
A Critical Review of Radiation Therapy: From Particle Beam Therapy (Proton, Carbon, and BNCT) to Beyond

 ,
,  and
and
Abstract
:1. Background: Particle Beam Therapy as a Novel Radiotherapy
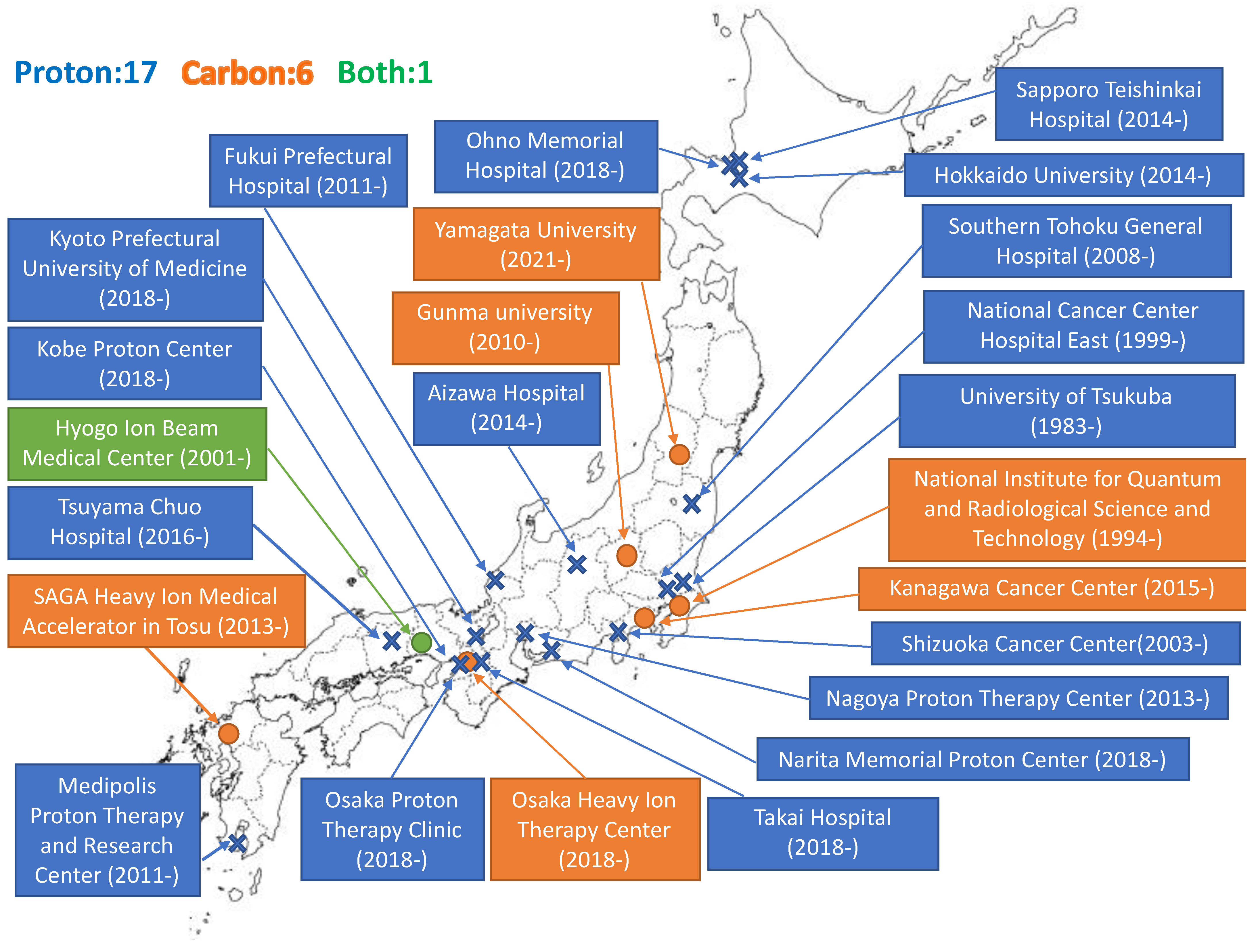
1.1. Promotion and Expansion of Particle Therapy Facilities
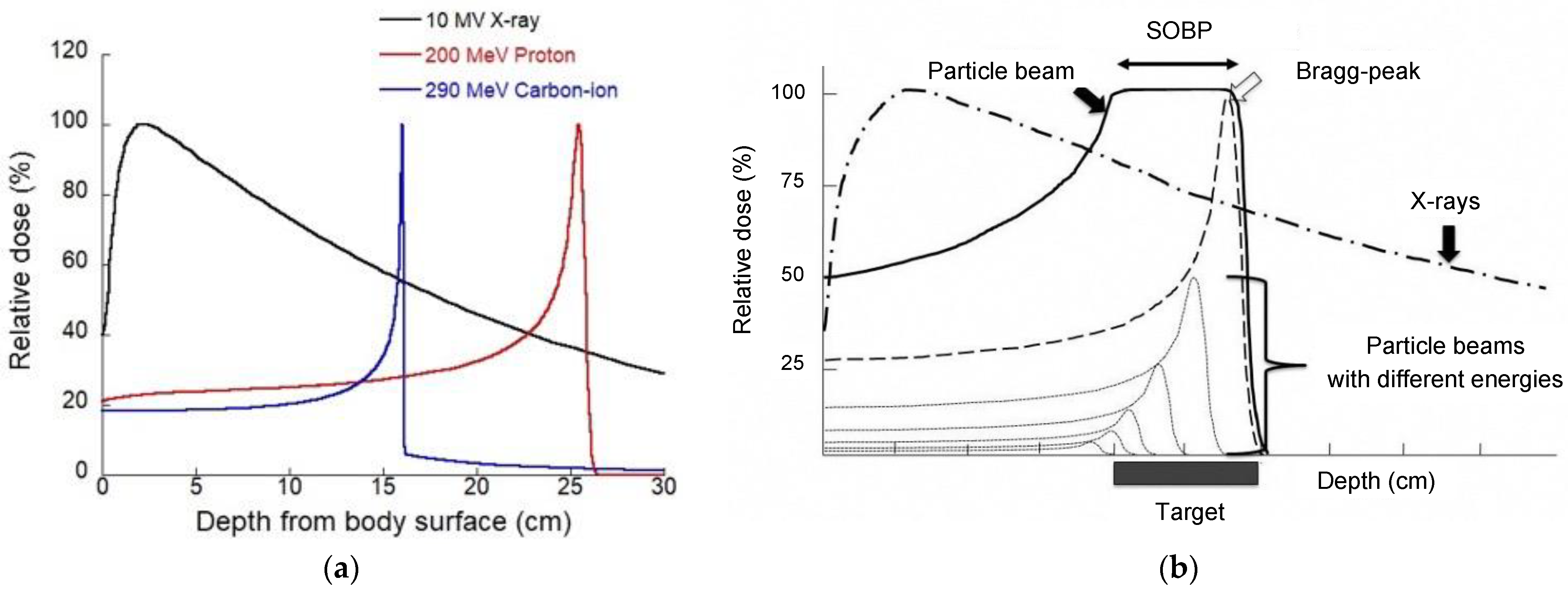
1.2. Physical Aspects of Particle Therapy
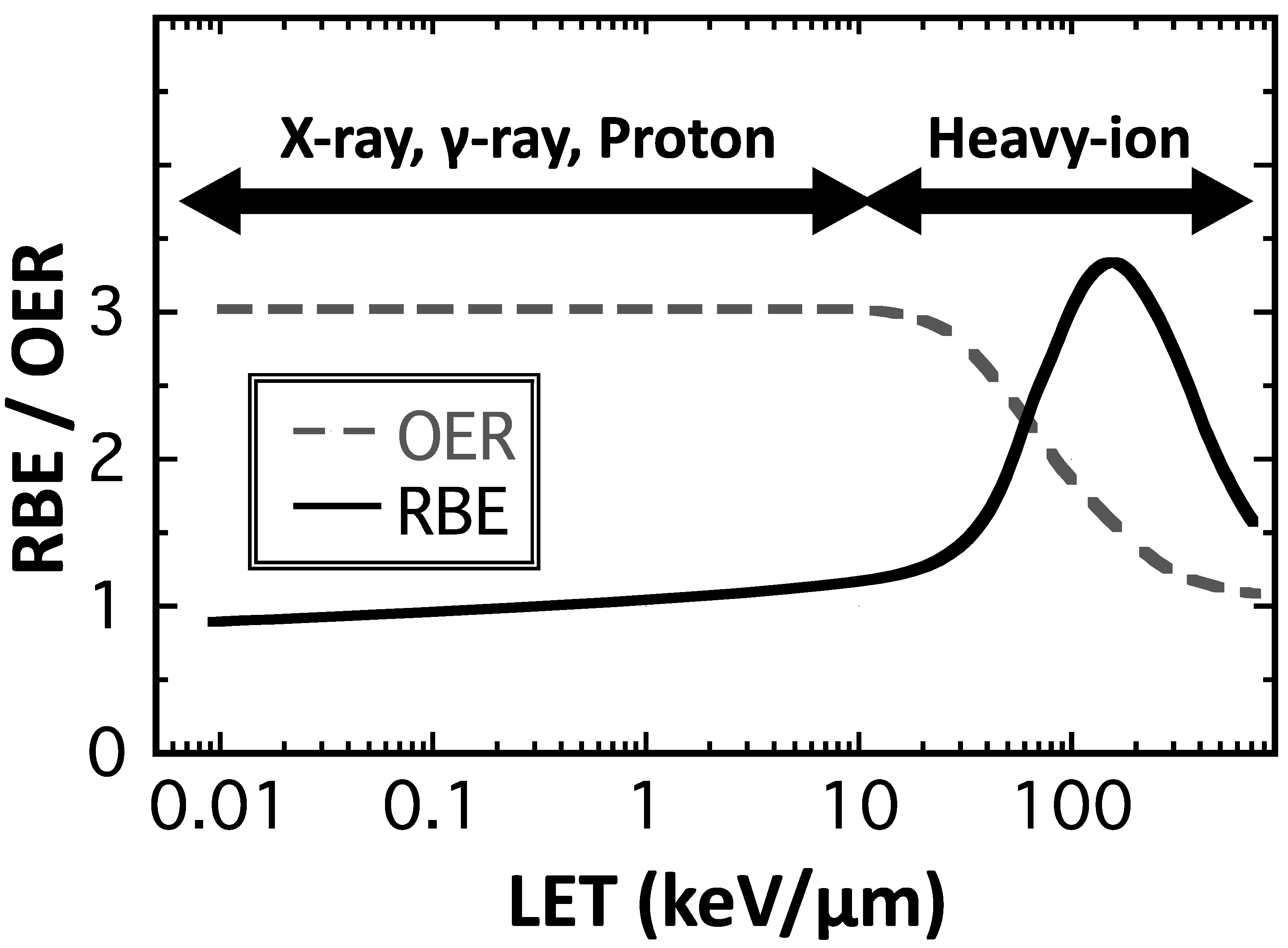
1.3. Biological Aspects of Particle Therapy
2. The Role of Particle Beam Therapy in Multidisciplinary Treatments in Clinics
2.1. Esophageal Cancer
2.2. Pancreatic Cancer
2.3. Prostate Cancer
2.4. Pediatric Cancer
3. Current Basic Research on Combination with Particle Therapy
3.1. Combination Therapy
3.2. Chemotherapy
3.3. Molecular Targeted Therapy
3.4. Nanoparticles
3.5. Immunotherapy
4. Relationship between Boron Neutron Capture Therapy (BNCT) and Boron Compounds
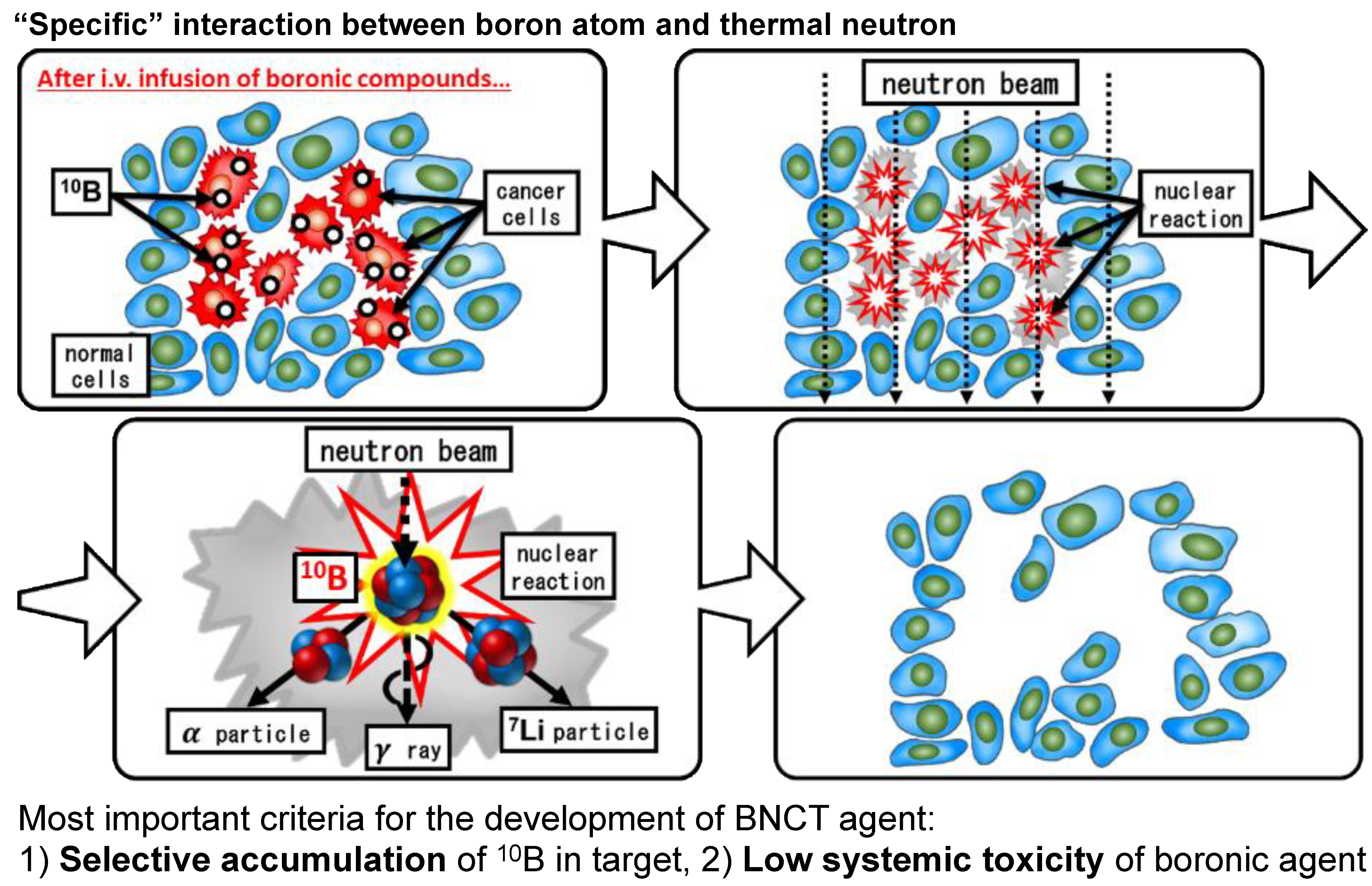
4.1. The Principle of BNCT
4.2. The History of BNCT
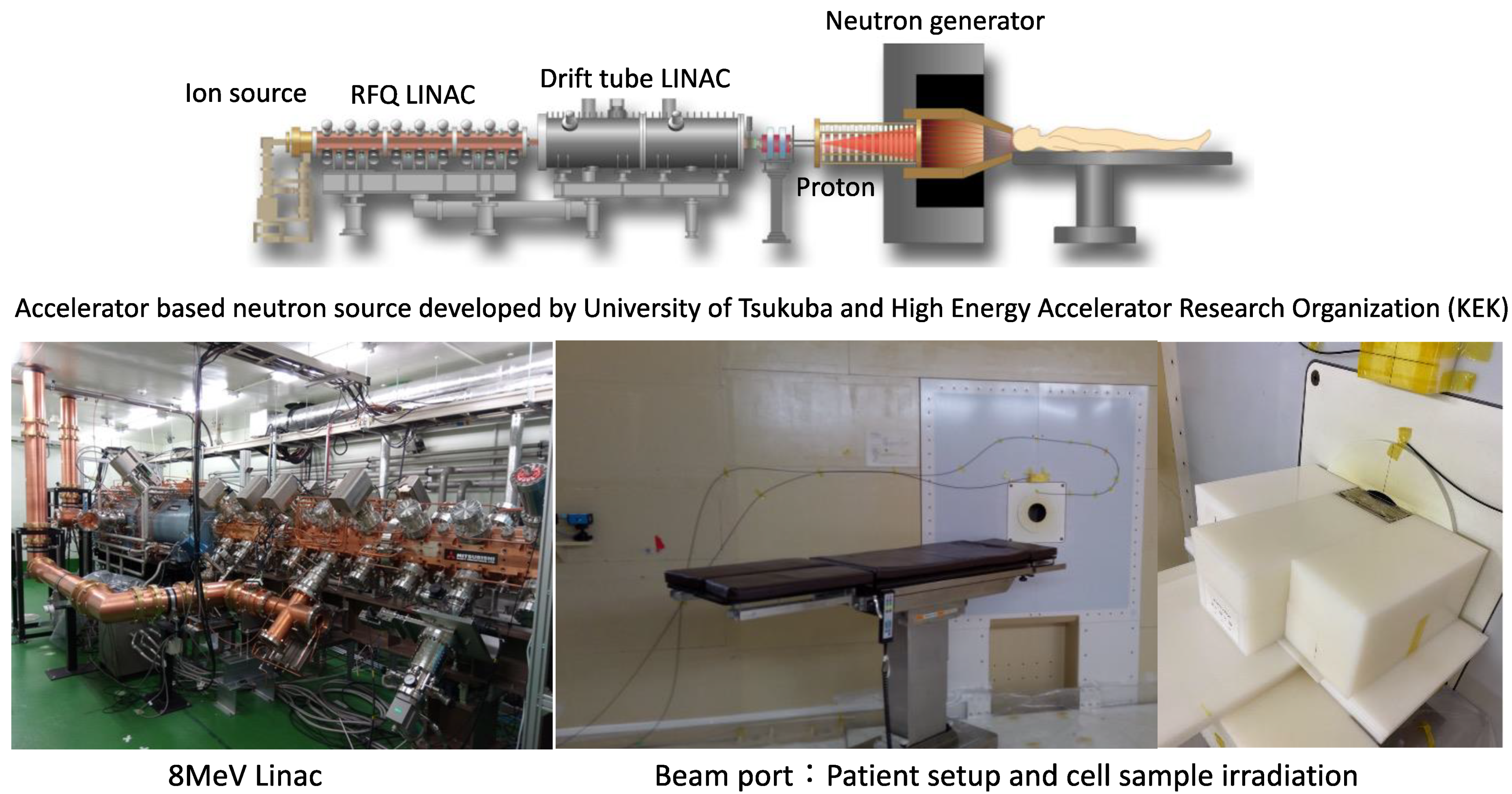
4.3. Reactor and Accelerator-Based Neutron Source
4.4. Head and Neck Cancers
4.5. Malignant Brain Tumor
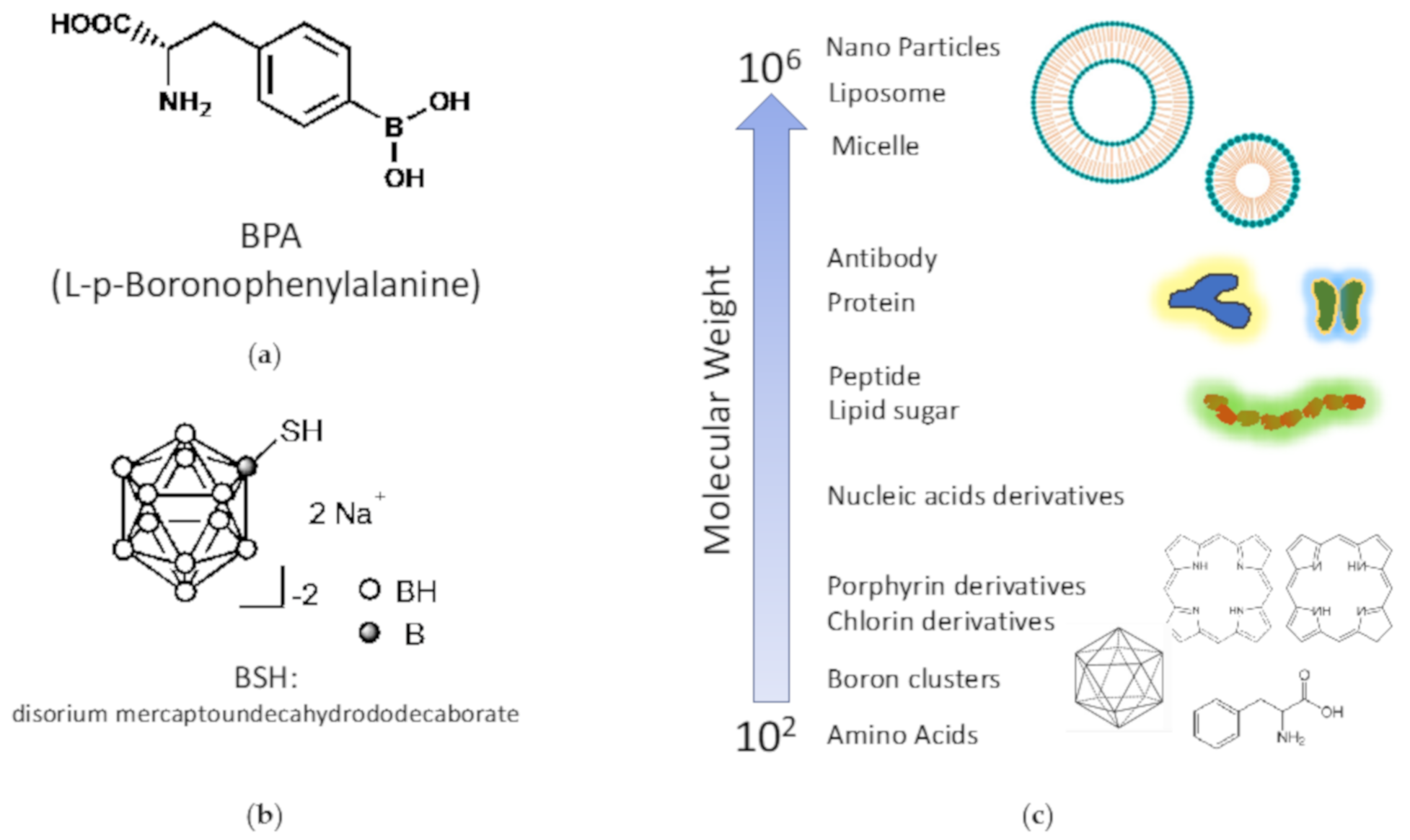
4.6. Requirements for Drugs for BNCT and Current Boron Compounds
- The concentration of 10B in the tumor tissue or cells must be at least 20 μg/mL during neutron irradiation.
- It must be safely administered and excreted.
- No toxicity is observed in bolus doses of several tens of grams.
- It must be water-soluble
- The tumor/normal tissue (T/N) ratio or tumor/blood (T/B) ratio should be as high as possible. The result is a drug with high therapeutic efficacy and reduced damage to normal tissues.
4.7. Development of New Boron Compounds
4.7.1. Problems with Existing Boron Compounds and New Drug Development
4.7.2. Drug Development Using Existing Boron Compounds
4.7.3. Development of Next-Generation Boron Drug for Fusion with Drug Delivery System Technology
4.7.4. Challenges in Conducting BNCT Research
5. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilson, R.R. Radiological use of fast protons. Radiology 1946, 47, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, J.H.; Tobias, C.A.; Born, J.L.; Mc, C.R.; Roberts, J.E.; Anger, H.O.; Low-Beer, B.V.; Huggins, C.B. Pituitary irradiation with high-energy proton beams: A preliminary report. Cancer Res. 1958, 18, 121–134. [Google Scholar]
- Particle Therapy Co-Operative Group. 2021. Available online: https://www.ptcog.ch/ (accessed on 22 July 2021).
