
Update on Robotic Total Mesorectal Excision for Rectal Cancer

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Surgical Technique
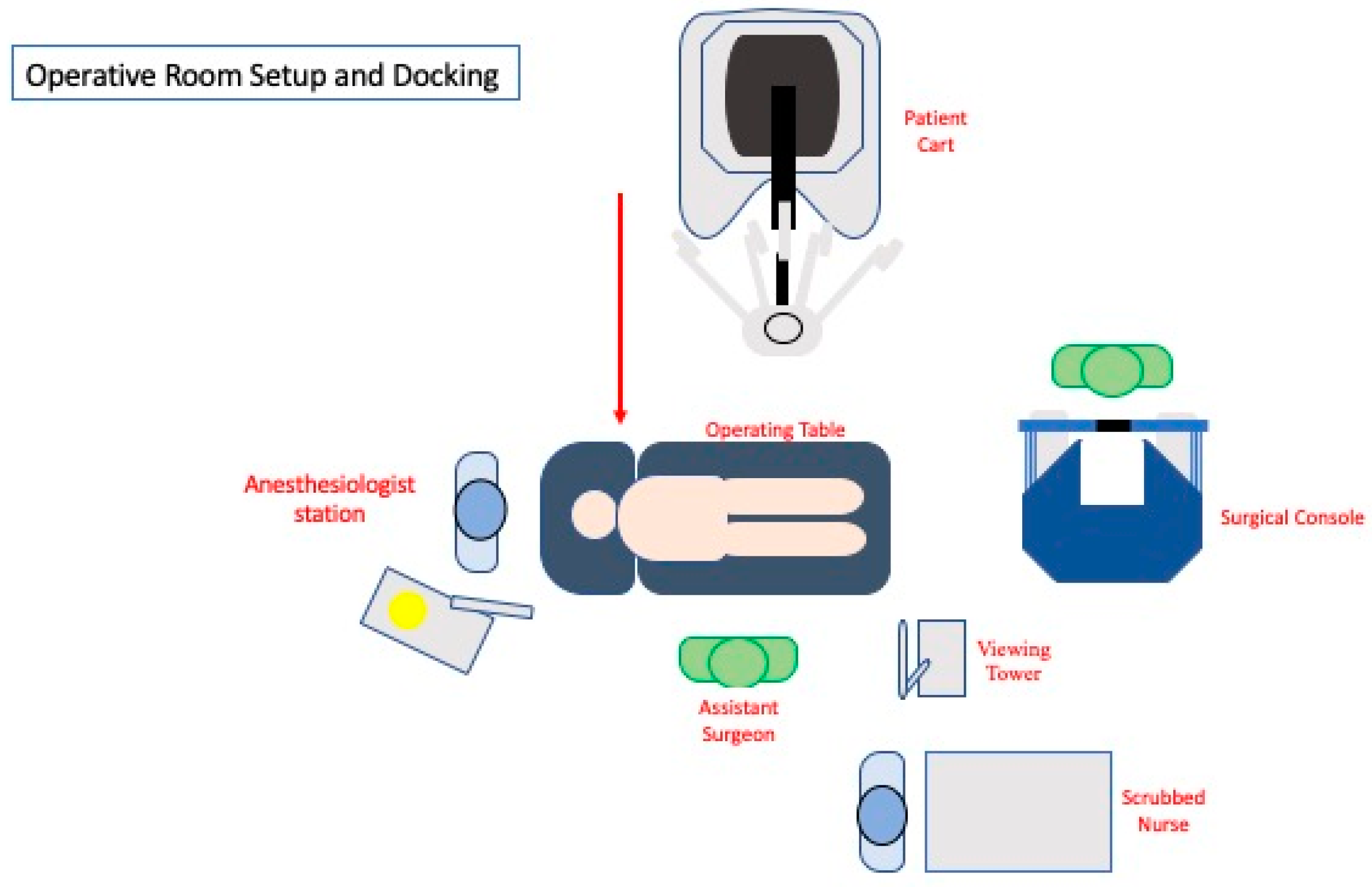
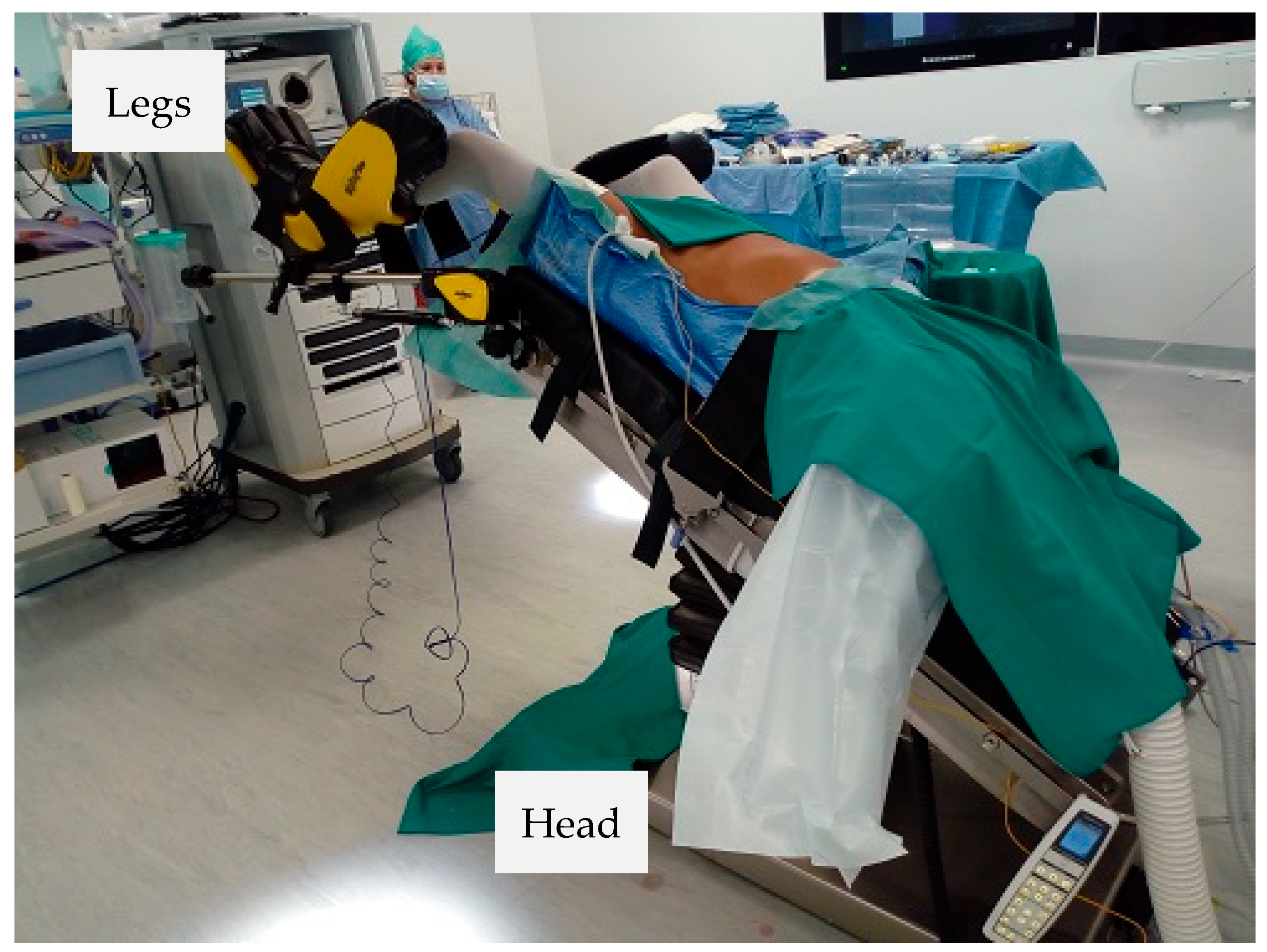
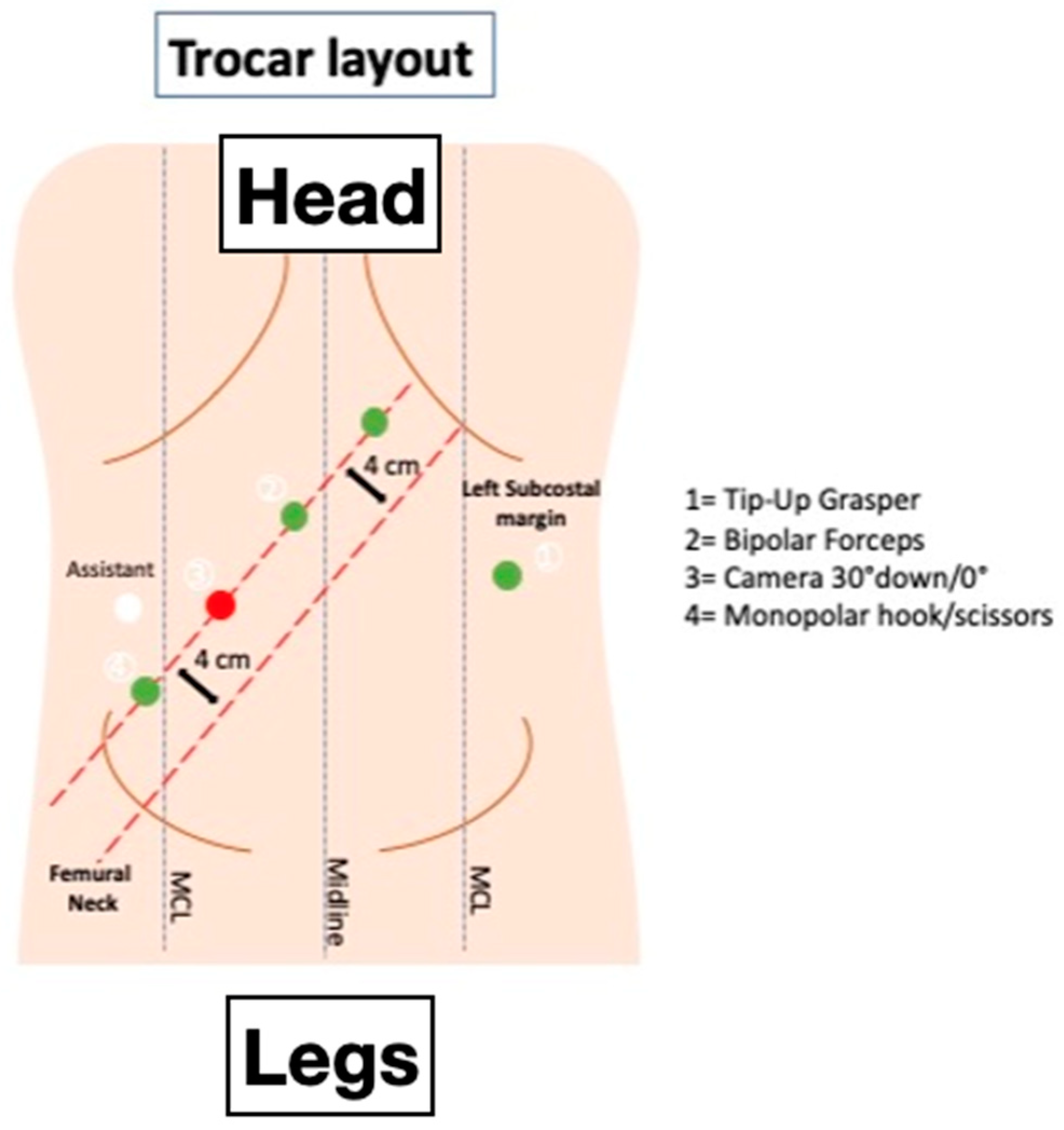
2.1. Patient Positioning and Docking
2.2. Step-By-Step Technique
- -
- Vascular control;
- -
- TME;
- -
- Splenic flexure mobilization.
2.3. Vascular Control
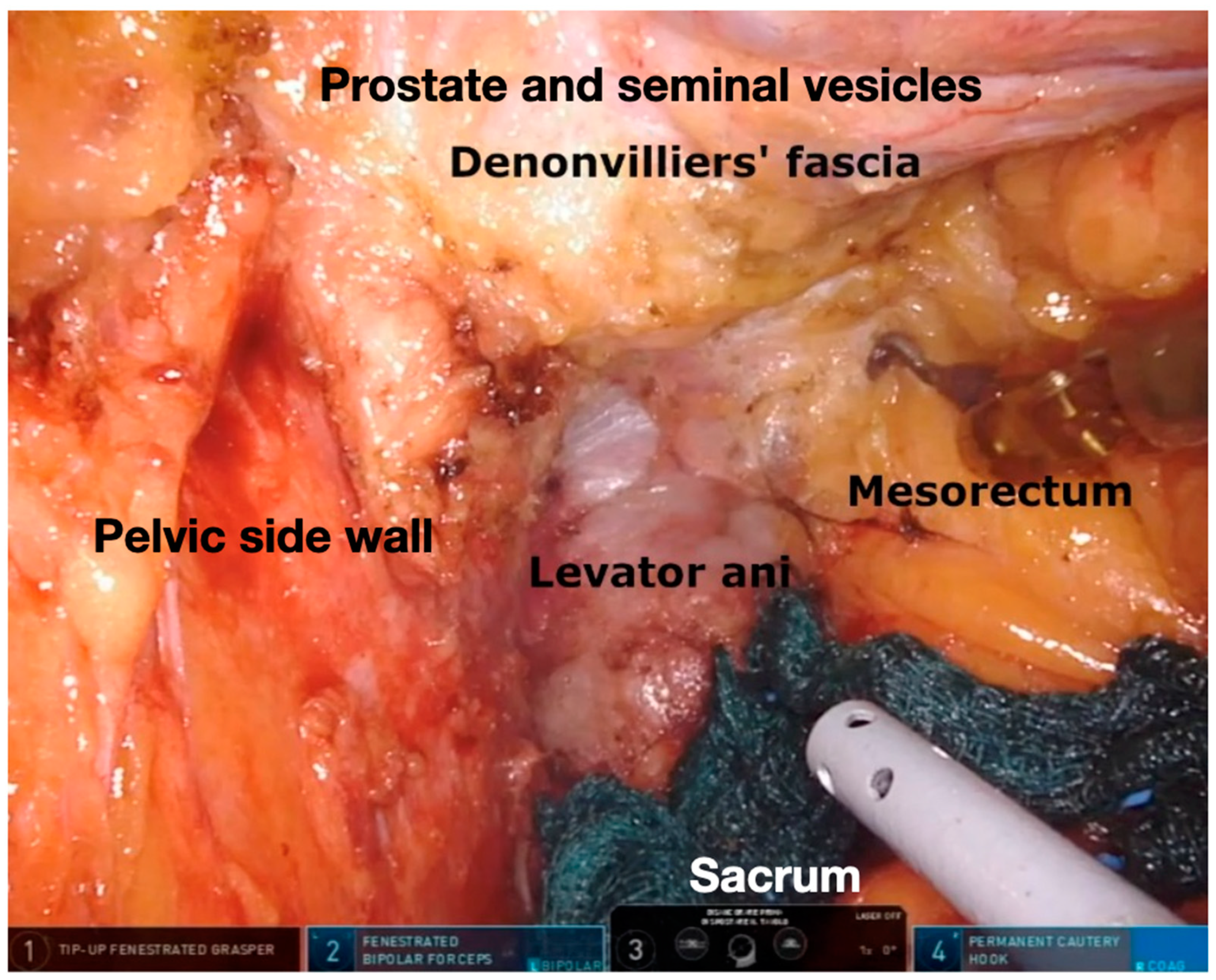
2.4. TME
2.5. Splenic Flexure Mobilization
3. Discussion and Literature Review
3.1. Intraoperative and Short-Term Postoperative Outcomes
3.2. Functional Outcomes
3.3. Oncological Outcomes
3.4. Costs
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heald, R.J.; Husband, E.M.; Ryall, R.D.H. The mesorectum in rectal cancer surgery—The clue to pelvic recurrence? J. Br. Surg. 2005, 69, 613–616. [Google Scholar] [CrossRef]
- Lacy, A.M.; Tasende, M.M.; Delgado, S.; Fernandez-Hevia, M.; Jimenez, M.; De Lacy, B.; Castells, A.; Bravo, R.; Wexner, S.D.; Heald, R.J. Transanal Total Mesorectal Excision for Rectal Cancer: Outcomes after 140 Patients. J. Am. Coll. Surg. 2015, 221, 415–423. [Google Scholar] [CrossRef]
- González-Abós, C.; De Lacy, F.B.; Guzmán, Y.; Nogueira, S.T.; Otero-Piñeiro, A.; Almenara, R.; Lacy, A.M. Transanal total mesorectal excision for stage II or III rectal cancer: Pattern of local recurrence in a tertiary referral center. Surg. Endosc. 2021, 1–9. [Google Scholar] [CrossRef]
- Deijen, C.L.; Velthuis, S.; Tsai, A.; Mavroveli, S.; Klerk, E.S.M.D.L.-D.; Sietses, C.; Tuynman, J.B.; Lacy, A.M.; Hanna, G.B.; Bonjer, H.J. COLOR III: A multicentre randomised clinical trial comparing transanal TME versus laparoscopic TME for mid and low rectal cancer. Surg. Endosc. 2016, 30, 3210–3215. [Google Scholar] [CrossRef] [Green Version]
- Roodbeen, S.X.; Penna, M.; MacKenzie, H.; Kusters, M.; Slater, A.; Jones, O.M.; Lindsey, I.; Guy, R.J.; Cunningham, C.; Hompes, R. Transanal total mesorectal excision (TaTME) versus laparoscopic TME for MRI-defined low rectal cancer: A propensity score-matched analysis of oncological outcomes. Surg. Endosc. 2019, 33, 2459–2467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillou, P.J.; Quirke, P.; Thorpe, H.; Walker, J.; Jayne, D.G.; Smith, A.M.; Heath, R.M.; Brown, J.M. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): Multicentre, randomised controlled trial. Lancet 2005, 365, 1718–1726. [Google Scholar] [CrossRef]
- Hazebroek, E.J.; The Color Study. COLOR: A randomized clinical trial comparing laparoscopic and open resection for colon cancer. Surg. Endosc. 2002, 16, 949–953. [Google Scholar] [CrossRef]
