
Should Age-Dependent Absolute Risk Thresholds Be Used for Risk Stratification in Risk-Stratified Breast Cancer Screening?

 , , , , ,
, , , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Calculating Age-Dependent Absolute Risk Thresholds
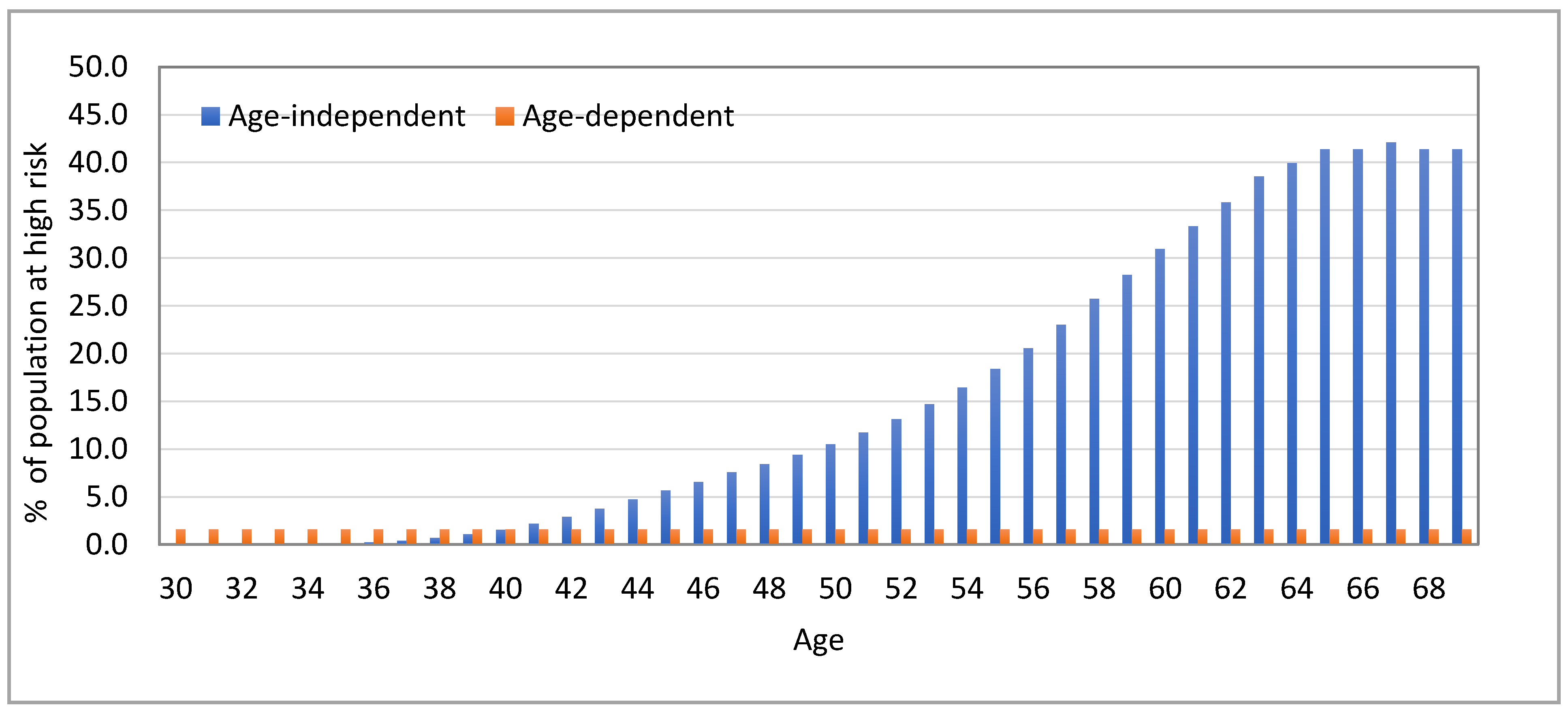
2.2. Estimating the Proportion at High Risk
3. Results
3.1. Age-Dependent Absolute Risk Thresholds
3.2. Implications on Risk Stratification
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- van den Broek, J.J.; Schechter, C.B.; van Ravesteyn, N.T.; Janssens, A.; Wolfson, M.C.; Trentham-Dietz, A.; Simard, J.; Easton, D.F.; Mandelblatt, J.S.; Kraft, P.; et al. Personalizing Breast Cancer Screening Based on Polygenic Risk and Family History. J. Natl. Cancer Inst. 2021, 113, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Pashayan, N.; Morris, S.; Gilbert, F.J.; Pharoah, P.D.P. Cost-effectiveness and Benefit-to-Harm Ratio of Risk-Stratified Screening for Breast Cancer: A Life-Table Model. JAMA Oncol. 2018, 4, 1504–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callender, T.; Emberton, M.; Morris, S.; Eeles, R.; Kote-Jarai, Z.; Pharoah, P.D.P.; Pashayan, N. Polygenic risk-tailored screening for prostate cancer: A benefit-harm and cost-effectiveness modelling study. PLoS Med. 2019, 16, e1002998. [Google Scholar] [CrossRef] [PubMed]
- Pashayan, N.; Antoniou, A.C.; Ivanus, U.; Esserman, L.J.; Easton, D.F.; French, D.; Sroczynski, G.; Hall, P.; Cuzick, J.; Evans, D.G.; et al. Personalized early detection and prevention of breast cancer: ENVISION consensus statement. Nat. Rev. Clin. Oncol. 2020, 17, 687–705. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, J.; Levesque, E.; The Clinical Advisory Committee on Breast Cancer Screening and Prevention; Borduas, F.; Chiquette, J.; Diorio, C.; Duchesne, N.; Dumais, M.; Eloy, L.; Foulkes, W.; et al. Recommendations on breast cancer screening and prevention in the context of implementing risk stratification: Impending changes to current policies. Curr. Oncol. 