
Efficacy and Safety of Enoxaparin versus New Oral Anticoagulants to Prevent Venous Thromboembolism after Total Hip Replacement: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Results
2.1. Study Identification
2.2. Study Characteristics
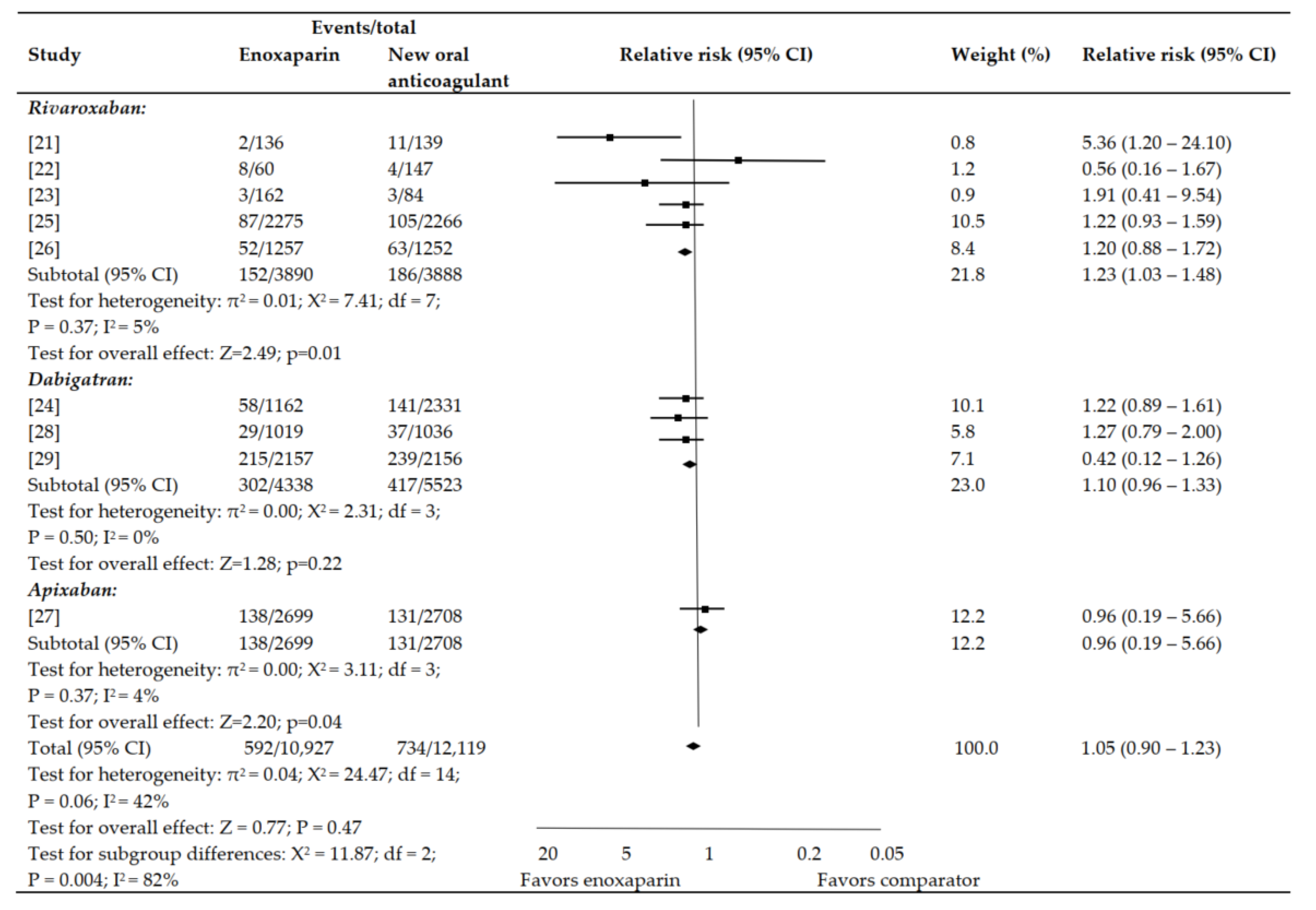
2.3. Primary Efficacy Outcome Analysis
2.4. Secondary Efficacy Outcome Analysis
2.5. Primary Safety Outcome Analysis
2.6. Secondary Safety Outcome Analysis
2.7. Net Clinical Endpoint
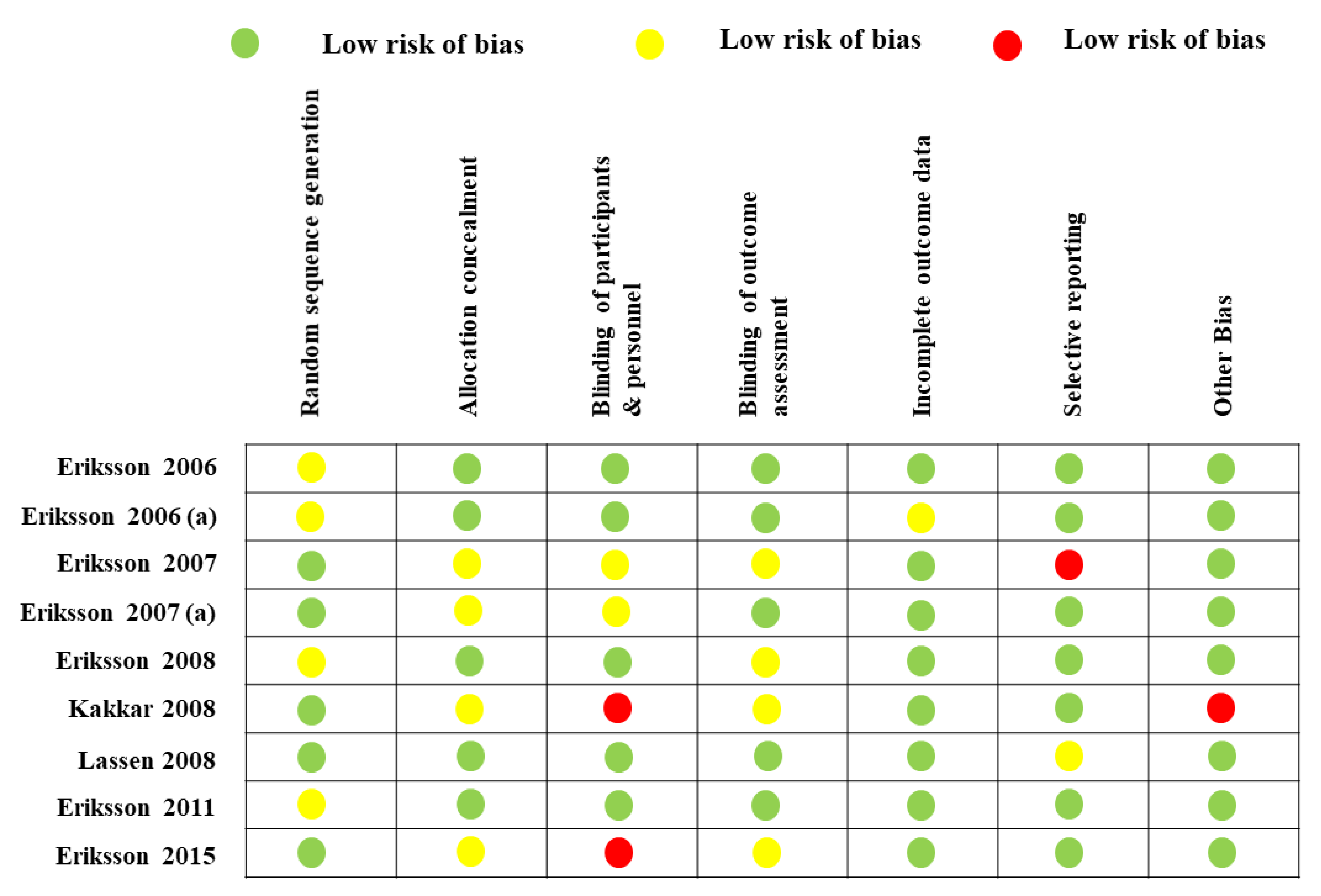
2.8. Risk of Bias
2.9. Indirect Comparisons
2.10. Absolute Difference in Events per One Thousand Subjects
3. Discussion
4. Materials and Methods
4.1. Data Sources
4.2. Study Selection
- RDBCTs that reported the effectiveness and safety of enoxaparin (with approved doses of 40 mg/day initiated 12 h prior to surgery [Europe] or 30 mg twice/day initiated 12–24 h after surgery [North America]) for thromboprophylaxis in comparison to either of the new oral anticoagulants (rivaroxaban with an approved dose of 10 mg once/day, apixaban with an approved dose of 5 mg once/day, or dabigatran with an approved dose of 150 mg or 220 mg once/day);
- RDBCTs that included human patients of all ages undergoing THR;
- RDBCTs that provided safety/efficacy information such as any DVT diagnosed by venography, hemorrhage, major bleeding, or pulmonary embolism (as defined by the authors);
- All other studies were excluded.
