
Locked-in Intact Functional Networks in Children with Autism Spectrum Disorder: A Case-Control Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Resting-State MRI
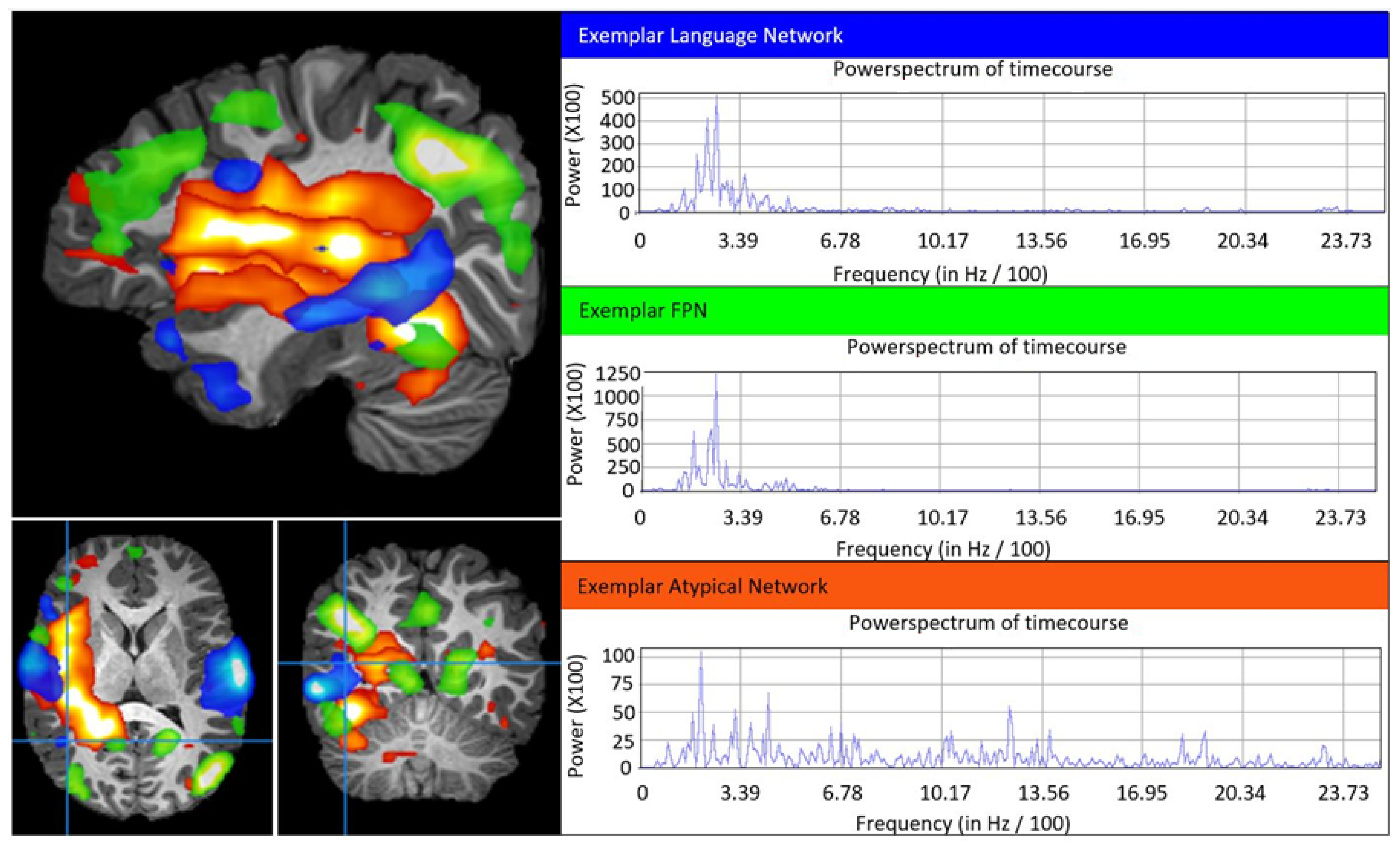
2.2. Independent Component Analysis Approach
2.3. Component Categorization
2.4. Statistical Analysis
3. Results
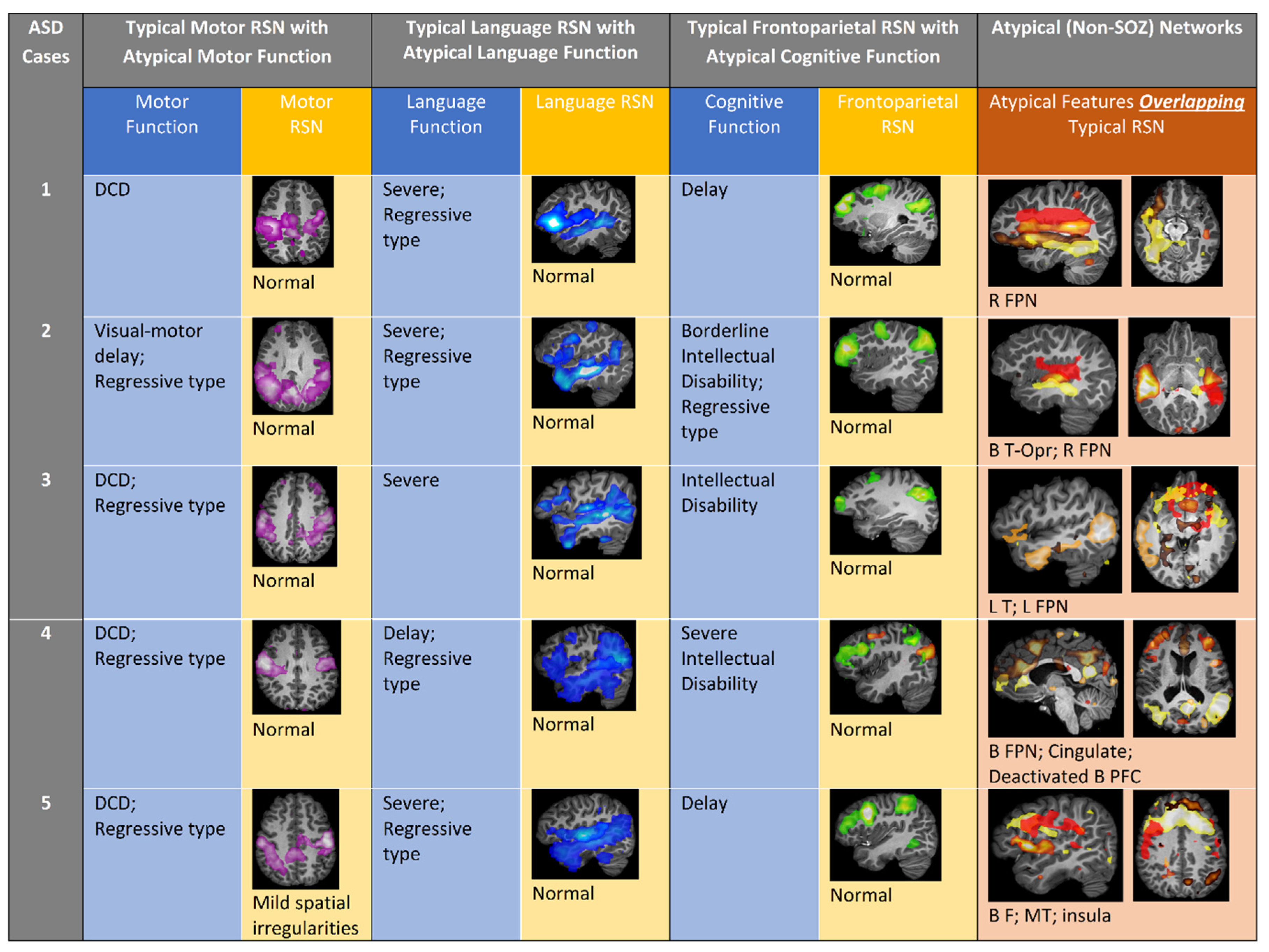
3.1. Patient Summaries of ASD Patients
3.1.1. Patient 1
3.1.2. Patient 2
3.1.3. Patient 3
3.1.4. Patient 4
3.1.5. Patient 5
3.2. Patient Summaries of TLE Patients (Controls)
3.2.1. Patient 6
3.2.2. Patient 7
3.2.3. Patient 8
3.2.4. Patient 9
3.2.5. Patient 10
3.3. Statistical Analysis
3.3.1. Clinical Characteristics
3.3.2. rs-fMRI Networks
3.3.3. Aberrant rs-fMRI Networks and Clinical Symptomatology
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years-Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- Hull, J.V.; Dokovna, L.B.; Jacokes, Z.J.; Torgerson, C.M.; Irimia, A.; Van Horn, J.D. Resting-State Functional Connectivity in Autism Spectrum Disorders: A Review. Front. Psychiatry 2016, 7, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zabihi, M.; Oldehinkel, M.; Wolfers, T.; Frouin, V.; Goyard, D.; Loth, E.; Charman, T.; Tillmann, J.; Banaschewski, T.; Dumas, G.; et al. Dissecting the Heterogeneous Cortical Anatomy of Autism Spectrum Disorder Using Normative Models. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019, 4, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Holiga, S.; Hipp, J.F.; Chatham, C.H.; Garces, P.; Spooren, W.; D’Ardhuy, X.L.; Bertolino, A.; Bouquet, C.; Buitelaar, J.K.; Bours, C.; et al. Patients with autism spectrum disorders display reproducible functional connectivity alterations. Sci. Transl. Med. 2019, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marek, S.; Dosenbach, N.U.F. The frontoparietal network: Function, electrophysiology, and importance of individual precision mapping. Dialogues Clin. Neurosci. 2018, 20, 133–140. [Google Scholar]
- Beckmann, C.F.; DeLuca, M.; Devlin, J.T.; Smith, S.M. Investigations into resting-state connectivity using independent component analysis. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2005, 360, 1001–1013. [Google Scholar] [CrossRef] [Green Version]
