7) | ||
| HIV viral load level, copies/mL | 0.4 | 0.037 | ||||
| <50 | 175 (90.7) | 112 (86.8) | 176 (91.7) | 111(85.4) | ||
| 50–400 | 9 (4.7) | 7 (5.4) | 10 (5.2) | 6 (4.6) | ||
| >400 | 9 (4.7) | 10 (7.6) | 6 (3.1) | 13 (10.0) | ||
| CD4+ level, copies/mL | 0.28 | 0.002 | ||||
| ≤200 | 10 (5.4) | 11 (9.1) | 7 (3.7) | 14 (11.9) | ||
| 201–500 | 42 (22.6) | 32 (26.5) | 39 (20.6) | 35 (29.6) | ||
| ≥500 | 134 (72.0) | 78 (64.5) | 143 (75.7) | 69 (58.5) | ||
| Current taking antiretroviral therapy | 188 (96.4) | 129 (97.7) | 0.7 F | 193 (98.0) | 124 (95.4) | 0.204 F |
| Time of antiretroviral therapy, years | 0.652 | 0.017 | ||||
| ≤2 | 24 (12.7) | 16 (12.9) | 16 (8.5) | 24 (19.5) | ||
| 3–9 | 29 (15.4) | 24 (19.4) | 33 (17.5) | 20 (16.3) | ||
| ≥10 | 135 (71.8) | 84 (67.7) | 140 (74.1) | 79 (64.2) | ||
| Smoking | 122 (63.2) | 87 (68.0) | 0.3 | 126 (64.3) | 83 (66.4) | 0.698 |
| Age of first sexual intercourse, years | 18.4 (1.0) | 16.9 (0.2) | 0.249 | 18.3 (1.0) | 17.1 (0.2) | 0.3317 |
| Number of sexual partners in the last three years | 1.1 (0.1) | 1.0(0.1) | 0.38 | 0.9 (0.5) | 1.2 (0.1) | 0.17 |
| Anal Sex | 34 (23.8) | 25 (27.8) | 0.494 | 40 (20.2) | 19 (20.9) | 0.212 |
| Previous STD | 76 (39.4) | 58 (45.7) | 0.264 | 77 (39.7) | 57 (45.2) | 0.32 |
| HCV co-infection | 58 (28.7) | 44 (33.3) | 0.370 | 59 (29.5) | 43 (32.1) | 0.615 |
| Previous cervical H-SIL | 44 (21.8) | 37 (28.0) | 0.193 | 45 (22.5) | 36 (36.9) | 0.362 |
| Current High risk HPV cervical infection | 54 (28.4) | 40 (35.7) | 0.186 | 31 (17.4) | 63 (50.8) | <0.001 |
| HPV 16 cervical infection | 14 (6.9) | 9 (6.8) | 0.968 | 11 (5.5) | 12 (9.0) | 0.222 |
| Characteristics | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| 0R (95% CI) | p-Value | 0R (95% CI) | p-Value | |
| HIV infection time, years | 0.6 (0.38; 0.98) | <0.001 | 0.6 (0.28; 1.16) | 0.124 |
| HIV viral load level, copies/mL | 0.5 (0.06;0.94) | 0.026 | 1.2 (0.7; 2.13) | 0.476 |
| CD4+ level, copies/mL | 0.7 (0.29; 0.97) | 0.001 | 0.7 (0.41; 1.11) | 0.127 |
| Time of antiretroviral therapy, years | 0.4 (0. 09; 0.72) | 0.012 | 1.4 (0.7; 2.72) | 0.346 |
| Current High risk HPV cervical infection | 1.6 (1.06; 2.11) | <0.001 | 5.1 (2.8; 9.18) | <0.001 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ART | antiretroviral therapy |
| ASC-H | atypical squamous cells, cannot rule out high-grade squamous intraepithelial lesion. |
| ASCUS | atypical squamous cells of undetermined significance. |
| CI | confidence intervals |
| HCV | hepatitis C viral |
| HIV | human immunodeficiency virus. |
| HRA | high-resolution anoscopy. |
| HPV | human papilloma virus |
| HR-HPV | high risk of human papilloma virus infection. |
| HSIL | high-grade squamous intraepithelial lesions. |
| IQR | interquartile range |
| IUD | intrauterine device |
| LSIL | low-grade squamous intraepithelial lesion [LSIL] |
| NILM | negative for intraepithelial lesion or malignancy |
| NR | not reported |
| OR | odds ratios |
| PLWH | people living with HIV. |
| SD | standard deviation |
| STD | sexually transmitted disease |
| WLWHs | women living with human immunodeficiency virus. |
References
- International Agency for Research Cancer. GLOBOCAN 2020: Estimated cancer incidence, mortality and prevalence worldwide in 2020. 2020. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/10-Anus-fact-sheet (accessed on 16 August 2022).
