
Preferred Treatment with Curative Intent for Left Lateral Segment Early Hepatocellular Carcinoma under the Era of Minimal Invasive Surgery

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Method
2.1. Patients
2.2. Diagnosis and Treatment of HCC
2.3. Follow-Up and Surveillance
2.4. Statistics
3. Results
3.1. Patient Characteristics
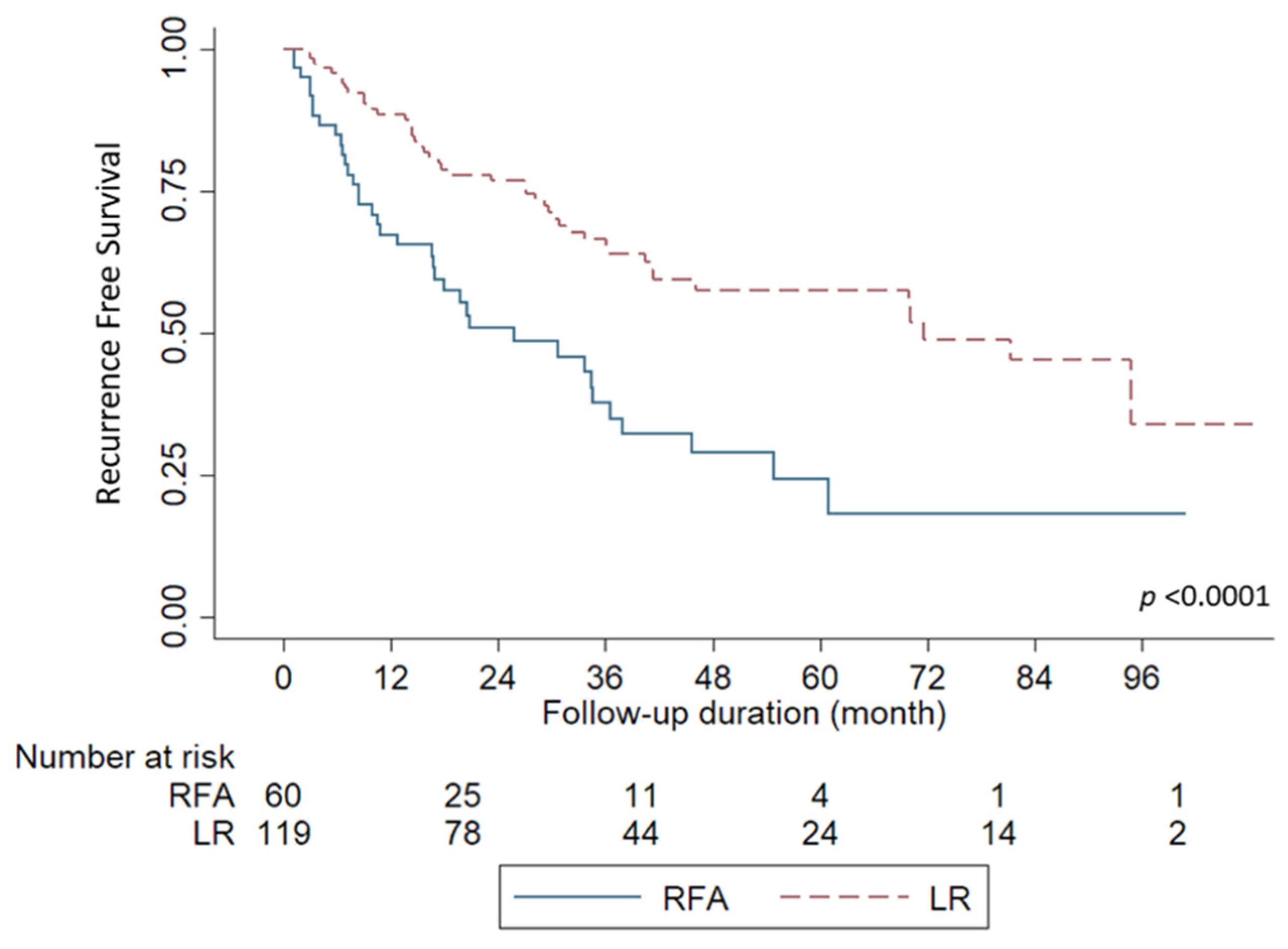
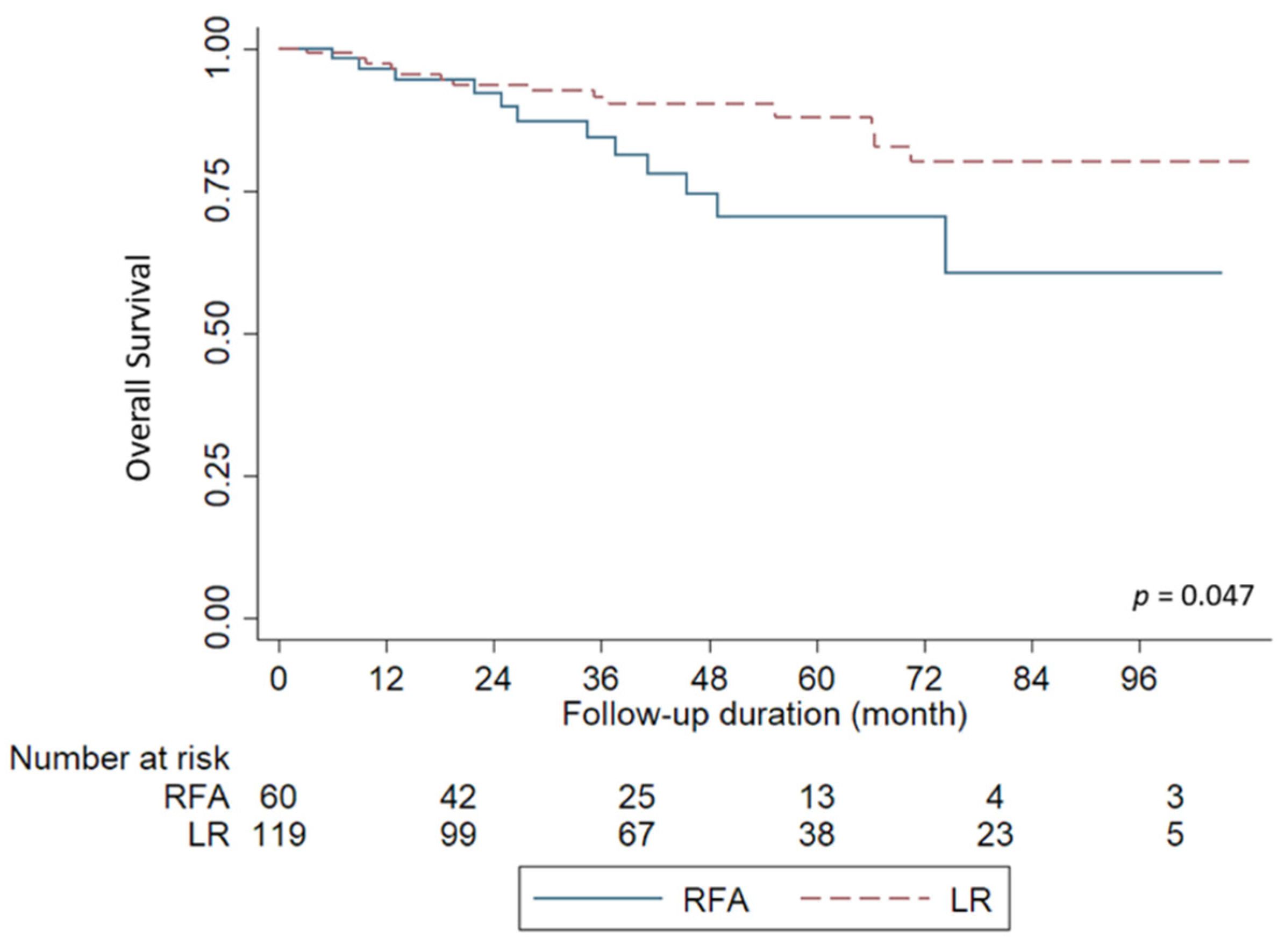
3.2. Survival Outcomes
3.3. Risk Factors for HCC Recurrence
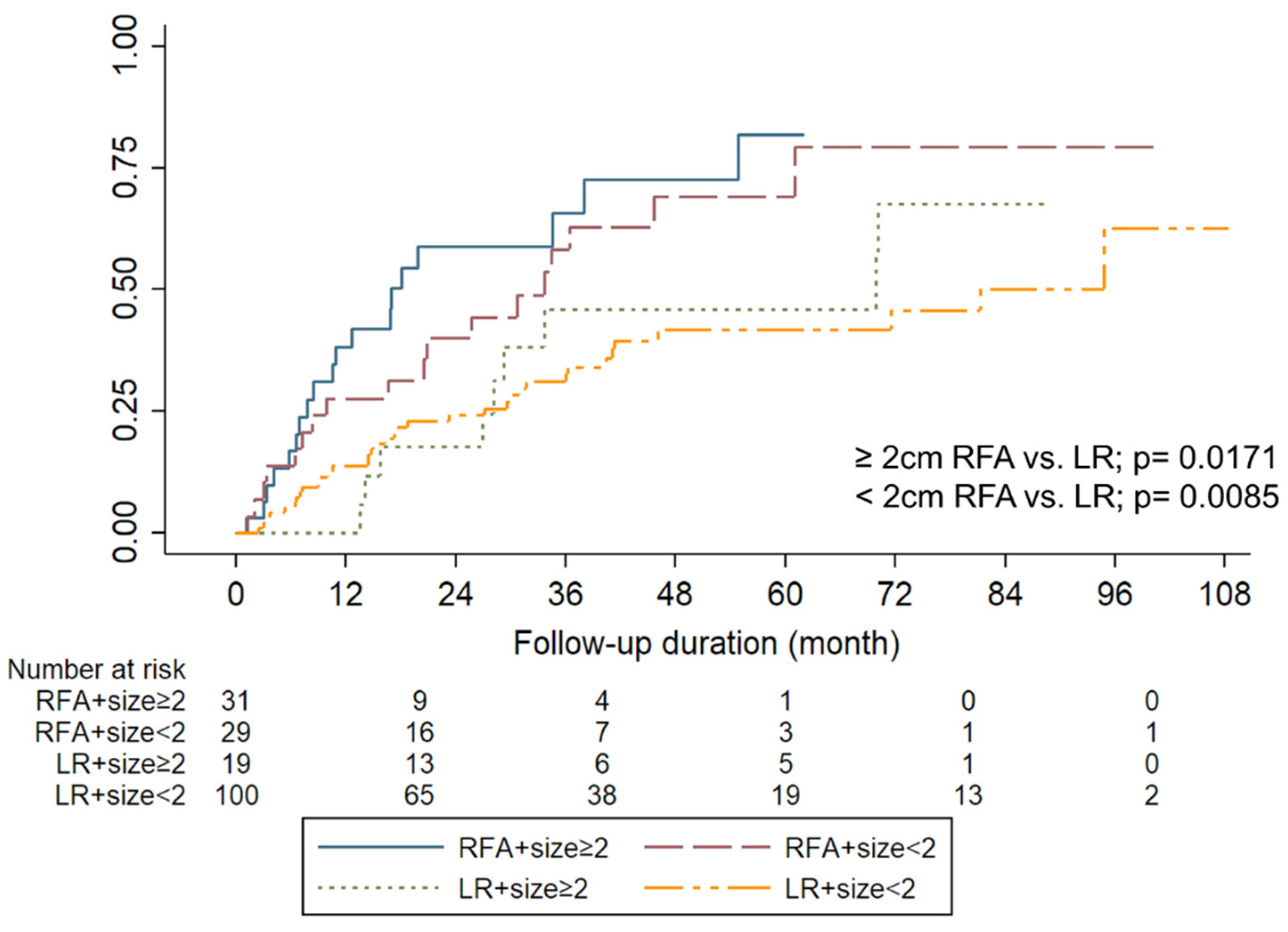
3.4. Small HCC (<2 cm)
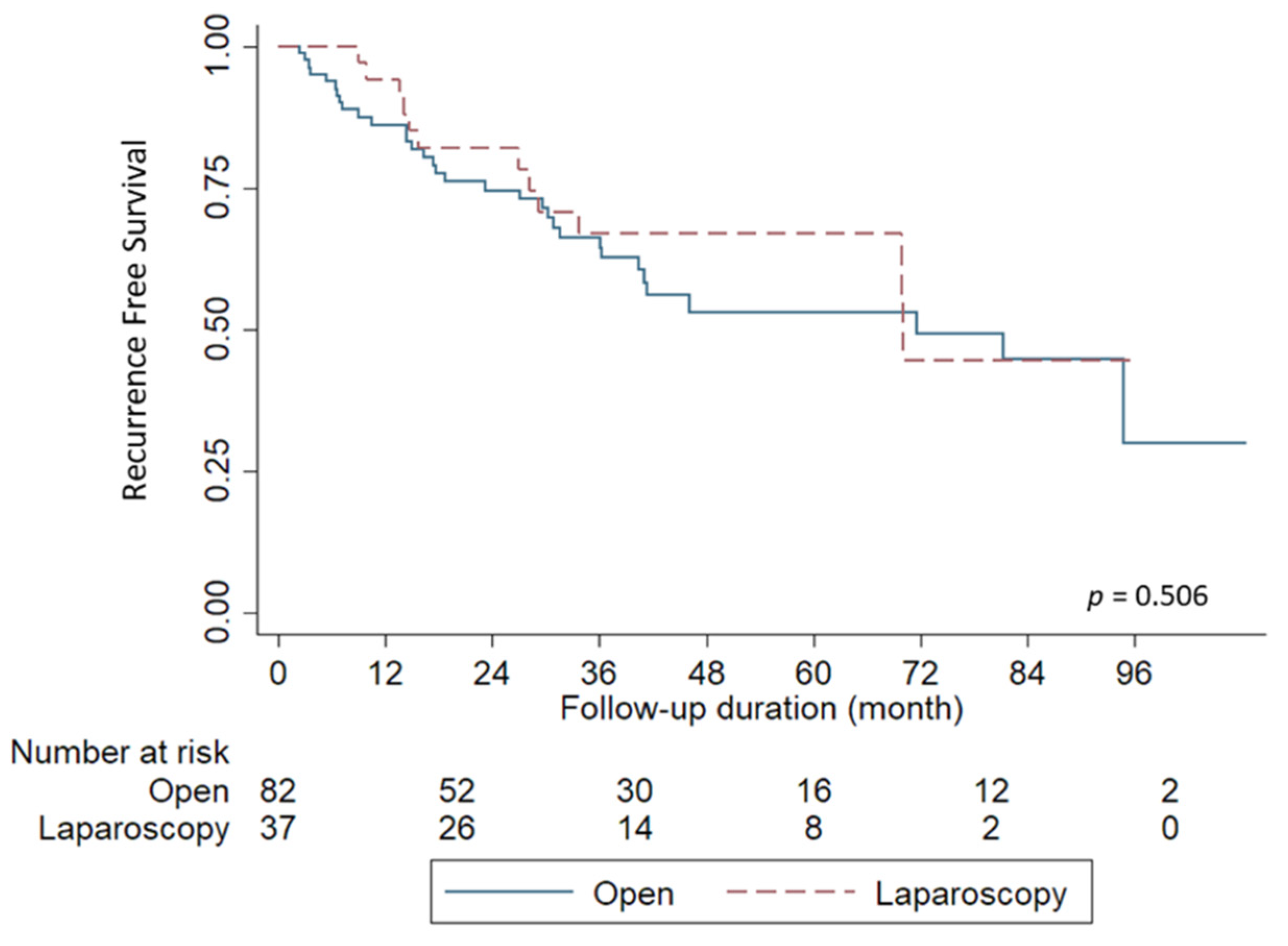
3.5. Liver Resection by Laparoscopy or Open Method
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ng, K.K.C.; Chok, K.S.H.; Chan, A.C.Y.; Cheung, T.T.; Wong, T.C.L.; Fung, J.Y.Y.; Yuen, J.; Poon, R.T.P.; Fan, S.T.; Lo, C.M. Randomized clinical trial of hepatic resection versus radiofrequency ablation for early-stage hepatocellular carcinoma. Br. J. Surg. 2017, 104, 1775–1784. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.-L.; Liu, X.-D.; Liang, M.; Luo, B.-M. Radiofrequency Ablation versus Hepatic Resection for Small Hepatocellular Carcinoma: Systematic Review of Randomized Controlled Trials with Meta-Analysis and Trial Sequential Analysis. Radiology 2018, 287, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kang, T.W.; Cha, D.I.; Song, K.D.; Lee, M.W.; Rhim, H.; Lim, H.K.; Sinn, D.H.; Kim, J.M.; Kim, K. Radiofrequency ablation vs. surgery for perivascular hepatocellular carcinoma: Propensity score analyses of long-term outcomes. J. Hepatol. 2018, 69, 70–78. [Google Scholar] [CrossRef]
- Lee, M.W.; Rhim, H.; Cha, D.I.; Kim, Y.J.; Lim, H.K. Planning US for Percutaneous Radiofrequency Ablation of Small Hepatocellular Carcinomas (1–3 cm): Value of Fusion Imaging with Conventional US and CT/MR Images. J. Vasc. Interv. Radiol. 2013, 24, 958–965. [Google Scholar] [CrossRef]
