
Physical Inactivity: A Modifiable Risk Factor for Morbidity and Mortality in Kidney Transplantation



{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Physical Activity before and after Kidney Transplantation
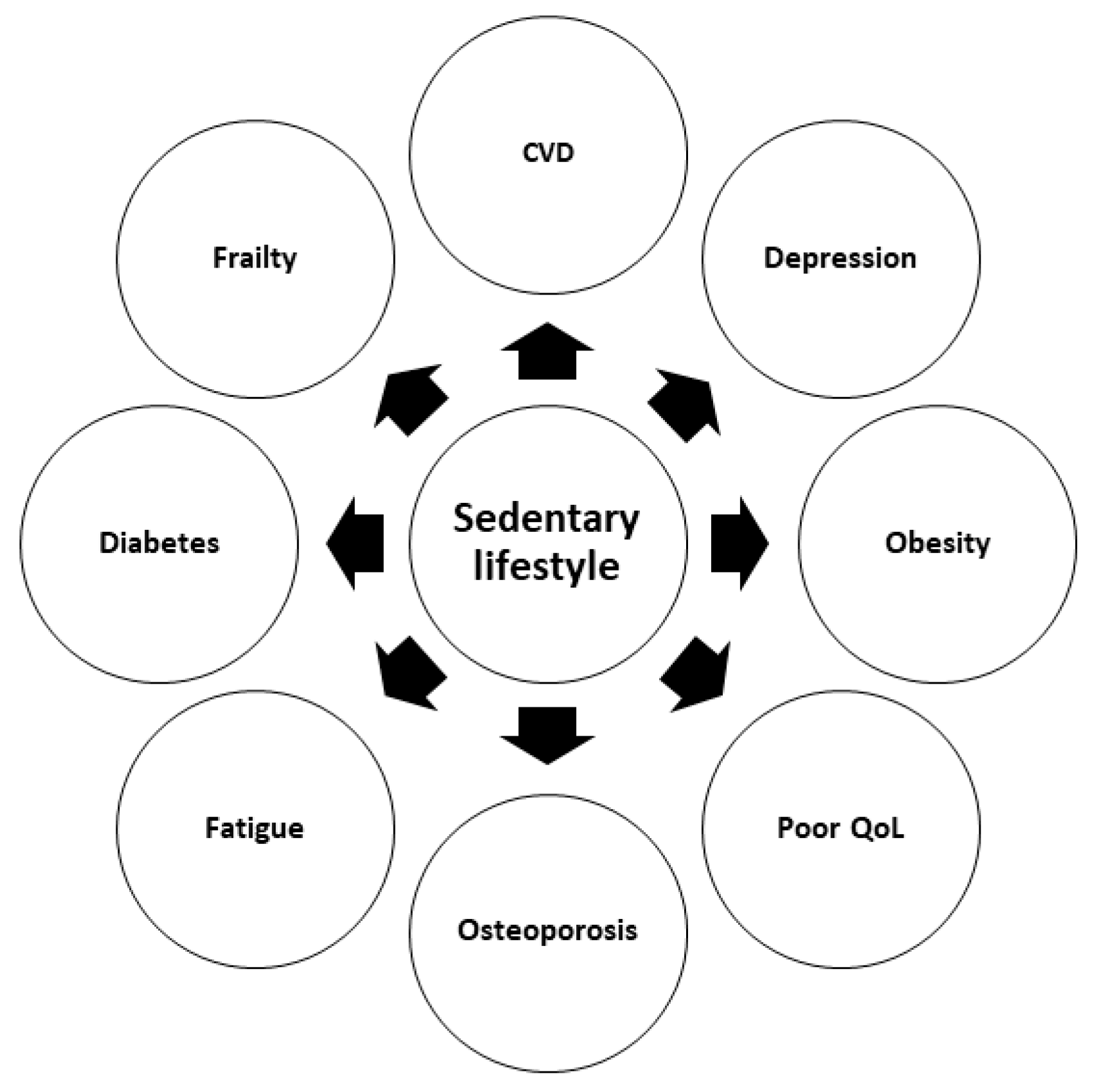
3. Consequences of Physical Inactivity
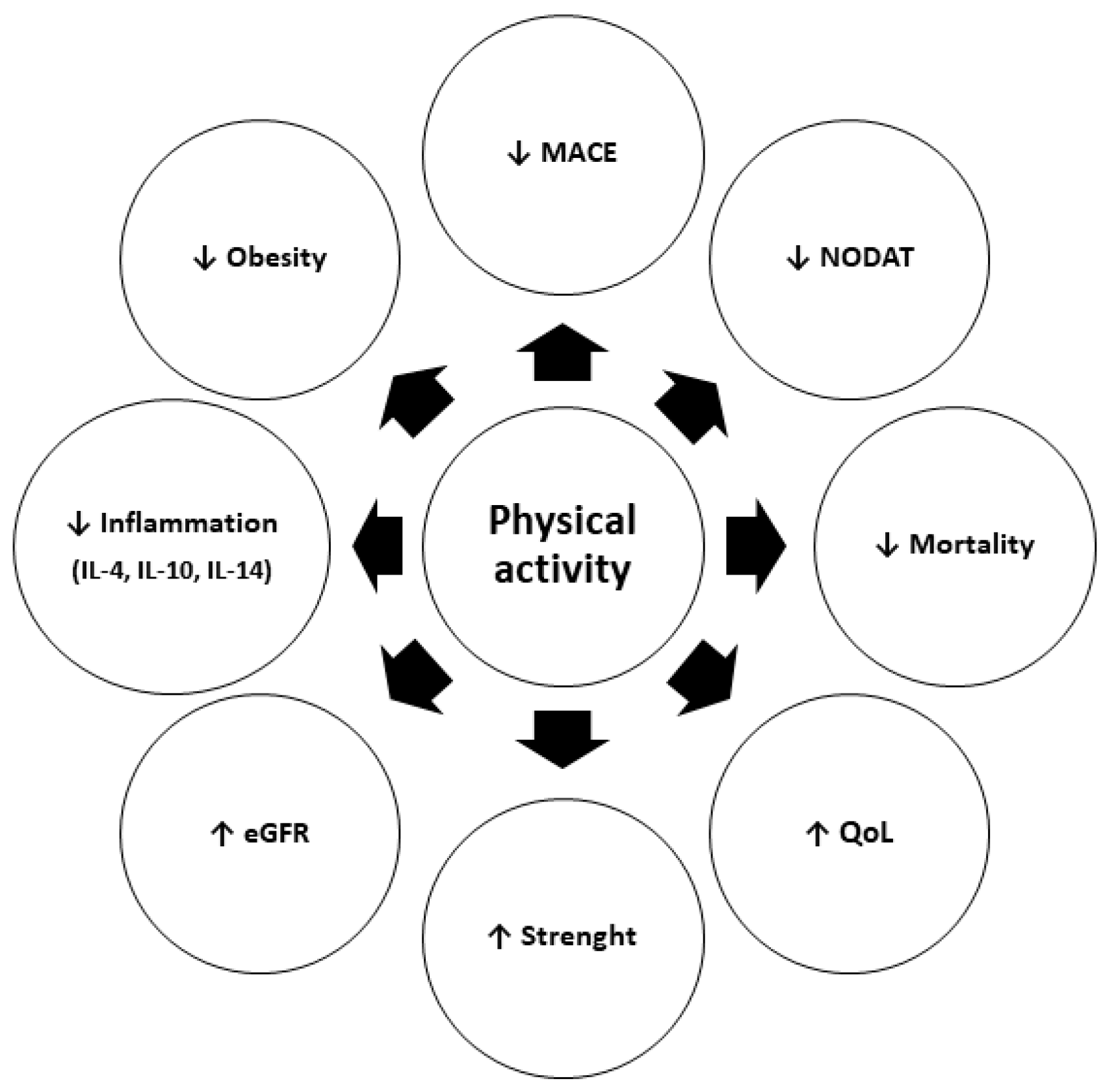
4. The Benefits of Physical Activity
5. Physical Exercise and Sport after Transplantation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kushi, L.H.; Fee, R.M.; Folsom, A.R.; Mink, P.J.; Anderson, K.E.; Sellers, T.A. Physical activity and mortality in postmenopausal women. JAMA 1997, 277, 1287–1292. [Google Scholar] [CrossRef]
- Fried, L.P.; Kronmal, R.A.; Newman, A.B.; Bild, D.E.; Mittelmark, M.B.; Polak, J.F.; Robbins, J.A.; Gardin, J.M. Risk factors for 5-year mortality in older adults: The Cardiovascular Health Study. JAMA 1998, 279, 585–592. [Google Scholar] [CrossRef]
- Andersen, L.B.; Schnohr, P.; Schroll, M.; Hein, H.O. All-cause mortality associated with physical activity during leisure time, work, sports, and cycling to work. Arch. Intern. Med. 2000, 160, 1621–1628. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M.; Lancet Physical Activity Series 2 Executive Committe; Lancet Sedentary Behaviour Working Group. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Kyu, H.H.; Bachman, V.F.; Alexander, L.T.; Mumford, J.E.; Afshin, A.; Estep, K.; Veerman, J.L.; Delwiche, K.; Iannarone, M.L.; Moyer, M.L.; et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: Systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ 2016, 354, i3857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Dwyer, T.; Durcan, L.; Wilson, F. Exercise and physical activity in systemic lupus erythematosus: A systematic review with meta-analyses. Semin. Arthritis Rheum. 2017, 47, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Groessl, E.J.; Kaplan, R.M.; Rejeski, W.J.; Katula, J.A.; Glynn, N.W.; King, A.C.; Anton, S.D.; Walkup, M.; Lu, C.J.; Reid, K.; et al. Physical Activity and Performance Impact Long-term Quality of Life in Older Adults at Risk for Major Mobility Disability. Am. J. Prev. Med. 2019, 56, 141–146. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.F.; George, R.P.; Warshaw, B.; Wang, E.; Greenbaum, L.A. Physical Activity and Kidney Injury in Pediatric and Young Adult Kidney Transplant Recipients. J Pediatr. 2016, 179, 90–95.e2. [Google Scholar] [CrossRef]