- Beckmann, C.F.; Smith, S.M. Probabilistic independent component analysis for functional magnetic resonance imaging. IEEE Trans. Med. Imaging 2004, 23, 137–152. [Google Scholar] [CrossRef]
- Boerwinkle, V.L.; Cediel, E.G.; Mirea, L.; Williams, K.; Kerrigan, J.F.; Lam, S.; Raskin, J.S.; Desai, V.R.; Wilfong, A.A.; Adelson, P.D.; et al. Network-targeted approach and postoperative resting-state functional magnetic resonance imaging are associated with seizure outcome. Ann. Neurol. 2019, 86, 344–356. [Google Scholar] [CrossRef] [Green Version]
- Boerwinkle, V.L.; Mirea, L.; Gaillard, W.D.; Sussman, B.L.; Larocque, D.; Bonnell, A.; Ronecker, J.S.; Troester, M.M.; Kerrigan, J.F.; Foldes, S.T.; et al. Resting-state functional MRI connectivity impact on epilepsy surgery plan and surgical candidacy: Prospective clinical work. J. Neurosurg. Pediatr. 2020, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Boerwinkle, V.L.; Wilfong, A.A.; Curry, D.J. Resting-state functional connectivity by independent component analysis-based markers corresponds to areas of initial seizure propagation established by prior modalities from the hypothalamus. Brain Connect. 2016, 6, 642–651. [Google Scholar] [CrossRef] [Green Version]
- Beckmann, C.F.; Noble, J.A.; Smith, S.M. Artefact detection in FMRI data using independent component analysis. NeuroImage 2000, 11, S614. [Google Scholar] [CrossRef]
- Griffanti, L.; Douaud, G.; Bijsterbosch, J.; Evangelisti, S.; Alfaro-Almagro, F.; Glasser, M.F.; Duff, E.P.; Fitzgibbon, S.; Westphal, R.; Carone, D.; et al. Hand classification of fMRI ICA noise components. Neuroimage 2017, 154, 188–205. [Google Scholar] [CrossRef]
- Damoiseaux, J.S.; Rombouts, S.A.; Barkhof, F.; Scheltens, P.; Stam, C.J.; Smith, S.M.; Beckmann, C.F. Consistent resting-state networks across healthy subjects. Proc. Natl. Acad. Sci. USA 2006, 103, 13848–13853. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Fox, P.T.; Miller, K.L.; Glahn, D.C.; Fox, P.M.; Mackay, C.E.; Filippini, N.; Watkins, K.E.; Toro, R.; Laird, A.R.; et al. Correspondence of the brain’s functional architecture during activation and rest. Proc. Natl. Acad. Sci. USA 2009, 106, 