- Song, K.D.; Lee, M.W.; Rhim, H.; Kang, T.W.; Cha, D.I.; Sinn, D.H.; Lim, H.K. Percutaneous US/MRI Fusion–guided Radiofrequency Ablation for Recurrent Subcentimeter Hepatocellular Carcinoma: Technical Feasibility and Therapeutic Outcomes. Radiology 2018, 288, 878–886. [Google Scholar] [CrossRef]
- Kondo, Y.; Yoshida, H.; Shiina, S.; Tateishi, R.; Teratani, T.; Omata, M. Artificial ascites technique for percutaneous radiofrequency ablation of liver cancer adjacent to the gastrointestinal tract. Br. J. Surg. 2006, 93, 1277–1282. [Google Scholar] [CrossRef]
- Wang, C.-C.; Kao, J.-H. Artificial ascites is feasible and effective for difficult-to-ablate hepatocellular carcinoma. Hepatol. Int. 2015, 9, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.S.; Raman, S.S.; Limanond, P.; Aziz, D.; Economou, J.; Busuttil, R.; Sayre, J. Influence of Large Peritumoral Vessels on Outcome of Radiofrequency Ablation of Liver Tumors. J. Vasc. Interv. Radiol. 2003, 14, 1267–1274. [Google Scholar] [CrossRef]
- Wakamatsu, T.; Ogasawara, S.; Chiba, T.; Yokoyama, M.; Inoue, M.; Kanogawa, N.; Saito, T.; Suzuki, E.; Ooka, Y.; Tawada, A.; et al. Impact of Radiofrequency Ablation-Induced Glisson’s Capsule-Associated Complications in Patients with Hepatocellular Carcinoma. PLoS ONE 2017, 12, e0170153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koda, M.; Murawaki, Y.; Hirooka, Y.; Kitamoto, M.; Ono, M.; Sakaeda, H.; Joko, K.; Sato, S.; Tamaki, K.; Yamasaki, T.; et al. Complications of radiofrequency ablation for hepatocellular carcinoma in a multicenter study: An analysis of 16 346 treated nodules in 13 283 patients. Hepatol. Res. 2012, 42, 1058–1064. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Nitta, H.; Sasaki, A.; Takahara, T.; Ito, N.; Fujita, T.; Kanno, S.; Nishizuka, S.; Wakabayashi, G. Laparoscopic left lateral sectionectomy as a training procedure for surgeons learning laparoscopic hepatectomy. J. Hepato-Biliary-Pancreat. Sci. 2013, 20, 525–530. [Google Scholar] [CrossRef]