- Deshmukh, A.A.; Suk, R.; Shiels, M.S.; Sonawane, K.; Nyitray, A.G.; Liu, Y.; Gaisa, M.M.; Palefsky, J.M.; Sigel, K. Recent Trends in Squamous Cell Carcinoma of the Anus Incidence and Mortality in the United States, 2001–2015. J. Natl. Cancer Inst. 2020, 112, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Arens, Y.; Gaisa, M.; Goldstone, S.E.; Liu, Y.; Wisnivesky, J.; Sigel, C.S.; Swartz, T.H.; Sigel, K. Risk of Invasive Anal Cancer in HIV-Infected Patients With High-Grade Anal Dysplasia: A Population-Based Cohort Study. Dis. Colon Rectum 2019, 62, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Georges, D.; Shiels, M.S.; Engels, E.A.; Albuquerque, A.; Poynten, I.M.; De Pokomandy, A.; Easson, A.M.; Stier, E.A. A meta-analysis of anal cancer incidence by risk group: Toward a unified anal cancer risk scale. Int. J. Cancer 2021, 148, 38–47. [Google Scholar] [CrossRef] [PubMed]
- de Sanjosé, S.; Brotons, M.; Pavón, M.A. The natural history of human papillomavirus infection. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 2–13. [Google Scholar] [CrossRef] [PubMed]
- De Sanjosé, S.; Serrano, B.; Tous, S.; Alejo, M.; Lloveras, B.; Quirós, B.; Clavero, O.; Vidal, A.; Ferrándiz-Pulido, C.; Pavón, M.; et al. Burden of Human Papillomavirus (HPV)-Related Cancers Attributable to HPVs 6/11/16/18/31/33/45/52 and 58. JNCI Cancer Spectr. 2018, 2, pky045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, G.; Sharma, M.; Tan, N.; Barnabas, R.V. HIV-positive women have higher risk of human papilloma virus infection, precancerous lesions, and cervical cancer. AIDS 2018, 32, 795–808. [Google Scholar] [CrossRef]
- Wang, C.-C.J.; Sparano, J.; Palefsky, J.M. Human Immunodeficiency Virus/AIDS, Human Papillomavirus, and Anal Cancer. Surg. Oncol. Clin. N. Am. 2017, 26, 17–31. [Google Scholar] [CrossRef] [Green Version]
- Solomon, D.; Davey, D.D.; Kurman, R.J.; Moriarty, A.T.; O’Connor, D.; Prey, M.U.; Raab, S.S.; Sherman, M.E.; Wilbur, D.C.; Wright, J.T.; et al. The 2001 Bethesda SystemTerminology for Reporting Results of Cervical Cytology. JAMA 2002, 287, 2114–2119. [Google Scholar] [CrossRef]
- Chittleborough, T.; Tapper, R.; Eglinton, T.; Frizelle, F. Anal squamous intraepithelial lesions: An update and proposed management algorithm. Tech. Coloproctol. 2020, 24, 95–103. [Google Scholar] [CrossRef]
