
Wear Risk Prevention and Reduction in Total Hip Arthroplasty. A Personalized Study Comparing Cement and Cementless Fixation Techniques Employing Finite Element Analysis

 , , ,
, , ,
Abstract
:1. Introduction
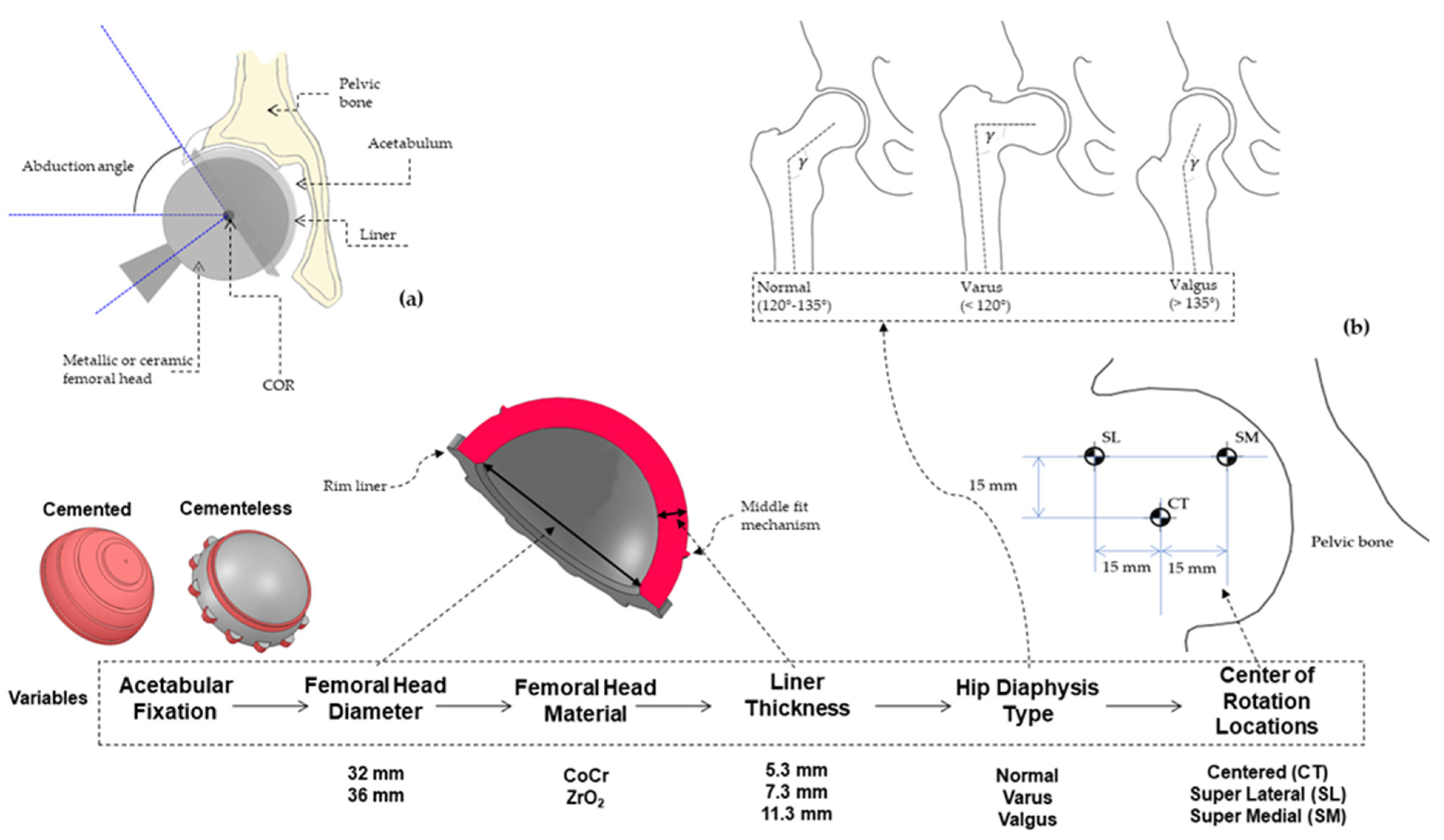
2. Materials and Methods
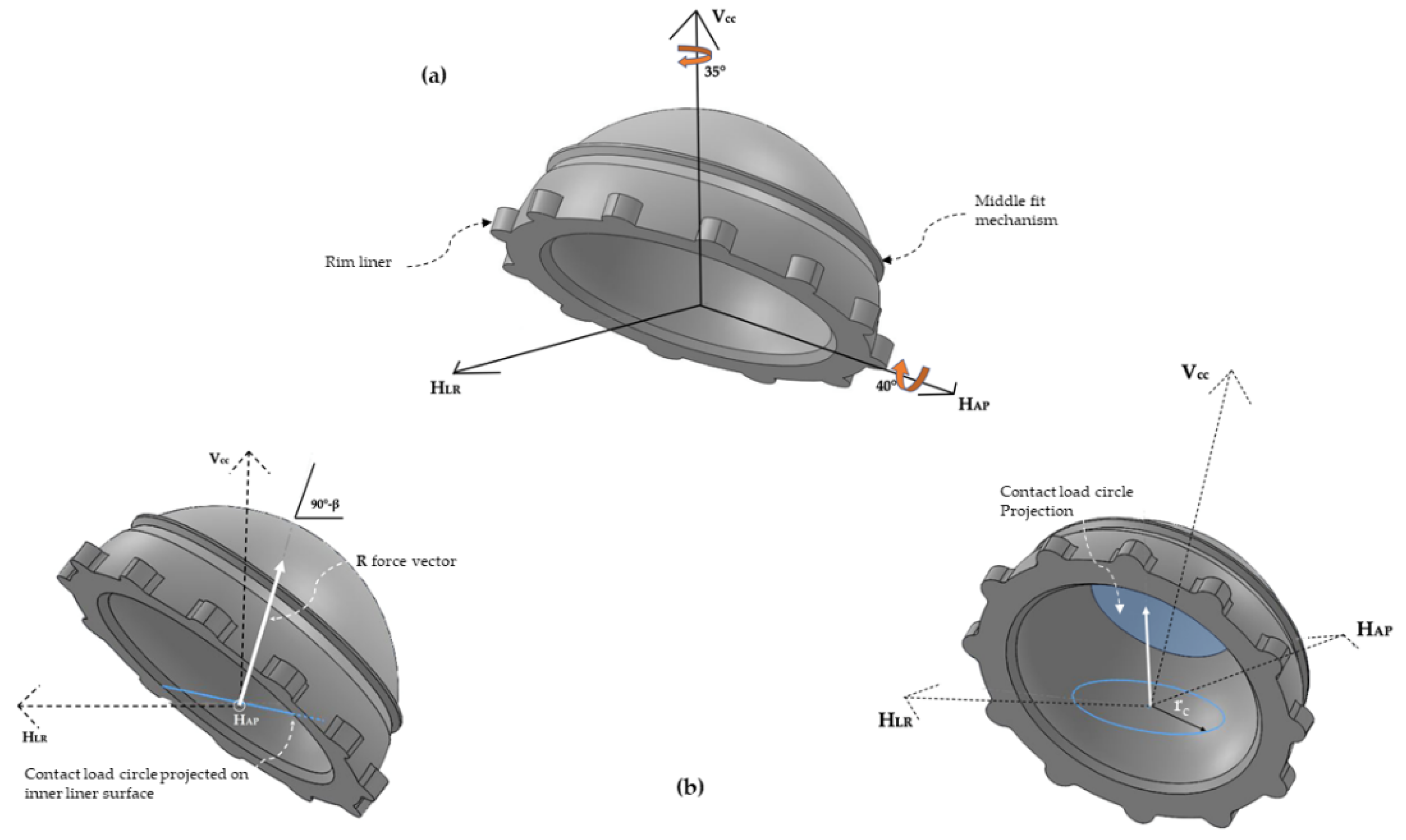
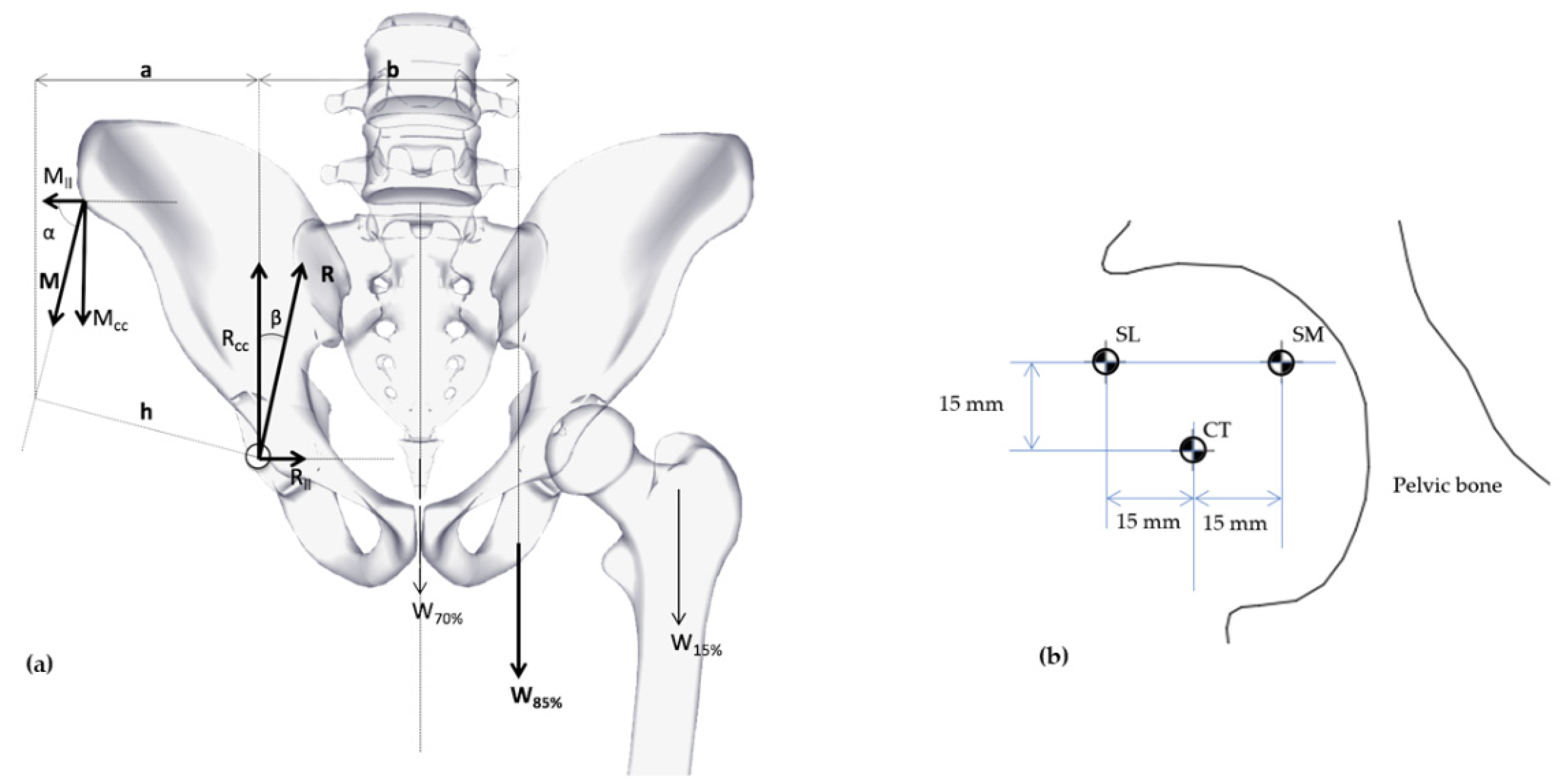
2.1. Load and Boundary Conditions
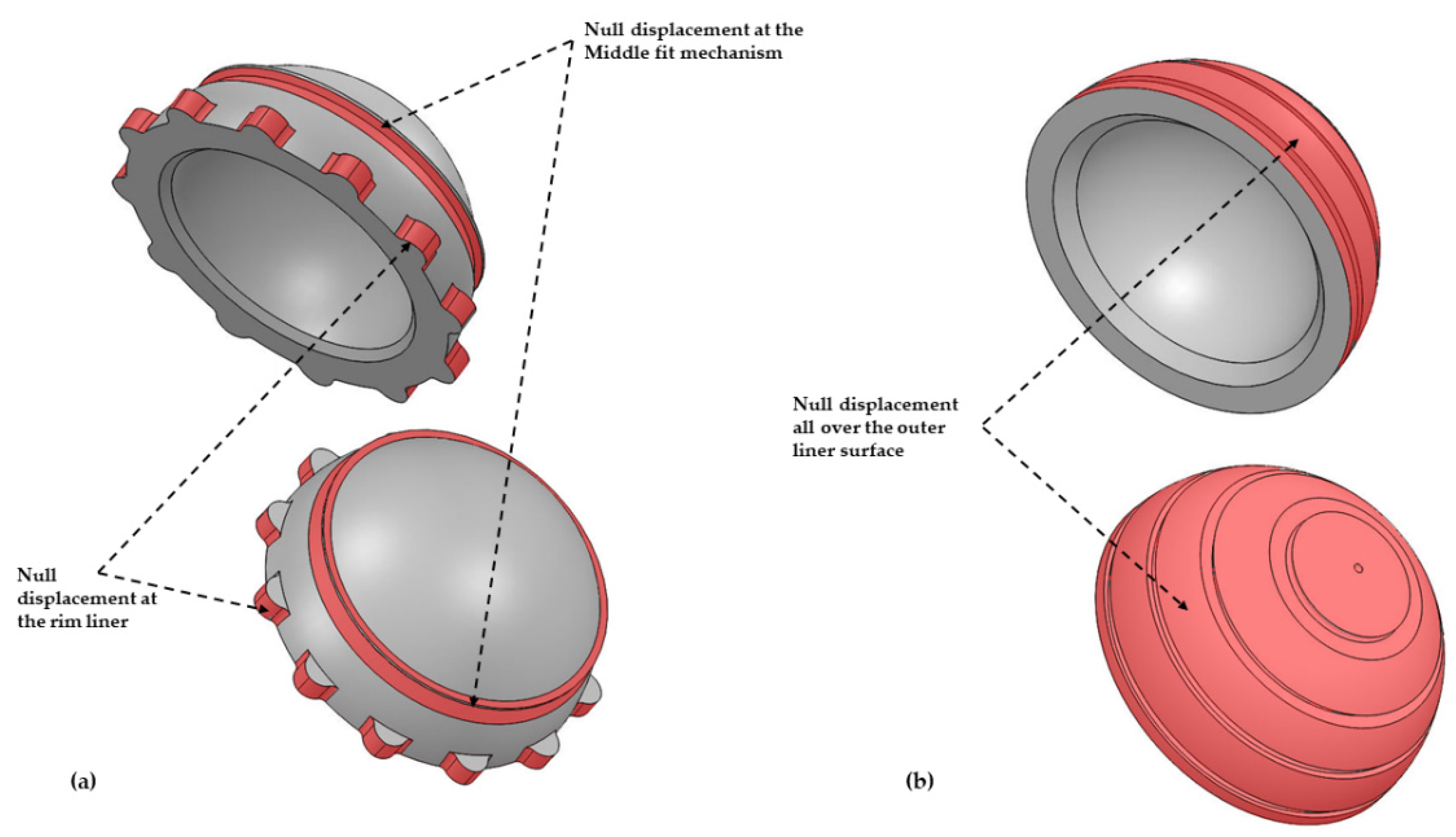
2.2. FE Modeling and Simulations
2.3. Wear Risk and Statistical Analyses
3. Results
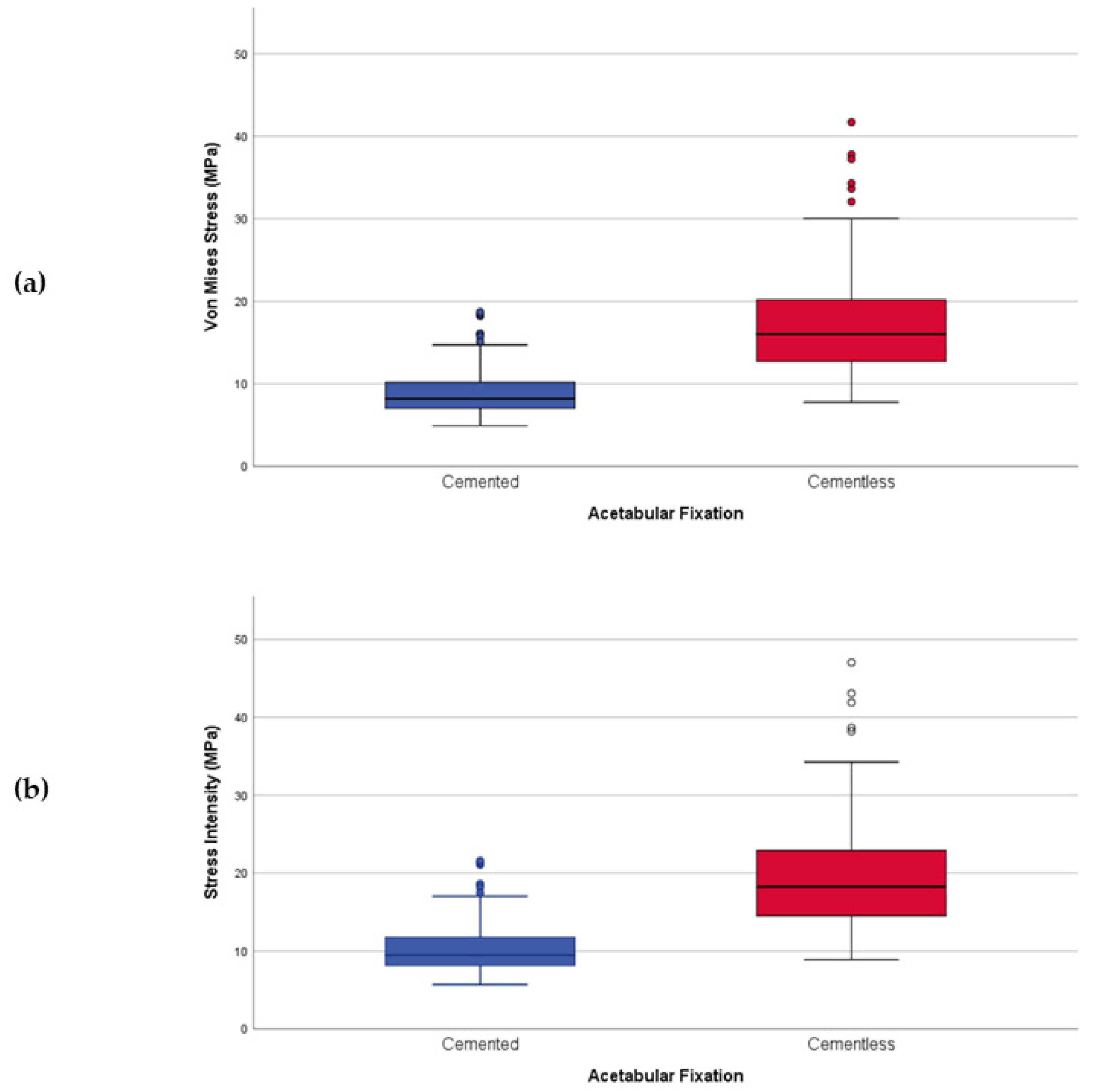
3.1. VM Stress vs. SI Stress
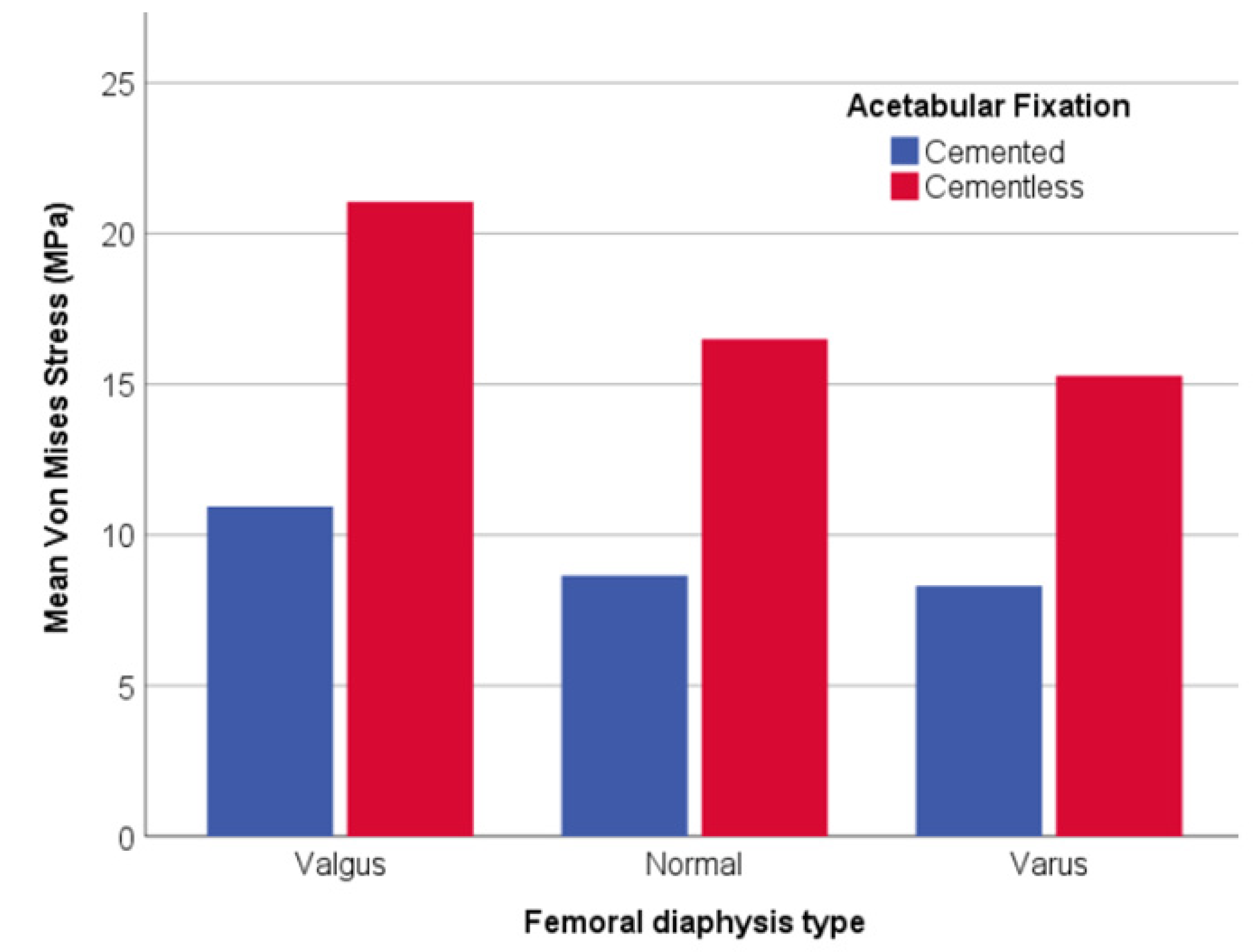
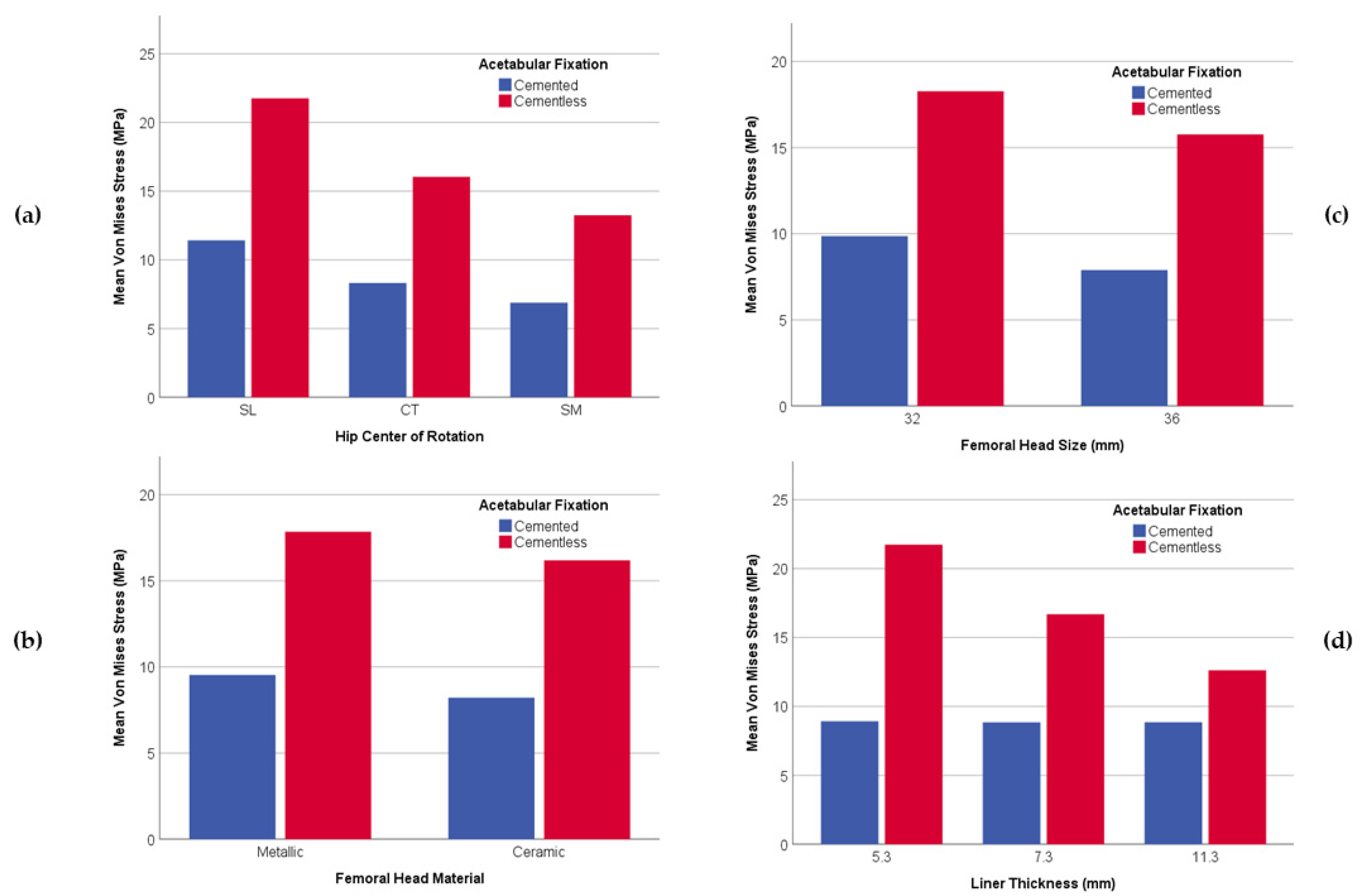
3.2. General Analyses of the Parameters
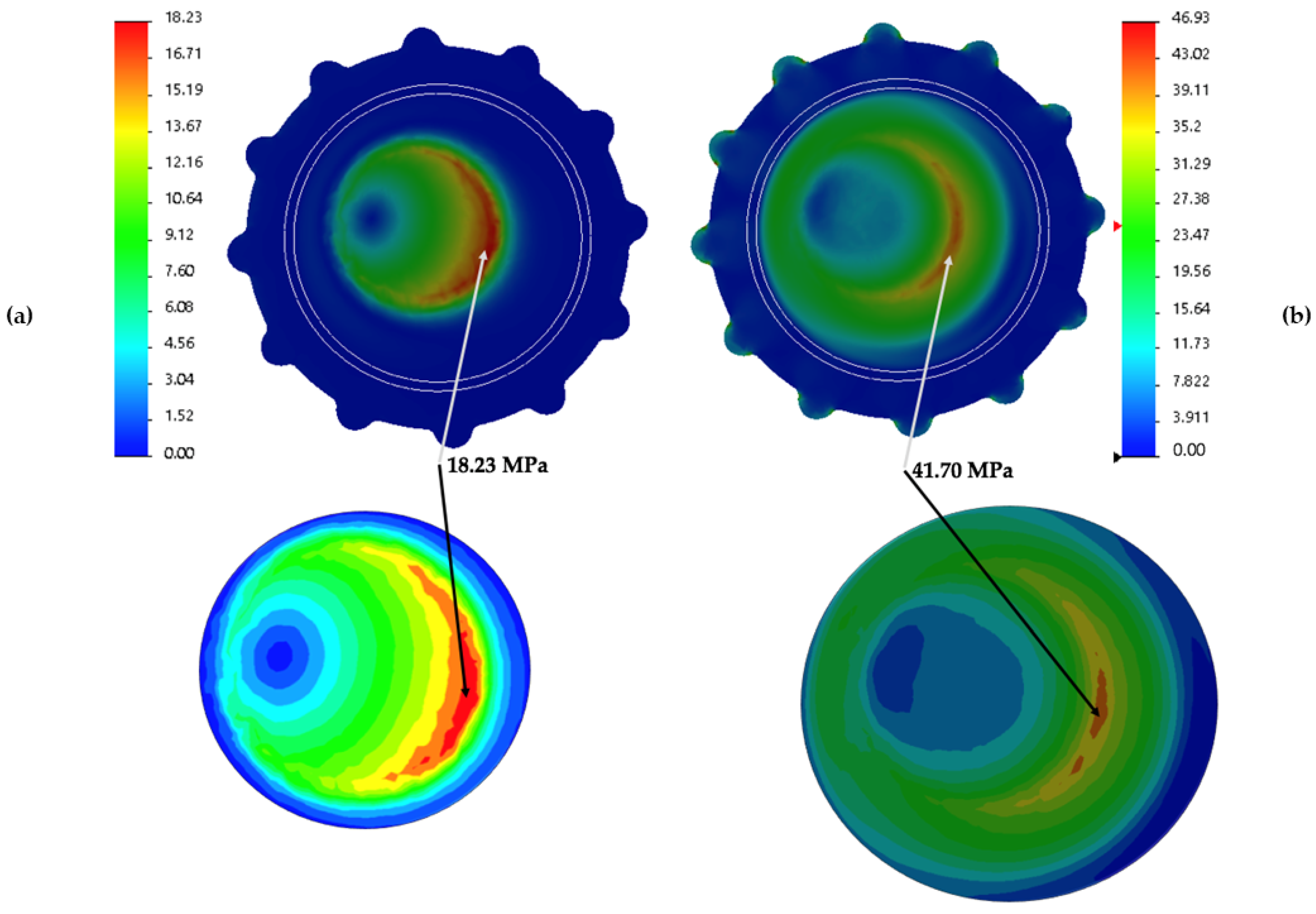
3.3. Stress Distribution over the Liner
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pakvis, D.; Van Hellemondt, G.; De Visser, E.; Jacobs, W.; Spruit, M. Is there evidence for a superior method of socket fixation in hip arthroplasty? A systematic review. Int. Orthop. 2011, 35, 1109–1118. [Google Scholar] [CrossRef] [Green Version]
- Van Der Veen, H.C.; Van Jonbergen, H.P.W.; Poolman, R.W.; Bulstra, S.K.; Van Raay, J.J.A.M. Is there evidence for accelerated polyethylene wear in uncemented compared to cemented acetabular components? A systematic review of the literature. Int. Orthop. 2013, 37, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Clement, N.D.; Biant, L.C.; Breusch, S.J. Total hip arthroplasty: To cement or not to cement the acetabular socket? A critical review of the literature. Arch. Orthop. Trauma Surg. 2012, 132, 411–427. [Google Scholar] [CrossRef]
- Berry, D.J.; Barnes, C.L.; Scott, R.D.; Cabanela, M.E.; Poss, R. Catastrophic failure of the polyethylene liner of uncemented acetabular components. J. Bone Jt. Surg. Br. 1994, 76, 575–578. [Google Scholar] [CrossRef] [Green Version]
- Harris, W.H. The problem is osteolysis. Clin. Orthop. Relat. Res. 1995, 311, 46–53. [Google Scholar]