- Suit, H.; DeLaney, T.; Goldberg, S.; Paganetti, H.; Clasie, B.; Gerweck, L.; Niemierko, A.; Hall, E.; Flanz, J.; Hallman, J.; et al. Proton vs carbon ion beams in the definitive radiation treatment of cancer patients. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2010, 95, 3–22. [Google Scholar] [CrossRef]
- Mohan, R.; Grosshans, D. Proton therapy—Present and future. Adv. Drug Deliv. Rev. 2017, 109, 26–44. [Google Scholar] [CrossRef] [Green Version]
- Lomax, A. Intensity modulation methods for proton radiotherapy. Phys. Med. Biol. 1999, 44, 185–205. [Google Scholar] [CrossRef]
- Bert, C.; Durante, M. Motion in radiotherapy: Particle therapy. Phys. Med. Biol. 2011, 56, R113–R144. [Google Scholar] [CrossRef]
- DeLaney, T.F. Proton therapy in the clinic. Front. Radiat Oncol. 2011, 43, 465–485. [Google Scholar]
- Engelsman, M.; Schwarz, M.; Dong, L. Physics controversies in proton therapy. Semin. Radiat. Oncol. 2013, 23, 88–96. [Google Scholar] [CrossRef]
- Hyer, D.E.; Hill, P.M.; Wang, D.; Smith, B.R.; Flynn, R.T. A dynamic collimation system for penumbra reduction in spot-scanning proton therapy: Proof of concept. Med. Phys. 2014, 41, 091701. [Google Scholar] [CrossRef] [Green Version]
- Schippers, J.M.; Lomax, A.J. Emerging technologies in proton therapy. Acta Oncol. 2011, 50, 838–850. [Google Scholar] [CrossRef]
- Durante, M.; Debus, J. Heavy charged particles: Does improved precision and higher biological effectiveness translate to better outcome in patients? Semin. Radiat. Oncol. 2018, 28, 160–167. [Google Scholar] [CrossRef]
- Weyrather, W.K.; Kraft, G. RBE of carbon ions: Experimental data and the strategy of RBE calculation for treatment planning. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2004, 73, S161. [Google Scholar] [CrossRef]
- Kanai, T.; Matsufuji, N.; Miyamoto, T.; Mizoe, J.; Kamada, T.; Tsuji, H.; Kato, H.; Baba, M.; Tsujii, H. Examination of GyE system for HIMAC carbon therapy. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Ando, K.; Kase, Y. Biological characteristics of carbon-ion therapy. Int. J. Radiat. Biol. 2009, 85, 715–728. [Google Scholar] [CrossRef] [PubMed]
- Furusawa, Y.; Fukutsu, K.; Aoki, M.; Itsukaichi, H.; Eguchi-Kasai, K.; Ohara, H.; Yatagai, F.; Kanai, T.; Ando, K. Inactivation of aerobic and hypoxic cells from three different cell lines by accelerated (3)He-, (12)C- and (20)Ne-ion beams. Radiat. Res. 2000, 154, 485–496. [Google Scholar] [CrossRef]
- Gray, L.H.; Green, F.O.; Hawes, C.A. Effect of nitric oxide on the radiosensitivity of tumour cells. Nature 1958, 182, 952–953. [Google Scholar] [CrossRef]
- Ito, A.; Nakano, H.; Kusano, Y.; Hirayama, R.; Furusawa, Y.; Murayama, C.; Mori, T.; Katsumura, Y.; Shinohara, K. Contribution of indirect action to radiation-induced mammalian cell inactivation: Dependence on photon energy and heavy-ion LET. Radiat. Res. 2006, 165, 703–712. [Google Scholar] [CrossRef]
- Hirayama, R.; Ito, A.; Tomita, M.; Tsukada, T.; Yatagai, F.; Noguchi, M.; Matsumoto, Y.; Kase, Y.; Ando, K.; Okayasu, R.; et al. Contributions of direct and indirect actions in cell killing by high-LET radiations. Radiat. Res. 2009, 171, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Aoki-Nakano, M.; Furusawa, Y. Misrepair of DNA double-strand breaks after exposure to heavy-ion beams causes a peak in the LET-RBE relationship with respect to cell killing in DT40 cells. J. Radiat. Res. 2013, 54, 1029–1035. [Google Scholar] [CrossRef]
- Takahashi, A.; Kubo, M.; Ma, H.; Nakagawa, A.; Yoshida, Y.; Isono, M.; Kanai, T.; Ohno, T.; Furusawa, Y.; Funayama, T.; et al. Nonhomologous end-joining repair plays a more important role than homologous recombination repair in defining radiosensitivity after exposure to high-LET radiation. Radiat. Res. 2014, 182, 338–344. [Google Scholar] [CrossRef] [Green Version]
- Blakely, E.A.; Tobias, C.A.; Yang, T.C.; Smith, K.C.; Lyman, J.T. Inactivation of human kidney cells by high-energy monoenergetic heavy-ion beams. Radiat. Res. 1979, 80, 122–160. [Google Scholar] [CrossRef] [Green Version]
- Hirayama, R.; Furusawa, Y.; Fukawa, T.; Ando, K. Repair kinetics of DNA-DSB induced by X-rays or carbon ions under oxic and hypoxic conditions. J. Radiat. Res. 2005, 46, 325–332. [Google Scholar] [CrossRef]
- Wenzl, T.; Wilkens, J.J. Theoretical analysis of the dose dependence of the oxygen enhancement ratio and its relevance for clinical applications. Radiat. Oncol. 2011, 6, 171. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Kitagawa, Y.; Uno, T.; Oyama, T.; Kato, K.; Kato, H.; Kawakubo, H.; Kawamura, O.; Kusano, M.; Kuwano, H.; Takeuchi, H.; et al. Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society: Part 1. Esophagus 2019, 16, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morota, M.; Gomi, K.; Kozuka, T.; Chin, K.; Matsuura, M.; Oguchi, M.; Ito, H.; Yamashita, T. Late toxicity after definitive concurrent chemoradiotherapy for thoracic esophageal carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.D.; Paulus, R.; Komaki, R.; Masters, G.; Blumenschein, G.; Schild, S.; Bogart, J.; Hu, C.; Forster, K.; Magliocco, A.; et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): A randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015, 16, 187–199. [Google Scholar]
- Minsky, B.D.; Pajak, T.F.; Ginsberg, R.J.; Pisansky, T.M.; Martenson, J.; Komaki, R.; Okawara, G.; Rosenthal, S.A.; Kelsen, D.P. INT 0123 (Radiation Therapy Oncology Group 94-05) phase III trial of combined-modality therapy for esophageal cancer: High-dose versus standard-dose radiation therapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2002, 20, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Muro, K.; Minashi, K.; Ohtsu, A.; Ishikura, S.; Boku, N.; Takiuchi, H.; Komatsu, Y.; Miyata, Y.; Fukuda, H.; et al. Phase II study of chemoradiotherapy with 5-fluorouracil and cisplatin for Stage II-III esophageal squamous cell carcinoma: JCOG trial (JCOG 9906). Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 684–690. [Google Scholar] [CrossRef]
- Shirai, K.; Tamaki, Y.; Kitamoto, Y.; Murata, K.; Satoh, Y.; Higuchi, K.; Nonaka, T.; Ishikawa, H.; Katoh, H.; Takahashi, T.; et al. Dose-volume histogram parameters and clinical factors associated with pleural effusion after chemoradiotherapy in esophageal cancer patients. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 1002–1007. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Liu, H.H.; Tucker, S.L.; Wang, S.; Mohan, R.; Cox, J.D.; Komaki, R.; Liao, Z. Risk factors for pericardial effusion in inoperable esophageal cancer patients treated with definitive chemoradiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Makishima, H.; Ishikawa, H.; Terunuma, T.; Hashimoto, T.; Yamanashi, K.; Sekiguchi, T.; Mizumoto, M.; Okumura, T.; Sakae, T.; Sakurai, H. Comparison of adverse effects of proton and X-ray chemoradiotherapy for esophageal cancer using an adaptive dose-volume histogram analysis. J. Radiat. Res. 2015, 56, 568–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirano, Y.; Onozawa, M.; Hojo, H.; Motegi, A.; Zenda, S.; Hotta, K.; Moriya, S.; Tachibana, H.; Nakamura, N.; Kojima, T.; et al. Dosimetric comparison between proton beam therapy and photon radiation therapy for locally advanced esophageal squamous cell carcinoma. Radiat. Oncol. 2018, 13, 23. [Google Scholar] [CrossRef] [Green Version]
- Mizumoto, M.; Sugahara, S.; Nakayama, H.; Hashii, H.; Nakahara, A.; Terashima, H.; Okumura, T.; Tsuboi, K.; Tokuuye, K.; Sakurai, H. Clinical results of proton-beam therapy for locoregionally advanced esophageal cancer. Strahlenther. Onkol. 2010, 186, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Hashimoto, T.; Moriwaki, T.; Hyodo, I.; Hisakura, K.; Terashima, H.; Ohkohchi, N.; Ohno, T.; Makishima, H.; Mizumoto, M.; et al. Proton beam therapy combined with concurrent chemotherapy for esophageal cancer. Anticancer Res. 2015, 35, 1757–1762. [Google Scholar] [CrossRef]
- Ono, T.; Wada, H.; Ishikawa, H.; Tamamura, H.; Tokumaru, S. Clinical results of proton beam therapy for esophageal cancer: Multicenter retrospective study in Japan. Cancers 2019, 11, 993. [Google Scholar] [CrossRef] [Green Version]
- DeCesaris, C.M.; Berger, M.; Choi, J.I.; Carr, S.R.; Burrows, W.M.; Regine, W.F.; Simone, C.B., 2nd; Molitoris, J.K. Pathologic complete response (pCR) rates and outcomes after neoadjuvant chemoradiotherapy with proton or photon radiation for adenocarcinomas of the esophagus and gastroesophageal junction. J. Gastrointest. Oncol. 2020, 11, 663–673. [Google Scholar] [CrossRef]
- Wang, X.; Palaskas, N.L.; Yusuf, S.W.; Abe, J.I.; Lopez-Mattei, J.; Banchs, J.; Gladish, G.W.; Lee, P.; Liao, Z.; Deswal, A.; et al. Incidence and onset of severe cardiac events after radiotherapy for esophageal cancer. J. Thorac. Oncol. 2020, 15, 1682–1690. [Google Scholar] [CrossRef]
- Wang, J.; Wei, C.; Tucker, S.L.; Myles, B.; Palmer, M.; Hofstetter, W.L.; Swisher, S.G.; Ajani, J.A.; Cox, J.D.; Komaki, R.; et al. Predictors of postoperative complications after trimodality therapy for esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 885–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xi, M.; Xu, C.; Liao, Z.; Chang, J.Y.; Gomez, D.R.; Jeter, M.; Cox, J.D.; Komaki, R.; Mehran, R.; Blum, M.A.; et al. Comparative outcomes after definitive chemoradiotherapy using proton beam therapy versus intensity modulated radiation therapy for esophageal cancer: A retrospective, single-institutional analysis. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 667–676. [Google Scholar] [CrossRef]
- Lin, S.H.; Hobbs, B.P.; Verma, V.; Tidwell, R.S.; Smith, G.L.; Lei, X.; Corsini, E.M.; Mok, I.; Wei, X.; Yao, L.; et al. Randomized phase IIB trial of proton beam therapy versus intensity-modulated radiation therapy for locally advanced esophageal cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 1569–1579. [Google Scholar] [CrossRef]
- Davuluri, R.; Jiang, W.; Fang, P.; Xu, C.; Komaki, R.; Gomez, D.R.; Welsh, J.; Cox, J.D.; Crane, C.H.; Hsu, C.C.; et al. Lymphocyte nadir and esophageal cancer survival outcomes after chemoradiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Fang, P.; Shiraishi, Y.; Verma, V.; Jiang, W.; Song, J.; Hobbs, B.P.; Lin, S.H. Lymphocyte-sparing effect of proton therapy in patients with esophageal cancer treated with definitive chemoradiation. Int. J. Part. 2018, 4, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Routman, D.M.; Garant, A.; Lester, S.C.; Day, C.N.; Harmsen, W.S.; Sanheuza, C.T.; Yoon, H.H.; Neben-Wittich, M.A.; Martenson, J.A.; Haddock, M.G.; et al. A Comparison of grade 4 lymphopenia with proton versus photon radiation therapy for esophageal cancer. Adv. Radiat. Oncol. 2019, 4, 63–69. [Google Scholar] [CrossRef] [Green Version]
- Hong, T.S.; Ryan, D.P.; Blaszkowsky, L.S.; Mamon, H.J.; Kwak, E.L.; Mino-Kenudson, M.; Adams, J.; Yeap, B.; Winrich, B.; DeLaney, T.F.; et al. Phase I study of preoperative short-course chemoradiation with proton beam therapy and capecitabine for resectable pancreatic ductal adenocarcinoma of the head. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 151–157. [Google Scholar] [CrossRef]
- Hong, T.S.; Ryan, D.P.; Borger, D.R.; Blaszkowsky, L.S.; Yeap, B.Y.; Ancukiewicz, M.; Deshpande, V.; Shinagare, S.; Wo, J.Y.; Boucher, Y.; et al. A phase 1/2 and biomarker study of preoperative short course chemoradiation with proton beam therapy and capecitabine followed by early surgery for resectable pancreatic ductal adenocarcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 830–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terashima, K.; Demizu, Y.; Hashimoto, N.; Jin, D.; Mima, M.; Fujii, O.; Niwa, Y.; Takatori, K.; Kitajima, N.; Sirakawa, S.; et al. A phase I/II study of gemcitabine-concurrent proton radiotherapy for locally advanced pancreatic cancer without distant metastasis. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2012, 103, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.H.; Lee, W.J.; Woo, S.M.; Kim, H.; Oh, E.S.; Lee, J.H.; Han, S.S.; Park, S.J.; Suh, Y.G.; Moon, S.H.; et al. Effectiveness and safety of simultaneous integrated boost-proton beam therapy for localized pancreatic cancer. Technol. Cancer Res. Treat. 2018, 17, 1533033818783879. [Google Scholar] [CrossRef]
- Jethwa, K.R.; Tryggestad, E.J.; Whitaker, T.J.; Giffey, B.T.; Kazemba, B.D.; Neben-Wittich, M.A.; Merrell, K.W.; Haddock, M.G.; Hallemeier, C.L. Initial experience with intensity modulated proton therapy for intact, clinically localized pancreas cancer: Clinical implementation, dosimetric analysis, acute treatment-related adverse events, and patient-reported outcomes. Adv. Radiat. Oncol. 2018, 3, 314–321. [Google Scholar] [CrossRef] [Green Version]
- Hiroshima, Y.; Fukumitsu, N.; Saito, T.; Numajiri, H.; Murofushi, K.N.; Ohnishi, K.; Nonaka, T.; Ishikawa, H.; Okumura, T.; Sakurai, H. Concurrent chemoradiotherapy using proton beams for unresectable locally advanced pancreatic cancer. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2019, 136, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Maemura, K.; Mataki, Y.; Kurahara, H.; Kawasaki, Y.; Iino, S.; Sakoda, M.; Ueno, S.; Arimura, T.; Higashi, R.; Yoshiura, T.; et al. Comparison of proton beam radiotherapy and hyper-fractionated accelerated chemoradiotherapy for locally advanced pancreatic cancer. Pancreatology 2017, 17, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Kawashiro, S.; Yamada, S.; Okamoto, M.; Ohno, T.; Nakano, T.; Shinoto, M.; Shioyama, Y.; Nemoto, K.; Isozaki, Y.; Tsuji, H.; et al. Multi-institutional study of carbon-ion radiotherapy for locally advanced pancreatic cancer: Japan carbon-ion radiation oncology study group (J-CROS) study 1403 pancreas. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1212–1221. [Google Scholar] [CrossRef]
- Sai, S.; Wakai, T.; Vares, G.; Yamada, S.; Kamijo, T.; Kamada, T.; Shirai, T. Combination of carbon ion beam and gemcitabine causes irreparable DNA damage and death of radioresistant pancreatic cancer stem-like cells in vitro and in vivo. Oncotarget 2015, 6, 5517–5535. [Google Scholar] [CrossRef] [Green Version]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [CrossRef] [PubMed]
- Zhan, H.X.; Xu, J.W.; Wu, D.; Wu, Z.Y.; Wang, L.; Hu, S.Y.; Zhang, G.Y. Neoadjuvant therapy in pancreatic cancer: A systematic review and meta-analysis of prospective studies. Cancer Med. 2017, 6, 1201–1219. [Google Scholar] [CrossRef]
- Blazer, M.; Wu, C.; Goldberg, R.M.; Phillips, G.; Schmidt, C.; Muscarella, P.; Wuthrick, E.; Williams, T.M.; Reardon, J.; Ellison, E.C.; et al. Neoadjuvant modified (m) FOLFIRINOX for locally advanced unresectable (LAPC) and borderline resectable (BRPC) adenocarcinoma of the pancreas. Ann. Surg. Oncol 2015, 22, 1153–1159. [Google Scholar] [CrossRef] [Green Version]
- Vitolo, V.; Cobianchi, L.; Brugnatelli, S.; Barcellini, A.; Peloso, A.; Facoetti, A.; Vanoli, A.; Delfanti, S.; Preda, L.; Molinelli, S.; et al. Preoperative chemotherapy and carbon ions therapy for treatment of resectable and borderline resectable pancreatic adenocarcinoma: A prospective, phase II, multicentre, single-arm study. BMC Cancer 2019, 19, 922. [Google Scholar] [CrossRef]
- Fukumitsu, N.; Okumura, T.; Hiroshima, Y.; Ishida, T.; Numajiri, H.; Murofushi, K.N.; Ohnishi, K.; Aihara, T.; Ishikawa, H.; Tsuboi, K.; et al. Simulation study of dosimetric effect in proton beam therapy using concomitant boost technique for unresectable pancreatic cancers. Jpn. J. Radiol. 2018, 36, 456–461. [Google Scholar] [CrossRef]
- Chuong, M.; Badiyan, S.N.; Yam, M.; Li, Z.; Langen, K.; Regine, W.; Morris, C.; Snider, J., 3rd; Mehta, M.; Huh, S.; et al. Pencil beam scanning versus passively scattered proton therapy for unresectable pancreatic cancer. J. Gastrointest. Oncol. 2018, 9, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Mori, S.; Shinoto, M.; Yamada, S. Four-dimensional treatment planning in layer-stacking boost irradiation for carbon-ion pancreatic therapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2014, 111, 258–263. [Google Scholar] [CrossRef]
- Cancer Registry and Statistics; Cancer Information Service, National Cancer Center: Tokyo, Japan, 2021; (Vital Statistics of Japan).
