
Salivary DNA Methylation as an Epigenetic Biomarker for Head and Neck Cancer. Part I: A Diagnostic Accuracy Meta-Analysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Strategy and Study Selection
2.3. Selection Criteria
2.4. Data Extraction
2.5. Quality Assessment of Individual Studies
2.6. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Quality Assessment of the Included Studies
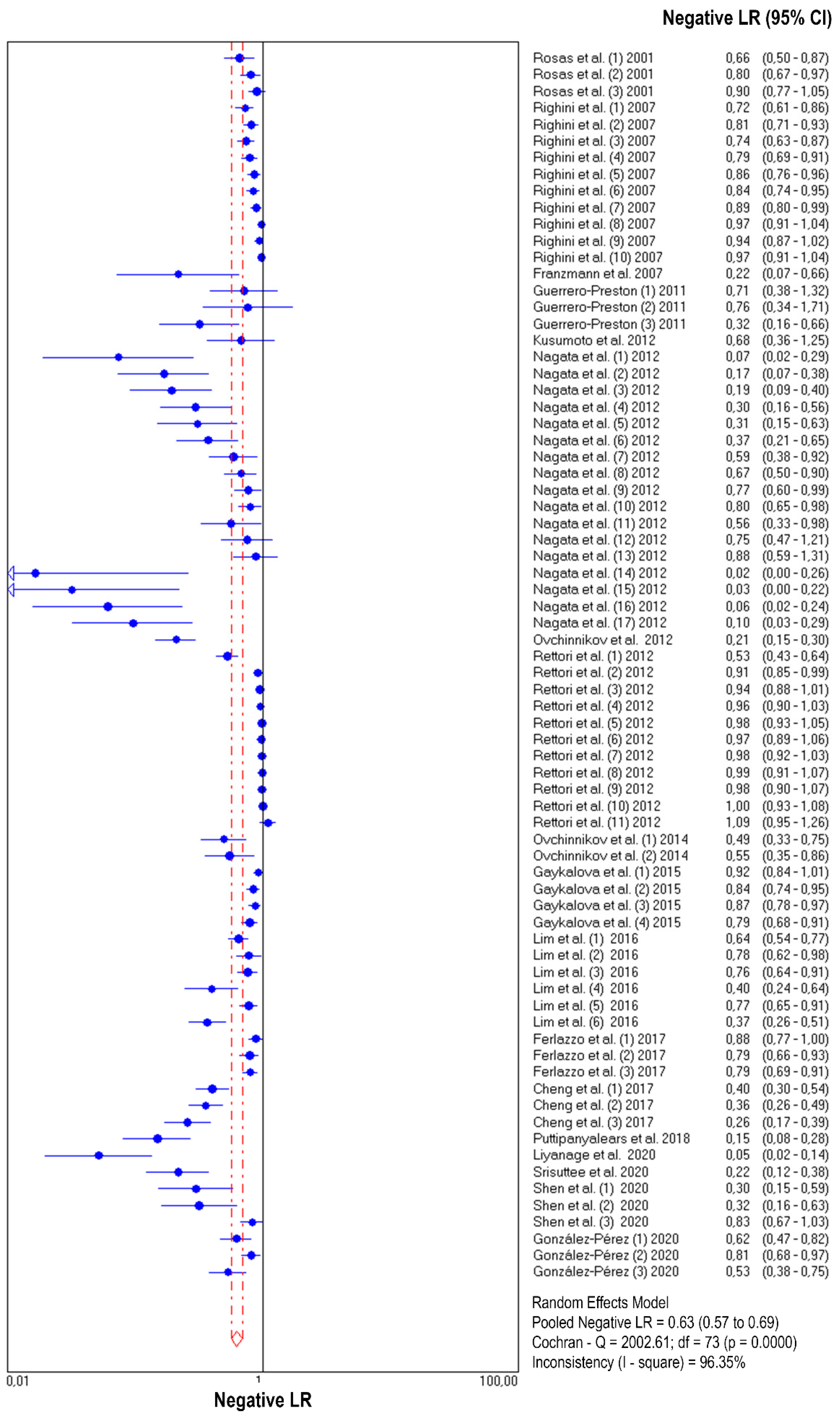
3.4. Diagnostic Accuracy of Salivary DNA Promoter Hypermethylation
3.5. Heterogeneity and Subgroup Analysis
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Leemans, C.R.; Snijders, P.J.F.; Brakenhoff, R.H. The molecular landscape of head and neck cancer. Nat. Rev. Cancer 2018, 18, 269–282. [Google Scholar] [CrossRef]
- Sacco, A.G.; Cohen, E.E. Current treatment options for recurrent or metastatic head and neck squamous cell carcinoma. J. Clin. Oncol. 2015, 33, 3305–3313. [Google Scholar] [CrossRef] [PubMed]
- Feller, L.; Altini, M.; Lemmer, J. Inflammation in the context of oral cancer. Oral Oncol. 2013, 49, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.A.; Baylin, S.B. The fundamental role of epigenetic events in cancer. Nat. Rev. Genet. 2002, 3, 415–428. [Google Scholar] [CrossRef] [PubMed]
- Darwiche, N. Epigenetic mechanisms and the hallmarks of cancer: An intimate affair. Am. J. Cancer Res. 2020, 10, 1954–1978. [Google Scholar] [PubMed]
- Castilho, R.M.; Squarize, C.H.; Almeida, L.O. Epigenetic modifications and head and neck cancer: Implications for tumor progression and resistance to therapy. Int. J. Mol. Sci. 2017, 18, 1506. [Google Scholar] [CrossRef]
- Garinis, G.A.; Patrinos, G.P.; Spanakis, N.E.; Menounos, P.G. DNA hypermethylation: When tumour suppressor genes go silent. Hum. Genet. 2002, 111, 115–127. [Google Scholar] [CrossRef]
- Misawa, K.; Imai, A.; Matsui, H.; Kanai, A.; Misawa, Y.; Mochizuki, D.; Mima, M.; Yamada, S.; Kurokawa, T.; Nakagawa, T.; et al. Identification of novel methylation markers in HPV-associated oropharyngeal cancer: Genome-wide discovery, tissue verification and validation testing in ctDNA. Oncogene 2020, 39, 4741–4755. [Google Scholar] [CrossRef]
- Liyanage, C.; Wathupola, A.; Muraleetharan, S.; Perera, K.; Punyadeera, C.; Udagama, P. Promoter hypermethylation of tumor-suppressor genes p16INK4a, RASSF1A, TIMP3, and PCQAP/MED15 in salivary DNA as a quadruple biomarker panel for early detection of oral and oropharyngeal cancers. Biomolecules 2019, 9, 148. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.; Wan, Y.; Vagenas, D.; Ovchinnikov, D.A.; Perry, C.F.L.; Davis, M.J.; Punyadeera, C. Salivary DNA methylation panel to diagnose HPV-positive and HPV-negative head and neck cancers. BMC Cancer 2016, 16, 749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerrero-Preston, R.; Soudry, E.; Acero, J.; Orera, M.; Moreno-López, L.; Macía-Colón, G.; Jaffe, A.; Berdasco, M.; Ili-Gangas, C.; Brebi-Mieville, P.; et al. NID2 and HOXA9 promoter hypermethylation as biomarkers for prevention and early detection in oral cavity squamous cell carcinoma tissues and saliva. Cancer Prev. Res. 2011, 4, 1061–1072. [Google Scholar] [CrossRef] [Green Version]
- Herman, J.G.; Baylin, S.B. Gene silencing in cancer in association with promoter hypermethylation. N. Engl. J. Med. 2003, 349, 2042–2054. [Google Scholar] [CrossRef]
- Borchiellini, M.; Ummarino, S.; Di Ruscio, A. The bright and dark side of DNA methylation: A matter of balance. Cells 2019, 8, 1243. [Google Scholar] [CrossRef] [Green Version]
- Kulis, M.; Esteller, M. DNA methylation and cancer. Adv. Genet. 2010, 70, 27–56. [Google Scholar] [CrossRef]
- Esteller, M.; Corn, P.G.; Baylin, S.B.; Herman, J.G. A gene hypermethylation profile of human cancer. Cancer Res. 2001, 61, 3225–3229. [Google Scholar] [PubMed]
- O’Reilly, E.; Tuzova, A.V.; Walsh, A.L.; Russell, N.M.; O’Brien, O.; Kelly, S.; Dhomhnallain, O.N.; DeBarra, L.; Dale, C.M.; Brugman, R.; et al. epiCaPture: A urine DNA methylation test for early detection of aggressive prostate cancer. JCO Precis. Oncol. 2019, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Zhao, Y.; Huang, W.; Gao, Y.; Xu, W.; Tao, J.; Yang, M.; Li, L.; Ping, W.; Shen, H.; et al. Non-invasive diagnosis of early-stage lung cancer using high-throughput targeted DNA methylation sequencing of circulating tumor DNA (ctDNA). Theranostics 2019, 9, 2056–2070. [Google Scholar] [CrossRef]
- Smith, A.K.; Kilaru, V.; Klengel, T.; Mercer, K.B.; Bradley, B.; Conneely, K.N.; Ressler, K.J.; Binder, E.B. DNA extracted from saliva for methylation studies of psychiatric traits: Evidence tissue specificity and relatedness to brain. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2015, 168, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Hearn, N.L.; Coleman, A.S.; Ho, V.; Chiu, C.L.; Lind, J.M. Comparing DNA methylation profiles in saliva and intestinal mucosa. BMC Genomics 2019, 20, 163. [Google Scholar] [CrossRef]
- Wu, H.C.; Wang, Q.; Chung, W.K.; Andrulis, I.L.; Daly, M.B.; John, E.M.; Keegan, T.H.; Knight, J.; Bradbury, A.R.; Kappil, M.A.; et al. Correlation of DNA methylation levels in blood and saliva DNA in young girls of the LEGACY girls study. Epigenetics 2014, 9, 929–933. [Google Scholar] [CrossRef] [Green Version]