- Clinical Outcomes of Surgical Therapy Study Group; Nelson, H.; Sargent, D.; Wieand, H.S.; Fleshman, J.; Anvari, M.; Stryker, S.J.; Beart, R.W.; Hellinger, M.; Flanagan, R.; et al. A Comparison of Laparoscopically Assisted and Open Colectomy for Colon Cancer. N. Engl. J. Med. 2004, 350, 2050–2059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kearney, D.E.; Coffey, J.C. A Randomized Trial of Laparoscopic versus Open Surgery for Rectal Cancer. N. Engl. J. Med. 2015, 373, 194. [Google Scholar] [CrossRef] [Green Version]
- Van der Pas, M.H.; Haglind, E.; Cuesta, M.A.; Fürst, A.; Lacy, A.M.; Hop, W.C.; Bonjer, H.J.; COlorectal cancer Laparoscopic or Open Resection II (COLOR II) Study Group. Laparoscopic versus open surgery for rectal cancer (COLOR II): Short-term outcomes of a randomised, phase 3 trial. Lancet Oncol. 2013, 14, 210–218. [Google Scholar] [CrossRef]
- Jayne, D.G.; Guillou, P.J.; Thorpe, H.; Quirke, P.; Copeland, J.; Smith, A.M.; Heath, R.M.; Brown, J.M. Randomized Trial of Laparoscopic-Assisted Resection of Colorectal Carcinoma: 3-Year Results of the UK MRC CLASICC Trial Group. J. Clin. Oncol. 2007, 25, 3061–3068. [Google Scholar] [CrossRef] [PubMed]
- Jayne, D.G.; Thorpe, H.C.; Copeland, J.; Quirke, P.; Brown, J.M.; Guillou, P.J. Five-year follow-up of the Medical Research Council CLASICC trial of laparoscopically assisted versus open surgery for colorectal cancer. J. Br. Surg. 2010, 97, 1638–1645. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.-Y.; Park, J.W.; Nam, B.H.; Kim, S.; Kang, S.-B.; Lim, S.-B.; Choi, H.S.; Kim, D.-W.; Chang, H.J.; Kim, D.Y.; et al. Open versus laparoscopic surgery for mid-rectal or low-rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): Survival outcomes of an open-label, non-inferiority, randomised controlled trial. Lancet Oncol. 2014, 15, 767–774. [Google Scholar] [CrossRef]
- Kang, S.-B.; Park, J.W.; Jeong, S.-Y.; Nam, B.H.; Choi, H.S.; Kim, D.-W.; Lim, S.-B.; Lee, T.-G.; Kim, D.Y.; Kim, J.-S.; et al. Open versus laparoscopic surgery for mid or low rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): Short-term outcomes of an open-label randomised controlled trial. Lancet Oncol. 2010, 11, 637–645. [Google Scholar] [CrossRef]
- Stevenson, A.R.L.; Solomon, M.; Lumley, J.W.; Hewett, P.; Clouston, A.; Gebski, V.; Davies, L.; Wilson, C.; Hague, W.; Simes, J. Effect of Laparoscopic-Assisted Resection vs Open Resection on Pathological Outcomes in Rectal Cancer: The ALaCaRT Randomized Clinical Trial. JAMA 2015, 314, 1356–1363. [Google Scholar] [CrossRef] [Green Version]