- Kutner, N.G.; Zhang, R.; Bowles, T.; Painter, P. Pretransplant physical functioning and kidney patients’ risk for posttransplantation hospitalization/death: Evidence from a national cohort. Clin. J. Am. Soc. Nephrol. 2006, 1, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, E.L.; Kitzman, D.; Rocco, M.; Leng, X.; Klepin, H.; Gordon, M.; Rejeski, J.; Berry, M.; Kritchevsky, S. Physical function in older candidates for renal transplantation: An impaired population. Clin. J. Am. Soc. Nephrol. 2009, 4, 588–594. [Google Scholar] [CrossRef] [Green Version]
- Manfredini, F.; Mallamaci, F.; D’Arrigo, G.; Baggetta, R.; Bolignano, D.; Torino, C.; Lamberti, N.; Bertoli, S.; Ciurlino, D.; Rocca-Rey, L.; et al. Exercise in Patients on Dialysis: A Multicenter, Randomized Clinical Trial. J. Am. Soc. Nephrol. 2017, 28, 1259–1268. [Google Scholar] [CrossRef]
- Mallamaci, F.; Pisano, A.; Tripepi, G. Physical activity in chronic kidney disease and the EXerCise Introduction to Enhance trial. Nephrol. Dial. Transplant. 2020, 35 (Suppl. 2), ii18–ii22. [Google Scholar] [CrossRef] [PubMed]
- Hargrove, N.; El Tobgy, N.; Zhou, O.; Pinder, M.; Plant, B.; Askin, N.; Bieber, L.; Collister, D.; Whitlock, R.; Tangri, N.; et al. Effect of Aerobic Exercise on Dialysis-Related Symptoms in Individuals Undergoing Maintenance Hemodialysis: A Systematic Review and Meta-Analysis of Clinical Trials. Clin. J. Am. Soc. Nephrol. 2021, 16, 560–574. [Google Scholar] [CrossRef] [PubMed]
- Hudson, M.B.; Price, S.R. Calcineurin: A poorly understood regulator of muscle mass. Int. J. Biochem. Cell Biol. 2013, 45, 2173–2178. [Google Scholar] [CrossRef] [Green Version]
- Bodine, S.C.; Stitt, T.N.; Gonzalez, M.; Kline, W.O.; Stover, G.L.; Bauerlein, R.; Zlotchenko, E.; Scrimgeour, A.; Lawrence, J.C.; Glass, D.J.; et al. Akt/mTOR pathway is a crucial regulator of skeletal muscle hypertrophy and can prevent muscle atrophy in vivo. Nat. Cell Biol. 2001, 3, 1014–1019. [Google Scholar] [CrossRef]
- Hasselgren, P.O. Glucocorticoids and muscle catabolism. Curr. Opin. Clin. Nutr. Metab. Care 1999, 2, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Gordon, E.J.; Prohaska, T.R.; Gallant, M.P.; Sehgal, A.R.; Strogatz, D.; Conti, D.; Siminoff, L.A. Prevalence and determinants of physical activity and fluid intake in kidney transplant recipients. Clin. Transplant. 2010, 24, E69–E81. [Google Scholar] [CrossRef] [Green Version]
- Masiero, L.; Puoti, F.; Bellis, L.; Lombardini, L.; Totti, V.; Angelini, M.L.; Spazzoli, A.; Nanni Costa, A.; Cardillo, M.; Sella, G.; et al. Physical activity and renal function in the Italian kidney transplant population. Ren. Fail. 2020, 42, 1192–1204. [Google Scholar] [CrossRef]
