
Prediction of Sarcopenia Using Multiple Biomarkers of Neuromuscular Junction Degeneration in Chronic Obstructive Pulmonary Disease


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. HGS and Body Composition
2.3. Spirometry
2.4. Measurement of Physical Performance
2.5. Measurement of Plasma Biomarkers
2.6. Measurements of Plasma 8-Isoprostanes, CRP, and Creatine Kinase
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
3.2. Changes in Circulating Biomarkers Levels in COPD
3.3. Evaluation of Sarcopenia Using a Cumulative Risk Score of Three Biomarkers
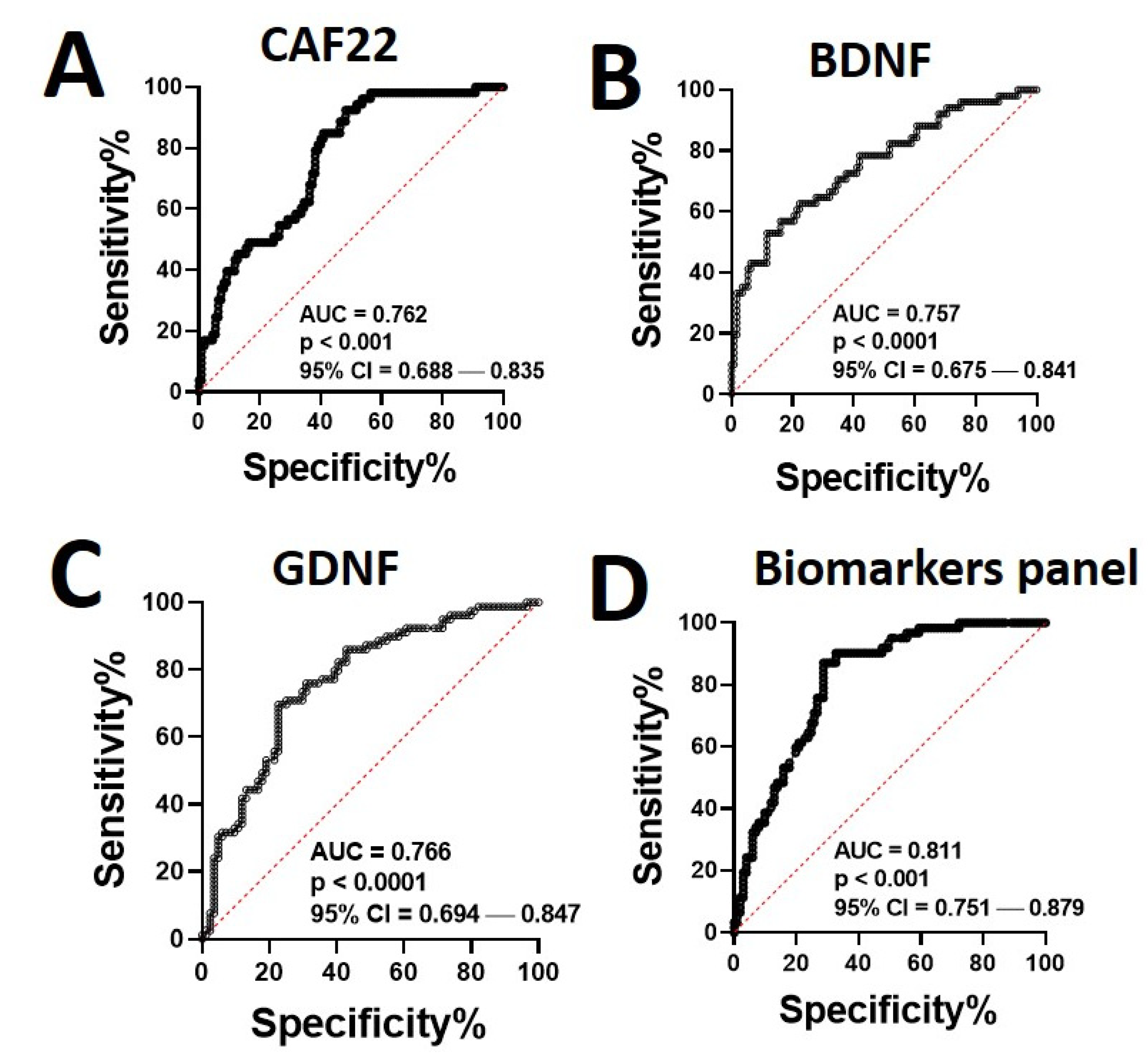
3.4. Significance of the Biomarker Panel in Diagnosis of Sarcopenia
3.5. Association of Biomarker Levels with the Indexes of Sarcopenia
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qaisar, R.; Karim, A.; Muhammad, T. Circulating Biomarkers of Handgrip Strength and Lung Function in Chronic Obstructive Pulmonary Disease. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 311–321. [Google Scholar] [CrossRef] [Green Version]
- Rausch-Osthoff, A.K.; Kohler, M.; Sievi, N.A.; Clarenbach, C.F.; van Gestel, A.J. Association between peripheral muscle strength, exercise performance, and physical activity in daily life in patients with Chronic Obstructive Pulmonary Disease. Multidiscip. Respir. Med. 2014, 9, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaitovich, A.; Barreiro, E. Skeletal Muscle Dysfunction in Chronic Obstructive Pulmonary Disease. What We Know and Can Do for Our Patients. Am. J. Respir. Crit. Care Med. 2018, 198, 175–186. [Google Scholar] [CrossRef]
- Cristea, A.; Qaisar, R.; Edlund, P.K.; Lindblad, J.; Bengtsson, E.; Larsson, L. Effects of aging and gender on the spatial organization of nuclei in single human skeletal muscle cells. Aging Cell 2010, 9, 685–697. [Google Scholar] [CrossRef] [PubMed]
- Qaisar, R.; Karim, A.; Muhammad, T.; Shah, I. Circulating Biomarkers of Accelerated Sarcopenia in Respiratory Diseases. Biology 2020, 9, 322. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [Green Version]
- Lee, L.W.; Lin, C.M.; Li, H.C.; Hsiao, P.L.; Chung, A.C.; Hsieh, C.J.; Wu, P.C.; Hsu, S.F. Body composition changes in male patients with chronic obstructive pulmonary disease: Aging or disease process? PLoS ONE 2017, 12, e0180928. [Google Scholar]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachex- Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Rygiel, K.A.; Picard, M.; Turnbull, D. The ageing neuromuscular system and sarcopenia: A mitochondrial perspective. J. Physiol. 2016, 594, 4499–4512. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, S.; Pollock, N.; MacPherson, P.C.; Ahn, B.; Piekarz, K.M.; Staunton, C.A.; Brown, J.L.; Qaisar, R.; Vasilaki, A.; Richardson, A.; et al. Neuron-specific deletion of CuZnSOD leads to an advanced sarcopenic phenotype in older mice. Aging Cell 2020, 19. [Google Scholar] [CrossRef] [PubMed]