- Yamaguchi, T.; Naito, M.; Asayama, I.; Shiramizu, K. Cementless total hip arthroplasty using an autograft of the femoral head for marked acetabular dysplasia: Case series. J. Orthop. Surg. Hong Kong 2004, 12, 14–18. [Google Scholar] [CrossRef]
- Gwynne-Jones, D.P.; Garneti, N.; Wainwright, C.; Matheson, J.A.; King, R. The Morscher Press Fit acetabular component: A NINE- TO 13-YEAR REVIEW. J. Bone Jt. Surg. Br. Vol. 2009, 91-B, 859–864. [Google Scholar] [CrossRef] [PubMed]
- Busch, V.; Klarenbeek, R.; Slooff, T.; Schreurs, B.W.; Gardeniers, J. Cemented hip designs are a reasonable option in young patients. Clin. Orthop. Relat. Res. 2010, 468, 3214–3220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Astion, D.J.; Saluan, P.; Stulberg, B.N.; Rimnac, C.M.; Li, S. The porous-coated anatomic total hip prosthesis: Failure of the metal-backed acetabular component. JBJS 1996, 78, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, F. Biomechanics of the Normal and Diseased Hip; Springer: Berlin/Heidelberg, Germany, 1976. [Google Scholar]
- Barbour, P.S.M.; Barton, D.C.; Fisher, J. The influence of contact stress on the wear of UHMWPE for total replacement hip prostheses. Wear 1995, 181–183, 250–257. [Google Scholar] [CrossRef]
- Bevill, S.L.; Bevill, G.R.; Penmetsa, J.R.; Petrella, A.J.; Rullkoetter, P.J. Finite element simulation of early creep and wear in total hip arthroplasty. J. Biomech. 2005, 38, 2365–2374. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Edidin, A.A.; Bartel, D.L. The role of backside polishing, cup angle, and polyethylene thickness on the contact stresses in metal-backed acetabular components. J. Biomech. 1997, 30, 639–642. [Google Scholar] [CrossRef]
- Liu, F.; Leslie, I.; Williams, S.; Fisher, J.; Jin, Z. Development of computational wear simulation of metal-on-metal hip resurfacing replacements. J. Biomech. 2008, 41, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Maxian, T.A.; Brown, T.D.; Pedersen, D.R.; Callaghan, J.J. A sliding-distance-coupled finite element formulation for polyethylene wear in total hip arthroplasty. J. Biomech. 1996, 29, 687–692. [Google Scholar] [CrossRef]
