
Review on Perioperative and Oncological Outcomes of Robotic Gastrectomy for Cancer

Abstract
:1. Introduction
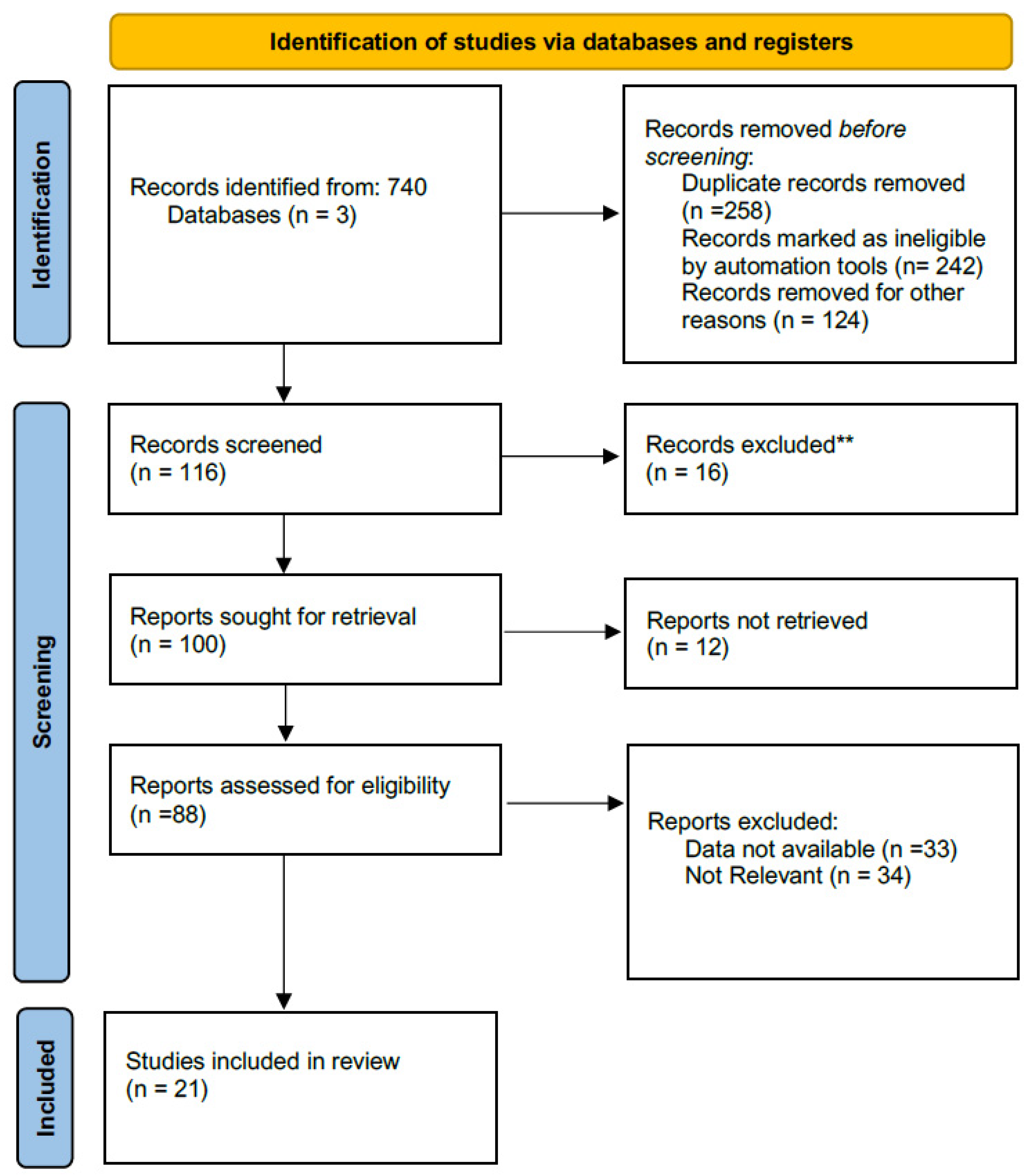
2. Methods
- inclusion of adult patients undergoing robotic or laparoscopic total or distal gastrectomy for gastric cancer;
- robotic and standard laparoscopic approach comparator intervention;
- data on perioperative, post-operative, and oncological outcomes.