- Kapchinsky, S.; Vuda, M.; Miguez, K.; Elkrief, D.; De Souza, A.R.; Baglole, C.J.; Aare, S.; Macmillan, N.J.; Baril, J.; Rozakis, P.; et al. Smoke-induced neuromuscular junction degeneration precedes the fibre type shift and atrophy in chronic obstructive pulmonary disease. J. Physiol. 2018, 596, 2865–2881. [Google Scholar] [CrossRef]
- Willis-Owen, S.A.G.; Thompson, A.; Kemp, P.R.; Polkey, M.I.; Cookson, W.O.C.M.; Moffatt, M.F.; Natanek, S.A. COPD is accompanied by co-ordinated transcriptional perturbation in the quadriceps affecting the mitochondria and extracellular matrix. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef]
- Qaisar, R.; Karim, A.; Muhammad, T. Plasma CAF22 Levels as a Useful Predictor of Muscle Health in Patients with Chronic Obstructive Pulmonary Disease. Biology 2020, 9, 166. [Google Scholar] [CrossRef] [PubMed]
- Pratt, J.; De Vito, G.; Narici, M.; Boreham, C. Neuromuscular Junction Aging: A Role for Biomarkers and Exercise. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2020, 76, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Calvani, R.; Lorenzi, M.; Martone, A.M.; Tosato, M.; Drey, M.; D’Angelo, E.; Capoluongo, E.; Russo, A.; Bernabei, R.; et al. Serum levels of C-terminal agrin fragment (CAF) are associated with sarcopenia in older multimorbid community-dwellers: Results from the ilSIRENTE study. Exp. Gerontol. 2016, 79, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Mirza, S.; Clay, R.D.; Koslow, M.; Scanlon, P.D. COPD Guidelines: A Review of the 2018 GOLD Report. Mayo Clin. Proc. 2018, 93, 1488–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corhay, J.L.; Nguyen, D.; Van Cauwenberge, H.; Louis, R. Pulmonary rehabilitation and COPD: Providing patients a good environment for optimizing therapy. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 27–39. [Google Scholar] [CrossRef] [Green Version]
- Sobestiansky, S.; Michaelsson, K.; Cederholm, T. Sarcopenia prevalence and associations with mortality and hospitalisation by various sarcopenia definitions in 85–89 year old community-dwelling men: A report from the ULSAM study. BMC Geriatr. 2019, 19, 1–13. [Google Scholar] [CrossRef]