- Kim, J.M.; Kang, T.W.; Kwon, C.H.; Joh, J.W.; Ko, J.S.; Park, J.B.; Rhim, H.; Lee, J.H.; Kim, S.J.; Paik, S.W. Single hepatocellular carcinoma ≤ 3 cm in left lateral segment: Liver resection or radiofrequency ablation? World J. Gastroenterol. 2014, 20, 4059–4065. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-C.; Lin, C.-J.; Hsu, C.-W.; Chen, Y.-C.; Chen, W.-T.; Lin, S.-M. Fine-needle aspiration cytology to distinguish dysplasia from hepatocellular carcinoma with different grades. J. Gastroenterol. Hepatol. 2008, 23, e146–e152. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M.; Llovet, J.M.; Beaugrand, M.; Lencioni, R.; Burroughs, A.K.; Christensen, E.; Pagliaro, L.; Colombo, M.; Rodés, J. Clinical Management of Hepatocellular Carcinoma. Conclusions of the Barcelona-2000 EASL Conference. J. Hepatol. 2001, 35, 421–430. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M. Practice Guidelines Committee AAftSoLD. Management of hepatocellular carcinoma. Hepatology 2005, 42, 1208–1236. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Renzulli, M.; Golfieri, R.; Bologna Liver Oncology Group (BLOG). Proposal of a new diagnostic algorithm for hepatocellular carcinoma based on the Japanese guidelines but adapted to the Western world for patients under surveillance for chronic liver disease. J. Gastroenterol. Hepatol. 2015, 31, 69–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, K.; Yan, J.; Li, X.; Xia, F.; Ma, K.; Wang, S.; Bie, P.; Dong, J. A randomized controlled trial of radiofrequency ablation and surgical resection in the treatment of small hepatocellular carcinoma. J. Hepatol. 2012, 57, 794–802. [Google Scholar] [CrossRef]
