
The Effect of Surgeon Expertise on the Outcome of Patients with Adrenocortical Carcinoma

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patient Characteristics
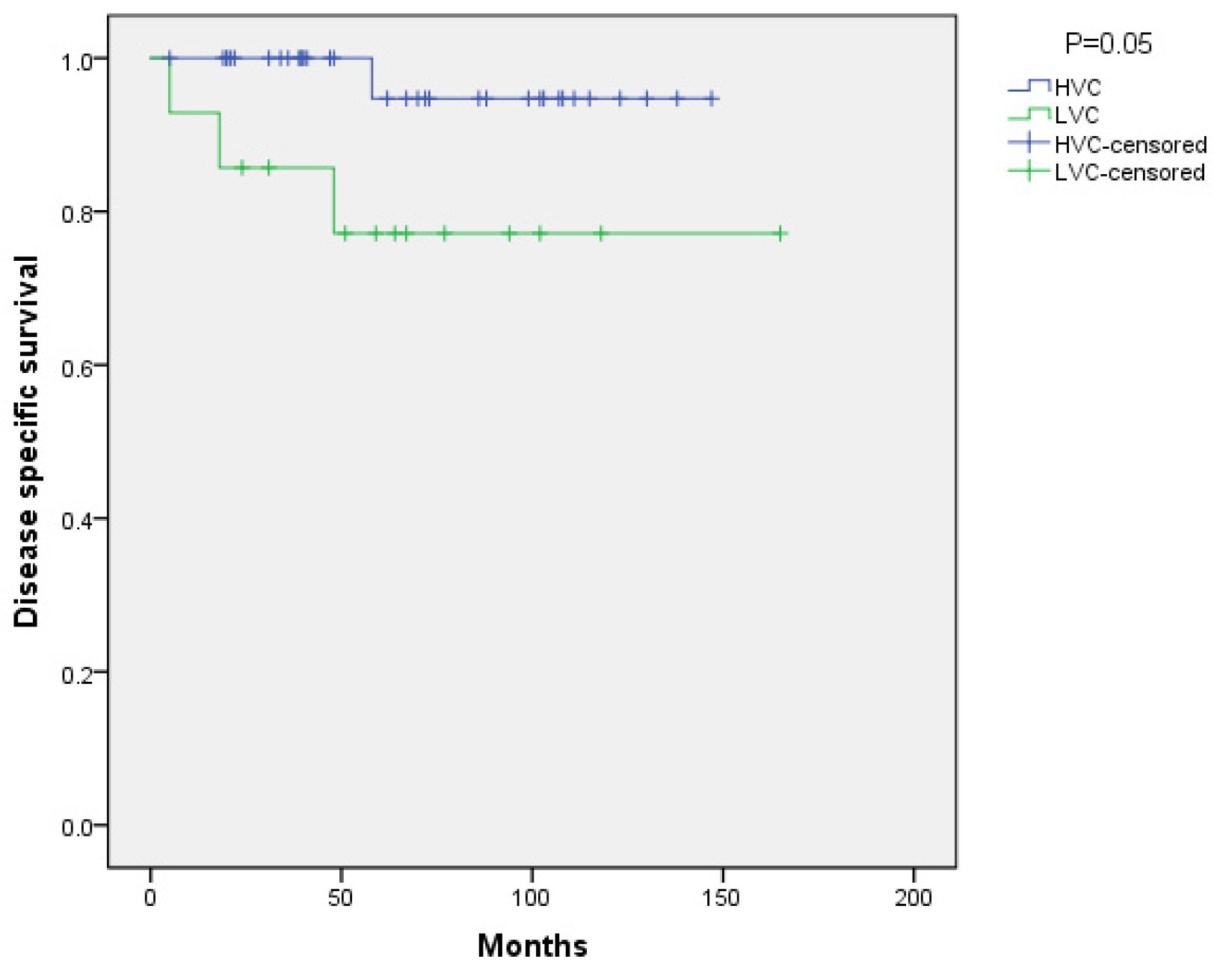
3.2. Long-Term Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kastelan, D.; Muzurovic, E.; Dusek, T. Approach to Patients with European Network for the Study of Adrenal Tumor Stages I and II Adrenocortical Carcinomas. Curr. Opin. Endocrinol. Diabetes Obes. 2021, 28, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Stavrakis, A.I.; Ituarte, P.H.G.; Ko, C.Y.; Yeh, M.W. Surgeon Volume as a Predictor of Outcomes in Inpatient and Outpatient Endocrine Surgery. Surgery 2007, 142, 887–899. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.M.; Moreno, P.; Ortega, J.; Bollo, E.; Ramírez, C.P.; Muñoz, N.; Martínez, C.; Domínguez-Adame, E.; Sancho, J.; Del Pino, J.M.; et al. Results of Adrenal Surgery. Data of a Spanish National Survey. Langenbeck’s Arch. Surg. 2010, 395, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.P.; Raffaelli, M.; Boniardi, M.; De Toma, G.; Marzano, L.A.; Miccoli, P.; Minni, F.; Morino, M.; Pelizzo, M.R.; Pietrabissa, A.; et al. Adrenocortical Carcinoma: Effect of Hospital Volume on Patient Outcome. Langenbeck’s Arch. Surg. 2012, 397, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Palazzo, F.; Dickinson, A.; Phillips, B.; Sahdev, A.; Bliss, R.; Rasheed, A.; Krukowski, Z.; Newell-Price, J. Adrenal Surgery in England: Better Outcomes in High-Volume Practices. Clin. Endocrinol. 2016, 85, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Al-Qurayshi, Z.; Robins, R.; Buell, J.; Kandil, E. Surgeon Volume Impact on Outcomes and Cost of Adrenal Surgeries. Eur. J. Surg. Oncol. 2016, 42, 1483–1490. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Dekkers, O.M.; Else, T.; Baudin, E.; Berruti, A.; De Krijger, R.R.; Haak, H.R.; Mihai, R.; Assie, G.; Terzolo, M. European Society of Endocrinology Clinical Practice Guidelines on the Management of Adrenocortical Carcinoma in Adults, in Collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 2018, 179, G1–G46. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Johanssen, S.; Fenske, W.; Weismann, D.; Agha, A.; Beuschlein, F.; Führer, D.; Jurowich, C.; Quinkler, M.; Petersenn, S.; et al. Improved Survival in Patients with Stage II Adrenocortical Carcinoma Followed up Prospectively by Specialized Centers. J. Clin. Endocrinol. Metab. 