1. Introduction
Glaucoma is the leading cause of irreversible blindness worldwide. The global prevalence of glaucoma in people aged from 40 to 80 years is estimated to be 3.5% [
1]. Visual field (VF) loss is detected by semiautomated perimeters, which are widely used to diagnose glaucoma and detect its progression, making them essential for glaucoma management [
2]. Static perimetry methods are utilized to estimate retinal function by measuring light sensitivity thresholds. The data of the test results are quantitative, which makes it possible to analyze them statistically. The presence of glaucoma itself and more severe stages of glaucoma are associated with a higher variability of VF testing [
3,
4,
5,
6,
7]. Other than visual acuity and other visual functions, aging, cognitive function, ethnicity, and mental status can affect the reliability of the VF tests. Therefore, VF testing is intrinsically variable and can have a certain amount of random variability even in healthy, trained, and reliable participants because it is a probabilistic rather than a deterministic examination [
8,
9,
10,
11,
12,
13]. Among the factors, aging is an important factor that affects the results of VF testing. It has been reported that threshold sensitivity declines with aging [
14,
15]; therefore, the age-related decline in light sensitivity is adjusted by the semiautomated perimeters.
The lower accuracy of the VF test will be reflected by the changes in the reliability indices, which include rates of fixation loss (FL), false negatives (FNs), and false positives (FPs). The evaluation of these indices is critical in monitoring glaucoma progression [
2,
9,
16,
17,
18,
19]. We previously reported the influence of aging on the reliability of VF testing by using a large dataset of a central 30-2 program by the Humphrey Visual Field Analyzer [
20]. However, the influence of aging on the reliability indices of VFs tested by the central 10-2 program, a program suitable to test both advanced cases and glaucoma with paracentral scotoma, is not well documented. In this study, we investigated the possible association between age and the VF reliability indices in a large dataset of the central 10-2 program tests to reflect on real-world consequences.
2. Materials and Methods
The study adhered to the tenets of the Declaration of Helsinki; the institutional review board (IRB) of Shimane University Hospital reviewed and approved the research (study no. 20080911-1). The IRB approval did not require each patient to provide written informed consent for the publication; instead, the study protocol was posted to the study institutions to notify the participants of the study. To analyze real-world data, all 6674 VF tests using the central 10-2 program, obtained by the Humphrey Visual Field Analyzer (Carl Zeiss Meditec, Dublin, CA, USA) with the SITA Standard, were extracted from the database stored at the Department of Ophthalmology, Shimane University Hospital, between 1988 and 2019. These VF data consisted of 1782 eyes of 1094 Japanese subjects (the mean age ± standard deviation [SD] was 66.6 ± 14.1 years). We also collected the subjects’ age during the VF testing, mean deviation (MD), pattern standard deviation (PSD), and rates of FLs, FNs, and FPs. The possible correlations among each parameter (age, MD, PSD, FL, FN, and FP) were assessed using the Spearman’s rank correlation test. The mean values of each reliability index (FL, FN, and FP) were calculated for each age group stratified by 10 years (i.e., 0–9 years, 10–19 years, and 90–99 years) and were compared between each of those age groups by a one-way analysis of variance followed by the post-hoc Tukey honesty significant difference (HSD) test for the adjustment of multi-pair comparisons. We also performed mixed-effect regression analyses in 40-year-old or older subjects, calculated by age, MD, and PSD as the fixed effects and by subject identification number and tested eye (right or left) as the random effects, in order to assess the influence of each parameter (age, MD, and PSD) on the reliability indices (FLs, FNs, and FPs). All statistical analyses were performed using the JMP Pro statistical software version 15.2.1 (SAS Institute, Inc., Cary, NC, USA).