- Huang, J.; Yan, L.; Cheng, Z.; Wu, H.; Du, L.; Wang, J.; Xu, Y.; Zeng, Y. A Randomized Trial Comparing Radiofrequency Ablation and Surgical Resection for HCC Conforming to the Milan Criteria. Ann. Surg. 2010, 252, 903–912. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.W.; Lee, J.M.; Yoon, J.-H.; Kim, Y.J.; Park, J.-W.; Park, S.-J.; Kim, S.H.; Yi, N.-J.; Suh, K.-S. A prospective randomized study comparing radiofrequency ablation and hepatic resection for hepatocellular carcinoma. Ann. Surg. Treat. Res. 2018, 94, 74–82. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.-S.; Li, J.-Q.; Zheng, Y.; Guo, R.; Liang, H.-H.; Zhang, Y.-Q.; Lin, X.-J.; Lau, W.Y. A Prospective Randomized Trial Comparing Percutaneous Local Ablative Therapy and Partial Hepatectomy for Small Hepatocellular Carcinoma. Ann. Surg. 2006, 243, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.W.; Ahn, K.S.; Kim, S.W.; Kim, T.S.; Kim, Y.H.; Kang, K.J. Liver Resection Versus Local Ablation Therapies for Hepatocellular Carcinoma Within the Milan Criteria: A Systematic Review and Meta-analysis. Ann. Surg. 2021, 273, 656–666. [Google Scholar] [CrossRef]
- Xu, X.F.; Xing, H.; Han, J.; Li, Z.L.; Lau, W.Y.; Zhou, Y.H.; Gu, W.M.; Wang, H.; Chen, T.H.; Zeng, Y.Y.; et al. Risk Factors, Patterns, and Outcomes of Late Recurrence After Liver Resection for Hepatocellular Carcinoma: A Multicenter Study From China. JAMA Surg. 2019, 154, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Shehta, A.; Han, H.-S.; Ahn, S.; Yoon, Y.-S.; Cho, J.Y.; Choi, Y. Post-resection recurrence of hepatocellular carcinoma in cirrhotic patients: Is thrombocytopenia a risk factor for recurrence? Surg. Oncol. 2016, 25, 364–369. [Google Scholar] [CrossRef]
- Chan, K.-M.; Lee, W.-C.; Hung, C.-F.; Yu, M.-C.; Jan, Y.-Y.; Chen, M.-F. Aggressive multimodality treatment for intra-hepatic recurrence of hepatocellular carcinoma following hepatic resection. Chang. Gung Med. J. 2005, 28, 543–550. [Google Scholar]