4.3. Data Extraction
4.4. Assessed Outcomes
4.5. Assessment of Methodological Quality
4.6. Statistical Analysis
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: Total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef]
- Select Committee on Health Written Evidence. Appendix 6. Available online: https://publications.parliament.uk/pa/cm200405/cmselect/cmhealth/99/99we07.htm (accessed on 28 December 2019).
- Eikelboom, J.W.; Quinlan, D.J.; Douketis, J.D. Extended-duration prophylaxis against venous thromboembolism after total hip or knee replacement: A meta-analysis of the randomized trials. Lancet 2001, 358, 9–15. [Google Scholar] [CrossRef]
- Bala, A.; Huddleston, J.I., III; Goodman, S.B.; Maloney, W.J.; Amanatullah, D.F. Venous thromboembolism prophylaxis after TKA: Aspirin, warfarin, enoxaparin, or factor Xa inhibitors? Clin. Orthop. Relat. Res. 2017, 475, 2205–2213. [Google Scholar] [CrossRef] [Green Version]
- European Medicines Agency. Pradaxa ®—Summary of Product Characteristics. 2011. Available online: www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000829/WC500041059.pdf (accessed on 31 July 2021).
- European Medicines Agency. Eliquis ®—Summary of Product Characteristics; European Medicines Agency: Amsterdam, The Netherlands, 2011.
- Available online: www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002148/WC500107728.pdf (accessed on 31 July 2021).
- European Medicines Agency. Xarelto ®—Summary of Product Characteristics; European Medicines Agency: Amsterdam, The Netherlands, 2011.
- Available online: www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000944/WC500057108.pdf (accessed on 31 July 2021).
- Parvizi, J.; Ceylan, H.H.; Kucukdurmaz, F.; Merli, G.; Tuncay, I.; Beverland, D. Venous thromboembolism following hip and knee arthroplasty: The role of aspirin. J. Bone. Jt. Surg. Am. 2017, 99, 961–972. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Orthopaedic Surgeons. Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty: Evidence-Based Guideline and Evidence Report. Available online: https://www.aaos.org/uploadedFiles/PreProduction/Quality/Guidelines_and_Reviews/VTE_fullguideline_10.31.16.pdf (accessed on 20 December 2019).
- Falck-Ytter, Y.; Francis, C.W.; Johanson, N.A.; Curley, C.; Dahl, O.E.; Schulman, S.; Ortel, T.L.; Pauker, S.G.; Colwell, C.W., Jr. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2012, 141, e278S–e325S. [Google Scholar] [PubMed] [Green Version]
- National Institute for Health and Care Excellence (NICE). Venous Thromboembolism in Over 16s: Reducing the Risk of Hospital-Acquired Deep Vein Thrombosis or Pulmonary Embolism. NICE Guideline [NG89]. Available online: https://www.nice.org.uk/guidance/ng89 (accessed on 20 December 2019).
- Monreal, M.; Folkerts, K.; Diamantopoulos, A.; Imberti, D.; Brosa, M. Cost-effectiveness impact of rivaroxaban versus new and existing prophylaxis for the prevention of venous thromboembolism after total hip or knee replacement surgery in France, Italy and Spain. Thromb. Haemost. 2013, 110, 987–994. [Google Scholar] [CrossRef]
- Brockbank, J.; Wolowacz, S. Economic evaluations of new oral anticoagulants for the prevention of venous thromboembolism after total hip or knee replacement: A systematic review. Pharmacoeconomics 2017, 35, 517–535. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, B.I.; Borris, L.; Dahl, O.E.; Haas, S.; Huisman, M.V.; Kakkar, A.K.; Misselwitz, F.; Kälebo, P.; ODIXa-HIP Study Investigators. Oral, direct Factor Xa inhibition with BAY 59-7939 for the prevention of venous thromboembolism after total hip replacement. J. Thromb. Haemost. 2006, 4, 121–128. [Google Scholar] [CrossRef]
- Eriksson, B.I.; Borris, L.C.; Dahl, O.E.; Haas, S.; Huisman, M.V.; Kakkar, A.K.; Muehlhofer, E.; Dierig, C.; Misselwitz, F.; Kälebo, P. A once-daily, oral, direct Factor Xa inhibitor, rivaroxaban (BAY 59-7939), for thromboprophylaxis after total hip replacement. Circulation 2006, 114, 2374–2381. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, B.I.; Borris, L.C.; Dahl, O.E.; Haas, S.; Huisman, M.V.; Kakkar, A.K.; Misselwitz, F.; Muehlhofer, E.; Kälebo, P. Dose-escalation study of rivaroxaban (BAY 59-7939)–an oral, direct Factor Xa inhibitor–for the prevention of venous thromboembolism in patients undergoing total hip replacement. Thromb. Res. 2007, 120, 685–693. [Google Scholar] [CrossRef]