- Thompson, T.M.; Sharfi, D.; Lee, M.; Yrigollen, C.M.; Naumova, O.Y.; Grigorenko, E.L. Comparison of whole-genome DNA methylation patterns in whole blood, saliva, and lymphoblastoid cell lines. Behav. Genet. 2013, 43, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langie, S.A.S.; Szarc Vel Szic, K.; Declerck, K.; Traen, S.; Koppen, G.; Van Camp, G.; Schoeters, G.; Vanden Berghe, W.; De Boever, P. Whole-genome saliva and blood DNA methylation profiling in individuals with a respiratory allergy. PLoS ONE 2016, 11, e0151109. [Google Scholar] [CrossRef]
- Carvalho, A.L.; Jeronimo, C.; Kim, M.M.; Henrique, R.; Zhang, Z.; Hoque, M.O.; Chang, S.; Brait, M.; Nayak, C.S.; Jiang, W.W.; et al. Evaluation of promoter hypermethylation detection in body fluids as a screening/diagnosis tool for head and neck squamous cell carcinoma. Clin. Cancer Res. 2008, 14, 97–107. [Google Scholar] [CrossRef] [Green Version]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; the PRISMA-DTA Group; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. Quadas-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Zamora, J.; Abraira, V.; Muriel, A.; Khan, K.; Coomarasamy, A. Meta-DiSc: A software for meta-analysis of test accuracy data. BMC Med. Res. Methodol. 2006, 6, 31. [Google Scholar] [CrossRef]
- Hellmich, M.; Lehmacher, W. A ruler for interpreting diagnostic test results. Methods Inf. Med. 2005, 44, 124–126. [Google Scholar]
- Deeks, J.J.; Macaskill, P.; Irwig, L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J. Clin. Epidemiol. 2005, 58, 882–893. [Google Scholar] [CrossRef]
- Rosas, S.L.; Koch, W.; da Costa Carvalho, M.G.; Wu, L.; Califano, J.; Westra, W.; Jen, J.; Sidransky, D. Promoter hypermethylation patterns of p16, O6-methylguanine-DNA-methyltransferase, and Death-associated protein kinase in tumors and saliva of head and neck cancer patients. Cancer Res. 2001, 61, 939–942. [Google Scholar] [PubMed]
- Kusumoto, T.; Hamada, T.; Yamada, N.; Nagata, S.; Kanmura, Y.; Houjou, I.; Kamikawa, Y.; Yonezawa, S.; Sugihara, K. Comprehensive Epigenetic Analysis Using Oral Rinse Samples: A Pilot Study. J. Oral Maxillofac. Surg. 2012, 70, 1486–1494. [Google Scholar] [CrossRef] [PubMed]