- Fleshman, J.W.; Branda, M.E.; Sargent, D.J.; Boller, A.M.; George, V.; Abbas, M.A.; Peters, W.R.; Maun, D.; Chang, G.; Herline, A.J.; et al. Effect of Laparoscopic-Assisted Resection vs Open Resection of Stage II or III Rectal Cancer on Pathologic Outcomes: The ACOSOG Z6051 Randomized Clinical Trial. JAMA 2015, 314, 1346–1355. [Google Scholar] [CrossRef]
- Fleshman, J.; Branda, M.E.; Sargent, D.J.; Boller, A.M.; George, V.V.; Abbas, M.A.; Peters, W.R.; Maun, D.C.; Chang, G.J.; Herline, A.; et al. Disease-free Survival and Local Recurrence for Laparoscopic Resection Compared with Open Resection of Stage II to III Rectal Cancer: Follow-up Results of the ACOSOG Z6051 Randomized Controlled Trial. Ann. Surg. 2019, 269, 589–595. [Google Scholar] [CrossRef]
- Pigazzi, A.; Ellenhorn, J.D.I.; Ballantyne, G.H.; Paz, I.B. Robotic-assisted laparoscopic low anterior resection with total mesorectal excision for rectal cancer. Surg. Endosc. 2006, 20, 1521–1525. [Google Scholar] [CrossRef]
- Jayne, D.; Pigazzi, A.; Marshall, H.; Croft, J.; Corrigan, N.; Copeland, J.; Quirke, P.; West, N.; Rautio, T.; Thomassen, N.; et al. Effect of Robotic-Assisted vs Conventional Laparoscopic Surgery on Risk of Conversion to Open Laparotomy Among Patients Undergoing Resection for Rectal Cancer: The ROLARR Randomized Clinical Trial. JAMA 2017, 318, 1569–1580. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Kim, J.; Adam, M.A.; Nussbaum, D.P.; Speicher, P.J.; Mantyh, C.R.; Migaly, J. Minimally Invasive Versus Open Low Anterior Resection: Equivalent Survival in a National Analysis of 14,033 Patients With Rectal Cancer. Ann. Surg. 2016, 263, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Bhama, A.R.; Obias, V.; Welch, K.B.; Vandewarker, J.F.; Cleary, R.K. A comparison of laparoscopic and robotic colorectal surgery outcomes using the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database. Surg. Endosc. 2015, 30, 1576–1584. [Google Scholar] [CrossRef]
- Tam, M.S.; Kaoutzanis, C.; Mullard, A.J.; Regenbogen, S.E.; Franz, M.G.; Hendren, S.; Krapohl, G.; Vandewarker, J.F.; Lampman, R.M.; Cleary, R.K. A population-based study comparing laparoscopic and robotic outcomes in colorectal surgery. Surg. Endosc. 2016, 30, 455–463. [Google Scholar] [CrossRef]
- Al-Mazrou, A.M.; Chiuzan, C.; Kiran, R.P. The robotic approach significantly reduces length of stay after colectomy: A propensity score-matched analysis. Int. J. Color. Dis. 2017, 32, 1415–1421. [Google Scholar] [CrossRef] [PubMed]