- Munro, J.T.; Anderson, I.A.; Walker, C.G.; Shim, V.B. Finite element analysis of retroacetabular osteolytic defects following total hip replacement. J. Biomech. 2013, 46, 2529–2533. [Google Scholar] [CrossRef]
- Nadzadi, M.E.; Pedersen, D.R.; Yack, H.J.; Callaghan, J.J.; Brown, T.D. Kinematics, kinetics, and finite element analysis of commonplace maneuvers at risk for total hip dislocation. J. Biomech. 2003, 36, 577–591. [Google Scholar] [CrossRef]
- Wang, L.; Yang, W.; Peng, X.; Li, D.; Dong, S.; Zhang, S.; Zhu, J.; Jin, Z. Effect of progressive wear on the contact mechanics of hip replacements—Does the realistic surface profile matter? J. Biomech. 2015, 48, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Hirakawa, K.; Mitsugi, N.; Koshino, T.; Saito, T.; Hirasawa, Y.; Kubo, T. Effect of Acetabular Cup Position. Clin. Orthop. Relat. Res. 2001, 388, 135–142. [Google Scholar] [CrossRef]
- Udomkiat, P.; Dorr, L.D.; Wan, Z. Cementless hemispheric porous-coated sockets implanted with press-fit technique without screws: Average ten-year follow-up. J. Bone Jt. Surg. Ser. A 2002, 84, 1195–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bobman, J.T.; Danoff, J.R.; Babatunde, O.M.; Zhu, K.; Peyser, K.; Geller, J.A.; Gorroochurn, P.; Macaulay, W. Total Hip Arthroplasty Functional Outcomes Are Independent of Acetabular Component Orientation When a Polyethylene Liner Is Used. J. Arthroplast. 2016, 31, 830–834.e3. [Google Scholar] [CrossRef] [PubMed]
- Del Schutte, H.J.; Lipman, A.J.; Bannar, S.M.; Livermore, J.T.; Ilstrup, D.; Morrey, B.F. Effects of acetabular abduction on cup wear rates in total hip arthroplasty. J. Arthroplast. 1998, 13, 621–626. [Google Scholar] [CrossRef]
- Esposito, C.I.; Gladnick, B.P.; Lee, Y.; Lyman, S.; Wright, T.M.; Mayman, D.J.; Padgett, D.E. Cup position alone does not predict risk of dislocation after hip arthroplasty. J. Arthroplast. 2015, 30, 109–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, J.G.; Rogers, W.B.; Soffe, K.E.; Sullivan, R.J.; Griffen, D.G.; Sheehan, L.J. Effect of acetabular component orientation on recurrent dislocation, pelvic osteolysis, polyethylene wear, and component migration. J. Arthroplast. 1998, 13, 530–534. [Google Scholar] [CrossRef]