- Gordon, E.J.; Prohaska, T.R.; Gallant, M.; Siminoff, L.A. Self-care strategies and barriers among kidney transplant recipients: A qualitative study. Chronic Illn. 2009, 5, 75–91. [Google Scholar] [CrossRef] [Green Version]
- Zelle, D.M.; Klaassen, G.; van Adrichem, E.; Bakker, S.J.; Corpeleijn, E.; Navis, G. Physical inactivity: A risk factor and target for intervention in renal care. Nat. Rev. Nephrol. 2017, 13, 152–168. [Google Scholar] [CrossRef]
- Perez-Dominguez, B.; Casaña-Granell, J.; Garcia-Maset, R.; Garcia-Testal, A.; Melendez-Oliva, E.; Segura-Orti, E. Effects of exercise programs on physical function and activity levels in patients undergoing hemodialysis. A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2021. Epub ahead of print. [Google Scholar] [CrossRef]
- Serper, M.; Barankay, I.; Chadha, S.; Shults, J.; Jones, L.S.; Olthoff, K.M.; Reese, P.P. A randomized, controlled, behavioral intervention to promote walking after abdominal organ transplantation: Results from the LIFT study. Transpl. Int. 2020, 33, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Gomarasca, M.; Banfi, G.; Lombardi, G. Myokines: The endocrine coupling of skeletal muscle and bone. Adv. Clin. Chem. 2020, 94, 155–218. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Burini, R.C.; Anderson, E.; Durstine, J.L.; Carson, J.A. Inflammation, physical activity, and chronic disease: An evolutionary perspective. Sports Med. Health Sci. 2020, 2, 1–6. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Steensberg, A.; Schjerling, P. Muscle-derived interleukin-6: Possible biological effects. J. Physiol. 2001, 536, 329–337. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Steensberg, A.; Fischer, C.; Keller, C.; Keller, P.; Plomgaard, P.; Febbraio, M.; Saltin, B. Searching for the exercise factor: Is IL-6 a candidate? J. Muscle Res. Cell Motil. 2003, 24, 113–119. [Google Scholar] [CrossRef]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Janssen, I.; Ardern, C.I. Physical inactivity, excess adiposity and premature mortality. Obes. Rev. 2003, 4, 257–290. [Google Scholar] [CrossRef]
- Hu, F.B.; Willett, W.C.; Li, T.; Stampfer, M.J.; Colditz, G.A.; Manson, J.E. Adiposity as compared with physical activity in predicting mortality among women. N. Engl. J. Med. 2004, 351, 2694–2703. [Google Scholar] [CrossRef]
- Yango, A.F.; Gohh, R.Y.; Monaco, A.P.; Reinert, S.E.; Gautam, A.; Dworkin, L.D.; Morrissey, P.E. Excess risk of renal allograft loss and early mortality among elderly recipients is associated with poor exercise capacity. Clin. Nephrol. 2006, 65, 401–407. [Google Scholar] [CrossRef]