- Altieri, M.S.; Yang, J.; Telem, D.A.; Zhu, J.; Halbert, C.; Talamini, M.; Pryor, A.D. Robotic approaches may offer benefit in colorectal procedures, more controversial in other areas: A review of 168,248 cases. Surg. Endosc. 2015, 30, 925–933. [Google Scholar] [CrossRef]
- Benlice, C.; Aytac, E.; Costedio, M.; Kessler, H.; Abbas, M.A.; Remzi, F.H.; Gorgun, E. Robotic, laparoscopic, and open colectomy: A case-matched comparison from the ACS-NSQIP. Int. J. Med. Robot. Comput. Assist. Surg. 2017, 13, e1783. [Google Scholar] [CrossRef]
- Al-Temimi, M.H.; Chandrasekaran, B.; Agapian, J.; Peters, W.R.; Wells, K.O. Robotic versus laparoscopic elective colectomy for left side diverticulitis: A propensity score–matched analysis of the NSQIP database. Int. J. Color. Dis. 2019, 34, 1385–1392. [Google Scholar] [CrossRef] [PubMed]
- Simillis, C.; Lal, N.; Thoukididou, S.N.; Kontovounisios, C.; Smith, J.J.; Hompes, R.; Adamina, M.; Tekkis, P.P. Open Versus Laparoscopic Versus Robotic Versus Transanal Mesorectal Excision for Rectal Cancer: A Systematic Review and Network Meta-analysis. Ann. Surg. 2019, 270, 59–68. [Google Scholar] [CrossRef]
- Polat, F.; Willems, L.H.; Dogan, K.; Rosman, C. The oncological and surgical safety of robot-assisted surgery in colorectal cancer: Outcomes of a longitudinal prospective cohort study. Surg. Endosc. 2019, 33, 3644–3655. [Google Scholar] [CrossRef] [Green Version]
- Phan, K.; Kahlaee, H.R.; Kim, S.H.; Toh, J.W.T. Laparoscopic vs. robotic rectal cancer surgery and the effect on conversion rates: A meta-analysis of randomized controlled trials and propensity-score-matched studies. Tech. Coloproctol. 2019, 23, 221–230. [Google Scholar] [CrossRef]
- Formisano, G.; Marano, A.; Bianchi, P.P.; Spinoglio, G. Challenges with robotic low anterior resection. Minerva Chir. 2015, 70, 341–354. [Google Scholar] [PubMed]
- Esposito, S.; Formisano, G.; Giuliani, G.; Misitano, P.; Krizzuk, D.; Salvischiani, L.; Bianchi, P.P. Update on robotic surgery for rectal cancer treatment. Ann. Laparosc. Endosc. Surg. 2017, 2, 132. [Google Scholar] [CrossRef]
- Park, S.Y.; Lee, S.M.; Park, J.S.; Kim, H.J.; Choi, G.S. Robot Surgery Shows Similar Long-term Oncologic Outcomes as Laparoscopic Surgery for Mid/Lower Rectal Cancer but Is Beneficial to ypT3/4 After Preoperative Chemoradiation. Dis. Colon. Rectum. 2021, 64, 812–821. [Google Scholar] [CrossRef] [PubMed]