- Nishii, T.; Sakai, T.; Takao, M.; Sugano, N. Fluctuation of Cup Orientation During Press-Fit Insertion: A Possible Cause of Malpositioning. J. Arthroplast. 2015, 30, 1847–1851. [Google Scholar] [CrossRef]
- Farhoudi, H.; Oskouei, R.H.; Jones, C.F.; Taylor, M. A novel analytical approach for determining the frictional moments and torques acting on modular femoral components in total hip replacements. J. Biomech. 2015, 48, 976–983. [Google Scholar] [CrossRef]
- Johnson, K.L.; Johnson, K.L. Contact Mechanics; Cambridge University Press: Cambridge, UK, 1987; ISBN 0521347963. [Google Scholar]
- Bishop, N.E.; Hothan, A.; Morlock, M.M. High friction moments in large hard-on-hard hip replacement bearings in conditions of poor lubrication. J. Orthop. Res. 2013, 31, 807–813. [Google Scholar] [CrossRef]
- Bergmann, G.; Deuretzabacher, G.; Heller, M.; Graichen, F.; Rohlmann, A. Hip forces and gait patterns from rountine activities. J. Biomech. 2001, 34, 859–871. [Google Scholar] [CrossRef]
- Simpson, D.J.; Monk, A.P.; Murray, D.W.; Gill, H.S. Biomechanics in orthopaedics: Considerations of the hip and knee. Surgery 2010, 28, 478–482. [Google Scholar] [CrossRef]
- Gottschalk, F.; Kourosh, S.; Leveau, B. The functional anatomy of tensor fasciae latae and gluteus medius and minimus. J. Anat. 1989, 166, 179. [Google Scholar] [PubMed]
- Inman, V.T. Functional aspects of the abductor muscles of the hip. JBJS 1947, 29, 607–619. [Google Scholar]
- Le Veau, B.; Williams, M.; Lissner, H.R. Biomecanichs of Human Motion; Mexico-Trillas: Mexico City, Mexico, 1991; ISBN 9682433088. [Google Scholar]
- Wong, C.; Stilling, M. Polyethylene wear in total hip arthroplasty for suboptimal acetabular cup positions and for different polyethylene types: Experimental evaluation of wear simulation by finite element analysis using clinical radiostereometric measurements. In Tribology in Total Hip Arthroplasty; Springer: Berlin/Heidelberg, Germany, 2011; pp. 135–158. [Google Scholar]