3. Results
3.1. Perioperative Details
3.2. Postoperative Outcomes
3.3. Oncological Outcomes
3.4. Costs
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kim, H.H.; Han, S.U.; Kim, M.C.; Kim, W.; Lee, H.J.; Ryu, S.W.; Cho, G.S.; Kim, C.Y.; Yang, H.-K.; Park, D.J.; et al. Effect of laparoscopic distal gastrectomy vs open distal gastrectomy on long-term surviv-al among patients with stage I gastric cancer: The KLASS-01 randomized clinical trial. JAMA Oncol. 2019, 5, 506–513. [Google Scholar] [CrossRef]
- Liu, F.; Huang, C.; Xu, Z.; Su, X.; Zhao, G.; Ye, J.; Du, X.; Huang, H.; Hu, J.; Li, G.; et al. Chinese Laparoscopic Gastrointestinal Surgery Study (CLASS) Group. Morbidity and Mortality of Laparoscopic vs Open Total Gastrectomy for Clinical Stage I Gastric Cancer: The CLASS02 Multicenter Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1590–1597. [Google Scholar] [CrossRef]
- Bracale, U.; Merola, G.; Pignata, G.; Andreuccetti, J.; Dolce, P.; Boni, L.; Cassinotti, E.; Olmi, S.; Uccelli, M.; Gualtierotti, M.; et al. Laparoscopic gastrectomy for stage II and III advanced gastric cancer: Long-term follow-up data from a Western multicenter retrospective study. Surg. Endosc. 2021, 1–12. [Google Scholar] [CrossRef]
- Bolger, J.C.; Al Azzawi, M.; Whooley, J.; Bolger, E.M.; Trench, L.; Allen, J.; Kelly, M.E.; Brosnan, C.; Arumugasamy, M.; Robb, W.B. Surgery by a minimally invasive approach is associated with improved textbook outcomes in oesophageal and gastric cancer. Eur. J. Surg. Oncol. 2021, 17. [Google Scholar] [CrossRef]
- Shin, H.-J.; Son, S.-Y.; Wang, B.; Roh, C.K.; Hur, H.; Han, S.-U. Long-term Comparison of Robotic and Laparoscopic Gastrectomy for Gastric Cancer. Ann. Surg. 2021, 274, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Hendriksen, B.S.; Brooks, A.J.; Hollenbeak, C.S.; Taylor, M.D.; Reed, M.F.; Soybel, D.I. The Impact of Minimally Invasive Gastrectomy on Survival in the USA. J. Gastrointest. Surg. 2019, 24, 1000–1009. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology (Version 2.2021) for Gastric Cancer. Available online: http://www.nccn.org/professionals/physician_gls/PDF/occult.pdf (accessed on 3 April 2021).
- Hikage, M.; Fujiya, K.; Kamiya, S.; Tanizawa, Y.; Bando, E.; Notsu, A.; Mori, K.; Terashima, M. Robotic Gastrectomy Compared with Laparoscopic Gastrectomy for Clinical Stage I/II Gastric Cancer Patients: A Propensity Score-Matched Analysis. World J. Surg. 2021, 1–12. [Google Scholar] [CrossRef]
- Park, Y.K.; Yoon, H.M.; Kim, Y.-W.; Park, J.Y.; Ryu, K.W.; Lee, Y.-J.; Jeong, O.; Yoon, K.Y.; Lee, J.H.; Lee, S.E.; et al. Laparoscopy-assisted versus Open D2 Distal Gastrectomy for Advanced Gastric Cancer. Ann. Surg. 2018, 267, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Giulianotti, P.C.; Coratti, A.; Angelini, M.; Sbrana, F.; Cecconi, S.; Balestracci, T.; Caravaglios, G. Robotics in general surgery: Per-sonal experience in a large community hospital. Arch. Surg. 2003, 138, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashizume, M.; Sugimachi, K. Robot-assisted gastric surgery. Surg. Clin. N. Am. 2003, 83, 1429–1444. [Google Scholar] [CrossRef]
- Stewart, C.L.; Ituarte, P.H.G.; Melstrom, K.A.; Warner, S.G.; Melstrom, L.G.; Lai, L.L.; Fong, Y.; Woo, Y. Robotic surgery trends in general surgical oncology from the National Inpatient Sample. Surg. Endosc. 2018, 33, 2591–2601. [Google Scholar] [CrossRef]