13040–13045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boerwinkle, V.L.; Mohanty, D.; Foldes, S.T.; Guffey, D.; Minard, C.G.; Vedantam, A.; Raskin, J.S.; Lam, S.; Bond, M.; Mirea, L.; et al. Correlating Resting-State Functional Magnetic Resonance Imaging Connectivity by Independent Component Analysis-Based Epileptogenic Zones with Intracranial Electroencephalogram Localized Seizure Onset Zones and Surgical Outcomes in Prospective Pediatric Intractable Epilepsy Study. Brain Connect. 2017, 7, 424–442. [Google Scholar] [CrossRef]
- Strasser, L.; Downes, M.; Kung, J.; Cross, J.H.; De Haan, M. Prevalence and risk factors for autism spectrum disorder in epilepsy: A systematic review and meta-analysis. Dev. Med. Child. Neurol. 2018, 60, 19–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Martino, F.; Gentile, F.; Esposito, F.; Balsi, M.; Di Salle, F.; Goebel, R.; Formisano, E. Classification of fMRI independent components using IC-fingerprints and support vector machine classifiers. Neuroimage 2007, 34, 177–194. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, M.; Bannister, P.; Brady, M.; Smith, S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage 2002, 17, 825–841. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, M.; Smith, S. A global optimisation method for robust affine registration of brain images. Med. Image Anal. 2001, 5, 143–156. [Google Scholar] [CrossRef]
- Greve, D.N.; Fischl, B. Accurate and robust brain image alignment using boundary-based registration. Neuroimage 2009, 48, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Pruim, R.H.R.; Mennes, M.; van Rooij, D.; Llera, A.; Buitelaar, J.K.; Beckmann, C.F. ICA-AROMA: A robust ICA-based strategy for removing motion artifacts from fMRI data. Neuroimage 2015, 112, 267–277. [Google Scholar] [CrossRef]
- Desai, V.R.; Vedantam, A.; Lam, S.K.; Mirea, L.; Foldes, S.T.; Curry, D.J.; Adelson, P.D.; Wilfong, A.A.; Boerwinkle, V.L. Language lateralization with resting-state and task-based functional MRI in pediatric epilepsy. J. Neurosurg. Pediatr. 2018, 23, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Hahamy, A.; Behrmann, M.; Malach, R. The idiosyncratic brain: Distortion of spontaneous connectivity patterns in autism spectrum disorder. Nat. Neurosci. 2015, 18, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.; Alcauter, S.; Smith, J.K.; Gilmore, J.H.; Lin, W. Development of human brain cortical network architecture during infancy. Brain Struct. Funct. 2015, 220, 1173–1186. [Google Scholar] [CrossRef] [PubMed]