- Shen, F.-W.; Lu, Z.; McKellop, H.A. Wear versus thickness and other features of 5-Mrad crosslinked UHMWPE acetabular liners. Clin. Orthop. Relat. Res. 2011, 469, 395–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartofilakidis, G.; Georgiades, G.; Babis, G.C. A comparison of the outcome of cemented all-polyethylene and cementless metal-backed acetabular sockets in primary total hip arthroplasty. J. Arthroplast. 2009, 24, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.H. Results of uncemented cups: A critical appraisal at 15 years. Clin. Orthop. Relat. Res. 2003, 121–125. [Google Scholar] [CrossRef]
- Bartel, D.L.; Burstein, A.H.; Toda, M.D.; Edwards, D.L. The effect of conformity and plastic thickness on contact stresses in metal-backed plastic implants. J. Biomech. Eng. 1985, 107, 193–199. [Google Scholar] [CrossRef]
- Georgiades, G.; Babis, G.C.; Kourlaba, G.; Hartofilakidis, G. Effect of cementless acetabular component orientation, position, and containment in total hip arthroplasty for congenital hip disease. J. Arthroplast. 2010, 25, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Gallo, J.; Havranek, V.; Zapletalova, J. Risk factors for accelerated polyethylene wear and osteolysis in ABG i total hip arthroplasty. Int. Orthop. 2010, 34, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karydakis, G.; Karachalios, T. Comparative In Vivo Wear Measurement of Conventional and Modern Bearing Surfaces in Total Hip Replacements by the Use of POLYWARE® Computerized System. In Tribology in Total Hip Arthroplasty; Springer: Berlin/Heidelberg, Germany, 2011; pp. 217–228. [Google Scholar]
- Sato, T.; Nakashima, Y.; Akiyama, M.; Yamamoto, T.; Mawatari, T.; Itokawa, T.; Ohishi, M.; Motomura, G.; Hirata, M.; Iwamoto, Y. Wear resistant performance of highly cross-linked and annealed ultra-high molecular weight polyethylene against ceramic heads in total hip arthroplasty. J. Orthop. Res. 2012, 30, 2031–2037. [Google Scholar] [CrossRef]