- Guerrini, G.P.; Esposito, G.; Magistri, P.; Serra, V.; Guidetti, C.; Olivieri, T.; Catellani, B.; Assirati, G.; Ballarin, R.; Di Sandro, S.; et al. Robotic versus laparoscopic gastrectomy for gastric cancer: The largest meta-analysis. Int. J. Surg. 2020, 82, 210–228. [Google Scholar] [CrossRef]
- Kim, Y.M.; Hyung, W.J. Current status of robotic gastrectomy for gastric cancer: Comparison with laparoscopic gastrectomy. Updat. Surg. 2021, 73, 853–863. [Google Scholar] [CrossRef]
- Gao, Y.; Xi, H.; Qiao, Z.; Li, J.; Zhang, K.; Xie, T.; Shen, W.; Cui, J.; Wei, B.; Chen, L. Comparison of robotic- and laparoscopic-assisted gastrectomy in advanced gastric cancer: Up-dated short- and long-term results. Surg. Endosc. 2019, 33, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Amore Bonapasta, S.; Guerra, F.; Linari, C.; Annecchiarico, M.; Boffi, B.; Calistri, M.; Coratti, A. Robot-assisted gastrectomy for cancer. Chirurg 2017, 88 (Suppl. 1), 12–18. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Wu, H.-Y.; Lin, X.-F.; Li, W. Pooled analysis of the oncological outcomes in robotic gastrectomy versus laparoscopic gastrectomy for gastric cancer. J. Minimal Access Surg. 2021, 17, 287. [Google Scholar] [CrossRef] [PubMed]
- Bobo, Z.; Xin, W.; Jiang, L.; Quan, W.; Liang, B.; Xiangbing, D.; Ziqiang, W. Robotic gastrectomy versus laparoscopic gastrectomy for gastric cancer: Meta-analysis and trial sequential analysis of prospective observational studies. Surg. Endosc. 2019, 33, 1033–1048. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Liu, H.; Kinoshita, T.; Tonouchi, A.; Kaito, A.; Tokunaga, M. What are the reasons for a longer operation time in robotic gastrectomy than in laparoscopic gastrectomy for stomach cancer? Surg. Endosc. 2019, 33, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Nakauchi, M.; Vos, E.; Janjigian, Y.Y.; Ku, G.Y.; Schattner, M.A.; Nishimura, M.; Gonen, M.; Coit, D.G.; Strong, V.E. Comparison of Long- and Short-term Outcomes in 845 Open and Minimally Invasive Gastrectomies for Gastric Cancer in the United States. Ann. Surg. Oncol. 2021, 28, 3532–3544. [Google Scholar] [CrossRef]
- Chen, K.; Pan, Y.; Zhang, B.; Maher, H.; Wang, X.F.; Cai, X.J. Robotic versus laparoscopic Gastrectomy for gastric cancer: A system-atic review and updated meta-analysis. BMC Surg. 2017, 17, 93. [Google Scholar] [CrossRef]
- Pan, H.F.; Wang, G.; Liu, J.; Liu, X.X.; Zhao, K.; Tang, X.F.; Jiang, Z.W. Robotic versus laparoscopic gastrectomy for locally advanced gastric cancer. Surg. Laparosc. Endosc. Percutan. Tech. 2017, 27, 428–433. [Google Scholar] [CrossRef]
- Lu, J.; Wu, D.; Wang, H.-G.; Zheng, C.-H.; Li, P.; Xie, J.-W.; Wang, J.-B.; Lin, J.-X.; Chen, Q.-Y.; Cao, L.-L.; et al. 114O Assessment of robotic versus laparoscopic distal gastrectomy for gastric cancer: A randomized controlled trial. Ann. Oncol. 2020, 31, S1287. [Google Scholar] [CrossRef]
- Tian, Y.; Cao, S.; Kong, Y.; Shen, S.; Niu, Z.; Zhang, J.; Chen, D.; Jiang, H.; Lv, L.; Liu, X.; et al. Short- and long-term comparison of robotic and laparoscopic gastrectomy for gastric cancer by the same surgical team: A propensity score matching analysis. Surg. Endosc. 2021, 1–11. [Google Scholar] [CrossRef]
- Kinoshita, T.; Sato, R.; Akimoto, E.; Tanaka, Y.; Okayama, T.; Habu, T. Reduction in postoperative complications by robotic surgery: A case–control study of robotic versus conventional laparoscopic surgery for gastric cancer. Surg. Endosc. 2021, 1–10. [Google Scholar] [CrossRef]