- Petz, W.; Ribero, D.; Bertani, E.; Polizzi, M.L.; Spinoglio, G. Notes of robotic surgical technique: Four ways to mobilize splenic flex-ure. Minerva Chir. 2016, 71, 345–348. [Google Scholar] [PubMed]
- Xiong, B.; Ma, L.; Huang, W.; Zhao, Q.; Cheng, Y.; Liu, J. Robotic Versus Laparoscopic Total Mesorectal Excision for Rectal Cancer: A Meta-analysis of Eight Studies. J. Gastrointest. Surg. 2015, 19, 516–526. [Google Scholar] [CrossRef] [PubMed]
- Xiong, B.; Ma, L.; Zhang, C.; Cheng, Y. Robotic versus laparoscopic total mesorectal excision for rectal cancer: A meta-analysis. J. Surg. Res. 2014, 188, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Trastulli, S.; Farinella, E.; Cirocchi, R.; Cavaliere, D.; Avenia, N.; Sciannameo, F.; Gullà, N.; Noya, G.; Boselli, C. Robotic resection compared with laparoscopic rectal resection for cancer: Systematic review and meta-analysis of short-term outcome. Color. Dis. 2012, 14, e134–e156. [Google Scholar] [CrossRef]
- Sun, Y.; Xu, H.; Li, Z.; Han, J.; Song, W.; Wang, J.; Xu, Z. Robotic versus laparoscopic low anterior resection for rectal cancer: A meta-analysis. World J. Surg. Oncol. 2016, 14, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Holmer, C.; Kreis, M.E. Systematic review of robotic low anterior resection for rectal cancer. Surg. Endosc. 2018, 32, 569–581. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, D.H.; Lim, S.W. Robotic versus laparoscopic intersphincteric resection for low rectal cancer: A systematic review and meta-analysis. Int. J. Color. Dis. 2018, 33, 1741–1753. [Google Scholar] [CrossRef]
- Ohtani, H.; Maeda, K.; Nomura, S.; Shinto, O.; Mizuyama, Y.; Nakagawa, H.; Nagahara, H.; Shibutani, M.; Fukuoka, T.; Amano, R.; et al. Meta-analysis of Robot-assisted Versus Laparoscopic Surgery for Rectal Cancer. In Vivo 2018, 32, 611–623. [Google Scholar] [CrossRef] [Green Version]
- Prete, F.; Pezzolla, A.; Prete, F.; Testini, M.; Marzaioli, R.; Patriti, A.; Jimenez-Rodriguez, R.M.; Gurrado, A.; Strippoli, G.F.M. Robotic Versus Laparoscopic Minimally Invasive Surgery for Rectal Cancer: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Ann. Surg. 2018, 267, 1034–1046. [Google Scholar] [CrossRef]
- Cui, Y.; Li, C.; Xu, Z.; Wang, Y.; Sun, Y.; Xu, H.; Li, Z.; Sun, Y. Robot-assisted versus conventional laparoscopic operation in anus-preserving rectal cancer: A meta-analysis. Ther. Clin. Risk Manag. 2017, 13, 1247–1257. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.J.; Park, S.C.; Park, J.W.; Chang, H.J.; Kim, D.Y.; Nam, B.-H.; Sohn, D.K.; Oh, J.H. Robot-assisted Versus Laparoscopic Surgery for Rectal Cancer: Phase II Open Label Prospective Randomized Controlled Trial. Ann. Surg. 2018, 267, 243–251. [Google Scholar] [CrossRef]