- Gaykalova, D.A.; Vatapalli, R.; Wei, Y.; Tsai, H.L.; Wang, H.; Zhang, C.; Hennessey, P.T.; Guo, T.; Tan, M.; Li, R.; et al. Outlier Analysis Defines Zinc Finger Gene Family DNA Methylation in Tumors and Saliva of Head and Neck Cancer Patients. PLoS ONE 2015, 10, e0142148. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.J.; Chang, C.F.; Ko, H.H.; Lee, J.J.; Chen, H.M.; Wang, H.J.; Lin, H.S.; Chiang, C.P. Hypermethylated ZNF582 and PAX1 genes in mouth rinse samples as biomarkers for oral dysplasia and oral cancer detection. Head Neck 2018, 40, 355–368. [Google Scholar] [CrossRef]
- Srisuttee, R.; Arayataweegool, A.; Mahattanasakul, P.; Tangjaturonrasme, N.; Kerekhanjanarong, V.; Keelawat, S.; Mutirangura, A.; Kitkumthorn, N. Evaluation of NID2 promoter methylation for screening of Oral squamous cell carcinoma. BMC Cancer 2020, 20, 218. [Google Scholar] [CrossRef]
- Nagata, S.; Hamada, T.; Yamada, N.; Yokoyama, S.; Kitamoto, S.; Kanmura, Y.; Nomura, M.; Kamikawa, Y.; Yonezawa, S.; Sugihara, K. Aberrant DNA methylation of tumor-related genes in oral rinse. Cancer 2012, 118, 4298–4308. [Google Scholar] [CrossRef]
- Franzmann, E.J.; Reategui, E.P.; Pedroso, F.; Pernas, F.G.; Karakullukcu, B.M.; Carraway, K.L.; Hamilton, K.; Singal, R.; Goodwin, W.J. Soluble CD44 is a potential marker for the early detection of head and neck cancer. Cancer Epidemiol. Biomarkers Prev. 2007, 16, 1348–1355. [Google Scholar] [CrossRef] [Green Version]
- Righini, C.A.; de Fraipont, F.; Timsit, J.F.; Faure, C.; Brambilla, E.; Reyt, E.; Favrot, M.C. Tumor-specific methylation in saliva: A promising biomarker for early detection of head and neck cancer recurrence. Clin. Cancer Res. 2007, 13, 1179–1185. [Google Scholar] [CrossRef] [Green Version]
- Ovchinnikov, D.A.; Cooper, M.A.; Pandit, P.; Coman, W.B.; Cooper-White, J.J.; Keith, P.; Wolvetang, E.J.; Slowey, P.D.; Punyadeera, C. Tumor-suppressor gene promoter hypermethylation in saliva of head and neck cancer patients. Transl. Oncol. 2012, 5, 321–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ovchinnikov, D.A.; Wan, Y.; Coman, W.B.; Pandit, P.; Cooper-White, J.J.; Herman, J.G.; Punyadeera, C. DNA methylation at the novel CpG sites in the promoter of MED15/PCQAP gene as a biomarker for head and neck cancers. Biomark. Insights 2014, 9, 53–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Pérez, L.; Isaza-Guzmán, D.; Arango-Pérez, E.; Tobón-Arroyave, S. Analysis of salivary detection of P16INK4A and RASSF1A promoter gene methylation and its association with oral squamous cell carcinoma in a Colombian population. J. Clin. Exp. Dent. 2020, e452–e460. [Google Scholar] [CrossRef] [PubMed]