- Zelle, D.M.; Corpeleijn, E.; Stolk, R.P.; de Greef, M.H.; Gans, R.O.; van der Heide, J.J.; Navis, G.; Bakker, S.J. Low physical activity and risk of cardiovascular and all-cause mortality in renal transplant recipients. Clin. J. Am. Soc. Nephrol. 2011, 6, 898–905. [Google Scholar] [CrossRef] [Green Version]
- Rosas, S.E.; Reese, P.P.; Huan, Y.; Doria, C.; Cochetti, P.T.; Doyle, A. Pretransplant physical activity predicts all-cause mortality in kidney transplant recipients. Am. J. Nephrol. 2012, 35, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, A.W.; Garber, C.E.; Eaton, C.B.; Risica, P.M.; Bostom, A.G. Physical Activity and Cardiovascular Risk among Kidney Transplant Patients. Med. Sci. Sports Exerc. 2019, 51, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Harhay, M.N.; Rao, M.K.; Woodside, K.J.; Johansen, K.L.; Lentine, K.L.; Tullius, S.G.; Parsons, R.F.; Alhamad, T.; Berger, J.; Cheng, X.S.; et al. An overview of frailty in kidney transplantation: Measurement, management and future considerations. Nephrol. Dial. Transplant. 2020, 35, 1099–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAdams-DeMarco, M.A.; Ying, H.; Olorundare, I.; King, E.A.; Haugen, C.; Buta, B.; Gross, A.L.; Kalyani, R.; Desai, N.M.; Dagher, N.N.; et al. Individual Frailty Components and Mortality in Kidney Transplant Recipients. Transplantation 2017, 101, 2126–2132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, V.D.; Tribess, S.; Meneguci, J.; Sasaki, J.E.; Garcia-Meneguci, C.A.; Carneiro, J.A.O.; Virtuoso, J.S., Jr. Association between frailty and the combination of physical activity level and sedentary behavior in older adults. BMC Public Health 2019, 19, 709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bossola, M.; Pepe, G.; Vulpio, C. Fatigue in kidney transplant recipients. Clin. Transplant. 2016, 30, 1387–1393. [Google Scholar] [CrossRef] [PubMed]
- Goedendorp, M.M.; Hoitsma, A.J.; Bloot, L.; Bleijenberg, G.; Knoop, H. Severe fatigue after kidney transplantation: A highly prevalent, disabling and multifactorial symptom. Transpl. Int. 2013, 26, 1007–1015. [Google Scholar] [CrossRef]
- Zelle, D.M.; Dorland, H.F.; Rosmalen, J.G.; Corpeleijn, E.; Gans, R.O.; Homan van der Heide, J.J.; van Son, W.J.; Navis, G.; Bakker, S.J. Impact of depression on long-term outcome after renal transplantation: A prospective cohort study. Transplantation 2012, 94, 1033–1040. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, A.; Hu, S.L.; Bostom, A. Physical Activity in Kidney Transplant Recipients: A Review. Am. J. Kidney Dis. 2018, 72, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, J.H.; Kirkman, D.; Jibani, M. Kidney transplantation: A systematic review of interventional and observational studies of physical activity on intermediate outcomes. Adv. Chronic Kidney Dis. 2009, 16, 482–500. [Google Scholar] [CrossRef] [PubMed]