- National Collaborating Centre for Chronic Conditions. Chronic Obstructive Pulmonary Disease. National clinical guideline on management of chronic obstructive pulmonary disease in adults in primary and secondary care. Thorax 2004, 59 (Suppl. S1), 1–232. [Google Scholar]
- Malmstrom, T.K.; Morley, J.E. SARC-F: A Simple Questionnaire to Rapidly Diagnose Sarcopenia. J. Am. Med Dir. Assoc. 2013, 14, 531–532. [Google Scholar] [CrossRef]
- World Medical, A. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Culver, B.H.; Graham, B.L.; Coates, A.L.; Wanger, J.; Berry, C.E.; Clarke, P.K.; Hallstrand, T.S.; Hankinson, J.L.; Kaminsky, D.A.; MacIntyre, N.R.; et al. Recommendations for a Standardized Pulmonary Function Report. An Official American Thoracic Society Technical Statement. Am. J. Respir. Crit. Care Med. 2017, 196, 1463–1472. [Google Scholar] [CrossRef] [PubMed]
- Zaigham, S.; Johnson, L.; Wollmer, P.; Engström, G. Measures of low lung function and the prediction of incident COPD events and acute coronary events. Respir. Med. 2018, 144, 68–73. [Google Scholar] [CrossRef]
- Safka, K.A.; Wald, J.; Wang, H.; McIvor, L.; McIvor, A. GOLD Stage and Treatment in COPD: A 500 Patient Point Prevalence Study. Chronic Obstr. Pulm. Dis. J. COPD Found. 2016, 4, 45–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landi, F.; Russo, A.; Cesari, M.; Pahor, M.; Bernabei, R.; Onder, G. HDL-cholesterol and physical performance: Results from the ageing and longevity study in the sirente geographic area (ilSIRENTE Study). Age Ageing 2007, 36, 514–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sataranatarajan, K.; Qaisar, R.; Davis, C.; Sakellariou, G.K.; Vasilaki, A.; Zhang, Y.; Liu, Y.; Bhaskaran, S.; McArdle, A.; Jackson, M.; et al. Neuron specific reduction in CuZnSOD is not sufficient to initiate a full sarcopenia phenotype. Redox Biol. 2015, 5, 140–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudolf, R.; Deschenes, M.R.; Sandri, M. Neuromuscular junction degeneration in muscle wasting. Curr. Opin. Clin. Nutr. Metab. Care 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drey, M.; Sieber, C.C.; Bauer, J.; Uter, W.; Dahinden, P.; Fariello, R.; Vrijbloed, J. C-terminal Agrin Fragment as a potential marker for sarcopenia caused by degeneration of the neuromuscular junction. Exp. Gerontol. 2013, 48, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Yang, L.; Li, G.; Jin, Y.; Wu, D.; Wang, Q.M.; Huang, P. Agrin Involvement in Synaptogenesis Induced by Exercise in a Rat Model of Experimental Stroke. Neurorehabilit. Neural Repair 2020, 34, 1124–1137. [Google Scholar] [CrossRef]