2016, 23, e615–e625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyrer, J.; Duffy, S.W.; Cuzick, J. A breast cancer prediction model incorporating familial and personal risk factors. Stat. Med. 2004, 23, 1111–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.; Mavaddat, N.; Wilcox, A.N.; Cunningham, A.P.; Carver, T.; Hartley, S.; de Babb Villiers, C.; Izquierdo, A.; Simard, J.; Schmidt, M.K.; et al. BOADICEA: A comprehensive breast cancer risk prediction model incorporating genetic and nongenetic risk factors. Genet. Med. 2019, 21, 1708–1718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tice, J.A.; Cummings, S.R.; Smith-Bindman, R.; Ichikawa, L.; Barlow, W.E.; Kerlikowske, K. Using clinical factors and mammographic breast density to estimate breast cancer risk: Development and validation of a new predictive model. Ann. Intern. Med. 2008, 148, 337–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Cancer Institute. Breast Cancer Risk Assessment Tool. Available online: https://bcrisktool.cancer.gov/ (accessed on 14 April 2021).
- National Comprehensive Cancer Network. September 2020. NCCN Clinical Practice Guidelines in Oncology: Breast Cancer Screening and Diagnosis. Version 1. 2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast-screening.pdf (accessed on 14 April 2021).
- American Cancer Society. Breast Cancer Early Detection and Diagnosis. Available online: https://www.cancer.org/content/dam/CRC/PDF/Public/8579.00.pdf (accessed on 14 April 2021).
- Canadian Partnership Against Cancer. January 2021. Breast Cancer Screening in Canada: Environmental Scan. Available online: https://s22457.pcdn.co/wp-content/uploads/2021/01/breast-cancer-screening-environmental-scan-2019-2020-Jan132021-EN.pdf (accessed on 14 April 2021).
- US National Library of Medicine. My Personalized Breast Screening (MyPeBS). Available online: https://clinicaltrials.gov/ct2/show/NCT03672331 (accessed on 14 April 2021).
- Esserman, L.J. The WISDOM Study: Breaking the deadlock in the breast cancer screening debate. NPJ Breast Cancer 2017, 3, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer Care Ontario. Breast Cancer Screening for Women at High Risk. Available online: https://www.cancercareontario.ca/en/guidelines-advice/cancer-continuum/screening/breast-cancer-high-risk-women (accessed on 14 April 2021).
- National Cancer Institute and Information Management Services. DevCan: Probability of Developing or Dying of Cancer Software [6.7.6]; 2019. Available online: https://surveillance.cancer.gov/devcan/ (accessed on 14 April 2021).