- Eriksson, B.I.; Dahl, O.E.; Rosencher, N.; Kurth, A.A.; van Dijk, C.N.; Frostick, S.P.; Prins, M.H.; Hettiarachchi, R.; Hantel, S.; Schnee, J.; et al. Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: A randomised, double-blind, non-inferiority trial. Lancet 2007, 370, 949–956. [Google Scholar] [CrossRef]
- Eriksson, B.I.; Borris, L.C.; Friedman, R.J.; Haas, S.; Huisman, M.V.; Kakkar, A.K.; Bandel, T.J.; Beckmann, H.; Muehlhofer, E.; Misselwitz, F.; et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N. Eng. J. Med. 2008, 358, 2765–2775. [Google Scholar] [CrossRef] [Green Version]
- Kakkar, A.K.; Brenner, B.; Dahl, O.E.; Eriksson, B.I.; Mouret, P.; Muntz, J.; Soglian, A.G.; Pap, Á.F.; Misselwitz, F.; Haas, S.; et al. Extended duration rivaroxaban versus short-term enoxaparin for the prevention of venous thromboembolism after total hip arthroplasty: A double-blind, randomised controlled trial. Lancet 2008, 372, 31–39. [Google Scholar] [CrossRef]
- Lassen, M.R.; Gallus, A.; Raskob, G.E.; Pineo, G.; Chen, D.; Ramirez, L.M. Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. N. Eng. J. Med. 2010, 363, 2487–2498. [Google Scholar] [CrossRef]
- Eriksson, B.I.; Dahl, O.E.; Huo, M.H.; Kurth, A.A.; Hantel, S.; Hermansson, K.; Schnee, J.M.; Friedman, R.J.; RE-NOVATE II Study Group. Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE-NOVATE II). Thromb. Haemost. 2011, 105, 721–729. [Google Scholar]
- Eriksson, B.I.; Dahl, O.E.; Rosencher, N.; Clemens, A.; Hantel, S.; Feuring, M.; Kreuzer, J.; Huo, M.; Friedman, R.J. Oral dabigatran etexilate versus enoxaparin for venous thromboembolism prevention after total hip arthroplasty: Pooled analysis of two phase 3 randomized trials. Thromb. J. 2015, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Turun, S.; Banghua, L.; Yuan, Y.; Zhenhui, L.; Ying, N.; Jin, C. A systematic review of rivaroxaban versus enoxaparin in the prevention of venous thromboembolism after hip or knee replacement. Thromb. Res. 2011, 127, 525–534. [Google Scholar] [CrossRef]
- Rahman, S. Deep vein thrombosis prophylaxis: Friend or foe. Am. J. Therap. 2009, 16, 300–303. [Google Scholar] [CrossRef]
- Geerts, W.H.; Bergqvist, D.; Pineo, G.F.; Heit, J.A.; Samama, C.M.; Lassen, M.R.; Colwell, C.W. Prevention of venous thromboembolism: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2008, 133, 381S–453S. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.; Treasure, T. Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital: Summary of the NICE guideline. Heart 2010, 96, 879–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Autar, R. A review of the evidence for the efficacy of Anti-Embolism Stockings (AES) in Venous Thromboembolism (VTE) prevention. J. Orthop. Nurs. 2009, 13, 41–49. [Google Scholar] [CrossRef]
- Samama, M.M.; Cohen, A.T.; Darmon, J.Y.; Desjardins, L.; Eldor, A.; Janbon, C.; Leizorovicz, A.; Nguyen, H.; Olsson, C.G.; Turpie, A.G.; et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. N. Eng. J. Med. 1999, 341, 793–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leizorovicz, A.; Cohen, A.T.; Turpie, A.G.; Olsson, C.G.; Vaitkus, P.T.; Goldhaber, S.Z. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation 2004, 110, 874–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Zhao, J.; Yan, Y.; Su, J. Effectiveness and safety of rivaroxaban for the prevention of thrombosis following total hip or knee replacement: A systematic review and meta-analysis. Medicine 2019, 98, e14539. [Google Scholar] [CrossRef]
