
Diabetes Mellitus and Heart Failure

 , ,
, ,
Abstract
:1. Introduction
2. Epidemiology
3. Heart Failure with Preserved Ejection Fraction and Diabetes
4. Mineralocorticoid Receptor Antagonists in DM and HF
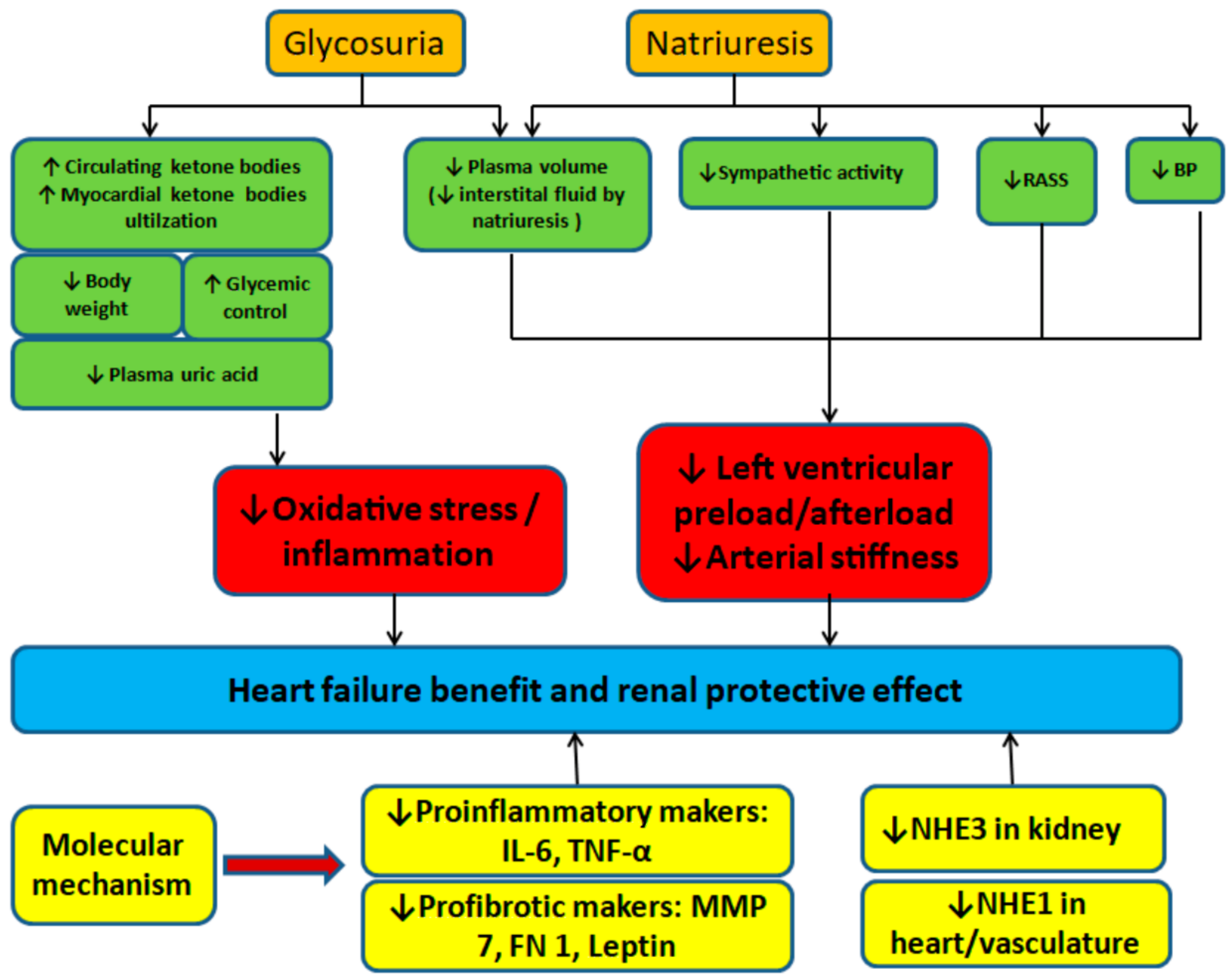
5. Sodium–Glucose Cotransporter 2 Inhibitors in Diabetes and Heart Failure
6. Sodium–Glucose Cotransporter 2 Inhibitors in Heart Failure with Reduced Ejection Fraction
7. Sodium–Glucose Cotransporter 2 Inhibitors in Heart Failure with Preserved Ejection Fraction
8. Updated Guidelines for Sodium–Glucose Cotransporter 2 Inhibitors
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guariguata, L.; Whiting, D.R.; Hambleton, I.; Beagley, J.; Linnenkamp, U.; Shaw, J.E. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 2014, 103, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Randhawa, V.K.; Dhanvantari, S.; Connelly, K.A. How Diabetes and Heart Failure Modulate Each Other and Condition Management. Can. J. Cardiol. 2021, 37, 595–608. [Google Scholar] [CrossRef]
- Petrie, M.C.; Verma, S.; Docherty, K.F.; Inzucchi, S.E.; Anand, I.; Belohlavek, J.; Böhm, M.; Chiang, C.E.; Chopra, V.K.; de Boer, R.A.; et al. Effect of dapagliflozin on worsening heart failure and cardiovascular death in patients with heart failure with and without diabetes. JAMA 2020, 323, 1353–1368. [Google Scholar] [CrossRef] [PubMed]
- Soläng, L.; Malmberg, K.; Ryden, L. Diabetes mellitus and congestive heart failure. Eur. Heart J. 1999, 20, 789–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amato, L.; Paolisso, G.; Cacciatore, F.; Ferrara, N.; Ferrara, P.; Canonico, S.; Varricchio, M.; Rengo, F. Congestive heart failure predicts the development of non-insulin-dependent diabetes mellitus in the elderly. The Osservatorio Geriatrico Regione Campania Group. Diabetes Metab. 1997, 23, 213–218. [Google Scholar]
- Kannel, W.B.; Hjortland, M.; Castelli, W.P. Role of diabetes in congestive heart failure: The Framingham study. Am. J. Cardiol. 1974, 34, 29–34. [Google Scholar] [CrossRef]
- Iribarren, C.; Karter, A.J.; Go, A.S.; Ferrara, A.; Liu, J.Y.; Sidney, S.; Selby, J.V. Glycemic control and heart failure among adult patients with diabetes. Circulation 2001, 103, 2668–2673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paolillo, S.; Salvioni, E.; Perrone Filardi, P.; Bonomi, A.; Sinagra, G.; Gentile, P.; Gargiulo, P.; Scoccia, A.; Cosentino, N.; Gugliandolo, P.; et al. Long-term prognostic role of diabetes mellitus and glycemic control in heart failure patients with reduced ejection fraction: Insights from the MECKI Score database. Int. J. Cardiol. 2020, 317, 103–110. [Google Scholar] [CrossRef]