- Facciorusso, A.; Del Prete, V.; Antonino, M.; Crucinio, N.; Neve, V.; Di Leo, A.; Carr, B.; Barone, M. Post-recurrence survival in hepatocellular carcinoma after percutaneous radiofrequency ablation. Dig. Liver Dis. 2014, 46, 1014–1019. [Google Scholar] [CrossRef]
- Livraghi, T.; Goldberg, S.N.; Lazzaroni, S.; Meloni, F.; Ierace, T.; Solbiati, L.; Gazelle, G.S. Hepatocellular Carcinoma: Radio-frequency Ablation of Medium and Large Lesions. Radiology 2000, 214, 761–768. [Google Scholar] [CrossRef]
- Schullian, P.; Johnston, E.W.; Putzer, D.; Eberle, G.; Laimer, G.; Bale, R. Safety and efficacy of stereotactic radiofrequency ablation for very large (>/=8 cm) primary and metastatic liver tumors. Sci. Rep. 2020, 10, 1618. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Bellanti, F.; Villani, R.; Salvatore, V.; Muscatiello, N.; Piscaglia, F.; Vendemiale, G.; Serviddio, G. Transarterial chemoembolization vs bland embolization in hepatocellular carcinoma: A meta-analysis of randomized trials. United Eur. Gastroenterol. J. 2017, 5, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Deng, T.; Zeng, L.; Chen, W. Efficacy and safety of radiofrequency ablation and transcatheter arterial chemoembolization for treatment of hepatocellular carcinoma: A meta-analysis. Hepatol. Res. 2015, 46, 58–71. [Google Scholar] [CrossRef]
- Ciria, R.; Cherqui, D.; Geller, D.A.; Briceno, J.; Wakabayashi, G. Comparative Short-term Benefits of Laparoscopic Liver Resection: 9000 Cases and Climbing. Ann. Surg. 2016, 263, 761–777. [Google Scholar] [CrossRef]
- Buell, J.F.; Cherqui, D.; Geller, D.A.; O’Rourke, N.; Iannitti, D.; Dagher, I.; Koffron, A.J.; Thomas, M.; Gayet, B.; Han, H.S.; et al. The international position on laparoscopic liver surgery: The Louisville Statement, 2008. Ann. Surg. 2009, 250, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Fuks, D.; Aldrighetti, L.; Jiao, L.R.; Wakabayashi, G.; Limongelli, P. Laparoscopic Management of Hepatocellular Carcinoma: A Critical Reappraisal. Surg. Laparosc. Endosc. Percutaneous Tech. 2017, 27, 203–205. [Google Scholar] [CrossRef] [PubMed]