- Yoshida, R.D.A.; Yoshida, W.B.; Rollo, H.D.A. New anticoagulants for the prophylaxis of venous thromboembolism. J. Vasc. Brasileiro. 2011, 10, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Ufer, M. Comparative efficacy and safety of the novel oral anticoagulants dabigatran, rivaroxaban and apixaban in preclinical and clinical development. Thromb. Haemost. 2010, 103, 572–585. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, B.I.; Quinlan, D.J.; Eikelboom, J.W. Novel oral factor Xa and thrombin inhibitors in the management of thromboembolism. Ann. Rev. Med. 2011, 62, 41–57. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.B.; Zhang, J.D.; Shen, H.; Jiang, Y.Y. Rivaroxaban versus enoxaparin for thromboprophylaxis after total hip or knee arthroplasty: A meta-analysis of randomized controlled trials. Eur. J. Clin. Pharmacol. 2010, 66, 1099–1108. [Google Scholar] [CrossRef]
- Gómez-Outes, A.; Terleira-Fernández, A.I.; Suárez-Gea, M.L.; Vargas-Castrillón, E. Dabigatran, rivaroxaban, or apixaban versus enoxaparin for thromboprophylaxis after total hip or knee replacement: Systematic review, meta-analysis, and indirect treatment comparisons. BMJ 2012, 344, e3675. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Cao, Y.; Liao, C.; Wu, L.; Gao, F. Apixaban versus enoxaparin in patients with total knee arthroplasty. Thromb. Haemost. 2011, 105, 245–253. [Google Scholar] [CrossRef] [Green Version]
- Huisman, M.; Quinlan, D.; Dahl, O.; Schulman, S. Enoxaparin versus Dabigatran or rivaroxaban for thromboprophylaxis after hip or knee arthroplasty: Results of separate pooled analyses of phase III multicenter randomized trials. Circulation 2010, 3, 652–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolowacz, S.E.; Roskell, N.S.; Plumb, J.M.; Caprini, J.A.; Eriksson, B.I. Efficacy and safety of dabigatran etexilate for the prevention of venous thromboembolism following total hip or knee arthroplasty. Thromb. Haemost. 2009, 101, 77–85. [Google Scholar]
- Friedman, R.J.; Dahl, O.E.; Rosencher, N.; Caprini, J.A.; Kurth, A.A.; Francis, C.W.; Clemens, A.; Hantel, S.; Schnee, J.M.; Eriksson, B.I. Dabigatran versus enoxaparin for prevention of venous thromboembolism after hip or knee arthroplasty: A pooled analysis of three trials. Thromb. Res. 2010, 126, 175–182. [Google Scholar] [CrossRef]
- Turpie, A.G.; Lassen, M.R.; Eriksson, B.I.; Gent, M.; Berkowitz, S.D.; Misselwitz, F.; Bandel, T.J.; Homering, M.; Westermeier, T.; Kakkar, A.K. Rivaroxaban for the prevention of venous thromboembolism after hip or knee arthroplasty. Thromb. Haemost. 2011, 105, 444–453. [Google Scholar]
- Hull, R.D.; Liang, J.; Brant, R. Pooled analysis of trials may, in the presence of heterogeneity inadvertently lead to fragile conclusions due to the importance of clinically relevant variables being either hidden or lost when the findings are pooled. Thromb. Res. 2010, 126, 164–165. [Google Scholar] [CrossRef]
- Merli, G.; Spyropoulos, A.C.; Caprini, J.A. Use of emerging oral anticoagulants in clinical practice: Translating results from clinical trials to orthopedic and general surgical patient populations. Ann. Surg. 2009, 250, 219–228. [Google Scholar] [CrossRef]
- Dahl, O.E.; Kurth, A.A.; Rosencher, N.; Noack, H.; Clemens, A.; Eriksson, B.I. Thromboprophylaxis with dabigatran etexilate in patients over seventy-five years of age with moderate renal impairment undergoing or knee replacement. Int. Orthop. 2012, 36, 741–748. [Google Scholar] [CrossRef] [Green Version]
- Kearon, C. Natural history of venous thromboembolism. Circulation 2003, 107, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Bjørnarå, B.T.; Gudmundsen, T.E.; Dahl, O.E. Frequency and timing of clinical venous thromboembolism after major joint surgery. J. Bone Jt. Surg. Br. 2006, 88, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Nuki, G.; Moskowitz, R.W.; Abramson, S.; Altman, R.D.; Arden, N.K.; Bierma-Zeinstra, S.; Brandt, K.D.; Croft, P.; Doherty, M.; et al. OARSI Recommendations for the Management of Hip and Knee Osteoarthritis: Part III: Changes in Evidence Following Systematic Cumulative Update of Research Published through January 2009. Osteoarthr. Cartil. 2010, 18, 476–499. [Google Scholar] [CrossRef] [Green Version]
- National Insititute for Health and Care Excellence. Glossary. Available online: https://www.nice.org.uk/glossary?letter=e (accessed on 31 July 2021).