- Bütikofer, L.; Zurlinden, A.; Bolliger, M.F.; Kunz, B.; Sonderegger, P. Destabilization of the neuromuscular junction by proteolytic cleavage of agrin results in precocious sarcopenia. FASEB J. 2011, 25, 4378–4393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyd, J.G.; Gordon, T. Glial cell line-derived neurotrophic factor and brain-derived neurotrophic factor sustain the axonal regeneration of chronically axotomized motoneurons in vivo. Exp. Neurol. 2003, 183, 610–619. [Google Scholar] [CrossRef]
- Håkansson, K.; Ledreux, A.; Daffner, K.; Terjestam, Y.; Bergman, P.; Carlsson, R.; Kivipelto, M.; Winblad, B.; Granholm, A.-C.; Mohammed, A.K.H. BDNF Responses in Healthy Older Persons to 35 Minutes of Physical Exercise, Cognitive Training, and Mindfulness: Associations with Working Memory Function. J. Alzheimer’s Dis. 2017, 55, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Harris-Love, M.O.; Benson, K.; Leasure, E.; Adams, B.; McIntosh, V. The Influence of Upper and Lower Extremity Strength on Performance-Based Sarcopenia Assessment Tests. J. Funct. Morphol. Kinesiol. 2018, 3, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy | COPD—At Dx | COPD—Follow-Up | |
|---|---|---|---|
| Age at baseline (years) | 67.9 ± 5.5 | 69.3 ± 6.2 | 70.3 ± 6.3 |
| Body composition | |||
| BMI (kg/m2) | 25.7 ± 3.5 | 25.1 ± 3.9 | 24.9 ± 3.4 |
| ASM (kg) | 22.7 ± 3.3 | 21 ± 2.2 * | 21.6 ± 2.6 |
| ASMI (kg/m2) | 8.3 ± 1.2 | 7.1 ± 1.6 * | 7.5 ± 1.5 * |
| Percent fat | 38.5 ± 4.1 | 39.2 ± 4.7 | 36.2 ± 4.9 |
| Phase angle | 5.7 ± 0.6 | 5.31 ± 0.36 * | 5.53 ± 0.44 # |
| Physical Parameters | |||
| HGS (kg) | 27.3 ± 5.9 | 21.4 ± 4.8 * | 23.7 ± 4.5 *,# |
| walking Speed (m/s) | 1.28 ± 0.28 | 1.02 ± 0.21 * | 1.16 ± 0.29 *,# |
| Daily steps count | 5375 ± 1137 | 3136 ± 782 * | 6294 ± 893 *,# |
| Plasma biomarkers | |||
| 8-isoprostanes (pg/mL) | 48.3 ± 11.23 | 85.4 ± 19.49 * | 62.38 ± 15.38 # |
| CRP (mg/dL) | 0.217 ± 0.027 | 0.298 ± 0.047 * | 0.262 ± 0.039 *,# |
| Creatine kinase (IU/L) | 176.32 ± 35.31 | 294.3 ± 41.71 * | 227.5 ± 49.29 *,# |
| AUC | 95% C–I | p Value | ||
|---|---|---|---|---|
| Biomarkers panel | Healthy controls | 0.805 | 0.717–0.839 | 0.003 |
| COPD—At Dx. | 0.819 | 0.728–0.874 | <0.001 | |
| COPD—Follow-up | 0.784 | 0.694–0.859 | 0.001 | |
| CAF22 | Healthy controls | 0.739 | 0.626–0.791 | 0.026 |
| COPD—At Dx. | 0.778 | 0.693–0.803 | <0.001 | |
| COPD—Follow-up | 0.788 | 0.715–0.831 | <0.001 | |
| BDNF | Healthy controls | 0.731 | 0.637–0.783 | 0.001 |