- Pavlović, A.; Polovina, M.; Ristić, A.; Seferović, J.P.; Veljić, I.; Simeunović, D.; Milinković, I.; Krljanac, G.; Ašanin, M.; Oštrić-Pavlović, I.; et al. Long-term mortality is increased in patients with undetected prediabetes and type-2 diabetes hospitalized for worsening heart failure and reduced ejection fraction. Eur. J. Prev. Cardiol. 2019, 26, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Konduracka, E.; Cieslik, G.; Galicka-Latala, D.; Rostoff, P.; Pietrucha, A.; Latacz, P.; Gajos, G.; Malecki, M.T.; Nessler, J. Myocardial dysfunction and chronic heart failure in patients with long-lasting type 1 diabetes: A 7-year prospective cohort study. Acta Diabetol. 2013, 50, 597–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.T.; Sogaard, P.; Andersen, H.U.; Bech, J.; Fritz Hansen, T.; Biering-Sørensen, T.; Jørgensen, P.G.; Galatius, S.; Madsen, J.K.; Rossing, P.; et al. Global longitudinal strain is not impaired in type 1 diabetes patients without albuminuria: The Thousand & 1 study. JACC Cardiovasc. Imaging 2015, 8, 400–410. [Google Scholar]
- Maddox, T.M.; Januzzi, J.L., Jr.; Allen, L.A.; Breathett, K.; Butler, J.; Davis, L.L.; Fonarow, G.C.; Ibrahim, N.E.; Lindenfeld, J.; Masoudi, F.A.; et al. 2021 Update to the 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2021, 77, 772–810. [Google Scholar]
- Johansson, I.; Edner, M.; Dahlström, U.; Näsman, P.; Rydén, L.; Norhammar, A. Is the prognosis in patients with diabetes and heart failure a matter of unsatisfactory management? An observational study from the Swedish Heart Failure Registry. Eur. J. Heart Fail. 2014, 16, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Cavender, M.A.; Steg, P.G.; Smith, S.C., Jr.; Eagle, K.; Ohman, E.M.; Goto, S.; Kuder, J.; Im, K.; Wilson, P.W.; Bhatt, D.L.; et al. Impact of diabetes mellitus on hospitalization for heart failure, cardiovascular events, and death: Outcomes at 4 years from the Reduction of Atherothrombosis for Continued Health (REACH) Registry. Circulation 2015, 132, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Rørth, R.; Jhund, P.S.; Kristensen, S.L.; Desai, A.S.; Køber, L.; Rouleau, J.L.; Solomon, S.D.; Swedberg, K.; Zile, M.R.; Packer, M.; et al. The prognostic value of troponin T and N-terminal pro B-type natriuretic peptide, alone and in combination, in heart failure patients with and without diabetes. Eur. J. Heart Fail. 2019, 21, 40–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srivastava, P.M.; Calafiore, P.; Macisaac, R.J.; Patel, S.K.; Thomas, M.C.; Jerums, G.; Burrell, L.M. Prevalence and predictors of cardiac hypertrophy and dysfunction in patients with Type 2 diabetes. Clin. Sci. 2008, 114, 313–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wai, B.; Patel, S.K.; Ord, M.; MacIsaac, R.J.; Jerums, G.; Srivastava, P.M.; Burrell, L.M. Prevalence, predictors and evolution of echocardiographically defined cardiac abnormalities in adults with type 1 diabetes: An observational cohort study. J. Diabetes Complicat. 2014, 28, 22–28. [Google Scholar] [CrossRef]