- Morelli, L.; Guadagni, S.; Di Franco, G.; Palmeri, M.; Caprili, G.; D’Isidoro, C.; Cobuccio, L.; Marciano, E.; Di Candio, G.; Mosca, F. Use of the new da Vinci Xi® during robotic rectal resection for cancer: A pilot matched-case comparison with the da Vinci Si®. Int. J. Med. Robot. Comput. Assist. Surg. 2016, 13, e1728. [Google Scholar] [CrossRef] [Green Version]
- Araujo, S.E.A.; Seid, V.E.; Klajner, S. Robotic surgery for rectal cancer: Current immediate clinical and oncological outcomes. World J. Gastroenterol. 2014, 20, 14359–14370. [Google Scholar] [CrossRef]
- Ackerman, S.J.; Daniel, S.; Baik, R.; Liu, E.; Mehendale, S.; Tackett, S.; Hellan, M. Comparison of complication and conversion rates between robotic-assisted and laparoscopic rectal resection for rectal cancer: Which patients and providers could benefit most from robotic-assisted surgery? J. Med. Econ. 2017, 21, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Crippa, J.; Grass, F.; Dozois, E.J.; Mathis, K.L.; Merchea, A.; Colibaseanu, D.T.; Kelley, S.R.; Larson, D.W. Robotic Surgery for Rectal Cancer Provides Advantageous Outcomes Over Laparoscopic Approach: Results From a Large Retrospective Cohort. Ann. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Crippa, J.; Grass, F.; Achilli, P.; Mathis, K.L.; Kelley, S.R.; Merchea, A.; Colibaseanu, D.T.; Larson, D.W. Risk factors for conversion in laparoscopic and robotic rectal cancer surgery. J. Br. Surg. 2020, 107, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Katsuno, H.; Hanai, T.; Masumori, K.; Koide, Y.; Ashida, K.; Matsuoka, H.; Tajima, Y.; Endo, T.; Mizuno, M.; Cheong, Y.; et al. Robotic Surgery for Rectal Cancer: Operative Technique and Review of the Literature. J. Anus Rectum Colon 2020, 4, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, P.P.; Ceriani, C.; Locatelli, A.; Spinoglio, G.; Zampino, M.G.; Sonzogni, A.M.; Crosta, C.; Andreoni, L.B. Robotic versus laparoscopic total mesorectal excision for rectal cancer: A comparative analysis of oncological safety and short-term outcomes. Surg. Endosc. 2010, 24, 2888–2894. [Google Scholar] [CrossRef] [PubMed]
- Fleming, C.A.; Cullinane, C.; Lynch, N.; Killeen, S.; Coffey, J.C.; Peirce, C.B. Urogenital function following robotic and laparoscopic rectal cancer surgery: Meta-analysis. J. Br. Surg. 2021, 108, 128–137. [Google Scholar] [CrossRef]