- Ogiso, S.; Seo, S.; Eso, Y.; Yoh, T.; Kawai, T.; Okumura, S.; Ishii, T.; Fukumitsu, K.; Taura, K.; Seno, H.; et al. Laparoscopic liver resection versus percutaneous radiofrequency ablation for small hepatocellular carcinoma. HPB 2021, 23, 533–537. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall (n = 179) | RFA (n = 60) | LR (n = 119) | p Value |
|---|---|---|---|---|
| Age, median (range) <50 years ≥50 years | 60.1 (36.5–90.9) 8 (4.5) 171 (95.5) | 71.7 (50.2–90.6) 0 (0) 60 (100.0) | 64.97 (36.54–90.9) 8 (6.7) 111 (93.3) | 0.0011 0.0399 |
| Sex Male Female | 123 (68.7) 56 (31.3) | 35 (58.3) 25 (41.7) | 88 (74.0) 31 (26.0) | 0.0334 |
| Cirrhosis No Yes | 47 (26.4) 132 (73.6) | 3 (5.0) 57 (95.0) | 44 (37.3) 75 (62.7) | <0.0001 |
| Etiology HBV HCV HBV+HCV | 78 (43.6) 48 (26.8) 7 (3.9) | 18 (30.0) 24 (40.0) 2 (3.3) | 60 (50.5) 24 (20.1) 5 (4.2) | 0.0075 |
| Others | 46 (25.7) | 16(26.7) | 30 (25.2) | |
| Tumor Number, median (range) | 1 (1–3) | 1 (1–3) | 1.00 (1.0–3.0) | 0.2987 |
| Tumor size (cm), median (range) | 2.3 (0.6–9.1) | 2.0 (0.9–5.2) | 2.7 (0.6–9.1) | 0.0113 |
| TNM Stage Stage I Stage II | 118 (65.9) 35 (19.5) | 51 (85.0) 7 (11.7) | 67 (56.3) 28 (23.5) | 0.0129 |
| Platelet, median (range) <10 × 103/μL ≥10 × 103/μL | 147.0 (30.0–536.0) 43 (24.1) 136 (75.9) | 112.0 (30.0–381.0) 26 (43.3) 34 (56.7) | 168.0 (38.0–536.0) 17 (14.3) 102 (85.7) | <0.0001 <0.0001 |
| AFP (ng/mL), median (range) | 21.2 (1.7–136275.9) | 23.7 (2.3–21075.7) | 20.1 (1.7–136275.9) | 0.2514 |
| HCC recurrence | 81(45.3) | 36 (61.6) | 45 (37.8) | 0.0025 |
| * HCC recurrent pattern | 0.0021 | |||
| Local intrahepatic | 7 (8.6) | 7 (19.4) | 0 (0) | |
| Distant intrahepatic | 67 (82.8) | 25 (69.4) | 42 (93.3) | |