- Paolillo, S.; Scardovi, A.B.; Campodonico, J. Role of comorbidities in heart failure prognosis Part I: Anaemia, iron deficiency, diabetes, atrial fibrillation. Eur. J. Prev. Cardiol. 2020, 27, S27–S34. [Google Scholar] [CrossRef]
- Boyer, J.K.; Thanigaraj, S.; Schechtman, K.B.; Pérez, J.E. Prevalence of ventricular diastolic dysfunction in asymptomatic, normotensive patients with diabetes mellitus. Am. J. Cardiol. 2004, 93, 870–875. [Google Scholar] [CrossRef] [PubMed]
- Echouffo-Tcheugui, J.B.; Xu, H.; DeVore, A.D.; Schulte, P.J.; Butler, J.; Yancy, C.W.; Bhatt, D.L.; Hernandez, A.F.; Heidenreich, P.A.; Fonarow, G.C. Temporal trends and factors associated with diabetes mellitus among patients hospitalized with heart failure: Findings from Get With The Guidelines–Heart Failure registry. Am. Heart J. 2016, 182, 9–20. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, M.R.; Petrie, M.C.; Varyani, F.; Ostergren, J.; Michelson, E.L.; Young, J.B.; Solomon, S.D.; Granger, C.B.; Swedberg, K.; Yusuf, S.; et al. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: An analysis of the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur. Heart J. 2008, 29, 1377–1385. [Google Scholar] [CrossRef] [Green Version]
- Aguilar, D.; Deswal, A.; Ramasubbu, K.; Mann, D.L.; Bozkurt, B. Comparison of patients with heart failure and preserved left ventricular ejection fraction among those with versus without diabetes mellitus. Am. J. Cardiol. 2010, 105, 373–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ernande, L.; Audureau, E.; Jellis, C.L.; Bergerot, C.; Henegar, C.; Sawaki, D.; Czibik, G.; Volpi, C.; Canoui-Poitrine, F.; Thibault, H.; et al. Clinical implications of echocardiographic phenotypes of patients with diabetes mellitus. J. Am. Coll. Cardiol. 2017, 70, 1704–1716. [Google Scholar] [CrossRef]
- Lindman, B.R.; Dávila-Román, V.G.; Mann, D.L.; McNulty, S.; Semigran, M.J.; Lewis, G.D.; de las Fuentes, L.; Joseph, S.M.; Vader, J.; Hernandez, A.F.; et al. Cardiovascular phenotype in HFpEF patients with or without diabetes: A RELAX trial ancillary study. J. Am. Coll. Cardiol. 2014, 64, 541–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smaha, L. A, American Heart Association. The American Heart Association get with the guidelines program. Am. Heart J. 2004, 148, S46–S48. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, S.L.; Mogensen, U.M.; Jhund, P.S.; Petrie, M.C.; Preiss, D.; Win, S.; Køber, L.; McKelvie, R.S.; Zile, M.R.; Anand, I.S.; et al. Clinical and echocardiographic characteristics and cardiovascular outcomes according to diabetes status in patients with heart failure and preserved ejection fraction: A report from the I-Preserve Trial (Irbesartan in Heart Failure With Preserved Ejection Fraction). Circulation 2017, 135, 724–735. [Google Scholar] [PubMed] [Green Version]