3. Results
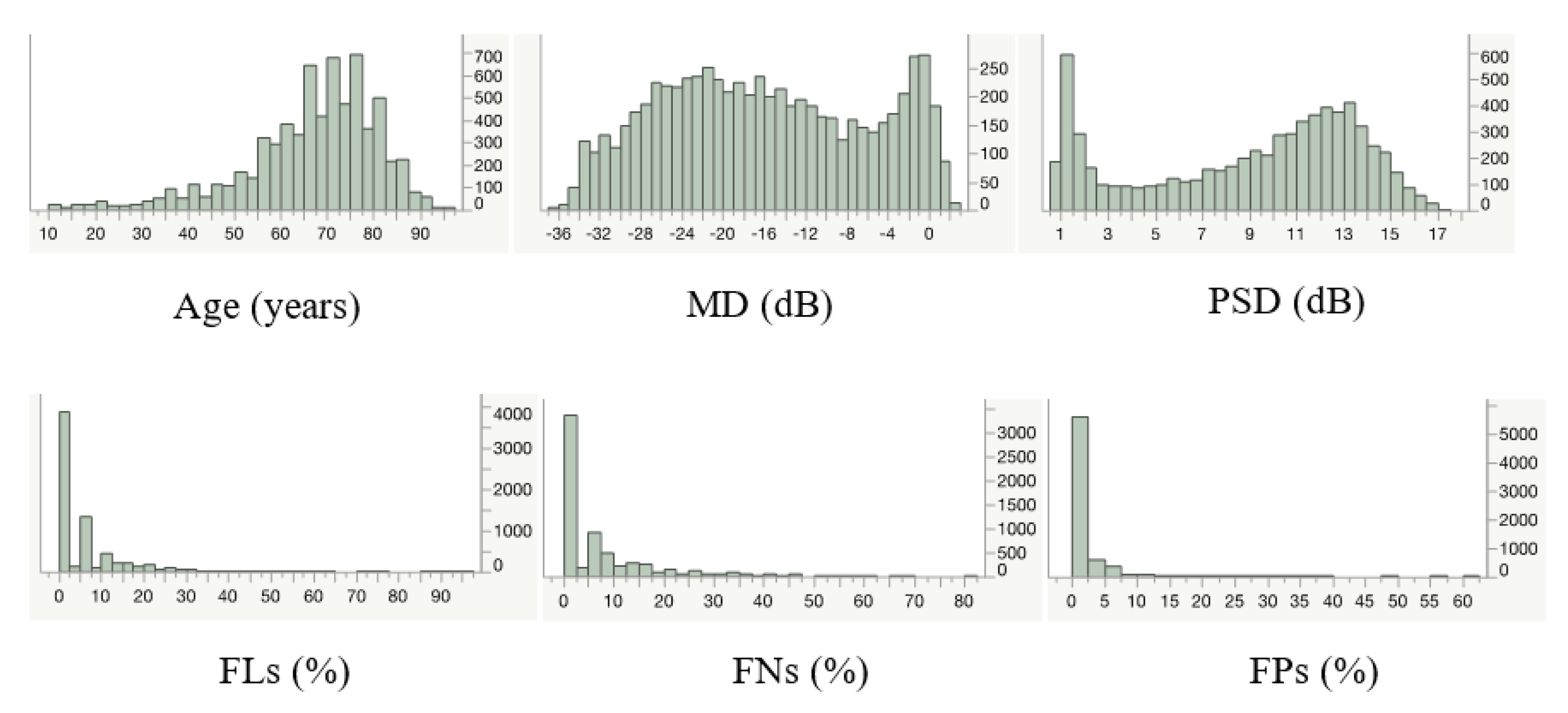
Table 1 summarizes the obtained parameters, and
Figure 1 shows their distribution. The mean age of the subjects was 66.6 years, with an age range of 0–95 years in this dataset.
The possible associations between age, VF parameters (MD and PSD), and the reliability indices are shown in
Table 2. There were no correlations between the pairs of age–FLs, age–FPs, and PSD–FPs. All of the other combinations of parameters had significant correlations (
p < 0.0001). The strongest correlation against age was with FNs (ρ = 0.21).
The values of each reliability index in each age-stratified group are shown in
Table 3,
Table 4 and
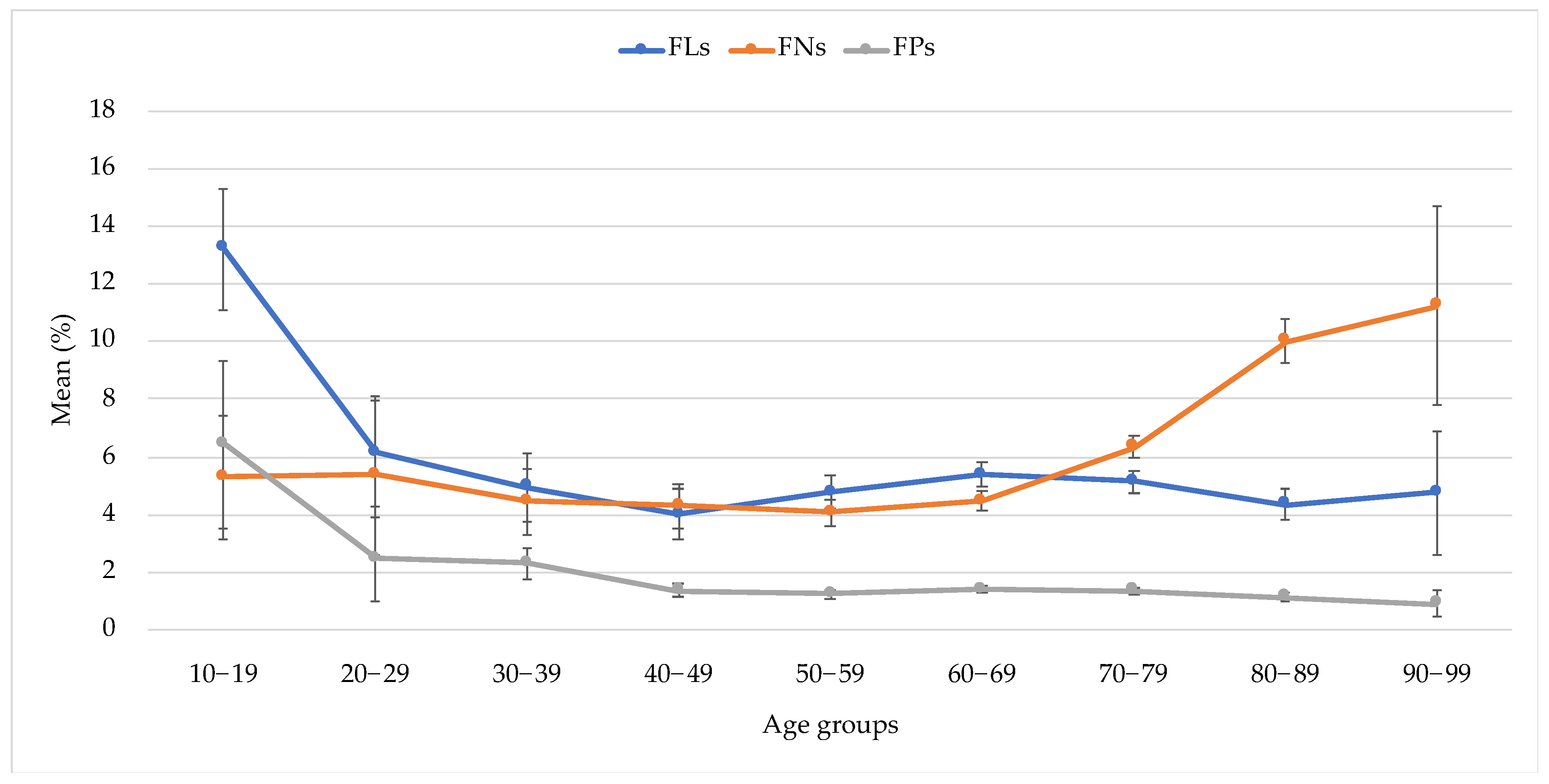
Table 5 for the FLs, FNs, and FPs, respectively. The FLs, FNs, and FPs were the lowest in their 40 s, 50 s, and 90 s, respectively. Each reliability index changes differently with aging (
Figure 2). The FLs were the highest in the first 10 s, decreased at 20 s, and remained constant after 20 s. The FNs remained constant for 60 s and rose up steeply after 70 s. The FPs reached their highest value in 10 s, after which they decreased gradually and remained constant after 40 s.
In order to further assess the influence of aging on the reliability indices, mixed-effect regression analyses on 40-year-old or older subjects were performed (
Table 6). Older age was significantly associated with higher FNs (
p <0.0001), but not with FLs (
p = 0.9014) and FPs (
p = 0.9267).
4. Discussion
We have previously investigated the relationships between age and the VF reliability indices in a 30-2 dataset [
20]. In subjects who are 40 years old or older, the mean ages of the two datasets (the 10-2 test from this study and the 30-2 test from our previous study) were virtually equivalent (68.8 years for the 10-2 and 68.4 years for the 30-2), while the MDs were distinctly different (−16.1 dB for the 10-2 and −7.3 dB for the 30-2) (