- Cohen, D. Out of joint: The story of the ASR. BMJ 2011, 342, d2905. [Google Scholar] [CrossRef] [Green Version]
- Morgan, M. Head, shoulders, knees, and toes-what’s next on the NHS waiting list? BMJ 2021, 372, n554. [Google Scholar] [CrossRef] [PubMed]
- Kynaston-Pearson, F.; Ashmore, A.M.; Malak, T.T.; Rombach, I.; Taylor, A.; Beard, D.; Arden, N.K.; Price, A.; Prieto-Alhambra, D.; Judge, A.; et al. Primary hip replacement prostheses and their evidence base: Systematic review of literature. BMJ 2013, 347, f6956. [Google Scholar] [CrossRef] [Green Version]
- Lohr, K.N.; Field, M.J. A provisional instrument for assessing clinical practice guidelines. In Guidelines for Clinical Practice. From Development to Use; Field, M.J., Lohr, K.N., Eds.; National Academy Press: Cambridge, MA, USA, 1992. [Google Scholar]
- Pencharz, J.N.; Grigoriadis, E.; Jansz, G.F.; Bombardier, C. A critical appraisal of clinical practice guidelines for the treatment of lower-limb osteoarthritis. Arthritis. Res. 2002, 4, 36–44. [Google Scholar] [CrossRef]
- Shekelle, P.G.; Woolf, S.H.; Eccles, M.; Grimshaw, J. Clinical guidelines: Developing guidelines. BMJ 1999, 318, 593–596. [Google Scholar] [CrossRef]
- Trkulja, V.; Kolundzic, R. Rivaroxaban vs dabigatran for thromboprophylaxis after joint-replacement surgery: Exploratory indirect comparison based on meta-analysis of pivotal clinical trials. Croat. Med. J. 2010, 51, 113–123. [Google Scholar] [CrossRef] [Green Version]
- Loke, Y.K.; Kwok, C.S. Dabigatran and rivaroxaban for prevention of venous thromboembolism—systematic review and adjusted indirect comparison. J. Clin. Pharm. Ther. 2011, 36, 111–124. [Google Scholar] [CrossRef]
- Waddell, J.; Johnson, K.; Hein, W.; Raabe, J.; FitzGerald, G.; Turibio, F. Orthopaedic practice in total hip arthroplasty and total knee arthroplasty: Results from the Global Orthopaedic Registry (GLORY). Am. J. Orthop. 2010, 39, 5–13. [Google Scholar]
- Deitelzweig, S.B.; Lin, J.; Lin, G. Preventing venous thromboembolism following orthopedic surgery in the United States: Impact of special populations on clinical outcomes. Clin. Appl. Thromb. Hemost. 2011, 17, 640–650. [Google Scholar] [CrossRef]
- Jensen, C.D.; Steval, A.; Partington, P.F.; Reed, M.R.; Muller, S.D. Return to theatre following total hip and knee replacement, before and after the introduction of rivaroxaban: A retrospective cohort study. J. Bone Jt. Surg. Br. 2011, 93, 91–95. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomized trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- The Nordic Cochrane Centre. The Cochrane Collaboration. Review Manager (RevMan) [Computer Program]; Version 5.1; The Nordic Cochrane Centre: Copenhagen, Denmark, 2011. [Google Scholar]
- Wells, G.A.; Sultan, S.A.; Chen, L.; Khan, M.; Coyle, D. Indirect Treatment Comparison [Computer Program]; Version 1.0; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2009. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Journal | No of Patients | Enoxaparin | Comparator | Duration of Treatment | Main Findings | |||||||
| Eriksson et al. (2006) [21] | J. Thromb. Haemost. | 706 | 40 mg/day | 2.5, 5, 10, 20, or 30 mg twice daily | 5–9 days | When efficacy and safety were considered together, rivaroxaban at 2.5–10 mg b.i.d., compared favorably with enoxaparin for the prevention of VTE in patients undergoing elective THR. | |||||||