- Darragh, T.M.; Colgan, T.J.; Cox, J.T.; Heller, D.S.; Henry, M.R.; Luff, R.D.; McCalmont, T.; Nayar, R.; Palefsky, J.M.; Stoler, M.H.; et al. The Lower Anogenital Squamous Terminology Standardization Project for HPV-associated Lesions: Background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Int. J. Gynecol. Pathol. 2013, 32, 76–115. [Google Scholar] [CrossRef]
- Palefsky, J.M.; Lee, J.Y.; Jay, N.; Goldstone, S.E.; Darragh, T.M.; Dunlevy, H.A.; Rosa-Cunha, I.; Arons, A.; Pugliese, J.C.; Vena, D.; et al. Treatment of Anal High-Grade Squamous Intraepithelial Lesions to Prevent Anal Cancer. N. Engl. J. Med. 2022, 386, 2273–2282. [Google Scholar] [CrossRef] [PubMed]
- Moscicki, A.-B.; Darragh, T.M.; Berry-Lawhorn, J.M.; Roberts, J.M.; Khan, M.J.; Boardman, L.A.; Chiao, E.; Einstein, M.H.; Goldstone, S.E.; Jay, N.; et al. Screening for Anal Cancer in Women. J. Low. Genit. Tract Dis. 2015, 19, S27–S42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, M.A.; Horberg, M.A.; Agwu, A.L.; Colasanti, J.A.; Jain, M.K.; Short, W.R.; Singh, T.; Aberg, J.A. Primary Care Guidance for Persons With Human Immunodeficiency Virus: 2020 Update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin. Infect. Dis. 2021, 73, e3572–e3605. [Google Scholar] [CrossRef] [PubMed]
- Hillman, R.J.; Cuming, T.; Darragh, T.; Nathan, M.; Berry-Lawthorn, M.; Goldstone, S.; Law, C.; Palefsky, J.; Barroso, L.F.; Stier, E.; et al. 2016 IANS International Guidelines for Practice Standards in the Detection of Anal Cancer Precursors. J. Low. Genit. Tract Dis. 2016, 20, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.A.; Deshmukh, A.A.; Suk, R.; Roberts, J.; Gilson, R.; Jay, N.; Stier, E.A.; Wentzensen, N. A systematic review and meta-analysis of cytology and HPV-related biomarkers for anal cancer screening among different risk groups. Int. J. Cancer 2022, 151, 1889–1901. [Google Scholar] [CrossRef]
- Official Journal of the European Union. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the Protection of Natural Persons with Regard to the Processing of Personal Data and on the Free Movement of Such Data, and Repealing Directive 95/46/EC(General Data Protection Regulation). Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed on 20 August 2021).
- Genomica Home Page. Available online: https://genomica.com/productos-clart-hpv/ (accessed on 13 August 2022).