- Garvin, K.L.; White, T.C.; Dusad, A.; Hartman, C.W.; Martell, J. Low Wear Rates Seen in THAs With Highly Crosslinked Polyethylene at 9 to 14 Years in Patients Younger Than Age 50 Years. Clin. Orthop. Relat. Res. 2015, 473, 3829–3835. [Google Scholar] [CrossRef]
- Teeter, M.G.; MacLean, C.J.; Somerville, L.E.; Howard, J.L.; McCalden, R.W.; Lanting, B.A.; Vasarhelyi, E.M. Wear performance of cobalt chromium, ceramic, and oxidized zirconium on highly crosslinked polyethylene at mid-term follow-up. J. Orthop. 2018, 15, 620–623. [Google Scholar] [CrossRef]
- Bragdon, C.R.; Doerner, M.; Martell, J.; Jarrett, B.; Palm, H.; Multicenter Study Group; Malchau, H. The 2012 John Charnley Award: Clinical multicenter studies of the wear performance of highly crosslinked remelted polyethylene in THA. Clin. Orthop. Relat. Res. 2013, 471, 393–402. [Google Scholar] [CrossRef] [Green Version]
- Lachiewicz, P.F.; Soileau, E.S.; Martell, J.M. Wear and Osteolysis of Highly Crosslinked Polyethylene at 10 to 14 Years: The Effect of Femoral Head Size. Clin. Orthop. Relat. Res. 2016, 474, 365–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muratoglu, O.K.; Bragdon, C.R.; O’Connor, D.; Perinchief, R.S.; Estok, D.M.; Jasty, M.; Harris, W.H. Larger diameter femoral heads used in conjunction with a highly cross-linked ultra-high molecular weight polyethylene: A new concept. J. Arthroplast. 2001, 16, 24–30. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) | |||||||||||||
| E 1 (MPa) | G 2 (MPa) | Ν 3 | Fy 4 (MPa) | fu 5 (MPa) 2 | Strain Max (%) | ||||||||
| 940 | 322 | 0.46 | 25 | 40 | 500 | ||||||||
| 1 Modulus of Elasticity; 2 Modulus of Rigidity; 3 Ratio of Poisson; 4 Yield Strenght; 5 Ultimate Strenght. | |||||||||||||
| (b) | |||||||||||||
| Material | E 1 (GPa) | ν 2 | μ (32) 3 | μ (36) 4 | |||||||||
| CoCr | 210 | 0.30 | 0.133 | 0.14 | |||||||||
| ZrO2 | 358 | 0.24 | 0.096 | 0.085 | |||||||||
| 1 Modulus of Elasticity; 2 Ratio of Poisson; 3 Fricction Coeffient for 32 mm of femoral head; 4 Fricction Coeffient for 36 mm of femoral head. | |||||||||||||
| (c) | |||||||||||||