- Vaduganathan, M.; Claggett, B.L.; Chatterjee, N.A.; Anand, I.S.; Sweitzer, N.K.; Fang, J.C.; O’Meara, E.; Shah, S.J.; Hegde, S.M.; Desai, A.S.; et al. Sudden death in heart failure with preserved ejection fraction: A competing risks analysis from the TOPCAT trial. JACC Heart Fail. 2018, 6, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Holland, D.J.; Marwick, T.H.; Haluska, B.A.; Leano, R.; Hordern, M.D.; Hare, J.L.; Fang, Z.Y.; Prins, J.B.; Stanton, T. Subclinical LV dysfunction and 10-year outcomes in type 2 diabetes mellitus. Heart 2015, 101, 1061–1066. [Google Scholar] [CrossRef]
- Seferović, P.M.; Petrie, M.C.; Filippatos, G.S.; Anker, S.D.; Rosano, G.; Bauersachs, J.; Paulus, W.J.; Komajda, M.; Cosentino, F.; de Boer, R.A.; et al. Type 2 diabetes mellitus and heart failure: A position statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018, 20, 853–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannel, W.B.; McGee, D.L. Diabetes and cardiovascular disease: The Framingham study. JAMA 1979, 241, 2035–2038. [Google Scholar] [CrossRef] [PubMed]
- Shivalkar, B.; Dhondt, D.; Goovaerts, I.; Van Gaal, L.; Bartunek, J.; Van Crombrugge, P.; Vrints, C. Flow mediated dilatation and cardiac function in type 1 diabetes mellitus. Am. J. Cardiol. 2006, 97, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Ernande, L.; Bergerot, C.; Rietzschel, E.R.; De Buyzere, M.L.; Thibault, H.; Pignonblanc, P.G.; Croisille, P.; Ovize, M.; Groisne, L.; Moulin, P.; et al. Diastolic dysfunction in patients with type 2 diabetes mellitus: Is it really the first marker of diabetic cardiomyopathy? J. Am. Soc. Echocardiogr. 2011, 24, 1268–1275. [Google Scholar] [CrossRef] [PubMed]
- Goldin, A.; Beckman, J.A.; Schmidt, A.M.; Creager, M.A. Advanced glycation end products: Sparking the development of diabetic vascular injury. Circulation 2006, 114, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Marwick, T.H.; Ritchie, R.; Shaw, J.E.; Kaye, D. Implications of underlying mechanisms for the recognition and management of diabetic cardiomyopathy. J. Am. Coll. Cardiol. 2018, 71, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Chiu, J.; Farhangkhoee, H.; Xu, B.Y.; Chen, S.; George, B.; Chakrabarti, S. PARP mediates structural alterations in diabetic cardiomyopathy. J. Mol. Cell Cardiol. 2008, 45, 385–393. [Google Scholar] [CrossRef]
- Van Linthout, S.; Seeland, U.; Riad, A.; Eckhardt, O.; Hohl, M.; Dhayat, N.; Richter, U.; Fischer, J.W.; Böhm, M.; Pauschinger, M.; et al. Reduced MMP-2 activity contributes to cardiac fibrosis in experimental diabetic cardiomyopathy. Basic Res. Cardiol. 2008, 103, 319–327. [Google Scholar] [CrossRef]