| Eriksson et al. (2006) [22] | Circulation | 873 | 40 mg/day | 5, 10, 20, 30, or 40 mg twice daily | 5–9 days | Rivaroxaban showed efficacy and safety similar to enoxaparin for thromboprophylaxis after THR, with the convenience of once-daily oral dosing and without the need for coagulation monitoring. | |||||||
| Eriksson et al. (2007) [23] | Thromb. Res. | 625 | 40 mg/day | 2.5, 5, 10, 20 and 30 mg twice daily or 30 mg/day | 5–9 days | This study demonstrated proof-of-principle for rivaroxaban for the prevention of VTE after THR. | |||||||
| Eriksson et al. (2007) [24] | Lancet | 3494 | 40 mg/day | 150 or 220 mg/daily | 28–35 days | Oral dabigatran was as effective as enoxaparin in reducing the risk of VTE after THR, with a similar safety profile. | |||||||
| Eriksson et al. (2008) [25] | N. Engl. J. Med. | 4541 | 40 mg/day | 10 mg/day | 31–39 days | A once-daily, 10-mg oral dose of rivaroxaban was significantly more effective for extended thromboprophylaxis than a once-daily, 40-mg subcutaneous dose of enoxaparin in patients undergoing THR. Moreover, the two drugs had similar safety profiles. | |||||||
| Kakkar et al. (2008) [26] | Lancet | 2509 | 40 mg/day | 10 mg/day | Enoxaparin: 10–14 days Rivaroxaban: 31–39 days | Extended thromboprophylaxis with rivaroxaban was significantly more effective than short-term enoxaparin plus placebo for the prevention of VTE, including symptomatic events, in patients undergoing THR. | |||||||
| Lassen et al. (2010) [27] | N. Engl. J. Med. | 5407 | 40 mg/day | 2.5 mg twice daily | 35 days | Among patients undergoing THR, thromboprophylaxis with apixaban, as compared with enoxaparin, was associated with lower rates of VTE, without increased bleeding. | |||||||
| Eriksson et al. (2011) [28] | Thromb. Haemost. | 2055 | 40 mg/day | 220 mg/day | 28–35 days | Extended prophylaxis with oral dabigatran 220 mg once-daily was as effective as subcutaneous enoxaparin 40 mg once-daily in reducing the risk of VTE after THR, and superior to enoxaparin for reducing the risk of major VTE. Moreover, the risk of bleeding and safety profiles were similar. | |||||||
| Eriksson et al. (2015) [29] | Thromb. J. | 4374 | 40 mg/day | 220 mg/day | 28–35 days | Extended prophylaxis with oral dabigatran 220 mg once daily was as effective as enoxaparin 40 mg once daily in reducing the risk of total VTE and all-cause mortality after THR, with a similar bleeding profile. The clinically relevant outcome of major VTE and VTE-related death was significantly reduced with dabigatran versus enoxaparin. | |||||||
| Study | Follow-Up (days) | Duration of Surgery (min) | Females (%) | Mean Age (Years) | Mean Weight (kgs) | BMI (kg/m2) | No of Subjects for Primary Efficacy Analysis | ||||||
| Eriksson et al. (2006) [21] | 30–60 | 85.6 | 59 | 65.3 | 77.5 | 28 | 548 | ||||||
| Eriksson et al. (2006) [22] | 30–60 | 86.8 | 58.6 | 64.9 | 76.4 | 27.2 | 618 | ||||||
| Eriksson et al. (2007) [23] | 30–60 | - | 59 | 65 | 78.5 | 28 | 55 | ||||||
| Eriksson et al. (2007) [24] | 94 | 85 | 56 | 64 | 79 | N/A | 2651 | ||||||
| Eriksson et al. (2008) [25] | 30–35 | 91 | 55.5 | 63.2 | 78.2 | 28 | 1492 | ||||||
| Kakkar et al. (2008) [26] | 30–35 | 94 | 53.6 | 61.5 | 74.7 | 26.9 | 864 | ||||||
| Lassen et al. (2010) [27] | 65–95 | 88 | 52.8 | 60.5 | 79.6 | 28.1 | 2029 | ||||||
| Eriksson et al. (2011) [28] | 90 | 80 | 51.8 | 62 | 79 | 27.8 | 1577 | ||||||
| Eriksson et al. (2015) [29] | 90 | 85 | 54 | 63 | 79 | 27.8 | 243 | ||||||