- Vleut, R.; Abramowicz, D.; Hellemans, R. Frailty: A new comorbidity in kidney transplant candidates? Nephrol. Dial. Transplant. 2020, 35, 1085–1087. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, C.; Podestà, M.A.; Graziani, G. Renal transplantation in elderly patients. How to select the candidates to the waiting list? Transplant. Rev. 2014, 28, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Tennankore, K.K.; Gunaratnam, L.; Suri, R.S.; Yohanna, S.; Walsh, M.; Tangri, N.; Prasad, B.; Gogan, N.; Rockwood, K.; Doucette, S.; et al. Frailty and the Kidney Transplant Wait List: Protocol for a Multicenter Prospective Study. Can. J. Kidney Health Dis. 2020, 7, 2054358120957430. [Google Scholar] [CrossRef] [PubMed]
- Schardong, J.; Marcolino, M.A.Z.; Plentz, R.D.M. Muscle Atrophy in Chronic Kidney Disease. Adv. Exp. Med. Biol. 2018, 1088, 393–412. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Sabia, S.; Batty, G.D.; Shipley, M.J.; Tabák, A.G.; Singh-Manoux, A.; Kivimaki, M. Physical activity and inflammatory markers over 10 years: Follow-up in men and women from the Whitehall II cohort study. Circulation 2012, 126, 928–933. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Cánoves, P.; Scheele, C.; Pedersen, B.K.; Serrano, A.L. Interleukin-6 myokine signaling in skeletal muscle: A double-edged sword? FEBS J. 2013, 280, 4131–4148. [Google Scholar] [CrossRef]
- Hamer, M. The relative influences of fitness and fatness on inflammatory factors. Prev. Med. 2007, 44, 3–11. [Google Scholar] [CrossRef]
- Pedersen, B.K. The anti-inflammatory effect of exercise: Its role in diabetes and cardiovascular disease control. Essays Biochem. 2006, 42, 105–117. [Google Scholar] [CrossRef]
- Kelly, D.P.; Scarpulla, R.C. Transcriptional regulatory circuits controlling mitochondrial biogenesis and function. Genes Dev. 2004, 18, 357–368. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Wu, H.; Tarr, P.T.; Zhang, C.Y.; Wu, Z.; Boss, O.; Michael, L.F.; Puigserver, P.; Isotani, E.; Olson, E.N.; et al. Transcriptional co-activator PGC-1 alpha drives the formation of slow-twitch muscle fibres. Nature 2002, 418, 797–801. [Google Scholar] [CrossRef]
- Schnyder, S.; Handschin, C. Skeletal muscle as an endocrine organ: PGC-1α, myokines and exercise. Bone 2015, 80, 115–125. [Google Scholar] [CrossRef] [Green Version]