- Westermann, D.; Rutschow, S.; Jäger, S.; Linderer, A.; Anker, S.; Riad, A.; Unger, T.; Schultheiss, H.P.; Pauschinger, M.; Tschöpe, C. Contributions of inflammation and cardiac matrix metalloproteinase activity to cardiac failure in diabetic cardiomyopathy: The role of angiotensin type 1 receptor antagonism. Diabetes 2007, 56, 641–646. [Google Scholar] [CrossRef] [Green Version]
- Buchanan, J.; Mazumder, P.K.; Hu, P.; Chakrabarti, G.; Roberts, M.W.; Yun, U.J.; Cooksey, R.C.; Litwin, S.E.; Abel, E.D. Reduced cardiac efficiency and altered substrate metabolism precedes the onset of hyperglycemia and contractile dysfunction in two mouse models of insulin resistance and obesity. Endocrinology 2005, 146, 5341–5349. [Google Scholar] [CrossRef] [Green Version]
- Montaigne, D.; Marechal, X.; Coisne, A.; Debry, N.; Modine, T.; Fayad, G.; Potelle, C.; El Arid, J.M.; Mouton, S.; Sebti, Y.; et al. Myocardial contractile dysfunction is associated with impaired mitochondrial function and dynamics in type 2 diabetic but not in obese patients. Circulation 2014, 130, 554–564. [Google Scholar] [CrossRef] [Green Version]
- Young, M.J.; Adler, G.K. Aldosterone, the mineralocorticoid receptor and mechanisms of cardiovascular disease. Vitam. Horm. 2019, 109, 361–385. [Google Scholar]
- Effectiveness of spironolactone added to an angiotensin-converting enzyme inhibitor and a loop diuretic for severe chronic congestive heart failure (the Randomized Aldactone Evaluation Study [RALES]). Am. J. Cardiol. 1996, 78, 902–907. [CrossRef]
- Rossello, X.; Ariti, C.; Pocock, S.J.; Ferreira, J.P.; Girerd, N.; McMurray, J.J.V.; Van Veldhuisen, D.J.; Pitt, B.; Zannad, F. Impact of mineralocorticoid receptor antagonists on the risk of sudden cardiac death in patients with heart failure and left-ventricular systolic dysfunction: An individual patient-level meta-analysis of three randomized-controlled trials. Clin. Res. Cardiol. 2019, 108, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Seferovic, P.M.; Ponikowski, P.; Anker, S.D.; Bauersachs, J.; Chioncel, O.; Cleland, J.G.F.; de Boer, R.A.; Drexel, H.; Ben Gal, T.; Hill, L.; et al. Clinical practice update on heart failure 2019: Pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 1169–1186. [Google Scholar] [CrossRef]
- Bakris, G.L.; Agarwal, R.; Anker, S.D.; Pitt, B.; Ruilope, L.M.; Rossing, P.; Kolkhof, P.; Nowack, C.; Schloemer, P.; Joseph, A.; et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N. Engl. J. Med. 2020, 383, 2219–2229. [Google Scholar] [CrossRef] [PubMed]