| Study | Death | Major, Postsurgical Bleeding | Critical/Fatal Bleeding | Clinically Overt Bleeding Associated with Fall in Hb of ≥2 g/dL | Clinically Overt Bleeding Leading to Transfusion of ≥2 Units of Blood | Clinically Overt Bleeding Leading to Re-Operation | |||||||
| Eriksson et al. (2006) [21] | - | 17 | 0 | 8 | 11 | 4 | |||||||
| Eriksson et al. (2006) [22] | 0 | 27 | 0 | 18 | 24 | 2 | |||||||
| Eriksson et al. (2007) [23] | 2 | 21 | - | 17 | 13 | 2 | |||||||
| Eriksson et al. (2007) [24] | 6 | 56 | 2 | 42 | 45 | 8 | |||||||
| Eriksson et al. (2008) [25] | 9 | 8 | 1 | 3 | 3 | 3 | |||||||
| Kakkar et al. (2008) [26] | 10 | 2 | 0 | 1 | 1 | 0 | |||||||
| Lassen et al. (2010) [27] | 7 | 40 | 0 | 23 | 30 | 2 | |||||||
| Eriksson et al. (2011) [28] | 2 | 23 | 0 | 20 | 18 | 0 | |||||||
| Eriksson et al. (2015) [29] | 4 | 64 | 1 | 50 | 55 | 5 | |||||||
| Relative Risk (95% CI) | |||
|---|---|---|---|
| Outcomes | Rivaroxaban vs. Dabigatran | Rivaroxaban vs. Apixaban | Apixaban vs. Dabigatran |
| Symptomatic venous thromboembolism | 0.76 (0.29 to 2.10) | 0.61 (0.29 to 1.22) | 1.20 (0.34 to 4.16) |
| Clinically relevant bleeding | 1.24 (0.95 to 1.53) | 1.49 (1.27 to 1.74) | 0.77 (0.59 to 0.88) |
| Major bleeding | 1.65 (0.87 to 2.53) | 1.63 (0.80 to 2.98) | 0.83 (0.39 to 1.76) |
| Net clinical endpoint | 0.89 (0.69 to 1.56) | 0.98 (0.72 to 1.38) | 0.99 (0.72 to 1.71) |
| Risk Difference (95% CI) | ||||
|---|---|---|---|---|
| Comparison | Symptomatic Venous Thromboembolism | Clinically Relevant Bleeding | Major Bleeding | Net Clinical Endpoint |
| Direct comparisons: | ||||
| Enoxaparin vs. Rivaroxaban | −4 (−8 to −1) | 8 (3 to 18) | 4 (−0.6 to 9) | −4 (−8 to 3) |
| Enoxaparin vs. Dabigatran | −2 (−8 to 4) | 4 (−3 to 12) | −1 (−5 to 4) | −1 (−7 to 8) |
| Enoxaparin vs. Apixaban | −1 (−5 to 2) | −7 (−14 to −1) | −1 (−6 to 4) | −1 (−5 to 2) |
| Indirect comparisons: | ||||
| Rivaroxaban vs. Dabigatran | −3 (−10 to 3) | 4 (−8 to 15) | 4 (−3 to 12) | −2 (−11 to 8) |
| Rivaroxaban vs. Apixaban | −4 (−8 to 2) | 17 (8 to 29) | 4 (−3 to 11) | −2 (−8 to 5) |
| Dabigatran vs. Apixaban | 1 (−8 to 7) | −12 (−23 to −3) | 0 (−7 to 6) | 0 (−8 to 8) |
| Population (P) | Subjects who have undergone total hip replacement surgery |
| Intervention (I) |
|
| Comparator (C) | Efficacy and safety outcomes of enoxaparin will be compared with apixaban, rivaroxaban, and/or dabigatran |
| Outcomes (O) | Primary efficacy outcomes: a combination of DVT, non-fatal pulmonary embolism, and death due to any reason during treatment. Secondary efficacy outcomes: major venous thromboembolism (combination of proximal DVT, non-fatal pulmonary embolism, and VTE-associated death). Safety outcomes: bleeding events including minor events, clinically significant non-fatal bleeding events, or major bleeding events. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfarhan, M.F.A. Efficacy and Safety of Enoxaparin versus New Oral Anticoagulants to Prevent Venous Thromboembolism after Total Hip Replacement: A Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 107. https://doi.org/10.3390/jpm12010107
Alfarhan MFA. Efficacy and Safety of Enoxaparin versus New Oral Anticoagulants to Prevent Venous Thromboembolism after Total Hip Replacement: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(1):107. https://doi.org/10.3390/jpm12010107
Chicago/Turabian StyleAlfarhan, Mohammed Farhan A. 2022. "Efficacy and Safety of Enoxaparin versus New Oral Anticoagulants to Prevent Venous Thromboembolism after Total Hip Replacement: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 1: 107. https://doi.org/10.3390/jpm12010107