- Fransson, P.; Aden, U.; Blennow, M.; Lagercrantz, H. The functional architecture of the infant brain as revealed by resting-state fMRI. Cereb. Cortex 2011, 21, 145–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bright Futures Steering Committee; Medical Home Initiatives for Children with Special Needs Project Advisory Committee. Identifying infants and young children with developmental disorders in the medical home: An algorithm for developmental surveillance and screening. Pediatrics 2006, 118, 405–420. [Google Scholar] [CrossRef] [Green Version]
- Marek, S.; Hwang, K.; Foran, W.; Hallquist, M.N.; Luna, B. The Contribution of Network Organization and Integration to the Development of Cognitive Control. PLoS Biol. 2015, 13, e1002328. [Google Scholar] [CrossRef] [Green Version]
- Boerwinkle, V.L.; Torrisi, S.J.; Foldes, S.T.; Marku, I.; Ranjan, M.; Wilfong, A.A.; Adelson, P.D. Resting-state fMRI in disorders of consciousness to facilitate early therapeutic intervention. Neurol. Clin. Pract. 2019, 9, e33–e35. [Google Scholar] [CrossRef] [PubMed]
- Boerwinkle, V.L.; Foldes, S.T.; Torrisi, S.J.; Temkit, H.; Gaillard, W.D.; Kerrigan, J.F.; Desai, V.R.; Raskin, J.S.; Vedantam, A.; Jarrar, R.; et al. Subcentimeter epilepsy surgery targets by resting state functional magnetic resonance imaging can improve outcomes in hypothalamic hamartoma. Epilepsia 2018, 59, 2284–2295. [Google Scholar] [CrossRef] [Green Version]
- Golkowski, D.; Larroque, S.K.; Vanhaudenhuyse, A.; Plenevaux, A.; Boly, M.; Di Perri, C.; Ranft, A.; Schneider, G.; Laureys, S.; Jordan, D.; et al. Changes in Whole Brain Dynamics and Connectivity Patterns during Sevoflurane- and Propofol-induced Unconsciousness Identified by Functional Magnetic Resonance Imaging. Anesthesiology 2019, 130, 898–911. [Google Scholar] [CrossRef] [Green Version]