- Bornstein, J.; Bentley, J.; Bösze, P.; Girardi, F.; Haefner, H.; Menton, M.; Perrotta, M.; Prendiville, W.; Russell, P.; Sideri, M.; et al. 2011 Colposcopic Terminology of the International Federation for Cervical Pathology and Colposcopy. Obstet. Gynecol. 2012, 120, 166–172. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.; Franceschi, S.; Clifford, G.M. Human papillomavirus types from infection to cancer in the anus, according to sex and HIV status: A systematic review and meta-analysis. Lancet Infect. Dis. 2018, 18, 198–206. [Google Scholar] [CrossRef] [Green Version]
- Faber, M.T.; Frederiksen, K.; Palefsky, J.M.; Kjaer, S.K. Risk of Anal Cancer Following Benign Anal Disease and Anal Cancer Precursor Lesions: A Danish Nationwide Cohort Study. Cancer Epidemiol. Biomark. Prev. 2020, 29, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R.; Kaur, A.; Sandeep; Singh, S.; Gupta, S. Anal cytological abnormalities and human papillomavirus infection in women living with HIV: A systematic review and meta-analysis. HIV Med. 2022, 23, 378–389. [Google Scholar] [CrossRef]
- Goeieman, B.J.; Firnhaber, C.S.; Jong, E.; Michelow, P.; Kegorilwe, P.; Swarts, A.; Williamson, A.-L.; Allan, B.; Smith, J.S.; Wilkin, T.J. Prevalence of Anal HPV and Anal Dysplasia in HIV-Infected Women From Johannesburg, South Africa. JAIDS J. Acquir. Immune Defic. Syndr. 2017, 75, e59–e64. [Google Scholar] [CrossRef] [PubMed]
- Palefsky, J.M.; Holly, E.A.; Ralston, M.L.; Da Costa, M.; Greenblatt, R.M. Prevalence and Risk Factors for Anal Human Papillomavirus Infection in Human Immunodeficiency Virus (HIV)–Positive and High-Risk HIV-Negative Women. J. Infect. Dis. 2001, 183, 383–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heard, I.; Etienney, I.; Potard, V.; Poizot-Martin, I.; Moore, C.; Lesage, A.-C.; Ressiot, E.; Crenn-Hebert, C.; Fléjou, J.-F.; Cubie, H.; et al. High prevalence of Anal Human Papillomavirus-associated cancer precursors in a contemporary cohort of asymptomatic HIV-infected women. Clin. Infect. Dis. 2015, 60, 1559–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahiri, C.D.; Nguyen, M.L.; Mehta, C.C.; Mosunjac, M.; Tadros, T.; Unger, E.R.; Rajeevan, M.S.; Richards, J.; Ofotokun, I.; Flowers, L. Pilot Study of Markers for High-grade Anal Dysplasia in a Southern Cohort From the Women’s Interagency Human Immunodeficiency Virus Study. Clin. Infect. Dis. 2020, 70, 1121–1128. [Google Scholar] [CrossRef]
- Ramautarsing, R.A.; Phanuphak, N.; Chaithongwongwatthana, S.; Wit, F.W.; Teeratakulpisarn, N.; Pankam, T.; Rodbamrung, P.; Lange, J.M.; Phanuphak, P.; Sahasrabuddhe, V.V.; et al. Cervical and anal HPV infection: Cytological and histological abnormalities in HIV-infected women in Thailand. J. Virus Erad. 2015, 1, 96–102. [Google Scholar] [CrossRef]
- Cranston, R.D.; Cespedes, M.S.; Paczuski, P.; Yang, M.; Coombs, R.W.; Dragavon, J.; Saah, A.; Godfrey, C.; Webster-Cyriaque, J.Y.; Chiao, E.Y.; et al. High Baseline Anal Human Papillomavirus and Abnormal Anal Cytology in a Phase 3 Trial of the Quadrivalent Human Papillomavirus Vaccine in Human Immunodeficiency Virus–Infected Individuals Older Than 26 Years: ACTG 5298. Sex Transm Dis 2018, 45, 266–271. [Google Scholar] [CrossRef]
- Weis, S.E.; Vecino, I.; Pogoda, J.M.; Susa, J.S.; Nevoit, J.; Radaford, D.; McNeely, P.; Colquitt, C.A.; Adams, E. Prevalence of Anal Intraepithelial Neoplasia Defined by Anal Cytology Screening and High-Resolution Anoscopy in a Primary Care Population of HIV-Infected Men and Women. Dis. Colon Rectum 2011, 54, 433–441. [Google Scholar] [CrossRef]