Table 7). This might reflect the actual operational situation, where the 10-2 perimetry was often tested on people with a relatively poor VF who had difficulty being evaluated with the 30-2 perimetry. For the reliability indices, the mean values for the FLs and FPs were lower in the 10-2 dataset (5.0% and 1.3%, respectively) than in the 30-2 dataset (8.1% and 2.4%, respectively) (
p < 0.0001 for both comparisons), but the value of the FNs was not different between both datasets (6.0% for the 10-2 and 4.9% for the 30-2;
p = 0.9364). Since the 10-2 perimetry test requires gazing at a smaller area than the 30-2 perimetry test, it makes sense that the fixation would be better and subsequent false positives would be reduced in the 10-2 test than in the 30-2 test. Especially for the FL, the value seems to have decreased more significantly in the 10-2 test than in the 30-2 test because the same blind spot method is used in the SITA Standard for both the 10-2 and the 30-2 programs [
21,
22], even though the 10-2 test has a narrower visual field presentation range. The FNs could also be lower in a smaller gazing area, such as in the 10-2 test, but the result was not. This may be due to the fact that the 10-2 subjects had a lower MD value than the 30-2 subjects. It has been reported that the FNs were elevated in eyes with reduced retinal sensitivity, such as those with reduced MD values [
3,
7,
19], and, therefore, it is possible that the improvement of the FN value in the 10-2 program was canceled by the patient’s background of having a lower MD value, although this speculation requires further study. In the central 30 degrees, the variability of the measured threshold values is highly dependent on eccentricity; reproducibility decreases when eccentricity increases [
23]. Thus, independent from the MD value, the difference in the test field might explain the differences in the reliability indices between the 10-2 and 30-2 tests observed in this study.