2010, 95, 4925–4932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerkhofs, T.M.A.; Verhoeven, R.H.A.; Bonjer, H.J.; Nieveen Van Dijkum, E.J.; Vriens, M.R.; De Vries, J.; Van Eijck, C.H.; Bonsing, B.A.; Van De Poll-Franse, L.V. Surgery for Adrenocortical Carcinoma in the Netherlands: Analysis of the National Cancer Registry Data. Eur. J. Endocrinol. 2013, 169, 83–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez, R.J.; Shapiro, S.; Sarlis, N.; Vassilopoulou-Sellin, R.; Perrier, N.D.; Evans, D.B.; Lee, J.E. Laparoscopic Resection of Adrenal Cortical Carcinoma: A Cautionary Note. Surgery 2005, 138, 1076–1078. [Google Scholar] [CrossRef] [PubMed]
- Bisceglia, M.; Ludovico, O.; Di Mattia, A.; Ben-Dor, D.; Sandbank, J.; Pasquinelli, G.; Lau, S.K.; Weiss, L.M. Adrenocortical Oncocytic Tumors: Report of 10 Cases and Review of the Literature. Int. J. Surg. Pathol. 2004, 12, 231–243. [Google Scholar] [CrossRef]
- Mihai, R.; Donatini, G.; Vidal, O.; Brunaud, L. Volume-Outcome Correlation in Adrenal Surgery-an ESES Consensus Statement. Langenbeck’s Arch. Surg. 2019, 404, 795–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van De Poll-Franse, L.V.; Lemmens, V.E.P.P.; Roukema, J.A.; Coebergh, J.W.W.; Nieuwenhuijzen, G.A.P. Impact of Concentration of Oesophageal and Gastric Cardia Cancer Surgery on Long-Term Population-Based Survival. Br. J. Surg. 2011, 98, 956–963. [Google Scholar] [CrossRef]
- Lemmens, V.E.P.P.; Bosscha, K.; van der Schelling, G.; Brenninkmeijer, S.; Coebergh, J.W.W.; de Hingh, I.H.J.T. Improving Outcome for Patients with Pancreatic Cancer through Centralization. Br. J. Surg. 2011, 98, 1455–1462. [Google Scholar] [CrossRef]
- Park, H.S.; Roman, S.A.; Sosa, J.A. Outcomes from 3144 Adrenalectomies in the United States: Which Matters More, Surgeon Volume or Specialty? Arch. Surg. 2009, 144, 1060–1067. [Google Scholar] [CrossRef] [Green Version]
- Grubbs, E.G.; Callender, G.G.; Xing, Y.; Perrier, N.D.; Evans, D.B.; Phan, A.T.; Lee, J.E. Recurrence of Adrenal Cortical Carcinoma Following Resection: Surgery Alone Can Achieve Results Equal to Surgery plus Mitotane. Ann. Surg. Oncol. 2010, 17, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Solak, M.; Kraljević, I.; Zibar Tomšić, K.; Kaštelan, M.; Kakarigi, L.; Kaštelan, D. Neutrophil-Lymphocyte Ratio as a Prognostic Marker in Adrenocortical Carcinoma. Endocr. Res. 2021, 46, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Kastelan, D.; Knezevic, N.; Zibar Tomsic, K.; Alduk, A.M.; Kakarigi, L.; Kastelan, M.; Coric, M.; Skoric-Polovina, T.; Solak, M.; Kraljevic, I.; et al. Open vs Laparoscopic Adrenalectomy for Localized Adrenocortical Carcinoma. Clin. Endocrinol. 