- Statistics Canada. Available online: https://www150.statcan.gc.ca/ (accessed on 14 April 2021).
- Pal Choudhury, P.; Brook, M.N.; Hurson, A.N.; Lee, A.; Mulder, C.V.; Coulson, P.; Schoemaker, M.J.; Jones, M.E.; Swerdlow, A.J.; Chatterjee, N.; et al. Comparative validation of the BOADICEA and Tyrer-Cuzick breast cancer risk models incorporating classical risk factors and polygenic risk in a population-based prospective cohort of women of European ancestry. Breast Cancer Res. 2021, 23, 22. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, A.; Song, M.; Brook, M.N.; Milne, R.L.; Mavaddat, N.; Michailidou, K.; Bolla, M.K.; Wang, Q.; Dennis, J.; Wilcox, A.N.; et al. Joint associations of a polygenic risk score and environmental risk factors for breast cancer in the Breast Cancer Association Consortium. Int. J. Epidemiol. 2018, 47, 526–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatterjee, N.; Wheeler, B.; Sampson, J.; Hartge, P.; Chanock, S.J.; Park, J.H. Projecting the performance of risk prediction based on polygenic analyses of genome-wide association studies. Nat. Genet. 2013, 45, 400–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pharoah, P.D.; Antoniou, A.; Bobrow, M.; Zimmern, R.L.; Easton, D.F.; Ponder, B.A. Polygenic susceptibility to breast cancer and implications for prevention. Nat. Genet. 2002, 31, 33–36. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Clinical Care Excellence. Familial Breast Cancer: Classification, Care and Managing Breast Cancer and Related Risks in People with a Family History of Breast Cancer. Clinical Guideline [CG164]. Last Updated 20 November 2019. Available online: www.nice.org.uk/guidance/cg164 (accessed on 14 April 2021).