Considering the results of
Table 3,
Table 4 and
Table 5 and
Figure 2, we found that the FLs, FNs, and FPs were the lowest in their 40 s, 50 s, and 90 s, respectively. Each reliability index changes differently with aging. The age-related transitions of the FLs and FPs were similar; they were the highest in the first 10 s and remained approximately constant after then. The maximum values of FLs and FPs and the minimum value of FNs might be explained by the influence of high sensitivity and restlessness in the teenage years. The younger age groups likely consisted of more first-time test takers than the older age groups; thus, the learning effects could be another explanation for the relatively stable transition of the reliability indices in the middle-age groups. On the other hand, the steep elevation of FNs in 70 s indicated the aging effect. Interestingly, the same steep elevation of FNs in 70 s was found in our previous study of the 30-2 test [
20]. There have been several reports of anatomical and functional aging changes in the macula and perifoveal area [
24,
25]. The accumulation of debris in the sub-macular Bruch’s membrane increased remarkably at the age of 70 and older [
26]. Sixty percent of subjects over the age of 70 exhibited fundoscopic signs of early age-related maculopathy; even those free from these signs demonstrated sensitivity loss [
27]. In normal eyes, age-related VF sensitivity loss accelerates after the age of 70 [
28]. Thus, these anatomical and functional aging changes occurring around the age of 70 can explain the rapid increase of FNs in the 70 s seen in this study. It is well known that the FNs increase as the MD worsens, and that the MD can be expected to worsen with age as glaucoma severity increases. Thus, the findings in this study contained the bulk effects of aging on the reliability indices.
Regarding the association among the parameters for all ages (
Table 2), aging correlated significantly with FNs, with no significant correlation between age and FL or between age and FPs; our previous reports on the 30-2 test showed that all three reliability indices correlated significantly with aging [
20]. To exclude the effects derived from the small number of extreme cases, only the subjects aged 40 years or older were included in the multivariate analyses. The mixed-effect regression analyses, with the exclusion of the young subjects, showed a significant correlation between age and FNs, and no correlation between age and FLs or FPs, similar to the univariate analysis. In the previously reported 30-2 study, both the FLs and FNs were correlated with age [
20]. The reason for the lack of correlation between FL and aging in the 10-2 test results can be explained by the fact that the mean value and the range of FL values of the 10-2 dataset are smaller than those of the 30-2 dataset, as shown in
Table 7. The results suggest that the selection of the 10-2 program rather than the selection of the 30-2 program is an effective way to reduce the FL, especially in older subjects with severe VF loss.
This study has several limitations. First, we did not assess factors such as fatigue and loss of concentration, which might affect the results of the reliability indices. Previous studies reported that a longer testing time was associated with wider variations in the reliability indices [
29,
30,
31,
32]. Second, the absence of information regarding ocular pathology and clinical backgrounds, such as visual acuity, was also a limitation of this study. The steep increase in the FNs in the age groups of 70 and older might simply coincide with the occurrence of age-related eye diseases, such as cataract, age-related macular degeneration, and rapidly progressing types of glaucoma, including exfoliation glaucoma and primary angle closure diseases. Accordingly, we cannot exclude the possibility that the age-related worsening of the reliability indices would not be observed if the analyses were performed among subjects without any ocular pathologies and with good physical and phycological health. The results of this study are supposed to reflect real-world outcomes with diverse pathological and background factors. Third, the VF testing used in this study was obtained via several different models of the Humphrey VF analyzer; therefore, the stringency of the reliability index assessment might have changed with consecutive updates. Finally, we discussed the 10-2 results of the current study in comparison with the 30-2 results of the previous study; for this purpose, we only performed simple statistical comparisons of the parameters. In the future, enough statistical comparison between the 10-2 and 30-2 datasets would provide a deeper understanding of the reliability indices.





{kind=link}
{kind=link}