- Filippatos, G.; Anker, S.D.; Agarwal, R.; Ruilope, L.M.; Rossing, P.; Bakris, G.L.; Tasto, C.; Joseph, A.; Kolkhof, P.; Lage, A.; et al. Finerenone reduces risk of incident heart failure in patients with chronic kidney disease and type 2 diabetes: Analyses From the FIGARO-DKD trial. Circulation 2022, 145, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Dardano, A.; Miccoli, R.; Bianchi, C.; Daniele, G.; Del Prato, S. Invited review. Series: Implications of the recent CVOTs in type 2 diabetes: Which patients for GLP-1RA or SGLT-2 inhibitor? Diabetes Res. Clin. Pract. 2020, 162, 108112. [Google Scholar] [CrossRef]
- Chen, H.Y.; Huang, J.Y.; Siao, W.Z.; Jong, G.P. The association between SGLT2 inhibitors and new-onset arrhythmias: A nationwide population-based longitudinal cohort study. Cardiovasc. Diabetol. 2020, 19, 73. [Google Scholar] [CrossRef]
- Zinman, B.; Broedl, U.C.; Inzucchi, S.E.; EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [Green Version]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Cannon, C.P.; Pratley, R.; Dagogo-Jack, S.; Mancuso, J.; Huyck, S.; Masiukiewicz, U.; Charbonnel, B.; Frederich, R.; Gallo, S.; Cosentino, F.; et al. Cardiovascular outcomes with ertugliflozin in type 2 diabetes. N. Engl. J. Med. 2020, 383, 1425–1435. [Google Scholar] [CrossRef] [PubMed]
- Cavender, M.A.; Norhammar, A.; Birkeland, K.I.; Jørgensen, M.E.; Wilding, J.P.; Khunti, K.; Fu, A.Z.; Bodegård, J.; Blak, B.T.; Wittbrodt, E.; et al. SGLT-2 inhibitors and cardiovascular risk: An analysis of CVD-REAL. J. Am. Coll. Cardiol. 2018, 71, 2497–2506. [Google Scholar] [CrossRef] [PubMed]
- Ryan, P.B.; Buse, J.B.; Schuemie, M.J.; DeFalco, F.; Yuan, Z.; Stang, P.E.; Berlin, J.A.; Rosenthal, N. Comparative effectiveness of canagliflozin, SGLT2 inhibitors and non-SGLT2 inhibitors on the risk of hospitalization for heart failure and amputation in patients with type 2 diabetes mellitus: A real-world meta-analysis of 4 observational databases (OBSERVE-4D). Diabetes Obes. Metab. 2018, 20, 2585–2597. [Google Scholar] [PubMed]
- Patorno, E.; Pawar, A.; Franklin, J.M.; Najafzadeh, M.; Déruaz-Luyet, A.; Brodovicz, K.G.; Sambevski, S.; Bessette, L.G.; Santiago Ortiz, A.J.; Kulldorff, M.; et al. Empagliflozin and the risk of heart failure hospitalization in routine clinical care: A first analysis from the EMPRISE study. Circulation 2019, 139, 2822–2830. [Google Scholar] [CrossRef]
- McMurray, J.J.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; Ferreira, J.P.; Pocock, S.J.; Anker, S.D.; Butler, J.; Filippatos, G.; Brueckmann, M.; Ofstad, A.P.; Pfarr, E.; Jamal, W.; et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: A meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet 2020, 396, 819–829. [Google Scholar] [CrossRef]
- Kato, E.T.; Silverman, M.G.; Mosenzon, O.; Zelniker, T.A.; Cahn, A.; Furtado, R.H.M.; Kuder, J.; Murphy, S.A.; Bhatt, D.L.; Leiter, L.A.; et al. Effect of dapagliflozin on heart failure and mortality in type 2 diabetes mellitus. Circulation 2019, 139, 2528–2536. [Google Scholar] [CrossRef]