- Fowler, J.F.; Ritter, M.A.; Chappell, R.J.; Brenner, D.J. What hypofractionated protocols should be tested for prostate cancer? Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 1093–1104. [Google Scholar] [CrossRef]
- Michalski, J.M.; Yan, Y.; Watkins-Bruner, D.; Bosch, W.R.; Winter, K.; Galvin, J.M.; Bahary, J.P.; Morton, G.C.; Parliament, M.B.; Sandler, H.M. Preliminary toxicity analysis of 3-dimensional conformal radiation therapy versus intensity modulated radiation therapy on the high-dose arm of the Radiation Therapy Oncology Group 0126 prostate cancer trial. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 932–938. [Google Scholar] [CrossRef] [Green Version]
- Fellin, G.; Mirri, M.A.; Santoro, L.; Jereczek-Fossa, B.A.; Divan, C.; Mussari, S.; Ziglio, F.; La Face, B.; Barbera, F.; Buglione, M.; et al. Low dose rate brachytherapy (LDR-BT) as monotherapy for early stage prostate cancer in Italy: Practice and outcome analysis in a series of 2237 patients from 11 institutions. Br. J. Radiol. 2016, 89, 20150981. [Google Scholar] [CrossRef] [PubMed]
- Shipley, W.U.; Verhey, L.J.; Munzenrider, J.E.; Suit, H.D.; Urie, M.M.; McManus, P.L.; Young, R.H.; Shipley, J.W.; Zietman, A.L.; Biggs, P.J.; et al. Advanced prostate cancer: The results of a randomized comparative trial of high dose irradiation boosting with conformal protons compared with conventional dose irradiation using photons alone. Int. J. Radiat. Oncol. Biol. Phys. 1995, 32, 3–12. [Google Scholar] [CrossRef]
- Roach, M., 3rd; DeSilvio, M.; Valicenti, R.; Grignon, D.; Asbell, S.O.; Lawton, C.; Thomas, C.R., Jr.; Shipley, W.U. Whole-pelvis, “mini-pelvis”, or prostate-only external beam radiotherapy after neoadjuvant and concurrent hormonal therapy in patients treated in the Radiation Therapy Oncology Group 9413 trial. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Zietman, A.L.; Bae, K.; Slater, J.D.; Shipley, W.U.; Efstathiou, J.A.; Coen, J.J.; Bush, D.A.; Lunt, M.; Spiegel, D.Y.; Skowronski, R.; et al. Randomized trial comparing conventional-dose with high-dose conformal radiation therapy in early-stage adenocarcinoma of the prostate: Long-term results from proton radiation oncology group/american college of radiology 95-09. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 1106–1111. [Google Scholar] [CrossRef] [Green Version]
- Kuban, D.A.; Tucker, S.L.; Dong, L.; Starkschall, G.; Huang, E.H.; Cheung, M.R.; Lee, A.K.; Pollack, A. Long-term results of the M. D. Anderson randomized dose-escalation trial for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 67–74. [Google Scholar] [CrossRef]
- D’Amico, A.V.; Manola, J.; Loffredo, M.; Renshaw, A.A.; DellaCroce, A.; Kantoff, P.W. 6-month androgen suppression plus radiation therapy vs radiation therapy alone for patients with clinically localized prostate cancer: A randomized controlled trial. JAMA 2004, 292, 821–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulte, R.W.; Slater, J.D.; Rossi, C.J., Jr.; Slater, J.M. Value and perspectives of proton radiation therapy for limited stage prostate cancer. Strahlenther. Onkol. 2000, 176, 3–8. [Google Scholar] [CrossRef]
- Ishikawa, H.; Tsuji, H.; Kamada, T.; Akakura, K.; Suzuki, H.; Shimazaki, J.; Tsujii, H.; Working Group for Genitourinary Tumors. Carbon-ion radiation therapy for prostate cancer. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2012, 19, 296–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murakami, M.; Ishikawa, H.; Shimizu, S.; Iwata, H.; Okimoto, T.; Takagi, M.; Murayama, S.; Akimoto, T.; Wada, H.; Arimura, T.; et al. Optimal androgen deprivation therapy combined with proton beam therapy for prostate cancer: Results from a multi-institutional study of the japanese radiation oncology study group. Cancers 2020, 12, 1690. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.E.; Hawley, J.; Levy, W.; Gooley, T.; Buckner, C.D.; Deeg, H.J.; Doney, K.; Storb, R.; Sullivan, K.; Witherspoon, R.; et al. Pregnancies following high-dose cyclophosphamide with or without high-dose busulfan or total-body irradiation and bone marrow transplantation. Blood 1996, 87, 3045–3052. [Google Scholar] [CrossRef]
- Green, D.M.; Whitton, J.A.; Stovall, M.; Mertens, A.C.; Donaldson, S.S.; Ruymann, F.B.; Pendergrass, T.W.; Robison, L.L. Pregnancy outcome of female survivors of childhood cancer: A report from the childhood cancer survivor study. Am. J. Obs. Gynecol. 2002, 187, 1070–1080. [Google Scholar] [CrossRef] [PubMed]
- Mertens, A.C.; Liu, Q.; Neglia, J.P.; Wasilewski, K.; Leisenring, W.; Armstrong, G.T.; Robison, L.L.; Yasui, Y. Cause-specific late mortality among 5-year survivors of childhood cancer: The Childhood Cancer Survivor Study. J. Natl. Cancer Inst. 2008, 100, 1368–1379. [Google Scholar] [CrossRef]
- Eaton, B.R.; Esiashvili, N.; Kim, S.; Weyman, E.A.; Thornton, L.T.; Mazewski, C.; MacDonald, T.; Ebb, D.; MacDonald, S.M.; Tarbell, N.J.; et al. Clinical Outcomes among children with standard-risk medulloblastoma treated with proton and photon radiation therapy: A comparison of disease control and overall survival. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 133–138. [Google Scholar] [CrossRef] [Green Version]
- Eaton, B.R.; Esiashvili, N.; Kim, S.; Patterson, B.; Weyman, E.A.; Thornton, L.T.; Mazewski, C.; MacDonald, T.J.; Ebb, D.; MacDonald, S.M.; et al. Endocrine outcomes with proton and photon radiotherapy for standard risk medulloblastoma. Neuro-Oncol. 2016, 18, 881–887. [Google Scholar] [CrossRef] [Green Version]
- Cotter, S.E.; Herrup, D.A.; Friedmann, A.; Macdonald, S.M.; Pieretti, R.V.; Robinson, G.; Adams, J.; Tarbell, N.J.; Yock, T.I. Proton radiotherapy for pediatric bladder/prostate rhabdomyosarcoma: Clinical outcomes and dosimetry compared to intensity-modulated radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 1367–1373. [Google Scholar] [CrossRef] [PubMed]
- Ladra, M.M.; Szymonifka, J.D.; Mahajan, A.; Friedmann, A.M.; Yong Yeap, B.; Goebel, C.P.; MacDonald, S.M.; Grosshans, D.R.; Rodriguez-Galindo, C.; Marcus, K.J.; et al. Preliminary results of a phase II trial of proton radiotherapy for pediatric rhabdomyosarcoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 3762–3770. [Google Scholar] [CrossRef] [Green Version]
- Weber, D.C.; Ares, C.; Albertini, F.; Frei-Welte, M.; Niggli, F.K.; Schneider, R.; Lomax, A.J. Pencil beam scanning proton therapy for pediatric parameningeal rhabdomyosarcomas: Clinical outcome of patients treated at the paul scherrer institute. Pediatr. Blood Cancer 2016, 63, 1731–1736. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, M.; Murayama, S.; Akimoto, T.; Demizu, Y.; Fukushima, T.; Ishida, Y.; Oshiro, Y.; Numajiri, H.; Fuji, H.; Okumura, T.; et al. Preliminary results of proton radiotherapy for pediatric rhabdomyosarcoma: A multi-institutional study in Japan. Cancer Med. 2018, 7, 1870–1874. [Google Scholar] [CrossRef] [Green Version]
- Pignon, J.P.; Bourhis, J.; Domenge, C.; Designe, L. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: Three meta-analyses of updated individual data. MACH-NC Collaborative Group. Meta-Analysis of Chemotherapy on Head and Neck Cancer. Lancet 2000, 355, 949–955. [Google Scholar] [CrossRef]
- Schlaich, F.; Brons, S.; Haberer, T.; Debus, J.; Combs, S.E.; Weber, K.J. Comparison of the effects of photon versus carbon ion irradiation when combined with chemotherapy in vitro. Radiat. Oncol. 2013, 8, 260. [Google Scholar] [CrossRef] [Green Version]
- Harrabi, S.; Combs, S.E.; Brons, S.; Haberer, T.; Debus, J.; Weber, K.J. Temozolomide in combination with carbon ion or photon irradiation in glioblastoma multiforme cell lines—Does scheduling matter? Int. J. Radiat. Biol. 2013, 89, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Harrabi, S.B.; Adeberg, S.; Winter, M.; Haberer, T.; Debus, J.; Weber, K.J. S-phase-specific radiosensitization by gemcitabine for therapeutic carbon ion exposure in vitro. J. Radiat. Res. 2016, 57, 110–114. [Google Scholar] [CrossRef] [Green Version]
- Carter, R.J.; Nickson, C.M.; Thompson, J.M.; Kacperek, A.; Hill, M.A.; Parsons, J.L. Complex DNA damage induced by high linear energy transfer alpha-particles and protons triggers a specific cellular DNA damage response. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 776–784. [Google Scholar] [CrossRef] [Green Version]
- Luhr, A.; von Neubeck, C.; Krause, M.; Troost, E.G.C. Relative biological effectiveness in proton beam therapy—Current knowledge and future challenges. Clin. Transl. Radiat. Oncol. 2018, 9, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Grosse, N.; Fontana, A.O.; Hug, E.B.; Lomax, A.; Coray, A.; Augsburger, M.; Paganetti, H.; Sartori, A.A.; Pruschy, M. Deficiency in homologous recombination renders Mammalian cells more sensitive to proton versus photon irradiation. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 175–181. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Ando, K.; Kato, T.A.; Sekino, Y.; Ishikawa, H.; Sakae, T.; Tsuboi, K.; Sakurai, H. Difference in degree of sub-lethal damage recovery between clinical proton beams and X-Rays. Radiat. Prot. Dosim. 2019, 183, 93–97. [Google Scholar] [CrossRef]
- Iwata, H.; Shuto, T.; Kamei, S.; Omachi, K.; Moriuchi, M.; Omachi, C.; Toshito, T.; Hashimoto, S.; Nakajima, K.; Sugie, C.; et al. Combined effects of cisplatin and photon or proton irradiation in cultured cells: Radiosensitization, patterns of cell death and cell cycle distribution. J. Radiat. Res. 2020, 61, 832–841. [Google Scholar] [CrossRef]
- Krause, M.; Zips, D.; Thames, H.D.; Kummermehr, J.; Baumann, M. Preclinical evaluation of molecular-targeted anticancer agents for radiotherapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2006, 80, 112–122. [Google Scholar] [CrossRef]
- Chae, Y.K.; Pan, A.P.; Davis, A.A.; Patel, S.P.; Carneiro, B.A.; Kurzrock, R.; Giles, F.J. Path toward precision oncology: Review of targeted therapy studies and tools to aid in defining “actionability” of a molecular lesion and patient management support. Mol. Cancer 2017, 16, 2645–2655. [Google Scholar] [CrossRef] [Green Version]
- Falzone, L.; Salomone, S.; Libra, M. Evolution of cancer pharmacological treatments at the turn of the third millennium. Front. Pharm. 2018, 9, 1300. [Google Scholar] [CrossRef] [Green Version]
- Koricanac, L.B.; Zakula, J.J.; Petrovic, I.M.; Valastro, L.M.; Cirrone, G.A.; Cuttone, G.; Ristic-Fira, A.M. Anti-tumour activity of fotemustine and protons in combination with bevacizumab. Chemotherapy 2010, 56, 214–222. [Google Scholar] [CrossRef]
- Park, H.J.; Oh, J.S.; Chang, J.W.; Hwang, S.G.; Kim, J.S. Proton irradiation sensitizes radioresistant non-small cell lung cancer cells by modulating epidermal growth factor receptor-mediated DNA repair. Anticancer. Res. 2016, 36, 205–212. [Google Scholar]
- Moncharmont, C.; Guy, J.B.; Wozny, A.S.; Gilormini, M.; Battiston-Montagne, P.; Ardail, D.; Beuve, M.; Alphonse, G.; Simoens, X.; Rancoule, C.; et al. Carbon ion irradiation withstands cancer stem cells’ migration/invasion process in Head and Neck Squamous Cell Carcinoma (HNSCC). Oncotarget 2016, 7, 47738–47749. [Google Scholar] [CrossRef] [Green Version]
- Hirai, T.; Saito, S.; Fujimori, H.; Matsushita, K.; Nishio, T.; Okayasu, R.; Masutani, M. Radiosensitization by PARP inhibition to proton beam irradiation in cancer cells. Biochem. Biophys. Res. Commun. 2016, 478, 234–240. [Google Scholar] [CrossRef]
- Wera, A.C.; Lobbens, A.; Stoyanov, M.; Lucas, S.; Michiels, C. Radiation-induced synthetic lethality: Combination of poly(ADP-ribose) polymerase and RAD51 inhibitors to sensitize cells to proton irradiation. Cell Cycle 2019, 18, 1770–1783. [Google Scholar] [CrossRef]