| Systemic metastasis | 7 (8.6) | 4 (11.2) | 3 (6.7) | |
| Complications (≥grade II) | 11(6.2) | 3 (5.0) | 8 (6.7) | 0.6519 |
| Hospital stay, days, median (range) | 3 (2–9) | 7 (4–38) | <0.0001 |
| Variables | Overall (n = 179) | Recurrence (n = 81) | Crude HR (95% CI) | p Value | Multivariate HR (95% CI) | p Value |
|---|---|---|---|---|---|---|
| Age, median(range) <50 years ≥50 years | 60.1 (36.5–90.9) 8 (4.5) 171 (95.5) | 68.6 (38.6–90.8) 2 (2.5) 79 (97.5) | 1.024 (1.004–1.045) 1.0 2.402 (0.589–9.794) | 0.0197 0.2216 | 1.022 (1.000–1.046) | 0.0550 |
| Sex Male Female | 123 (68.7) 56 (31.3) | 62 (76.5) 19 (23.5) | 1.0 0.750 (0.449–1.253) | 0.2714 | ||
| Cirrhosis No Yes | 47 (26.4) 132 (73.6) | 12 (14.8) 69 (85.2) | 1.0 2.353 (1.274–4.343) | 0.0062 | 2.130 (1.113–4.075) | 0.0224 |
| Etiology HBV HCV HBV+HCV | 78 (43.6) 48 (26.8) 7 (3.9) | 40 (49.4) 21 (25.9) 2 (2.5) | 1.0 1.055 (0.619–1.796) 0.636 (0.153–2.635) | 0.8448 0.5322 | ||
| Others | 46 (25.7) | 18 (22.2) | 0.855 (0.494–1.478) | 0.5741 | ||
| Tumor Number | 1 (1–3) | 1 (1–3) | 2.909 (1.658–5.106) | 0.0002 | 3.209 (1.794–5.738) | <0.0001 |
| Tumor size (cm) | 2.3 (0.6–9.1) | 2.4 (0.8–8.0) | 1.011 (0.870–1.175) | 0.8823 | ||
| TNM Stage Stage I Stage II | 118 (65.9) 35 (19.5) | 53 (65.4) 15 (18.5) | 1.0 0.867 (0.489–1.539) | 0.6262 | ||
| Platelet <10 × 103/μL ≥10 × 103/μL | 43 (24.1) 136 (75.9) | 134.00 (30.0–531.0) 20 (24.7) 61 (75.3) | 1.0 0.727 (0.436–1.210) | 0.2198 | ||
| AFP (ng/mL) | 21.2(1.7–136275.9) | 32.5 (1.7–136275.9) | 1.000 (1.000–1.000) | 0.0623 | ||
| Treatment RFA LR | 60 (33.5) 119 (66.5) | 36 (37.8) 45 (61.6) | 2.426 (1.559–3.776) 1.0 | <0.0001 | 1.804 (1.127–2.886) | 0.0140 |
| Characteristic | Laparoscopy (n = 37) | Open (n = 82) | p Value |
|---|---|---|---|
| Age, median (range) <50 years ≥50 years | 64.4 (36.5–90.9) 2 (5.0) 35 (95.0) | 65.1 (39.9–90.1) 6 (7.32) 76 (92.68) | 0.9138 0.6999 |