- Hudetz, A.G. General anesthesia and human brain connectivity. Brain Connect. 2012, 2, 291–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirsch, M.; Guldenmund, P.; Ali Bahri, M.; Demertzi, A.; Baquero, K.; Heine, L.; Charland-Verville, V.; Vanhaudenhuyse, A.; Bruno, M.A.; Gosseries, O.; et al. Sedation of Patients With Disorders of Consciousness During Neuroimaging: Effects on Resting State Functional Brain Connectivity. Anesth. Analg. 2017, 124, 588–598. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic/Network | Participants with ASD (n = 5) | Participants with TLE (n = 5) | Fisher Exact Test p-Value |
| Clinical Characteristics | |||
| Motor Dysfunction | 100% (5) | 0% (0) | 0.008 |
| Language Dysfunction | 100% (5) | 40% (2) | 0.167 |
| Cognitive Dysfunction | 100% (5) | 0% (0) | 0.008 |
| Typical Resting-State Networks | |||
| Motor Network | 100% (5) | 100% (5) | 1.000 |
| Language Network | 100% (5) | 100% (5) | 1.000 |
| Frontoparietal Network | 100% (5) | 100% (5) | 1.000 |
| Aberrant Resting-State Networks | |||
| Motor Network | 40% (2) | 40% (2) | 1.000 |
| Language Network | 80% (4) | 20% (1) | 0.167 |
| Frontoparietal Network | 100% (5) | 0% (0) | 0.008 |
| Aberrant Network | Clinical Dysfunction Subserved by Network | No Clinical Dysfunction Subserved by Network | Fisher’s Exact Test p-Value |
|---|---|---|---|
| Motor Dysfunction | 100% (5) | 0% (0) | 1.000 |
| Language Dysfunction | 100% (5) | 40% (2) | 0.167 |
| Frontoparietal Network | 100% (5) | 0% (0) | 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pines, A.R.; Sussman, B.; Wyckoff, S.N.; McCarty, P.J.; Bunch, R.; Frye, R.E.; Boerwinkle, V.L. Locked-in Intact Functional Networks in Children with Autism Spectrum Disorder: A Case-Control Study. J. Pers. Med. 2021, 11, 854. https://doi.org/10.3390/jpm11090854
Pines AR, Sussman B, Wyckoff SN, McCarty PJ, Bunch R, Frye RE, Boerwinkle VL. Locked-in Intact Functional Networks in Children with Autism Spectrum Disorder: A Case-Control Study. Journal of Personalized Medicine. 2021; 11(9):854. https://doi.org/10.3390/jpm11090854
Chicago/Turabian StylePines, Andrew R., Bethany Sussman, Sarah N. Wyckoff, Patrick J. McCarty, Raymond Bunch, Richard E. Frye, and Varina L. Boerwinkle. 2021. "Locked-in Intact Functional Networks in Children with Autism Spectrum Disorder: A Case-Control Study" Journal of Personalized Medicine 11, no. 9: 854. https://doi.org/10.3390/jpm11090854