2020, 93, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Kulis, T.; Knezevic, N.; Pekez, M.; Kastelan, D.; Grkovic, M.; Kastelan, Z. Laparoscopic Adrenalectomy: Lessons Learned from 306 Cases. J. Laparoendosc. Adv. Surg. Tech. 2012, 22, 22–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fassnacht, M.; Assie, G.; Baudin, E.; Eisenhofer, G.; de la Fouchardiere, C.; Haak, H.R.; de Krijger, R.; Porpiglia, F.; Terzolo, M.; Berruti, A. Adrenocortical Carcinomas and Malignant Phaeochromocytomas: ESMO-EURACAN Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2020, 31, 1476–1490. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | HVC (n = 35) | LVC (n = 14) | p-Value |
|---|---|---|---|
| Age (year) | 46 (18–77) | 56.5 (24–78) | 0.22 |
| Female gender (n, %) | 24 (68.5) | 10 (71.4) | 0.85 |
| Tumor size (mm) | 80 (26–176) | 107.5 (70–250) | 0.05 |
| ENSAT tumor stage (n, %) | |||
| Stage I | 6 (17.1) | 0(0) | |
| Stage II | 21 (60.0) | 10 (71.4) | |
| Stage III | 8 (22.9) | 4(28.6) | |
| Excess glucocorticoid secretion (n, %) | 13 (37.1) | 4 (28.6) | 0.57 |
| Ki-67 (%) | 12 (1–60) | 14 (4–65) | 0.25 |
| Weiss score | 6 (3–9) | 6.5 (4–8) | 0.79 |
| Adjuvant mitotane (n, %) | 21 (60) | 6 (42.9) | 0.28 |
| Follow-up (months) | 62 (5–147) | 61.5(5–165) | 0.85 |
| Laparoscopic surgery (n, %) | 25 (71.4) | 4(28.6) | 0.006 |
| Recurrence (n, %) | 8 (22.9) | 8(57.1) | 0.02 |
| Laparoscopic surgery (n, %) | 6(24) | 3(75) | 0.157 |
| Open surgery (n, %) | 2(20) | 5(50) | |
| Death (n, %) | 4(11.4) | 4(28.6) | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barac Nekic, A.; Knezevic, N.; Zibar Tomsic, K.; Kraljevic, I.; Balasko, A.; Skoric Polovina, T.; Solak, M.; Dusek, T.; Kastelan, D.; Croatian ACC Study Group. The Effect of Surgeon Expertise on the Outcome of Patients with Adrenocortical Carcinoma. J. Pers. Med. 2022, 12, 100. https://doi.org/10.3390/jpm12010100
Barac Nekic A, Knezevic N, Zibar Tomsic K, Kraljevic I, Balasko A, Skoric Polovina T, Solak M, Dusek T, Kastelan D, Croatian ACC Study Group. The Effect of Surgeon Expertise on the Outcome of Patients with Adrenocortical Carcinoma. Journal of Personalized Medicine. 2022; 12(1):100. https://doi.org/10.3390/jpm12010100
Chicago/Turabian StyleBarac Nekic, Anja, Nikola Knezevic, Karin Zibar Tomsic, Ivana Kraljevic, Annemarie Balasko, Tanja Skoric Polovina, Mirsala Solak, Tina Dusek, Darko Kastelan, and Croatian ACC Study Group. 2022. "The Effect of Surgeon Expertise on the Outcome of Patients with Adrenocortical Carcinoma" Journal of Personalized Medicine 12, no. 1: 100. https://doi.org/10.3390/jpm12010100