| Sex Male Female | 30 (81.1) 7 (18.9) | 58 (70.7) 24 (29.3) | 0.2338 |
| Cirrhosis No Yes | 12 (32.4) 25 (67.6) | 33 (39.0) 49 (61.0) | 0.3163 |
| Etiology HBV HCV HBV+HCV | 21 (56.8) 8 (21.6) 1 (2.7) | 39 (47.6) 16 (19.5) 4 (4.8) | 0.7942 |
| Others | 7(18.9) | 23(28.1) | |
| Tumor Number, median (range) | 1.0 (1.0–2.0) | 1.0 (1.0–3.0) | 0.9077 |
| Tumor size (cm), median (range) | 2.6 (0.5–7.8) | 3.2 (0.9–9.10) | 0.1161 |
| TNM Stage Stage I Stage II | 26 (70.3) 11 (29.7) | 49 (59.8) 33 (40.2) | 0.2736 |
| Platelet, median (range) <10 × 103/μL ≥10 × 103/μL | 167.0 (95.0–312.0) 2 (5.4) 35 (94.6) | 179.0 (38.0–536.0) 15 (18.3) 67 (81.7) | 0.36 0.3319 |
| AFP (ng/mL), median (range) | 8.2 (1.7–24529.2) | 29.9 (2.2–136275.9) | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, T.-H.; Wang, Y.-C.; Hung, H.-C.; Lee, J.-C.; Wu, C.-Y.; Cheng, C.-H.; Lee, C.-F.; Wu, T.-J.; Chou, H.-S.; Chan, K.-M.; et al. Preferred Treatment with Curative Intent for Left Lateral Segment Early Hepatocellular Carcinoma under the Era of Minimal Invasive Surgery. J. Pers. Med. 2022, 12, 79. https://doi.org/10.3390/jpm12010079
Wu T-H, Wang Y-C, Hung H-C, Lee J-C, Wu C-Y, Cheng C-H, Lee C-F, Wu T-J, Chou H-S, Chan K-M, et al. Preferred Treatment with Curative Intent for Left Lateral Segment Early Hepatocellular Carcinoma under the Era of Minimal Invasive Surgery. Journal of Personalized Medicine. 2022; 12(1):79. https://doi.org/10.3390/jpm12010079
Chicago/Turabian StyleWu, Tsung-Han, Yu-Chao Wang, Hao-Chien Hung, Jin-Chiao Lee, Chia-Ying Wu, Chih-Hsien Cheng, Chen-Fang Lee, Ting-Jung Wu, Hong-Shiue Chou, Kun-Ming Chan, and et al. 2022. "Preferred Treatment with Curative Intent for Left Lateral Segment Early Hepatocellular Carcinoma under the Era of Minimal Invasive Surgery" Journal of Personalized Medicine 12, no. 1: 79. https://doi.org/10.3390/jpm12010079