- Li, Z.-Y.; Zhao, Y.-L.; Qian, F.; Tang, B.; Chen, J.; He, T.; Luo, Z.-Y.; Li, P.-A.; Shi, Y.; Yu, P.-W. Long-term oncologic outcomes of robotic versus laparoscopic gastrectomy for locally advanced gastric cancer: A propensity score-matched analysis of 1170 patients. Surg. Endosc. 2021, 1–10. [Google Scholar] [CrossRef]
- Alhossaini, R.M.; Altamran, A.A.; Cho, M.; Roh, C.K.; Seo, W.J.; Choi, S.; Son, T.; Kim, H.; Hyung, W.J. Lower rate of conversion using robotic-assisted surgery compared to lapa-roscopy in completion total gastrectomy for remnant gastric cancer. Surg. Endosc. 2020, 34, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.-J.; Li, H.-T.; Yu, J.-P.; Su, L.; Guo, C.; Chen, P.; Yan, L.; Li, K.; Ma, Y.-W.; Wang, L.; et al. Severity and incidence of complications assessed by the Clavien–Dindo classification following robotic and laparoscopic gastrectomy for advanced gastric cancer: A retrospective and propensity score-matched study. Surg. Endosc. 2018, 33, 3341–3354. [Google Scholar] [CrossRef]
- Choi, S.; Song, J.H.; Lee, S.; Cho, M.; Kim, Y.M.; Hyung, W.J.; Kim, H.-I. Surgical Merits of Open, Laparoscopic, and Robotic Gastrectomy Techniques with D2 Lymphadenectomy in Obese Patients with Gastric Cancer. Ann. Surg. Oncol. 2021, 1–10. [Google Scholar] [CrossRef]
- Uyama, I.; Suda, K.; Nakauchi, M.; Kinoshita, T.; Noshiro, H.; Takiguchi, S.; Ehara, K.; Obama, K.; Kuwabara, S.; Okabe, H.; et al. Clinical advantages of robotic gastrectomy for clinical stage I/II gastric cancer: A multi-institutional prospective sin-gle-arm study. Gastric Cancer 2019, 22, 377–385. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.I.; Han, S.U.; Yang, H.K.; Kim, Y.W.; Lee, H.J.; Ryu, K.W.; Park, J.M.; An, J.Y.; Kim, M.C.; Park, S.; et al. Multicenter Prospective Comparative Study of Robotic Versus Laparoscopic Gas-trectomy for Gastric Adenocarcinoma. Ann. Surg. 2016, 263, 103–109. [Google Scholar] [CrossRef]
- Xie, F.-N.; Chen, J.; Li, Z.-Y.; Bai, B.; Song, D.; Xu, S.; Song, X.-T.; Ji, G. Impact of Laparoscopic Converted to Open Gastrectomy on Short- and Long-Term Outcomes of Patients with Locally Advanced Gastric Cancer: A Propensity Score-Matched Analysis. J. Gastrointest. Surg. 2021, 1–11. [Google Scholar] [CrossRef]
- Guerra, F.; Giuliani, G.; Coletta, D. The risk of conversion in minimally invasive oncological abdominal surgery. Me-ta-analysis of randomized evidence comparing traditional laparoscopic versus robot-assisted techniques. Langenbecks Arch. Surg. 2021, 406, 607–612. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Coletta, D.; Sandri, G.B.L.; Giuliani, G.; Guerra, F. Robot-assisted versus conventional laparoscopic major hepatectomies: Systematic review with meta-analysis. Int. J. Med Robot. Comput. Assist. Surg. 2021, 17. [Google Scholar] [CrossRef] [PubMed]
- Cortolillo, N.; Patel, C.; Parreco, J.; Kaza, S.; Castillo, A. Nationwide outcomes and costs of laparoscopic and robotic vs. open hepatectomy. J. Robot. Surg. 2018, 13, 557–565. [Google Scholar] [CrossRef]
- Park, S.H.; Hyung, W.J. Current perspectives on the safety and efficacy of robot-assisted surgery for gastric cancer. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Amore Bonapasta, S.; Checcacci, P.; Guerra, F.; Mirasolo, V.M.; Moraldi, L.; Ferrara, A.; Annecchiarico, M.; Coratti, A. Time-to-administration in postoperative chemotherapy for colorectal cancer: Does minimally-invasive surgery help? Minerva Chir. 2016, 71, 173–179. [Google Scholar] [PubMed]