- Egan, B.; Carson, B.P.; Garcia-Roves, P.M.; Chibalin, A.V.; Sarsfield, F.M.; Barron, N.; McCaffrey, N.; Moyna, N.M.; Zierath, J.R.; O’Gorman, D.J. Exercise intensity-dependent regulation of peroxisome proliferator-activated receptor coactivator-1 mRNA abundance is associated with differential activation of upstream signalling kinases in human skeletal muscle. J. Physiol. 2010, 588, 1779–1790. [Google Scholar] [CrossRef]
- Ji, L.L.; Kang, C. Role of PGC-1α in sarcopenia: Etiology and potential intervention—A mini-review. Gerontology 2015, 61, 139–148. [Google Scholar] [CrossRef]
- Warburton, D.E.R.; Bredin, S.S.D. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P.; American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Benatti, F.B.; Pedersen, B.K. Exercise as an anti-inflammatory therapy for rheumatic diseases-myokine regulation. Nat. Rev. Rheumatol. 2015, 11, 86–97. [Google Scholar] [CrossRef]
- Schujmann, D.S.; Lunardi, A.C.; Fu, C. Progressive mobility program and technology to increase the level of physical activity and its benefits in respiratory, muscular system, and functionality of ICU patients: Study protocol for a randomized controlled trial. Trials 2018, 19, 274. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P. Interventions for Human Frailty: Physical Activity as a Model. Cold Spring Harb. Perspect. Med. 2016, 6, a025916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiwe, S.; Jacobson, S.H. Exercise training in adults with CKD: A systematic review and meta-analysis. Am. J. Kidney Dis. 2014, 64, 383–393. [Google Scholar] [CrossRef]
- Kang, A.W.; Bostom, A.G.; Kim, H.; Eaton, C.B.; Gohh, R.; Kusek, J.W.; Pfeffer, M.A.; Risica, P.M.; Garber, C.E. Physical activity and risk of cardiovascular events and all-cause mortality among kidney transplant recipients. Nephrol. Dial. Transplant. 2020, 35, 1436–1443. [Google Scholar] [CrossRef] [PubMed]
- Cicognani, E.; Mazzoni, D.; Totti, V.; Roi, G.S.; Mosconi, G.; Nanni Costa, A. Health-related quality of life after solid organ transplantation: The role of sport activity. Psychol. Health Med. 2015, 20, 997–1004. [Google Scholar] [CrossRef]
- Kim, H.L.; Kim, S.H. Pulse Wave Velocity in Atherosclerosis. Front. Cardiovasc. Med. 2019, 6, 41. [Google Scholar] [CrossRef]
- Greenwood, S.A.; Koufaki, P.; Mercer, T.H.; Rush, R.; O’Connor, E.; Tuffnell, R.; Lindup, H.; Haggis, L.; Dew, T.; Abdulnassir, L.; et al. Aerobic or Resistance Training and Pulse Wave Velocity in Kidney Transplant Recipients: A 12-Week Pilot Randomized Controlled Trial (the Exercise in Renal Transplant [ExeRT] Trial). Am. J. Kidney Dis. 2015, 66, 689–698. [Google Scholar] [CrossRef]