| Cervical-Diaphyseal Angle | COR 1 | a 2 (mm) | b 3 (mm) | h 4 (mm) | α 5 (◦) | β 6 (◦) | M 7 (N) | R 8 (N) | |||||
| SL 9 | 53 | 125 | 45.23 | 71 | 13.98 | 1879.33 | 2531.98 | ||||||
| Normal | CT 10 | 68 | 110 | 64.30 | 71 | 12.01 | 1163.38 | 1819.85 | |||||
| SM 11 | 83 | 95 | 73.79 | 71 | 10.72 | 877.78 | 1526.77 | ||||||
| SL | 65 | 125 | 46.34 | 52 | 27.98 | 1834.38 | 2406.92 | ||||||
| Varus | CT | 80 | 110 | 63.04 | 52 | 24.34 | 1186.83 | 1772.53 | |||||
| SM | 95 | 95 | 69.98 | 52 | 21.99 | 923.15 | 1517.88 | ||||||
| SL | 35 | 125 | 29.35 | 78 | 9.73 | 2895.92 | 3563.87 | ||||||
| Valgus | CT | 50 | 110 | 48.91 | 78 | 8.31 | 1529.42 | 2199.11 | |||||
| SM | 65 | 95 | 58.70 | 78 | 7.42 | 1100.58 | 1771.38 | ||||||
| 1 Center of Rotation; 2 Horizontal distance between COR and vector of gluteus medius; 3 Horizontal distance between COR and body weight vector; 4 Perpendicular distance between COR and vector of gluteus medius; 5 Gluteus medius vector angle with horizontal axis; 6 Total force vector angle with vertical axis; 7 Gluteus medius vector; 8 Total force vector; 9 Super Lateral COR location; 10 Centered COR location; 11 Super Medial COR location. | |||||||||||||
| Liner Thickness (mm) | Femoral Head (mm) | Element Type/Mesh Quality | Elements Size (mm) | Total Elements | Total Nodes | Element Acept. Ratio < 3 (%) |
|---|---|---|---|---|---|---|
| 5.3 | 32 | Solid Tetrahedron/High quality | 1.14319 | 55,010 | 82,156 | 99.1 |
| 7.3 | 77,960 | 113,960 | 99.1 | |||
| 11.3 | 137,728 | 196,708 | 99.5 | |||
| 5.3 | 36 | 66,777 | 99,442 | 99.1 | ||
| 7.3 | 95,977 | 139,850 | 99.3 | |||
| 11.3 | 159,946 | 228,141 | 99.5 |
| (a) | ||||||
| R | R Square | Adjusted R Square | Std. Error of the Estimate | |||
| 0.755 | 0.570 | 0.558 | 4.409221380 | |||
| (b) | ||||||
| Sum of Squares | df | Mean Square | F | p-value | ||
| Regression | 5394.873 | 6 | 899.146 | 46.249 | <0.0001 | |
| Residual | 4063.218 | 209 | 19.441 | - | - | |
| Total | 9458.091 | 215 | - | - | - | |
| (c) | ||||||
| B | Std. Error | Beta | t | p-value | ||