- Zelniker, T.A.; Morrow, D.A.; Mosenzon, O.; Goodrich, E.L.; Jarolim, P.; Murphy, S.A.; Bhatt, D.L.; Leiter, L.A.; McGuire, D.K.; Wilding, J.; et al. Relationship between baseline cardiac biomarkers and cardiovascular death or hospitalization for heart failure with and without SGLT2 inhibitor therapy in DECLARE-TIMI 58. Eur. J. Heart Fail. 2021, 23, 1026–1036. [Google Scholar] [CrossRef]
- Nassif, M.E.; Windsor, S.L.; Tang, F.; Khariton, Y.; Husain, M.; Inzucchi, S.E.; McGuire, D.K.; Pitt, B.; Scirica, B.M.; Austin, B.; et al. Dapagliflozin effects on biomarkers, symptoms, and functional status in patients with heart failure with reduced ejection fraction: The DEFINE-HF trial. Circulation 2019, 140, 1463–1476. [Google Scholar] [CrossRef]
- Figtree, G.A.; Rådholm, K.; Barrett, T.D.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Matthews, D.R.; Shaw, W.; Neal, B. Effects of canagliflozin on heart failure outcomes associated with preserved and reduced ejection fraction in type 2 diabetes mellitus: Results from the CANVAS Program. Circulation 2019, 139, 2591–2593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nassif, M.E.; Windsor, S.L.; Borlaug, B.A.; Kitzman, D.W.; Shah, S.J.; Tang, F.; Khariton, Y.; Malik, A.O.; Khumri, T.; Umpierrez, G.; et al. The SGLT2 inhibitor dapaglifozin in heart failure with preserved ejection fraction: A multicenter randomized trial. Nat. Med. 2021, 27, 1954–1960. [Google Scholar] [CrossRef] [PubMed]
- Spertus, J.A.; Birmingham, M.C.; Nassif, M.; Damaraju, C.V.; Abbate, A.; Butler, J.; Lanfear, D.E.; Lingvay, I.; Kosiborod, M.N.; Januzzi, J.L. The SGLT2 inhibitor canaglifozin in heart failure: The CHIEF-HF remote, patient-centered randomized trial. Nat. Med. 2022, 28, 809–813. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empaglifozin in heart failure with a preserved ejection fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Solomon, S.D.; Vaduganathan, M.; Claggett, B.L.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Baseline characteristics of patients with HFwith mildly reduced and preserved ejection fraction: DELIVER trial. JACC Heart Fail. 2022, 10, 184–197. [Google Scholar] [CrossRef]
- Association Diabetes Association, 9. Pharmacologic approaches to glycemic treatment: Standards of Medical Care in Diabetes—2020. Diabetes Care. 2020, 43, S98–S110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: A report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J. Am. Coll. Cardiol. 2022, 79, 1757–1780. [Google Scholar] [CrossRef]


{kind=link}
| EMPA-REG Outcome (2015) | CANVAS Program (2017) | DECLARE-TIMI 58 (2019) | VERTIS-CV (2020) | |
|---|---|---|---|---|
| tudy population | T2D and established CVD | T2D and high CV risk | T2D and high CV risk | T2D and established ASCVD |
| Study numbers (n) | 7020 | 10,142 | 17,160 | 8246 |