- O’Connor, E.M.; Koufaki, P.; Mercer, T.H.; Lindup, H.; Nugent, E.; Goldsmith, D.; Macdougall, I.C.; Greenwood, S.A. Long-term pulse wave velocity outcomes with aerobic and resistance training in kidney transplant recipients—A pilot randomised controlled trial. PLoS ONE 2017, 12, e0171063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenwood, S.A.; Koufaki, P.; Mercer, T.H.; MacLaughlin, H.L.; Rush, R.; Lindup, H.; O’Connor, E.; Jones, C.; Hendry, B.M.; Macdougall, I.C.; et al. Effect of exercise training on estimated GFR, vascular health, and cardiorespiratory fitness in patients with CKD: A pilot randomized controlled trial. Am. J. Kidney Dis. 2015, 65, 425–434. [Google Scholar] [CrossRef]
- Byambasukh, O.; Osté, M.C.J.; Gomes-Neto, A.W.; van den Berg, E.; Navis, G.; Bakker, S.J.L.; Corpeleijn, E. Physical Activity and the Development of Post-Transplant Diabetes Mellitus, and Cardiovascular- and All-Cause Mortality in Renal Transplant Recipients. J. Clin. Med. 2020, 9, 415. [Google Scholar] [CrossRef] [Green Version]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Königsrainer, I.; Zieker, D.; Löffler, M.; Bühler, S.; Walter, M.; Beckert, S.; Glatzle, J.; Northoff, H.; Nadalin, S.; Königsrainer, A. Influence of exhaustive exercise on the immune system in solid organ transplant recipients. Exerc. Immunol. Rev. 2010, 16, 184–193. [Google Scholar] [PubMed]
- Didsbury, M.; McGee, R.G.; Tong, A.; Craig, J.C.; Chapman, J.R.; Chadban, S.; Wong, G. Exercise training in solid organ transplant recipients: A systematic review and meta-analysis. Transplantation 2013, 95, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.S.; Myers, J.; Han, J.; Stedman, M.R.; Watford, D.J.; Lee, J.; Discipulo, K.V.; Chan, K.N.; Chertow, G.M.; Tan, J.C. Physical Performance Testing in Kidney Transplant Candidates at the Top of the Waitlist. Am. J. Kidney Dis. 2020, 76, 815–825. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; Ying, H.; Van Pilsum Rasmussen, S.; Schrack, J.; Haugen, C.E.; Chu, N.M.; González Fernández, M.; Desai, N.; Walston, J.D.; Segev, D.L. Prehabilitation prior to kidney transplantation: Results from a pilot study. Clin. Transplant. 2019, 33, e13450. [Google Scholar] [CrossRef]
- Totti, V.; Zancanaro, M.; Trerotola, M.; Nanni Costa, A.; Antonetti, T.; Anedda, A.; Roi, G.S. Quality of life and energy expenditure in transplant recipient football players. Transplant. Proc. 2013, 45, 2758–2760. [Google Scholar] [CrossRef] [PubMed]