- Brooks, J.D.; Nabi, H.H.; Andrulis, I.L.; Antoniou, A.C.; Chiquette, J.; Després, P.; Devilee, P.; Dorval, M.; Droit, A.; Easton, D.F.; et al. Personalized Risk Assessment for Prevention and Early Detection of Breast Cancer: Integration and Implementation (PERSPECTIVE I&I). J. Pers. Med. 2021, 11, 511. [Google Scholar] [PubMed]
- Quante, A.S.; Whittemore, A.S.; Shriver, T.; Hopper, J.L.; Strauch, K.; Terry, M.B. Practical problems with clinical guidelines for breast cancer prevention based on remaining lifetime risk. J. Natl. Cancer Inst. 2015, 107, djv124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacInnis, R.J.; Knight, J.A.; Chung, W.K.; Milne, R.L.; Whittemore, A.S.; Buchsbaum, R.; Liao, Y.; Zeinomar, N.; Dite, G.S.; Southey, M.C.; et al. Comparing Five-Year and Lifetime Risks of Breast Cancer in the Prospective Family Study Cohort. J. Natl. Cancer Inst. 2020, 113, 786–791. [Google Scholar]
- Feuer, E.J.; Wun, L.M.; Boring, C.C.; Flanders, W.D.; Timmel, M.J.; Tong, T. The lifetime risk of developing breast cancer. J. Natl. Cancer Inst. 1993, 85, 892–897. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
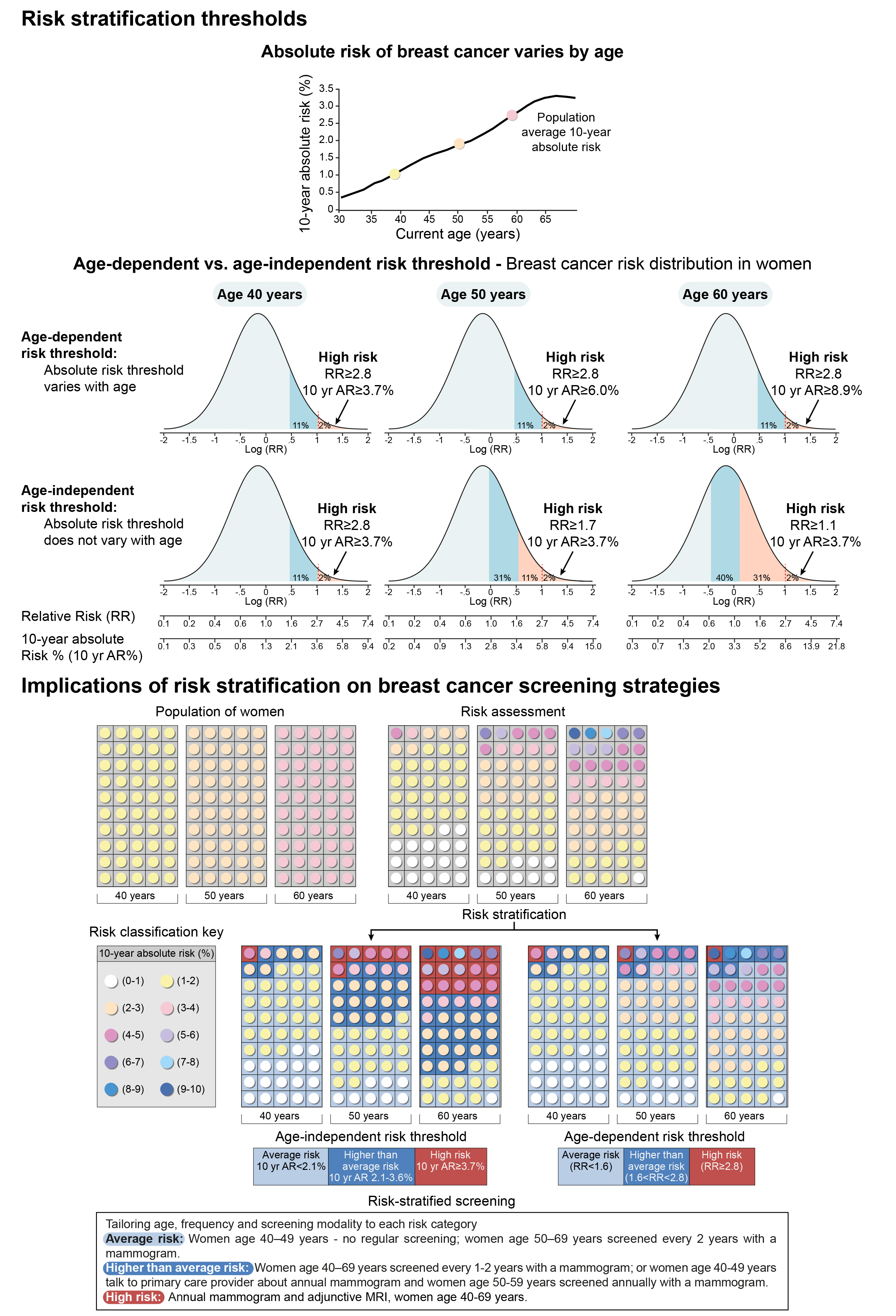
| Average Risk | Higher Than Average Risk | High Risk | |
|---|---|---|---|
| Age | 10-Year Absolute Risk % | 10-Year Absolute Risk % | 10-Year Absolute Risk % |
| 40 | [0, 2.0) | [2.0, 3.6) | [3.6, ) |
| 41 | [0, 2.2) | [2.2, 3.8) | [3.8, ) |
| 42 | [0, 2.3) | [2.3, 4.1) | [4.1, ) |
| 43 | [0, 2.5) | [2.5, 4.3) | [4.3, ) |
| 44 | [0, 2.6) | [2.6, 4.6) | [4.6, ) |
| 45 | [0, 2.8) | [2.8, 4.8) | [4.8, ) |
| 46 | [0, 2.9) | [2.9, 5.0) | [5.0, ) |
| 47 | [0, 3.0) | [3.0, 5.2) | [5.2, ) |
| 48 | [0, 3.1) | [3.1, 5.4) | [5.4, ) |