- Kowalewski, K.F.; Seifert, L.; Ali, S.; Schmidt, M.W.; Seide, S.; Haney, C.; Tapking, C.; Shamiyeh, A.; Kulu, Y.; Hackert, T.; et al. Functional outcomes after laparoscopic versus robotic-assisted rectal resection: A systematic review and meta-analysis. Surg. Endosc. 2021, 35, 81–95. [Google Scholar] [CrossRef] [Green Version]
- Quirke, P.; Steele, R.J.; Monson, J.; Grieve, R.; Khanna, S.; Couture, J.; O’Callaghan, C.; Myint, A.S.; Bessell, E.; Thompson, L.C.; et al. Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: A prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. Lancet 2009, 373, 821–828. [Google Scholar] [CrossRef] [Green Version]
- Baik, S.H.; Kwon, H.Y.; Kim, J.S.; Hur, H.; Sohn, S.K.; Cho, C.H.; Kim, H. Robotic Versus Laparoscopic Low Anterior Resection of Rectal Cancer: Short-Term Outcome of a Prospective Comparative Study. Ann. Surg. Oncol. 2009, 16, 1480–1487. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kim, N.-K.; Lee, K.Y.; Hur, H.; Min, B.S.; Kim, J.H. A Comparative Study of Voiding and Sexual Function after Total Mesorectal Excision with Autonomic Nerve Preservation for Rectal Cancer: Laparoscopic Versus Robotic Surgery. Ann. Surg. Oncol. 2012, 19, 2485–2493. [Google Scholar] [CrossRef]
- Nagtegaal, I.; van Krieken, J. The role of pathologists in the quality control of diagnosis and treatment of rectal cancer—An overview. Eur. J. Cancer 2002, 38, 964–972. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Quirke, P. What Is the Role for the Circumferential Margin in the Modern Treatment of Rectal Cancer? J. Clin. Oncol. 2008, 26, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Milone, M.; Manigrasso, M.; Velotti, N.; Torino, S.; Vozza, A.; Sarnelli, G.; Aprea, G.; Maione, F.; Gennarelli, N.; Musella, M.; et al. Completeness of total mesorectum excision of laparoscopic versus robotic surgery: A review with a meta-analysis. Int. J. Color. Dis. 2019, 34, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Park, E.J.; Cho, M.S.; Baek, S.J.; Hur, H.; Min, B.S.; Baik, S.H.; Lee, K.Y.; Kim, N.-K. Long-term Oncologic Outcomes of Robotic Low Anterior Resection for Rectal Cancer: A comparative study with laparoscopic surgery. Ann. Surg. 2015, 261, 129–137. [Google Scholar] [CrossRef]
- Cho, M.S.; Baek, S.J.; Hur, H.; Min, B.S.; Baik, S.H.; Lee, K.Y.; Kim, N.-K. Short and Long-Term Outcomes of Robotic versus Laparoscopic Total Mesorectal Excision for Rectal Cancer: A case-matched retrospective study. Medicine 2015, 94, e522. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Baek, S.-J.; Kang, D.-W.; Roh, Y.-E.; Lee, J.W.; Kwak, H.-D.; Kwak, J.M.; Kim, S.-H. Robotic Resection is a Good Prognostic Factor in Rectal Cancer Compared with Laparoscopic Resection: Long-term Survival Analysis Using Propensity Score Matching. Dis. Colon Rectum 2017, 60, 266–273. [Google Scholar] [CrossRef]