- van Boxel, G.I.; Ruurda, J.P.; van Hillegersberg, R. Robotic-assisted gastrectomy for gastric cancer: A European perspective. Gastric Cancer 2019, 22, 909–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, F.; Giuliani, G.; Formisano, G.; Bianchi, P.P.; Patriti, A.; Coratti, A. Pancreatic Complications After Conventional Laparo-scopic Radical Gastrectomy Versus Robotic Radical Gastrectomy: Systematic Review and Meta-Analysis. J. Laparoendosc Adv. Surg. Tech. A 2018, 28, 1207–1215. [Google Scholar] [CrossRef]
- Seo, H.S.; Shim, J.H.; Jeon, H.M.; Park, C.H.; Song, K.Y. Postoperative pancreatic fistula after robot distal gastrectomy. J. Surg. Res. 2015, 194, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Kwon, I.G.; Son, T.; Kim, H.I.; Hyung, W.J. Fluorescent lymphography-guided lymphadenectomy during robotic radical gastrec-tomy for gastric cancer. JAMA Surg. 2019, 154, 150–158. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Year | Study | Origin | Approach | n. Patients | Type of Resection |
|---|---|---|---|---|---|---|
| Kim HI et al. | 2016 | Prospective | Korea | LG/RG | 434 | TG/DG/PPG/PG |
| Chen K et al. | 2017 | Mata–Analysis | China | LG/RG | 5953 | TG/DG/PG |
| Pan HF et al. | 2017 | RCT | China | LG/RG | 163 | TG/DG/PG |
| Hendriksen BS et al. | 2018 | Retrospective | USA | LG/RG/OG | 17.449 | TG/ DG |
| Liu H et al. | 2019 | Retrospective | China | LG/RG | 20 | DG |
| Wang WJ et al. | 2018 | Retrospective | China | LG/RG | 527 | TG/DG |
| Uyama I et al. | 2018 | Prospective | Japan | RG | 326 | TG/DG/PG |
| Gao, Y Q et al. | 2019 | Retrospective | China | LG/RG | 502 | TG/DG/PG |
| Bobo Z et al. | 2019 | Mata–Analysis | China | LG/RG | 4576 | TG/DG |
| Hikage M et al. | 2020 | Retrospective | Japan | LG/RG | 1208 | TG / DG/PPG/PG |
| Guerrini GP et al. | 2020 | Mata–Analysis | Italy | LG/RG | 17.712 | TG/DG/PPG/PG |
| Yang P. et al. | 2020 | Mata–Analysis | China | LG/RG | 4142 | TG/DG |
| Li ZY et al. | 2020 | Retrospective | China | LG/RG | 1476 | DG |
| Alhossaini RM et al. | 2020 | Retrospective | Korea | LG/RG | 55 | CG |
| Bolger JC et al. | 2021 | Retrospective | Ireland | LG | 258 | TG/DG |
| Shin HJ et al. | 2021 | Retrospective | Korea | LG / RG | 2084 | TG/ DG |
| Nakauchi M et al. | 2021 | Retrospective | USA | LG/RG/OG | 845 | TG/DG/PG |
| Lu J et al. | 2021 | RCT | China | LG/RG | 300 | DG |
| Tian Y et al. | 2021 | Retrospective | China | LG/RG | 1686 | TG/DG |
| Kinoshita T et al. | 2021 | Retrospective | Japan | LG/RG | 1172 | TG/DG/PPG/PG |
| Choi S et al. | 2021 | Retrospective | Korea | LG/RG/OG | 185 | TG/DG |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giuliani, G.; Guerra, F.; De Franco, L.; Salvischiani, L.; Benigni, R.; Coratti, A. Review on Perioperative and Oncological Outcomes of Robotic Gastrectomy for Cancer. J. Pers. Med. 2021, 11, 638. https://doi.org/10.3390/jpm11070638
Giuliani G, Guerra F, De Franco L, Salvischiani L, Benigni R, Coratti A. Review on Perioperative and Oncological Outcomes of Robotic Gastrectomy for Cancer. Journal of Personalized Medicine. 2021; 11(7):638. https://doi.org/10.3390/jpm11070638
Chicago/Turabian StyleGiuliani, Giuseppe, Francesco Guerra, Lorenzo De Franco, Lucia Salvischiani, Roberto Benigni, and Andrea Coratti. 2021. "Review on Perioperative and Oncological Outcomes of Robotic Gastrectomy for Cancer" Journal of Personalized Medicine 11, no. 7: 638. https://doi.org/10.3390/jpm11070638