- Kageyama, S.I.; Junyan, D.; Hojo, H.; Motegi, A.; Nakamura, M.; Tsuchihara, K.; Akimoto, T. PARP inhibitor olaparib sensitizes esophageal carcinoma cells to fractionated proton irradiation. J. Radiat. Res. 2020, 61, 177–186. [Google Scholar] [CrossRef]
- Wang, L.; Cao, J.; Wang, X.; Lin, E.; Wang, Z.; Li, Y.; Li, Y.; Chen, M.; Wang, X.; Jiang, B.; et al. Proton and photon radiosensitization effects of niraparib, a PARP-1/-2 inhibitor, on human head and neck cancer cells. Head Neck 2020, 42, 2244–2256. [Google Scholar] [CrossRef]
- Hirai, T.; Shirai, H.; Fujimori, H.; Okayasu, R.; Sasai, K.; Masutani, M. Radiosensitization effect of poly(ADP-ribose) polymerase inhibition in cells exposed to low and high liner energy transfer radiation. Cancer Sci. 2012, 103, 1045–1050. [Google Scholar] [CrossRef] [PubMed]
- Lesueur, P.; Chevalier, F.; El-Habr, E.A.; Junier, M.P.; Chneiweiss, H.; Castera, L.; Muller, E.; Stefan, D.; Saintigny, Y. Radiosensitization effect of talazoparib, a parp inhibitor, on glioblastoma stem cells exposed to low and high linear energy transfer radiation. Sci. Rep. 2018, 8, 3664. [Google Scholar] [CrossRef] [PubMed]
- Hirakawa, H.; Fujisawa, H.; Masaoka, A.; Noguchi, M.; Hirayama, R.; Takahashi, M.; Fujimori, A.; Okayasu, R. The combination of Hsp90 inhibitor 17AAG and heavy-ion irradiation provides effective tumor control in human lung cancer cells. Cancer Med. 2015, 4, 426–436. [Google Scholar] [CrossRef]
- Li, H.K.; Matsumoto, Y.; Furusawa, Y.; Kamada, T. PU-H71, a novel Hsp90 inhibitor, as a potential cancer-specific sensitizer to carbon-ion beam therapy. J. Radiat. Res. 2016, 57, 572–575. [Google Scholar] [CrossRef]
- Yu, J.I.; Choi, C.; Shin, S.W.; Son, A.; Lee, G.H.; Kim, S.Y.; Park, H.C. Valproic acid sensitizes hepatocellular carcinoma cells to proton therapy by suppressing NRF2 activation. Sci. Rep. 2017, 7, 14986. [Google Scholar] [CrossRef] [PubMed]
- Gerelchuluun, A.; Maeda, J.; Manabe, E.; Brents, C.A.; Sakae, T.; Fujimori, A.; Chen, D.J.; Tsuboi, K.; Kato, T.A. Histone deacetylase inhibitor induced radiation sensitization effects on human cancer cells after photon and hadron radiation exposure. Int. J. Mol. Sci. 2018, 19, 496. [Google Scholar] [CrossRef] [Green Version]
- Rosa, S.; Connolly, C.; Schettino, G.; Butterworth, K.T.; Prise, K.M. Biological mechanisms of gold nanoparticle radiosensitization. Cancer Nanotechnol. 2017, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Mu, X.; He, H.; Zhang, X.D. Cancer radiosensitizers. Trends Pharm. Sci. 2018, 39, 24–48. [Google Scholar] [CrossRef]
- Klebowski, B.; Depciuch, J.; Parlinska-Wojtan, M.; Baran, J. Applications of noble metal-based nanoparticles in medicine. Int. J. Mol. Sci. 2018, 19, 4031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeremic, B.; Aguerri, A.R.; Filipovic, N. Radiosensitization by gold nanoparticles. Clin. Transl. Oncol. 2013, 15, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Schuemann, J.; Bagley, A.F.; Berbeco, R.; Bromma, K.; Butterworth, K.T.; Byrne, H.L.; Chithrani, B.D.; Cho, S.H.; Cook, J.R.; Favaudon, V.; et al. Roadmap for metal nanoparticles in radiation therapy: Current status, translational challenges, and future directions. Phys. Med. Biol. 2020, 65, 21RM02. [Google Scholar] [CrossRef]
- Peukert, D.; Kempson, I.; Douglass, M.; Bezak, E. Metallic nanoparticle radiosensitisation of ion radiotherapy: A review. Phys. Med. 2018, 47, 121–128. [Google Scholar] [CrossRef]
- Lacombe, S.; Porcel, E.; Scifoni, E. Particle therapy and nanomedicine: State of art and research perspectives. Cancer Nanotechnol. 2017, 8, 9. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Fujisawa, N.; Takanohashi, M.; Najmina, M.; Uto, K.; Ebara, M. A smart hyperthermia nanofiber-platform-enabled sustained release of doxorubicin and 17AAG for synergistic cancer therapy. Int. J. Mol. Sci. 2021, 22, 2542. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Wu, Z.; Yang, H.; Guo, S.; Li, D.; Cheng, L. In vitro and in vivo evaluation of injectable implants for intratumoral delivery of 5-fluorouracil. Pharm. Dev. Technol. 2014, 19, 223–231. [Google Scholar] [CrossRef]
- Kim, Y.J.; Ebara, M.; Aoyagi, T. Temperature-responsive electrospun nanofibers for ‘on-off’ switchable release of dextran. Sci. Technol. Adv. Mater. 2012, 13, 064203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Kotsuchibashi, Y.; Liu, Y.; Narain, R. Study of bacterial adhesion on biomimetic temperature responsive glycopolymer surfaces. ACS Appl. Mater. Interfaces 2015, 7, 1652–1661. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Kotsuchibashi, Y.; Uto, K.; Ebara, M.; Aoyagi, T.; Liu, Y.; Narain, R. pH and glucose responsive nanofibers for the reversible capture and release of lectins. Biomater. Sci. 2015, 3, 152–162. [Google Scholar] [CrossRef]
- Okada, T.; Niiyama, E.; Uto, K.; Aoyagi, T.; Ebara, M. Inactivated sendai virus (HVJ-E) immobilized electrospun nanofiber for cancer therapy. Materials 2015, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, K.; Tanaka, H.; Ebara, M.; Uto, K.; Matsuoka, H.; Nishimoto, S.; Okada, K.; Murase, T.; Yoshikawa, H. Electrospun nanofiber sheets incorporating methylcobalamin promote nerve regeneration and functional recovery in a rat sciatic nerve crush injury model. Acta Biomater. 2017, 53, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Niiyama, E.; Uto, K.; Lee, C.M.; Sakura, K.; Ebara, M. Hyperthermia nanofiber platform synergized by sustained release of paclitaxel to improve antitumor efficiency. Adv. Healthc Mater. 2019, 8, e1900102. [Google Scholar] [CrossRef]
- Niiyama, E.; Uto, K.; Lee, C.M.; Sakura, K.; Ebara, M. Alternating magnetic field-triggered switchable nanofiber mesh for cancer thermo-chemotherapy. Polymers 2018, 10, 1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujisawa, N.; Takanohashi, M.; Chen, L.; Uto, K.; Matsumoto, Y.; Takeuchi, M.; Ebara, M. A Diels-Alder polymer platform for thermally enhanced drug release toward efficient local cancer chemotherapy. Sci. Technol. Adv. Mater. 2021, 22, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Formenti, S.C.; Demaria, S. Systemic effects of local radiotherapy. Lancet Oncol. 2009, 10, 718–726. [Google Scholar] [CrossRef] [Green Version]
- Haikerwal, S.J.; Hagekyriakou, J.; MacManus, M.; Martin, O.A.; Haynes, N.M. Building immunity to cancer with radiation therapy. Cancer Lett 2015, 368, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Scheithauer, H.; Belka, C.; Lauber, K.; Gaipl, U.S. Immunological aspects of radiotherapy. Radiat. Oncol. 2014, 9, 185. [Google Scholar] [CrossRef] [Green Version]
- Galluzzi, L.; Buque, A.; Kepp, O.; Zitvogel, L.; Kroemer, G. Immunogenic cell death in cancer and infectious disease. Nat. Rev. Immunol. 2017, 17, 97–111. [Google Scholar] [CrossRef]
- Grass, G.D.; Krishna, N.; Kim, S. The immune mechanisms of abscopal effect in radiation therapy. Curr. Probl. Cancer 2016, 40, 10–24. [Google Scholar] [CrossRef]
- Girdhani, S.; Lamont, C.; Hahnfeldt, P.; Abdollahi, A.; Hlatky, L. Proton irradiation suppresses angiogenic genes and impairs cell invasion and tumor growth. Radiat. Res. 2012, 178, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, S.R.; Malamas, A.S.; Bernstein, M.B.; Tsang, K.Y.; Vassantachart, A.; Sahoo, N.; Tailor, R.; Pidikiti, R.; Guha, C.P.; Hahn, S.M.; et al. Tumor cells surviving exposure to proton or photon radiation share a common immunogenic modulation signature, rendering them more sensitive to T cell-mediated killing. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 120–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girdhani, S.; Sachs, R.; Hlatky, L. Biological effects of proton radiation: What we know and don’t know. Radiat. Res. 2013, 179, 257–272. [Google Scholar] [CrossRef] [PubMed]
- Ando, K.; Fujita, H.; Hosoi, A.; Ma, L.; Wakatsuki, M.; Seino, K.I.; Kakimi, K.; Imai, T.; Shimokawa, T.; Nakano, T. Intravenous dendritic cell administration enhances suppression of lung metastasis induced by carbon-ion irradiation. J. Radiat. Res. 2017, 58, 446–455. [Google Scholar] [CrossRef] [Green Version]
- Ogata, T.; Teshima, T.; Kagawa, K.; Hishikawa, Y.; Takahashi, Y.; Kawaguchi, A.; Suzumoto, Y.; Nojima, K.; Furusawa, Y.; Matsuura, N. Particle irradiation suppresses metastatic potential of cancer cells. Cancer Res. 2005, 65, 113–120. [Google Scholar] [PubMed]
- Ohkubo, Y.; Iwakawa, M.; Seino, K.; Nakawatari, M.; Wada, H.; Kamijuku, H.; Nakamura, E.; Nakano, T.; Imai, T. Combining carbon ion radiotherapy and local injection of alpha-galactosylceramide-pulsed dendritic cells inhibits lung metastases in an in vivo murine model. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1524–1531. [Google Scholar] [CrossRef]
- Durante, M.; Brenner, D.J.; Formenti, S.C. Does heavy ion therapy work through the immune system? Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 934–936. [Google Scholar] [CrossRef] [PubMed]
- Durante, M.; Reppingen, N.; Held, K.D. Immunologically augmented cancer treatment using modern radiotherapy. Trends Mol. Med. 2013, 19, 565–582. [Google Scholar] [CrossRef]
- Abei, M.; Okumura, T.; Fukuda, K.; Hashimoto, T.; Araki, M.; Ishige, K.; Hyodo, I.; Kanemoto, A.; Numajiri, H.; Mizumoto, M.; et al. A phase I study on combined therapy with proton-beam radiotherapy and in situ tumor vaccination for locally advanced recurrent hepatocellular carcinoma. Radiat. Oncol. 2013, 8, 239. [Google Scholar] [CrossRef] [Green Version]
- Taylor, H.J.; Goldhaber, M. Detection of nuclear disintegration in a photographic emulsion. Nature 1935, 135, 341. [Google Scholar] [CrossRef]
- GL, L. Biological effects and therapeutic possiblilities of neutron. Am. J. Roentgenol. 1936, 36, 1–13. [Google Scholar]
- Farr, L.E.; Sweet, W.H.; Robertson, J.S.; Foster, C.G.; Locksley, H.B.; Sutherland, D.L.; Mendelsohn, M.L.; Stickley, E.E. Neutron capture therapy with boron in the treatment of glioblastoma multiforme. Am. J. Roentgenol. Radium Nucl. Med. 1954, 71, 279–293. [Google Scholar]
- Slatkin, D.N. A history of boron neutron capture therapy of brain tumours. Postulation of a brain radiation dose tolerance limit. Brain 1991, 114, 1609–1629. [Google Scholar] [CrossRef] [PubMed]
- Sweet, W.H. Early history of development of boron neutron capture therapy of tumors. J. Neurooncol. 1997, 33, 19–26. [Google Scholar] [CrossRef]
- Hatanaka, H.; Nakagawa, Y. Clinical results of long-surviving brain tumor patients who underwent boron neutron capture therapy. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 1061–1066. [Google Scholar] [CrossRef]
- Mishima, Y.; Honda, C.; Ichihashi, M.; Obara, H.; Hiratsuka, J.; Fukuda, H.; Karashima, H.; Kobayashi, T.; Kanda, K.; Yoshino, K. Treatment of malignant melanoma by single thermal neutron capture therapy with melanoma-seeking 10B-compound. Lancet 1989, 2, 388–389. [Google Scholar] [CrossRef]
- Sauerwein, W.; Zurlo, A.; Group, E.B.N.C.T. The EORTC Boron Neutron Capture Therapy (BNCT) Group: Achievements and future projects. Eur. J. Cancer 2002, 38, S31–S34. [Google Scholar] [CrossRef]
- Wittig, A.; Moss, R.L.; Stecher-Rasmussen, F.; Appelman, K.; Rassow, J.; Roca, A.; Sauerwein, W. Neutron activation of patients following boron neutron capture therapy of brain tumors at the high flux reactor (HFR) Petten (EORTC Trials 11961 and 11011). Strahlenther. Onkol. 2005, 181, 774–782. [Google Scholar] [CrossRef]
- Sakamoto, S.; Kiger, W.S., 3rd; Harling, O.K. Sensitivity studies of beam directionality, beam size, and neutron spectrum for a fission converter-based epithermal neutron beam for boron neutron capture therapy. Med. Phys. 1999, 26, 1979–1988. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Kanda, K.; Ujeno, Y.; Ishida, M.R. Biomedical irradiation system for boron neutron capture therapy at the Kyoto University Reactor. Basic Life Sci. 1990, 54, 321–339. [Google Scholar]