- Darragh, T.M.; Tokugawa, D.; Castle, P.E.; Follansbee, S.; Borgonovo, S.; LaMere, B.J.; Schwartz, L.; Gage, J.C.; Fetterman, B.; Lorey, T.; et al. Interrater agreement of anal cytology. Cancer Cytopathol. 2013, 121, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Cachay, E.R.; Agmas, W.; Mathews, W.C. Relative Accuracy of Cervical and Anal Cytology for Detection of High Grade Lesions by Colposcope Guided Biopsy: A Cut-Point Meta-Analytic Comparison. PLoS ONE 2012, 7, e38956. [Google Scholar] [CrossRef] [Green Version]
- Gaisa, M.; Ita-Nagy, F.; Sigel, K.; Arens, Y.; Hennessy, M.A.; Rodriguez-Caprio, G.; Mullen, M.; Aberg, J.A.; Cespedes, M. High Rates of Anal High-Grade Squamous Intraepithelial Lesions in HIV-Infected Women Who Do Not Meet Screening Guidelines. Clin. Infect. Dis. 2017, 64, 289–294. [Google Scholar] [CrossRef]
- Silvera, R.; Gaisa, M.M.; Goldstone, S.E. Random Biopsy During High-Resolution Anoscopy Increases Diagnosis of Anal High-Grade Squamous Intraepithelial Lesions. JAIDS J. Acquir. Immune Defic. Syndr. 2014, 65, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Stier, E.A.; Lensing, S.Y.; Darragh, T.M.; Deshmukh, A.A.; Einstein, M.H.; Palefsky, J.M.; Jay, N.; Berry-Lawhorn, J.M.; Wilkin, T.; Wiley, D.J.; et al. Prevalence of and Risk Factors for Anal High-grade Squamous Intraepithelial Lesions in Women Living with Human Immunodeficiency Virus. Clin. Infect. Dis. 2020, 70, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Kelly, H.; Chikandiwa, A.; Vilches, L.A.; Palefsky, J.M.; de Sanjose, S.; Mayaud, P. Association of antiretroviral therapy with anal high-risk human papillomavirus, anal intraepithelial neoplasia, and anal cancer in people living with HIV: A systematic review and meta-analysis. Lancet HIV 2020, 7, e262–e278. [Google Scholar] [CrossRef]
- Lin, C.; Slama, J.; Gonzalez, P.; Goodman, M.T.; Xia, N.; Kreimer, A.R.; Wu, T.; Hessol, N.A.; Shvetsov, Y.; Ortiz, A.P.; et al. Cervical determinants of anal HPV infection and high-grade anal lesions in women: A collaborative pooled analysis. Lancet Infect. Dis. 2019, 19, 880–891. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Hernando, L.; Oliver-Pérez, R.; Bravo-Violeta, V.; Olloqui, A.; Parte-Izquierdo, B.; Almansa-González, C.; Bermejo-Martinez, R.; Bolivar-De Miguel, A.B.; Diez, A.; Seoane-Ruiz, J.M.; et al. Prevalence of Anal High-Risk Human Papilloma Virus Infection and Abnormal Anal Cytology among Women Living with HIV. J. Pers. Med. 2022, 12, 1778. https://doi.org/10.3390/jpm12111778
Muñoz-Hernando L, Oliver-Pérez R, Bravo-Violeta V, Olloqui A, Parte-Izquierdo B, Almansa-González C, Bermejo-Martinez R, Bolivar-De Miguel AB, Diez A, Seoane-Ruiz JM, et al. Prevalence of Anal High-Risk Human Papilloma Virus Infection and Abnormal Anal Cytology among Women Living with HIV. Journal of Personalized Medicine. 2022; 12(11):1778. https://doi.org/10.3390/jpm12111778
Chicago/Turabian StyleMuñoz-Hernando, Leticia, Reyes Oliver-Pérez, Victoria Bravo-Violeta, Alejandro Olloqui, Belen Parte-Izquierdo, Cristina Almansa-González, Rocio Bermejo-Martinez, Ana Belen Bolivar-De Miguel, Alvaro Diez, Jose Miguel Seoane-Ruiz, and et al. 2022. "Prevalence of Anal High-Risk Human Papilloma Virus Infection and Abnormal Anal Cytology among Women Living with HIV" Journal of Personalized Medicine 12, no. 11: 1778. https://doi.org/10.3390/jpm12111778