| Drug | Empagliflozin 10 mg or 25 mg | Canagliflozin 100 mg or 300 mg | Dapagliflozin 10 mg | Ertugliflozin 5 mg or 15 mg |
| Age (years) | 63.1 ± 8.6 | 63.3 ± 8.3 | 63.9 ± 6.8 | 64.4 ± 8.1 |
| Male (%) | 71.2 | 64.2 | 63.1 | 70.3 |
| Median follow up (years) | 3.1 | 2.4 | 4.2 | 3.5 |
| ASCVD (%) | 99.4 | 72.2 | 40.5 | 100 |
| CAD (%) | 75.6 | 56.4 | 32.9 | 75.4 |
| Heart failure (%) | 9.9 | 14.4 | 9.9 | 23.4 |
| HbA1c (%) | 8.07 ± 0.85 | 8.2 ± 0.9 | 8.3 ± 1.2 | 8.2 ± 1.0 |
| Baseline eGFR | 74 | 77 | 85 | 76.1 ± 20.9 |
| Body mass index | 30.6 ± 5.3 | 32.0 ± 5.9 | 32.1 ± 6.0 | 31.9 ± 5.4 |
| Primary outcome, HR (95% CI) | MACE 0.86 (0.74–0.99) (p = 0.04 for superiority) | MACE 0.86 (0.75–0.97) (p = 0.02 for superiority) | MACE 0.93 (0.84–1.03) (p = 0.17 for superiority) | MACE 0.97 (0.85–1.11) (p < 0.001 for noninferiority) |
| HHF, HR (95% CI) | 0.65 (0.50–0.85) | 0.67 (0.52–0.87) | 0.73 (0.61−0.88) | 0.70 (0.54-0.90) |
| CV death, HR (95% CI) | 0.62 (0.49–0.77) | 0.87 (0.72–1.06) | 0.98 (0.82−1.17) | 0.92 (0.77–1.11) |
| All cause death HR (95% CI) | 0.68 (0.57–0.82) | 0.87 (0.74–1.01) | 0.93 (0.82–1.04) | 0.93 (0.80–1.08) |
| Nonfatal MI, HR (95% CI) | 0.87 (0.70–1.09) | 0.85 (0.69–1.05) | Fatal/nonfatal MI 0.89 (0.77−1.01) | Fatal/nonfatal MI 1.04 (0.76–1.32) |
| Nonfatal stroke, HR (95% CI) | 1.24 (0.92–1.67) | 0.90 (0.71–1.15) | Fatal or nonfatal 1.01 (0.84−1.21) | 1.00 (0.76-1.32) |
| Genital infection Intervention/Placebo | Male: 5.0%/1.5% Female: 10.0%/2.6% (Both p < 0.001) | Event rate (per 1000 patient-yr): Female: 68.8/17.5 (p < 0.001) | HR (95% CI): 8.36 (4.19–16.68) (p < 0.001) | Risk difference (95% CI) Ertugliflozin 5 mg Female:3.6 (1.8–5.7) (p < 0.001) Ertugliflozin 15 mg Female:5.4 (3.4–7.7) (p < 0.001) |
| Diabetic ketoacidosis Intervention/Placebo | 0.1%/<0.1% No significant differences | Event rate (per 1000 patient-yr): 0.6/0.3 (p = 0.14) | HR (95% CI): 2.18 (1.10–4.30) (p = 0.02) | Ertugliflozin 5 mg/15 mg/placebo 0.3%/0.4%/0.1% |
| Bone fracture | 3.8 vs. 3.9 No significant differences | Event rate (per 1000 patient-yr): 15.4/11.9(p = 0.02) | HR (95% CI): 1.04 (0.91–1.18) (p = 0.59) | Ertugliflozin 5 mg/15 mg/placebo 3.6%/3.7%/3.6% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siao, W.-Z.; Chen, Y.-H.; Tsai, C.-F.; Lee, C.-M.; Jong, G.-P. Diabetes Mellitus and Heart Failure. J. Pers. Med. 2022, 12, 1698. https://doi.org/10.3390/jpm12101698
Siao W-Z, Chen Y-H, Tsai C-F, Lee C-M, Jong G-P. Diabetes Mellitus and Heart Failure. Journal of Personalized Medicine. 2022; 12(10):1698. https://doi.org/10.3390/jpm12101698
Chicago/Turabian StyleSiao, Wun-Zhih, Yong-Hsin Chen, Chin-Feng Tsai, Chun-Ming Lee, and Gwo-Ping Jong. 2022. "Diabetes Mellitus and Heart Failure" Journal of Personalized Medicine 12, no. 10: 1698. https://doi.org/10.3390/jpm12101698