- Auterinen, I.; Kotiluoto, P.; Hippelainen, E.; Kortesniemi, M.; Seppala, T.; Seren, T.; Mannila, V.; Poyry, P.; Kankaanranta, L.; Collan, J.; et al. Design and construction of shoulder recesses into the beam aperture shields for improved patient positioning at the FiR 1 BNCT facility. Appl. Radiat. Isot. 2004, 61, 799–803. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Horiguchi, H.; Kishi, T.; Motohashi, J.; Sasajima, F.; Kumada, H. Resumption of JRR-4 and characteristics of neutron beam for BNCT. Appl. Radiat. Isot. 2011, 69, 1932–1935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.K.; Blue, T.E.; Gahbauer, R.A. A design study of an accelerator-based epithermal neutron source for boron neutron capture therapy. Strahlenther. Onkol. 1989, 165, 75–78. [Google Scholar] [PubMed]
- Kreiner, A.J.; Baldo, M.; Bergueiro, J.R.; Cartelli, D.; Castell, W.; Thatar Vento, V.; Gomez Asoia, J.; Mercuri, D.; Padulo, J.; Suarez Sandin, J.C.; et al. Accelerator-based BNCT. Appl. Radiat. Isot. 2014, 88, 185–189. [Google Scholar] [CrossRef] [Green Version]
- Kumada, H.; Kurihara, T.; Yoshioka, M.; Kobayashi, H.; Matsumoto, H.; Sugano, T.; Sakurai, H.; Sakae, T.; Matsumura, A. development of beryllium-based neutron target system with three-layer structure for accelerator-based neutron source for boron neutron capture therapy. Appl. Radiat. Isot. 2015, 106, 78–83. [Google Scholar] [CrossRef]
- Taskaev, S.; Berendeev, E.; Bikchurina, M.; Bykov, T.; Kasatov, D.; Kolesnikov, I.; Koshkarev, A.; Makarov, A.; Ostreinov, G.; Porosev, V.; et al. Neutron source based on vacuum insulated tandem accelerator and lithium target. Biology 2021, 10, 350. [Google Scholar]
- Hirose, K.; Konno, A.; Hiratsuka, J.; Yoshimoto, S.; Kato, T.; Ono, K.; Otsuki, N.; Hatazawa, J.; Tanaka, H.; Takayama, K.; et al. Boron neutron capture therapy using cyclotron-based epithermal neutron source and borofalan ((10)B) for recurrent or locally advanced head and neck cancer (JHN002): An open-label phase II trial. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2021, 155, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Kanno, H.; Nagata, H.; Ishiguro, A.; Tsuzuranuki, S.; Nakano, S.; Nonaka, T.; Kiyohara, K.; Kimura, T.; Sugawara, A.; Okazaki, Y.; et al. Designation products: Boron neutron capture therapy for head and neck carcinoma. Oncologist 2021, 26, e1250–e1255. [Google Scholar] [CrossRef] [PubMed]
- Miyatake, S.I.; Wanibuchi, M.; Hu, N.; Ono, K. Boron neutron capture therapy for malignant brain tumors. J. Neurooncol. 2020, 149, 1–11. [Google Scholar] [CrossRef]
- Provenzano, L.; Koivunoro, H.; Postuma, I.; Longhino, J.M.; Boggio, E.F.; Farias, R.O.; Bortolussi, S.; Gonzalez, S.J. The essential role of radiobiological figures of merit for the assessment and comparison of beam performances in boron neutron capture therapy. Phys. Med. 2019, 67, 9–19. [Google Scholar] [CrossRef]
- Lee, P.Y.; Tang, X.; Geng, C.; Liu, Y.H. A bi-tapered and air-gapped beam shaping assembly used for AB-BNCT. Appl. Radiat. Isot. 2021, 167, 109392. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Matsumura, A.; Yamamoto, K.; Kumada, H.; Shibata, Y.; Nose, T. In-phantom two-dimensional thermal neutron distribution for intraoperative boron neutron capture therapy of brain tumours. Phys. Med. Biol. 2002, 47, 2387–2396. [Google Scholar] [CrossRef]
- Kumada, H.; Yamamoto, K.; Matsumura, A.; Yamamoto, T.; Nakagawa, Y.; Nakai, K.; Kageji, T. Verification of the computational dosimetry system in JAERI (JCDS) for boron neutron capture therapy. Phys. Med. Biol. 2004, 49, 3353–3365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wojnecki, C.; Green, S. A preliminary comparative study of two treatment planning systems developed for boron neutron capture therapy: MacNCTPlan and SERA. Med. Phys. 2002, 29, 1710–1715. [Google Scholar] [CrossRef]
- Koivunoro, H.; Kumada, H.; Seppala, T.; Kotiluoto, P.; Auterinen, I.; Kankaanranta, L.; Savolainen, S. Comparative study of dose calculations with SERA and JCDS treatment planning systems. Appl. Radiat. Isot. 2009, 67, S126–S129. [Google Scholar] [CrossRef]
- Li, H.S.; Liu, Y.W.; Lee, C.Y.; Lin, T.Y.; Hsu, F.Y. Verification of the accuracy of BNCT treatment planning system THORplan. Appl. Radiat. Isot. 2009, 67, S122–S125. [Google Scholar] [CrossRef] [PubMed]
- Kumada, H.; Yamamoto, K.; Yamamoto, T.; Nakai, K.; Nakagawa, Y.; Kageji, T.; Matsumura, A. Improvement of dose calculation accuracy for BNCT dosimetry by the multi-voxel method in JCDS. Appl. Radiat. Isot. 2004, 61, 1045–1050. [Google Scholar] [CrossRef]
- Nakagawa, Y.; Pooh, K.; Kobayashi, T.; Kageji, T.; Uyama, S.; Matsumura, A.; Kumada, H. Clinical review of the Japanese experience with boron neutron capture therapy and a proposed strategy using epithermal neutron beams. J. Neurooncol. 2003, 62, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Yoshihashi, S.; Ishikawa, A.; Honda, S.; Yamazaki, A.; Tsurita, Y.; Uritani, A.; Tsuchida, K.; Kiyanagi, Y. First experimental verification of the neutron field of Nagoya University Accelerator-driven neutron source for boron neutron capture therapy. Appl. Radiat. Isot. 2021, 168, 109553. [Google Scholar] [CrossRef]
- Nakamura, S.; Igaki, H.; Ito, M.; Imamichi, S.; Kashihara, T.; Okamoto, H.; Nishioka, S.; Iijima, K.; Chiba, T.; Nakayama, H.; et al. Neutron flux evaluation model provided in the accelerator-based boron neutron capture therapy system employing a solid-state lithium target. Sci. Rep. 2021, 11, 8090. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.; Ono, K.; Sakurai, Y.; Ohmae, M.; Maruhashi, A.; Imahori, Y.; Kirihata, M.; Nakazawa, M.; Yura, Y. Effectiveness of BNCT for recurrent head and neck malignancies. Appl. Radiat. Isot. 2004, 61, 1069–1073. [Google Scholar] [CrossRef]
- Kato, I.; Fujita, Y.; Maruhashi, A.; Kumada, H.; Ohmae, M.; Kirihata, M.; Imahori, Y.; Suzuki, M.; Sakrai, Y.; Sumi, T.; et al. Effectiveness of boron neutron capture therapy for recurrent head and neck malignancies. Appl. Radiat. Isot. 2009, 67, S37–S42. [Google Scholar] [CrossRef]
- Aihara, T.; Morita, N.; Kamitani, N.; Kumada, H.; Ono, K.; Hiratsuka, J.; Harada, T. BNCT for advanced or recurrent head and neck cancer. Appl. Radiat. Isot. 2014, 88, 12–15. [Google Scholar] [CrossRef]
- Kankaanranta, L.; Seppala, T.; Koivunoro, H.; Saarilahti, K.; Atula, T.; Collan, J.; Salli, E.; Kortesniemi, M.; Uusi-Simola, J.; Valimaki, P.; et al. Boron neutron capture therapy in the treatment of locally recurred head-and-neck cancer: Final analysis of a phase I/II trial. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e67–e75. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.W.; Wang, S.J.; Chu, P.Y.; Ho, C.Y.; Jiang, S.H.; Liu, Y.W.; Liu, Y.H.; Liu, H.M.; Peir, J.J.; Chou, F.I.; et al. BNCT for locally recurrent head and neck cancer: Preliminary clinical experience from a phase I/II trial at Tsing Hua Open-Pool Reactor. Appl. Radiat. Isot. 2011, 69, 1803–1806. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. New Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Barth, R.F.; Yang, W.; Rotaru, J.H.; Moeschberger, M.L.; Boesel, C.P.; Soloway, A.H.; Joel, D.D.; Nawrocky, M.M.; Ono, K.; Goodman, J.H. Boron neutron capture therapy of brain tumors: Enhanced survival and cure following blood-brain barrier disruption and intracarotid injection of sodium borocaptate and boronophenylalanine. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 209–218. [Google Scholar] [CrossRef]
- Yamamoto, T.; Nakai, K.; Kageji, T.; Kumada, H.; Endo, K.; Matsuda, M.; Shibata, Y.; Matsumura, A. Boron neutron capture therapy for newly diagnosed glioblastoma. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2009, 91, 80–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takai, S.; Wanibuchi, M.; Kawabata, S.; Takeuchi, K.; Sakurai, Y.; Suzuki, M.; Ono, K.; Miyatake, S.I. Reactor-based boron neutron capture therapy for 44 cases of recurrent and refractory high-grade meningiomas with long-term follow-up. Neuro-Oncol. 2021. [Google Scholar] [CrossRef]
- Kageji, T.; Nagahiro, S.; Matsuzaki, K.; Mizobuchi, Y.; Toi, H.; Nakagawa, Y.; Kumada, H. Boron neutron capture therapy using mixed epithermal and thermal neutron beams in patients with malignant glioma-correlation between radiation dose and radiation injury and clinical outcome. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 1446–1455. [Google Scholar] [CrossRef]
- Kageji, T.; Mizobuchi, Y.; Nagahiro, S.; Nakagawa, Y.; Kumada, H. Clinical results of boron neutron capture therapy (BNCT) for glioblastoma. Appl. Radiat. Isot. 2011, 69, 1823–1825. [Google Scholar] [CrossRef] [PubMed]
- Miyatake, S.; Kawabata, S.; Kajimoto, Y.; Aoki, A.; Yokoyama, K.; Yamada, M.; Kuroiwa, T.; Tsuji, M.; Imahori, Y.; Kirihata, M.; et al. Modified boron neutron capture therapy for malignant gliomas performed using epithermal neutron and two boron compounds with different accumulation mechanisms: An efficacy study based on findings on neuroimages. J. Neurosurg. 2005, 103, 1000–1009. [Google Scholar] [CrossRef]
- Kawabata, S.; Miyatake, S.; Kuroiwa, T.; Yokoyama, K.; Doi, A.; Iida, K.; Miyata, S.; Nonoguchi, N.; Michiue, H.; Takahashi, M.; et al. Boron neutron capture therapy for newly diagnosed glioblastoma. J. Radiat. Res. 2009, 50, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyatake, S.; Kawabata, S.; Yokoyama, K.; Kuroiwa, T.; Michiue, H.; Sakurai, Y.; Kumada, H.; Suzuki, M.; Maruhashi, A.; Kirihata, M.; et al. Survival benefit of Boron neutron capture therapy for recurrent malignant gliomas. J. Neurooncol. 2009, 91, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Ono, K.; Masunaga, S.; Suzuki, M.; Kinashi, Y.; Takagaki, M.; Akaboshi, M. The combined effect of boronophenylalanine and borocaptate in boron neutron capture therapy for SCCVII tumors in mice. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 431–436. [Google Scholar] [CrossRef]
- Coderre, J.A.; Elowitz, E.H.; Chadha, M.; Bergland, R.; Capala, J.; Joel, D.D.; Liu, H.B.; Slatkin, D.N.; Chanana, A.D. Boron neutron capture therapy for glioblastoma multiforme using p-boronophenylalanine and epithermal neutrons: Trial design and early clinical results. J. Neurooncol. 1997, 33, 141–152. [Google Scholar] [CrossRef]
- Finkel, G.C.; Poletti, C.E.; Fairchild, R.G.; Slatkin, D.N.; Sweet, W.H. Distribution of 10B after infusion of Na210B12H11SH into a patient with malignant astrocytoma: Implications for boron neutron capture therapy. Neurosurgery 1989, 24, 6–11. [Google Scholar] [CrossRef]
- Kageji, T.; Nakagawa, Y.; Kitamura, K.; Matsumoto, K.; Hatanaka, H. Pharmacokinetics and boron uptake of BSH (Na2B12H11SH) in patients with intracranial tumors. J. Neurooncol 1997, 33, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Imahori, Y.; Ueda, S.; Ohmori, Y.; Sakae, K.; Kusuki, T.; Kobayashi, T.; Takagaki, M.; Ono, K.; Ido, T.; Fujii, R. Positron emission tomography-based boron neutron capture therapy using boronophenylalanine for high-grade gliomas: Part I. Clin. Cancer Res. 1998, 4, 1825–1832. [Google Scholar] [PubMed]
- Imahori, Y.; Ueda, S.; Ohmori, Y.; Sakae, K.; Kusuki, T.; Kobayashi, T.; Takagaki, M.; Ono, K.; Ido, T.; Fujii, R. Positron emission tomography-based boron neutron capture therapy using boronophenylalanine for high-grade gliomas: Part II. Clin. Cancer Res. 1998, 4, 1833–1841. [Google Scholar] [PubMed]
- Aihara, T.; Hiratsuka, J.; Morita, N.; Uno, M.; Sakurai, Y.; Maruhashi, A.; Ono, K.; Harada, T. First clinical case of boron neutron capture therapy for head and neck malignancies using 18F-BPA PET. Head Neck 2006, 28, 850–855. [Google Scholar] [CrossRef]
- Guidebook on Accelerator BPA-BNCT; Japan Society for Neutron Capture Therapy, Osaka/Japan Society for Radiation Oncology: Tokyo, Japan, 2020.