- Fung, A.K.; Aly, E.H. Robotic colonic surgery: Is it advisable to commence a new learning curve? Dis. Colon Rectum 2013, 56, 786–796. [Google Scholar] [CrossRef] [PubMed]
- Rouanet, P.; Gourgou, S.; Gögenur, I.; Jayne, D.; Ulrich, A.; Rautio, T.; Spinoglio, G.; Bouazza, N.; Moussion, A.; Ruiz, M.G. Rectal Surgery Evaluation Trial: Protocol for a parallel cohort trial of outcomes using surgical techniques for total mesorectal excision with low anterior resection in high-risk rectal cancer patients. Color. Dis. 2019, 21, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Higgins, R.M.; Frelich, M.J.; Bosler, M.E.; Gould, J.C. Cost analysis of robotic versus laparoscopic general surgery procedures. Surg. Endosc. 2016, 31, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Khorgami, Z.; Li, W.T.; Jackson, T.N.; Howard, C.A.; Sclabas, G.M. The cost of robotics: An analysis of the added costs of robotic-assisted versus laparoscopic surgery using the National Inpatient Sample. Surg. Endosc. 2018, 33, 2217–2221. [Google Scholar] [CrossRef] [PubMed]
- Cleary, R.K.; Mullard, A.J.; Ferraro, J.; Regenbogen, S.E. The cost of conversion in robotic and laparoscopic colorectal surgery. Surg. Endosc. 2018, 32, 1515–1524. [Google Scholar] [CrossRef] [PubMed]
- Regenbogen, S.E.; Veenstra, C.M.; Hawley, S.T.; Banerjee, M.; Ward, K.C.; Kato, I.; Morris, A.M. The personal financial burden of complications after colorectal cancer surgery. Cancer 2014, 120, 3074–3081. [Google Scholar] [CrossRef] [Green Version]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giuratrabocchetta, S.; Formisano, G.; Salaj, A.; Opocher, E.; Ferraro, L.; Toti, F.; Bianchi, P.P. Update on Robotic Total Mesorectal Excision for Rectal Cancer. J. Pers. Med. 2021, 11, 900. https://doi.org/10.3390/jpm11090900
Giuratrabocchetta S, Formisano G, Salaj A, Opocher E, Ferraro L, Toti F, Bianchi PP. Update on Robotic Total Mesorectal Excision for Rectal Cancer. Journal of Personalized Medicine. 2021; 11(9):900. https://doi.org/10.3390/jpm11090900
Chicago/Turabian StyleGiuratrabocchetta, Simona, Giampaolo Formisano, Adelona Salaj, Enrico Opocher, Luca Ferraro, Francesco Toti, and Paolo Pietro Bianchi. 2021. "Update on Robotic Total Mesorectal Excision for Rectal Cancer" Journal of Personalized Medicine 11, no. 9: 900. https://doi.org/10.3390/jpm11090900