| (Constant) | 23.240 | 5.417 | 4.290 | <0.0001 | ||
| Acetabular Fixation | 8.303 | 0.600 | 0.627 | 13.837 | <0.0001 | |
| Cervical-Diaphyseal Angle | 1.711 | 0.367 | 0.211 | 4.656 | <0.0001 | |
| Thickness Liner | −2.321 | 0.367 | −0.286 | −6.317 | <0.0001 | |
| COR | −0.986 | 0.367 | −0.122 | −2.684 | 0.008 | |
| Head Material | −1.521 | 0.600 | −0.115 | −2.536 | 0.012 | |
| Head Diameter | −0.493 | 0.150 | −0.149 | −3.287 | 0.001 | |
| Author | COR (L) | COR (S) | Thickness | Head Size | Head Material |
|---|---|---|---|---|---|
| Gerogiades, 2010 | 0.001 | 0.049 | - | - | - |
| Hirakawa, 2001 | <0.0001 | 0.39 | - | - | - |
| Sato, 2012 | - | - | - | - | 0.45 |
| Garvin, 2015 | - | - | - | - | 0.58 |
| Gwynne-Jones, 2009 | - | - | - | 0.21 | 0.6 |
| Bragdon, 2012 | - | - | - | 0.23–0.90 | - |
| Lachiewicz, 2016 | - | - | - | 0.593 | - |
| Teeter, 2018 | - | - | - | <0.001/0.055 | 0.316 |
| Astion, 1996 | - | - | 0.03 | - | - |
| Shen, 2011 | - | - | 0.17 | 0.19–0.64 | - |
| Current study | <0.0001 | 0.001 | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Bravo, C.; Ortega, M.A.; Buján, J.; Torre, B.d.l.; Barrios, L. Wear Risk Prevention and Reduction in Total Hip Arthroplasty. A Personalized Study Comparing Cement and Cementless Fixation Techniques Employing Finite Element Analysis. J. Pers. Med. 2021, 11, 780. https://doi.org/10.3390/jpm11080780
González-Bravo C, Ortega MA, Buján J, Torre Bdl, Barrios L. Wear Risk Prevention and Reduction in Total Hip Arthroplasty. A Personalized Study Comparing Cement and Cementless Fixation Techniques Employing Finite Element Analysis. Journal of Personalized Medicine. 2021; 11(8):780. https://doi.org/10.3390/jpm11080780
Chicago/Turabian StyleGonzález-Bravo, Carlos, Miguel A. Ortega, Julia Buján, Basilio de la Torre, and Loreto Barrios. 2021. "Wear Risk Prevention and Reduction in Total Hip Arthroplasty. A Personalized Study Comparing Cement and Cementless Fixation Techniques Employing Finite Element Analysis" Journal of Personalized Medicine 11, no. 8: 780. https://doi.org/10.3390/jpm11080780