- Masunaga, S.; Ono, K.; Sakurai, Y.; Suzuki, M.; Takagaki, M.; Kobayashi, T.; Kinashi, Y.; Akaboshi, M. Responses of total and quiescent cell populations in solid tumors to boron and gadolinium neutron capture reaction using neutrons with two different energy spectra. Jpn. J. Cancer Res. 1998, 89, 81–88. [Google Scholar] [CrossRef]
- Masunaga, S.; Ono, K.; Sakurai, Y.; Takagaki, M.; Kobayashi, T.; Suzuki, M.; Kinashi, Y.; Akaboshi, M. Response of quiescent and total tumor cells in solid tumors to neutrons with various cadmium ratios. Int. J. Radiat. Oncol. Biol. Phys. 1998, 41, 1163–1170. [Google Scholar] [CrossRef]
- Abad, E.; Samino, S.; Yanes, O.; Potesil, D.; Zdrahal, Z.; Lyakhovich, A. Activation of glycogenolysis and glycolysis in breast cancer stem cell models. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165886. [Google Scholar] [CrossRef]
- Bao, B.; Azmi, A.S.; Li, Y.; Ahmad, A.; Ali, S.; Banerjee, S.; Kong, D.; Sarkar, F.H. Targeting CSCs in tumor microenvironment: The potential role of ROS-associated miRNAs in tumor aggressiveness. Curr. Stem. Cell Res. 2014, 9, 22–35. [Google Scholar] [CrossRef] [Green Version]
- Luo, M.; Wicha, M.S. Targeting cancer stem cell redox metabolism to enhance therapy responses. Semin. Radiat. Oncol. 2019, 29, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H. Boron lipid-based liposomal boron delivery system for neutron capture therapy: Recent development and future perspective. Future Med. Chem. 2013, 5, 715–730. [Google Scholar] [CrossRef] [PubMed]
- Nakase, I.; Aoki, A.; Sakai, Y.; Hirase, S.; Ishimura, M.; Takatani-Nakase, T.; Hattori, Y.; Kirihata, M. Antibody-based receptor targeting using an fc-binding peptide-dodecaborate conjugate and macropinocytosis induction for boron neutron capture therapy. ACS Omega 2020, 5, 22731–22738. [Google Scholar] [CrossRef] [PubMed]
- Yamagami, M.; Tajima, T.; Ishimoto, K.; Miyake, H.; Michiue, H.; Takaguchi, Y. Physical modification of carbon nanotubes with a dendrimer bearing terminal mercaptoundecahydrododecaborates (Na2B12H11S). Heteroat. Chem. 2018, 29, e21467. [Google Scholar] [CrossRef]
- Kueffer, P.J.; Maitz, C.A.; Khan, A.A.; Schuster, S.A.; Shlyakhtina, N.I.; Jalisatgi, S.S.; Brockman, J.D.; Nigg, D.W.; Hawthorne, M.F. Boron neutron capture therapy demonstrated in mice bearing EMT6 tumors following selective delivery of boron by rationally designed liposomes. Proc. Natl. Acad. Sci. USA 2013, 110, 6512–6517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, W.; Svirskis, D.; Sarojini, V.; McGregor, A.L.; Bevitt, J.; Wu, Z. Cyclic-RGDyC functionalized liposomes for dual-targeting of tumor vasculature and cancer cells in glioblastoma: An in vitro boron neutron capture therapy study. Oncotarget 2017, 8, 36614–36627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruyama, K.; Ishida, O.; Kasaoka, S.; Takizawa, T.; Utoguchi, N.; Shinohara, A.; Chiba, M.; Kobayashi, H.; Eriguchi, M.; Yanagie, H. Intracellular targeting of sodium mercaptoundecahydrododecaborate (BSH) to solid tumors by transferrin-PEG liposomes, for boron neutron-capture therapy (BNCT). J. Control. Release 2004, 98, 195–207. [Google Scholar] [CrossRef]
- Nomoto, T.; Inoue, Y.; Yao, Y.; Suzuki, M.; Kanamori, K.; Takemoto, H.; Matsui, M.; Tomoda, K.; Nishiyama, N. Poly(vinyl alcohol) boosting therapeutic potential of p-boronophenylalanine in neutron capture therapy by modulating metabolism. Sci. Adv. 2020, 6, eaaz1722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
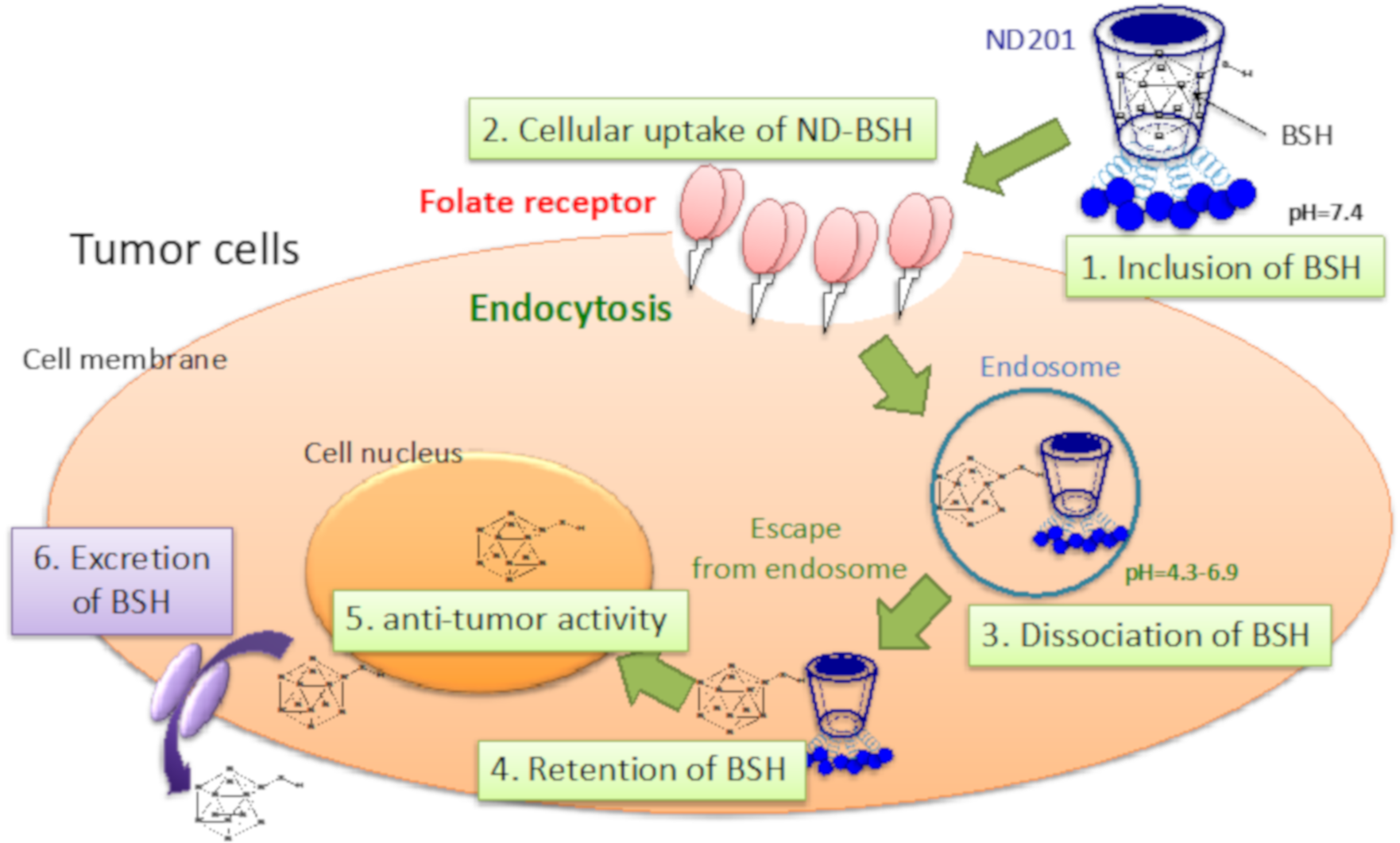
- Matsumoto, Y.; Hattori, K.; Arima, H.; Motoyama, K.; Higashi, T.; Ishikawa, H.; Fukumitsu, N.; Aihara, T.; Nakai, K.; Kumada, H.; et al. Folate-appended cyclodextrin improves the intratumoral accumulation of existing boron compounds. Appl. Radiat. Isot. 2020, 163, 109201. [Google Scholar] [CrossRef] [PubMed]
- Maeda, H. The 35th anniversary of the discovery of EPR effect: A new wave of nanomedicines for tumor-targeted drug delivery-personal remarks and future prospects. J. Pers. Med. 2021, 11, 229. [Google Scholar] [CrossRef]
- Matsumura, Y.; Maeda, H. A new concept for macromolecular therapeutics in cancer chemotherapy: Mechanism of tumoritropic accumulation of proteins and the antitumor agent smancs. Cancer Res. 1986, 46, 6387–6392. [Google Scholar]
- Koganei, H.; Ueno, M.; Tachikawa, S.; Tasaki, L.; Ban, H.S.; Suzuki, M.; Shiraishi, K.; Kawano, K.; Yokoyama, M.; Maitani, Y.; et al. Development of high boron content liposomes and their promising antitumor effect for neutron capture therapy of cancers. Bioconjug Chem. 2013, 24, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Tachikawa, S.; Miyoshi, T.; Koganei, H.; El-Zaria, M.E.; Vinas, C.; Suzuki, M.; Ono, K.; Nakamura, H. Spermidinium closo-dodecaborate-encapsulating liposomes as efficient boron delivery vehicles for neutron capture therapy. Chem. Commun. 2014, 50, 12325–12328. [Google Scholar] [CrossRef] [Green Version]
- Mi, P.; Yanagie, H.; Dewi, N.; Yen, H.C.; Liu, X.; Suzuki, M.; Sakurai, Y.; Ono, K.; Takahashi, H.; Cabral, H.; et al. Block copolymer-boron cluster conjugate for effective boron neutron capture therapy of solid tumors. J. Control. Release 2017, 254, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, S.; Kanoh, D.; Sato, S.; Sakurai, Y.; Suzuki, M.; Nakamura, H. Maleimide-functionalized closo-dodecaborate albumin conjugates (MID-AC): Unique ligation at cysteine and lysine residues enables efficient boron delivery to tumor for neutron capture therapy. J. Control. Release 2016, 237, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Ishii, S.; Sato, S.; Asami, H.; Hasegawa, T.; Kohno, J.Y.; Nakamura, H. Design of S-S bond containing maleimide-conjugated closo-dodecaborate (SSMID): Identification of unique modification sites on albumin and investigation of intracellular uptake. Org. Biomol. Chem. 2019, 17, 5496–5499. [Google Scholar] [CrossRef]