| COPD—At Dx. | 0.769 | 0.663–0.839 | <0.001 | |
| COPD—Follow-up | 0.746 | 0.724–0.862 | <0.001 | |
| GDNF | Healthy controls | 0.783 | 0.654–0.801 | <0.001 |
| COPD—At Dx. | 0.762 | 0.651–0.794 | <0.001 | |
| COPD—Follow-up | 0.803 | 0.704–0.852 | <0.001 | |
| Coefficient | p | |
|---|---|---|
| Changes in the Biomarker Panel (Log Values) vs. Change in | ||
| HGS | 0.272 | 0.011 |
| ASM | 0.103 | 0.099 |
| Phase angle | 0.153 | 0.066 |
| Walking speed | 0.182 | 0.144 |
| Changes in CAF22 vs. change in | ||
| HGS | –0.316 | 0.007 |
| ASM | –0.147 | 0.071 |
| Phase angle | –0.102 | 0.084 |
| Walking speed | –0.081 | 0.184 |
| Changes in BDNF vs. change in | ||
| HGS | 0.182 | 0.057 |
| ASM | 0.041 | 0.081 |
| Phase angle | 0.148 | 0.092 |
| Walking speed | 0.052 | 0.121 |
| Changes in GDNF vs. change in | ||
| HGS | 0.252 | 0.021 |
| ASM | 0.095 | 0.144 |
| Phase angle | 0.053 | 0.187 |
| Walking speed | 0.092 | 0.126 |
| CAF22 | BDNF | GDNF | Biomarkers Panel | |
|---|---|---|---|---|
| HGS | ||||
| Healthy controls | 0.298 * | 0.169 * | 0.141 | 0.194 * |
| COPD—At Dx. | 0.315 * | 0.248 * | 0.108 | 0.205 * |
| COPD—Follow-up | 0.341 * | 0.271 * | 0.129 | 0.228 * |
| ASMI | ||||
| Healthy controls | 0.104 | 0.118 | 0.94 | 0.121 * |
| COPD—At Dx. | 0.094 | 0.131 * | 0.146 * | 0.139 * |
| COPD—Follow-up | 0.116 | 0.084 | 0.223 * | 0.148 * |
| Phase angle | ||||
| Healthy controls | 0.103 | 0.075 | 0.102 | 0.095 * |
| COPD—At Dx. | 0.128 * | 0.081 | 0.083 | 0.089 |
| COPD—Follow-up | 0.081 | 0.059 | 0.120 * | 0.078 |
| Walking speed | ||||
| Healthy controls | 0.068 | 0.99 | 0.147 | 0.104 * |
| COPD—At Dx. | 0.091 | 0.113 | 0.163 * | 0.134 * |
| COPD—Follow-up | 0.103 | 0.106 | 0.193 * | 0.146 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karim, A.; Muhammad, T.; Qaisar, R. Prediction of Sarcopenia Using Multiple Biomarkers of Neuromuscular Junction Degeneration in Chronic Obstructive Pulmonary Disease. J. Pers. Med. 2021, 11, 919. https://doi.org/10.3390/jpm11090919
Karim A, Muhammad T, Qaisar R. Prediction of Sarcopenia Using Multiple Biomarkers of Neuromuscular Junction Degeneration in Chronic Obstructive Pulmonary Disease. Journal of Personalized Medicine. 2021; 11(9):919. https://doi.org/10.3390/jpm11090919
Chicago/Turabian StyleKarim, Asima, Tahir Muhammad, and Rizwan Qaisar. 2021. "Prediction of Sarcopenia Using Multiple Biomarkers of Neuromuscular Junction Degeneration in Chronic Obstructive Pulmonary Disease" Journal of Personalized Medicine 11, no. 9: 919. https://doi.org/10.3390/jpm11090919