- Calella, P.; Hernández-Sánchez, S.; Garofalo, C.; Ruiz, J.R.; Carrero, J.J.; Bellizzi, V. Exercise training in kidney transplant recipients: A systematic review. J. Nephrol. 2019, 32, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Griffin, P. Exercise and sport after organ transplantation. Br. J. Sports Med. 1998, 32, 194. [Google Scholar] [CrossRef] [Green Version]
- Nytrøen, K.; Gullestad, L. Exercise after heart transplantation: An overview. World J. Transplant. 2013, 3, 78–90. [Google Scholar] [CrossRef]
- Wisløff, U.; Støylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [Green Version]
- Arena, R.; Myers, J.; Forman, D.E.; Lavie, C.J.; Guazzi, M. Should high-intensity-aerobic interval training become the clinical standard in heart failure? Heart Fail. Rev. 2013, 18, 95–105. [Google Scholar] [CrossRef]
- Nytrøen, K.; Rolid, K.; Andreassen, A.K.; Yardley, M.; Gude, E.; Dahle, D.O.; Bjørkelund, E.; Relbo Authen, A.; Grov, I.; Philip Wigh, J.; et al. Effect of High-Intensity Interval Training in De Novo Heart Transplant Recipients in Scandinavia. Circulation 2019, 139, 2198–2211. [Google Scholar] [CrossRef]
- Hart, A.; Weir, M.R.; Kasiske, B.L. Cardiovascular risk assessment in kidney transplantation. Kidney Int. 2015, 87, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awan, A.A.; Niu, J.; Pan, J.S.; Erickson, K.F.; Mandayam, S.; Winkelmayer, W.C.; Navaneethan, S.D.; Ramanathan, V. Trends in the Causes of Death among Kidney Transplant Recipients in the United States (1996–2014). Am. J. Nephrol. 2018, 48, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Stoumpos, S.; Jardine, A.G.; Mark, P.B. Cardiovascular morbidity and mortality after kidney transplantation. Transpl. Int. 2015, 28, 10–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Smet, S.; Van Craenenbroeck, A.H. Exercise training in patients after kidney transplantation. Clin. Kidney J. 2021, 14 (Suppl. 2), ii15–ii24. [Google Scholar] [CrossRef]
- World Kidney Day. Available online: https://www.worldkidneyday.org (accessed on 28 May 2021).


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ponticelli, C.; Favi, E. Physical Inactivity: A Modifiable Risk Factor for Morbidity and Mortality in Kidney Transplantation. J. Pers. Med. 2021, 11, 927. https://doi.org/10.3390/jpm11090927
Ponticelli C, Favi E. Physical Inactivity: A Modifiable Risk Factor for Morbidity and Mortality in Kidney Transplantation. Journal of Personalized Medicine. 2021; 11(9):927. https://doi.org/10.3390/jpm11090927
Chicago/Turabian StylePonticelli, Claudio, and Evaldo Favi. 2021. "Physical Inactivity: A Modifiable Risk Factor for Morbidity and Mortality in Kidney Transplantation" Journal of Personalized Medicine 11, no. 9: 927. https://doi.org/10.3390/jpm11090927