- Sumitani, S.; Oishi, M.; Yaguchi, T.; Murotani, H.; Horiguchi, Y.; Suzuki, M.; Ono, K.; Yanagie, H.; Nagasaki, Y. Pharmacokinetics of core-polymerized, boron-conjugated micelles designed for boron neutron capture therapy for cancer. Biomaterials 2012, 33, 3568–3577. [Google Scholar] [PubMed] [Green Version]
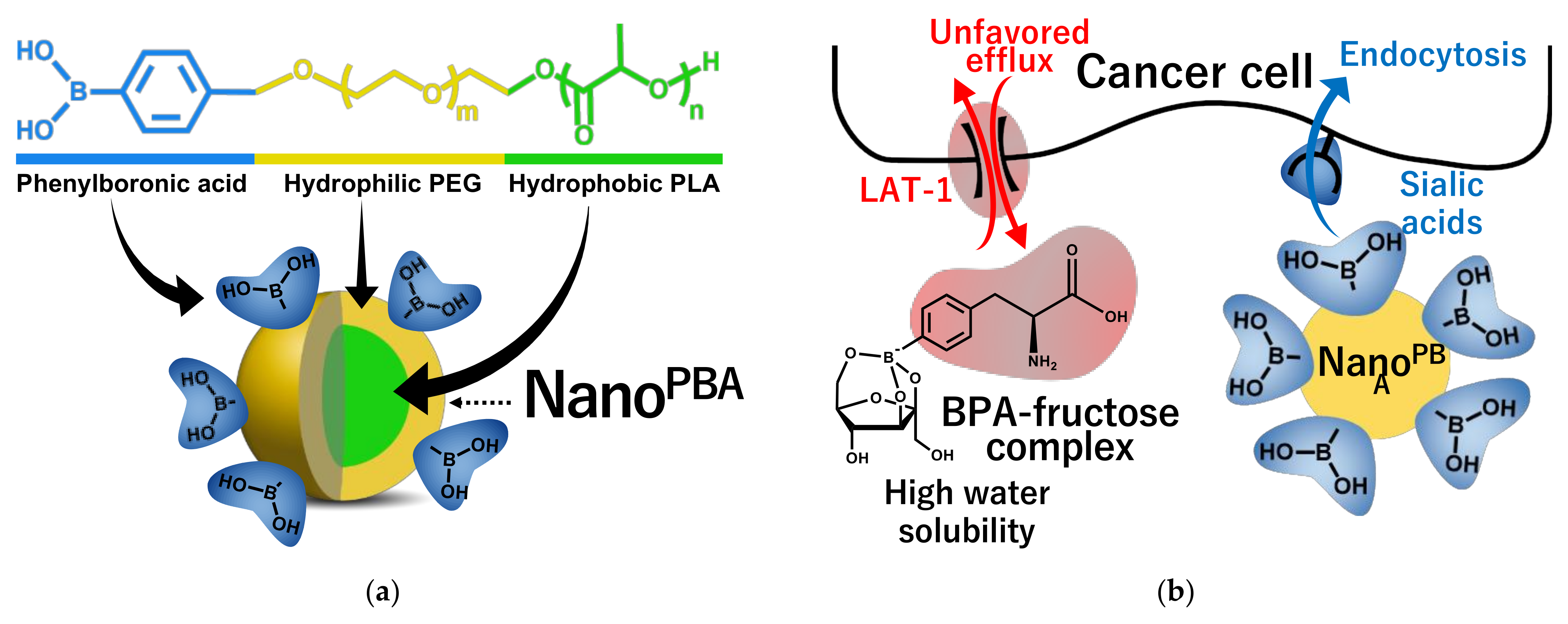
- Kim, A.; Suzuki, M.; Matsumoto, Y.; Fukumitsu, N.; Nagasaki, Y. Non-isotope enriched phenylboronic acid-decorated dual-functional nano-assembles for an actively targeting BNCT drug. Biomaterials 2021, 268, 120551. [Google Scholar] [PubMed]
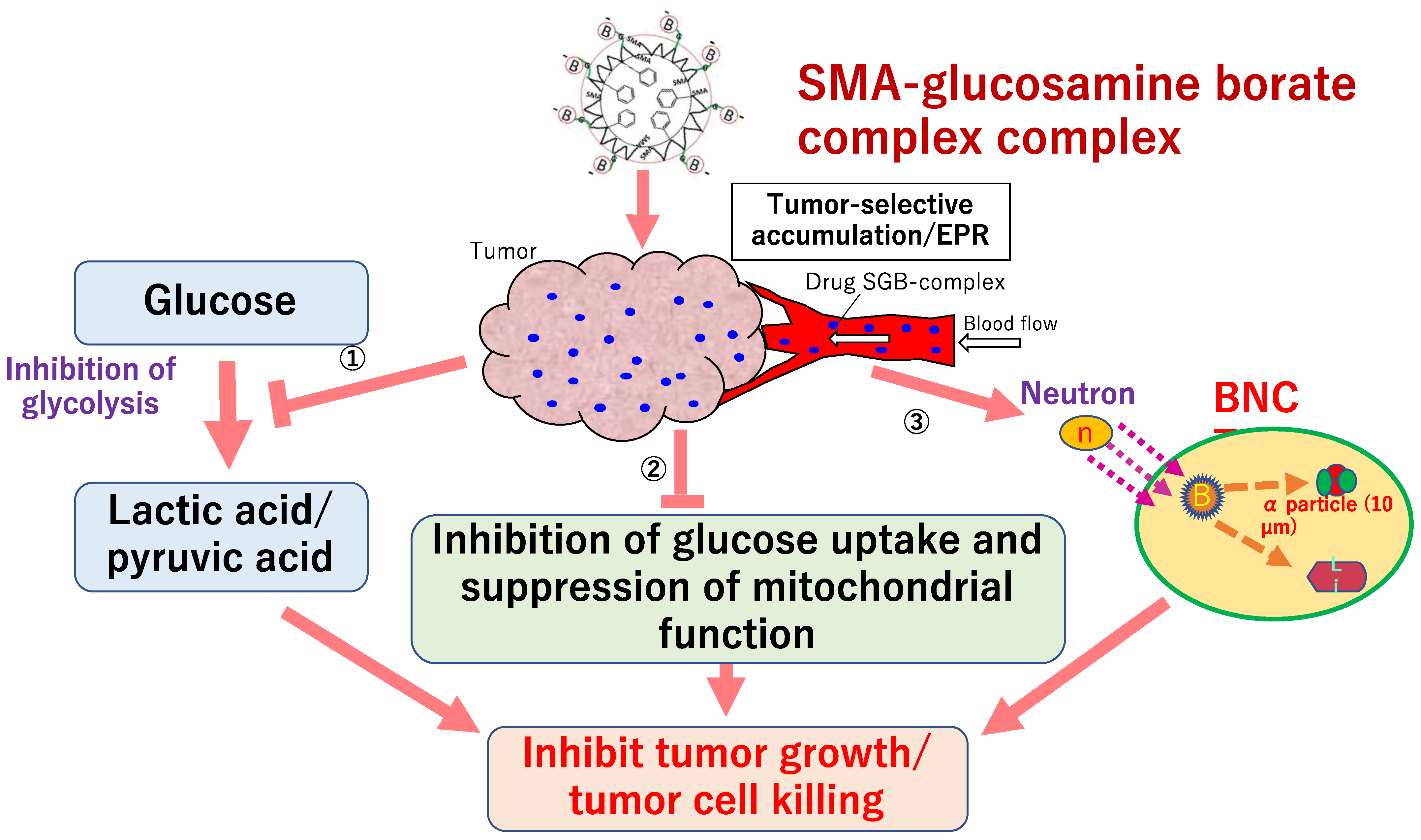
- Islam, W.; Matsumoto, Y.; Fang, J.; Harada, A.; Niidome, T.; Ono, K.; Tsutsuki, H.; Sawa, T.; Imamura, T.; Sakurai, K.; et al. Polymer-conjugated glucosamine complexed with boric acid shows tumor-selective accumulation and simultaneous inhibition of glycolysis. Biomaterials 2021, 269, 120631. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | N | RT Modality | Treatment | Endpoint | Late Toxicity Rate | |
|---|---|---|---|---|---|---|
| Heat | Lung | |||||
| DeCesaris [15] | 36 | Photon RT | Preope/definitive | Perioperative death | 13.9% | |
| 18 | Proton | 0% | ||||
| Wang [6] | 320 | IMRT | Preope/definitive | Grade 3 (2y/5y) | 18%/21% | NA |
| 159 | Proton | 11%/13% | NA | |||
| Wang [17] | 208 | 3DCRT | Preoperative | Perioperative complication | 15.9% | 30.3% |
| 164 | IMRT | 17.1% | 23.8% | |||
| 72 | Proton | 9.7% | 13.9% | |||
| Makishima [10] | 19 | 3DCRT | Definitive | Grade 3 | 0% | 10.3% |
| 25 | Proton | 0% | 0% | |||
| Xi [18] | 211 | IMRT | Preope/definitive | Grade 3 | 2.4% | 4.7% |
| 132 | Proton | 0.8% | 2.3% | |||
| Lin [19] | 61 | IMRT | Preope/definitive | Grade 3 | 5 * | 11 * |
| 46 | Proton | 3 * | 5 * | |||
| Author | N | RT | Dose | Chemotherapy | Treatment | Outcome |
|---|---|---|---|---|---|---|
| Hong [46] | 25 | proton | 30GyRBE/10fr 25GyRBE/5fr | capecitabine | preoperative | OS: 75%/1Y |
| Terashima [48] | 50 | proton | 50GyRBE/25fr 70.2GyRBE/26fr 67.5GyRBE/25fr | gemcitabine | curative | OS: 76.8%/1Y, PFS: 64.3%/1Y |
| Hong [47] | 50 | proton | 25GyRBE/5fr | capecitabine | preoperative | OS: 42%/2Y |
| Maemura [52] | 10 | proton | 50GyRBE/25fr 67.5GyRBE/25fr | gemcitabine, S-1 | curative | OS: 80, 45, 22.5%/1, 2, 3Y |
| Kim [49] | 37 | proton | 45GyRBE/10fr | capecitabine, 5-FU | curative | OS: 75.7%/1Y, PFS: 64.8%/1Y, 19.3M |
| Jethea [50] | 13 | proton | 50GyRBE/25fr | capecitabine, 5-FU | curative | OS: 62, 40%/1, 2Y, 16M |
| Hiroshima [51] | 42 | proton | 50–67.5GyRBE/25-33fr | gemcitabine, S-1 | curative | OS: 77.5, 50.8%/1, 2Y, 25.6M |
| Kawashiro [53] | 72 | carbon | 52.8GyRBE/12fr 55.2GyRBE/12fr | gemcitabine, S-1 (n = 56) | curative | OS: 73, 46%/1, 2Y, 21.5M |
| Vitolo [58] | carbon | 38.4GyRBE/4fr | FOLFIRINOX, gemcitabine | preoperative |
| Author | N | RT Modality | Total Dose (Gy) | Photon (Gy) | Proton (GyRBE) | Efficacy (%) | Late toxicity (Grade 3) (%) | |
|---|---|---|---|---|---|---|---|---|
| GI | GU | |||||||
| Shipley [67] | 202 | Photon +Proton | 75.6 67.2 | 50.4 (pelvis) 50.4 (pelvis) + 16.8 (local) | 25.2 (local) | 8y-LC:73 | 2.9 | NA |
| Photon | - | 59 | 0 | NA | ||||
| Roach [68] | 440 | Photon | 70.2 70.2 | 50.4 (pelvis) + 19.8 (local) 70.2 (local) | 7y-PFS:40 | 4.3 | 3 | |
| Photon | 27 | 0 | 0 | |||||
| Local prostate irradiation | ||||||||
| Zeitman [69] | 393 | Photon +Proton | 79.2 70.2 | 50.4 (local) 50.4 (local) | 28.8 (local) | 10y-bRF:83 | 1 | 2 |
| Photon +Proton | 19.8 (local) | 67 | 0 | 2 | ||||
| Kuban [70] | 301 | Photon | 78.0 70.0 | 78.0 (local) 78.0 (local) | 10y-FFF:73 | 7 | 3 | |
| Photon | 50 | 1 | 5 | |||||
| Facility | Neutron Source | Year | Tumor | Patients No. | Boron Agents | Clinical Course |
|---|---|---|---|---|---|---|
| Osaka University [171,172] | KUR JRR4 | 2001–2014 | Rec H&N | 45 | BSH, BPA | 5y 32% 10y 21% PR 29% CR 51% |
| Kawasaki Medical College [173] | KUR JRR4 | 2003–2011 | Rec H&N | 20 | BPA | PR 35% CR 55% |
| Kawasaki Medical College | KUR JRR4 | 2006–2012 | H&N preop. | 7 | BPA | 5y 42% PR 1/7 CR 5/7 |
| Helsinki University Central Hospital [174] | FiR-1 | 2003–2008 | Rec H&N | 30 | BPA | MST 13mo PR31% CR 45% |
| Taipei Veterans General Hospital [175] | THOR | 2010–2011 | Rec H&N | 10 | BPA | PR 40% CR 30% |
| Facility | Neutron Source | Year | Tumor | Patients No. | Boron Agents | Clinical Course (Month) |
|---|---|---|---|---|---|---|
| University of Tsukuba [178] | JRR4 | 1998–2007 | GBM | 15 | BPA, BSH | MST 23.3 27.1 |
| Tokusima University [180,181] | KUR JRR4 | 1998–2008 | GBM | 23 | BSH | MST 15.5 19.5 26.2 |
| Osaka Medical College [182,183,184] | KUR | 2002–2006 | GBM | 21 | BPA, BSH | MST 14.5 23.5 |
| 2002–2007 | rGBM | 19 | BSH, BPA | MST 10.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, Y.; Fukumitsu, N.; Ishikawa, H.; Nakai, K.; Sakurai, H. A Critical Review of Radiation Therapy: From Particle Beam Therapy (Proton, Carbon, and BNCT) to Beyond. J. Pers. Med. 2021, 11, 825. https://doi.org/10.3390/jpm11080825
Matsumoto Y, Fukumitsu N, Ishikawa H, Nakai K, Sakurai H. A Critical Review of Radiation Therapy: From Particle Beam Therapy (Proton, Carbon, and BNCT) to Beyond. Journal of Personalized Medicine. 2021; 11(8):825. https://doi.org/10.3390/jpm11080825
Chicago/Turabian StyleMatsumoto, Yoshitaka, Nobuyoshi Fukumitsu, Hitoshi Ishikawa, Kei Nakai, and Hideyuki Sakurai. 2021. "A Critical Review of Radiation Therapy: From Particle Beam Therapy (Proton, Carbon, and BNCT) to Beyond" Journal of Personalized Medicine 11, no. 8: 825. https://doi.org/10.3390/jpm11080825