| 49 | [0, 3.2) | [3.2, 5.6) | [5.6, ) |
| 50 | [0, 3.3) | [3.3, 5.8) | [5.8, ) |
| 51 | [0, 3.4) | [3.4, 6.0) | [6.0, ) |
| 52 | [0, 3.5) | [3.5, 6.2) | [6.2, ) |
| 53 | [0, 3.7) | [3.7, 6.4) | [6.4, ) |
| 54 | [0, 3.8) | [3.8, 6.7) | [6.7, ) |
| 55 | [0, 4.0) | [4.0, 7.0) | [7.0, ) |
| 56 | [0, 4.2) | [4.2, 7.2) | [7.2, ) |
| 57 | [0, 4.4) | [4.4, 7.6) | [7.6, ) |
| 58 | [0, 4.6) | [4.6, 7.9) | [7.9, ) |
| 59 | [0, 4.8) | [4.8, 8.3) | [8.3, ) |
| 60 | [0, 5.0) | [5.0, 8.6) | [8.6, ) |
| 61 | [0, 5.1) | [5.1, 8.9) | [8.9, ) |
| 62 | [0, 5.3) | [5.3, 9.2) | [9.2, ) |
| 63 | [0, 5.5) | [5.5, 9.5) | [9.5, ) |
| 64 | [0, 5.6) | [5.6, 9.7) | [9.7, ) |
| 65 | [0, 5.7) | [5.7, 9.9) | [9.9, ) |
| 66 | [0, 5.8) | [5.8, 10.0) | [10.0, ) |
| 67 | [0, 5.8) | [5.8, 10.0) | [10.0, ) |
| 68 | [0, 5.8) | [5.8, 10.0) | [10.0, ) |
| 69 | [0, 5.7) | [5.7, 10.0) | [10.0, ) |
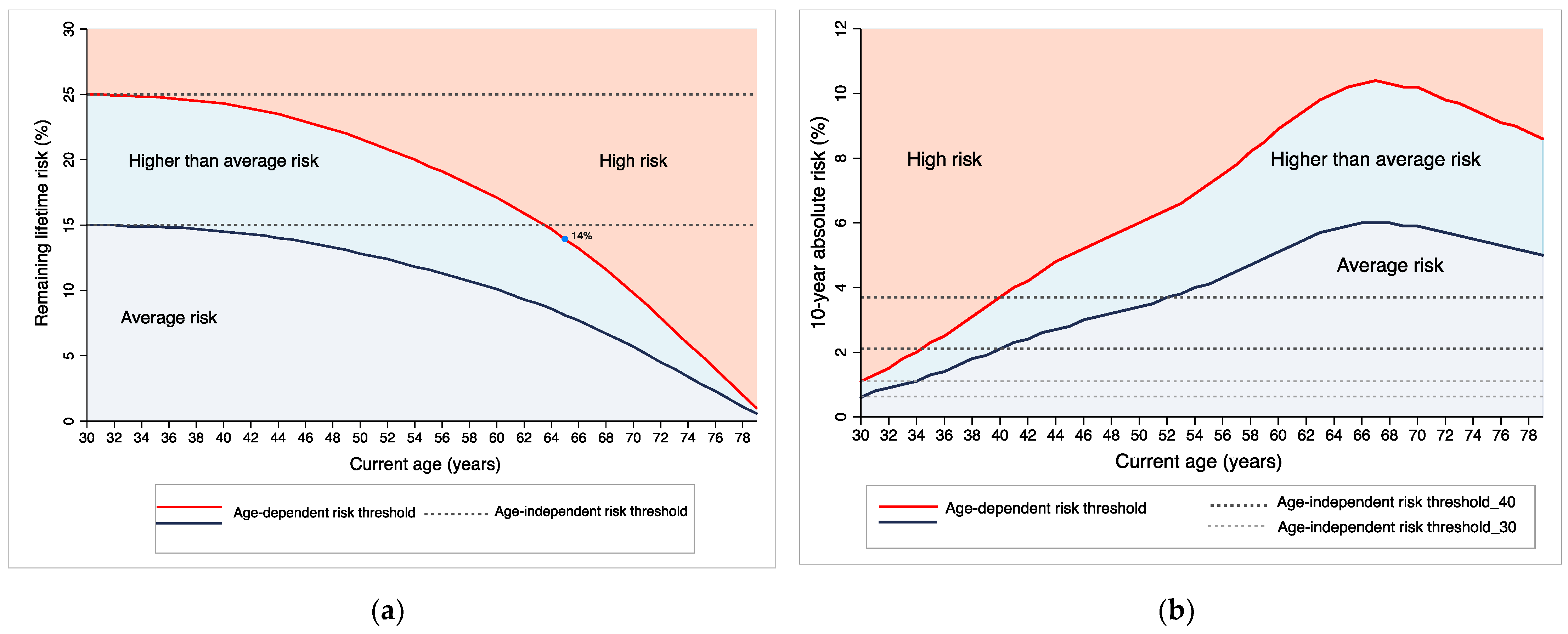
| Remaining Lifetime Risk Metric | |||||
| Age-independent risk threshold | Age-dependent risk threshold | ||||
| Current age | Population average remaining lifetime risk % | Remaining lifetime risk threshold for high risk (%) | Relative risk (high risk vs. population average risk) | Remaining lifetime risk threshold for high risk (%) | Relative risk (high risk vs. population average risk) |
| 30 | 10.1 | 25.0 | 2.7 | 25.0 | 2.7 |
| 35 | 10.0 | 25.0 | 2.7 | 24.8 | 2.7 |
| 40 | 9.8 | 25.0 | 2.8 | 24.3 | 2.7 |
| 45 | 9.3 | 25.0 | 2.9 | 23.2 | 2.7 |
| 50 | 8.6 | 25.0 | 3.2 | 21.6 | 2.7 |
| 55 | 7.7 | 25.0 | 3.6 | 19.5 | 2.7 |
| 60 | 6.7 | 25.0 | 4.1 | 17.1 | 2.7 |
| 65 | 5.4 | 25.0 | 5.2 | 13.9 | 2.7 |
| 10-year Absolute Risk Metric | |||||
| Age-independent risk threshold | Age-dependent risk threshold | ||||
| Current age | Population average 10-year absolute risk % | 10-year absolute risk threshold for high risk (%) | Relative risk (high risk vs. population average risk) | 10-year absolute risk threshold for high risk (%) | Relative risk (high risk vs. population average risk) |
| 30 | 0.4 | 1.1 | 2.7 | 1.1 | 2.7 |
| 35 | 0.8 | 1.1 | 1.4 | 2.2 | 2.7 |
| 40 | 1.3 | 1.1 | 0.8 | 3.6 | 2.7 |
| 45 | 1.8 | 1.1 | 0.6 | 4.8 | 2.7 |
| 50 | 2.2 | 1.1 | 0.5 | 5.8 | 2.7 |
| 55 | 2.6 | 1.1 | 0.4 | 7.0 | 2.7 |
| 60 | 3.3 | 1.1 | 0.3 | 8.6 | 2.7 |
| 65 | 3.8 | 1.1 | 0.3 | 9.9 | 2.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pashayan, N.; Antoniou, A.C.; Lee, A.; Wolfson, M.; Chiquette, J.; Eloy, L.; Eisen, A.; Stockley, T.L.; Nabi, H.; Brooks, J.D.; et al. Should Age-Dependent Absolute Risk Thresholds Be Used for Risk Stratification in Risk-Stratified Breast Cancer Screening? J. Pers. Med. 2021, 11, 916. https://doi.org/10.3390/jpm11090916
Pashayan N, Antoniou AC, Lee A, Wolfson M, Chiquette J, Eloy L, Eisen A, Stockley TL, Nabi H, Brooks JD, et al. Should Age-Dependent Absolute Risk Thresholds Be Used for Risk Stratification in Risk-Stratified Breast Cancer Screening? Journal of Personalized Medicine. 2021; 11(9):916. https://doi.org/10.3390/jpm11090916
Chicago/Turabian StylePashayan, Nora, Antonis C. Antoniou, Andrew Lee, Michael Wolfson, Jocelyne Chiquette, Laurence Eloy, Andrea Eisen, Tracy L. Stockley, Hermann Nabi, Jennifer D. Brooks, and et al. 2021. "Should Age-Dependent Absolute Risk Thresholds Be Used for Risk Stratification in Risk-Stratified Breast Cancer Screening?" Journal of Personalized Medicine 11, no. 9: 916. https://doi.org/10.3390/jpm11090916