- Puttipanyalears, C.; Arayataweegool, A.; Chalertpet, K.; Rattanachayoto, P.; Mahattanasakul, P.; Tangjaturonsasme, N.; Kerekhanjanarong, V.; Mutirangura, A.; Kitkumthorn, N. TRH site-specific methylation in oral and oropharyngeal squamous cell carcinoma. BMC Cancer 2018, 18, 786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlazzo, N.; Currò, M.; Zinellu, A.; Caccamo, D.; Isola, G.; Ventura, V.; Carru, C.; Matarese, G.; Ientile, R. Influence of MTHFR genetic background on p16 and MGMT methylation in oral squamous cell cancer. Int. J. Mol. Sci. 2017, 18, 724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, S.; Saito, Y.; Ren, S.; Liu, C.; Guo, T.; Qualliotine, J.; Khan, Z.; Sadat, S.; Califano, J.A. Targeting viral DNA and promoter hypermethylation in salivary rinses for recurrent HPV-positive oropharyngeal cancer. Otolaryngol. Neck Surg. 2020, 162, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Rettori, M.M.; de Carvalho, A.C.; Bomfim Longo, A.L.; de Oliveira, C.Z.; Kowalski, L.P.; Carvalho, A.L.; Vettore, A.L. Prognostic significance of TIMP3 hypermethylation in post-treatment salivary rinse from head and neck squamous cell carcinoma patients. Carcinogenesis 2013, 34, 20–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, E.N.S.; Acevedo, A.C.; Leite, A.F.; Gozal, D.; Chardin, H.; De Luca Canto, G. Diagnostic capability of salivary biomarkers in the assessment of head and neck cancer: A systematic review and meta-analysis. Oral Oncol. 2015, 51, 805–818. [Google Scholar] [CrossRef]
- Rapado-González, Ó.; Martínez-Reglero, C.; Salgado-Barreira, Á.; Takkouche, B.; López-López, R.; Suárez-Cunqueiro, M.M.; Muinelo-Romay, L. Salivary biomarkers for cancer diagnosis: A meta-analysis. Ann. Med. 2020, 52, 131–144. [Google Scholar] [CrossRef]
- Yoshizawa, J.M.; Schafer, C.A.; Schafer, J.J.; Farrell, J.J.; Paster, B.J.; Wong, D.T.W. Salivary biomarkers: Toward future clinical and diagnostic utilities. Clin. Microbiol. Rev. 2013, 26, 781–791. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Anatomic Tumor Location | Type of Sample | Method | Biomarker | Cancer Group N (M+) | Control Group N (M+) |
|---|---|---|---|---|---|---|
| Rosas 2001 | HNC | Oral rinse (NaCl) | MSP | p16 | 30 (11+) | 30 (1+) |
| DAPK | 30 (6+) | 30 (0+) | ||||
| MGMT | 30 (4+) | 30 (1+) | ||||
| Righini 2007 | HNC | Oral rinse (NaCl) | MSP | TIMP3 | 60 (17+) | 30 (0+) |
| ECAD | 60 (12+) | |||||
| p16 | 60 (16+) | |||||
| MGMT | 60 (13+) | |||||
| DAPK | 60 (9+) | |||||
| RASSF1A | 60 (10+) | |||||
| p15 | 60 (7+) | |||||
| p14 | 60 (2+) | |||||
| APC | 60 (4+) | |||||
| FHIT | 60 (2+) | |||||
| hMLH1 | 60 (0+) | |||||
| Franzmann 2007 | HNC | Oral rinse (NaCl) | MSP | CD44 | 11 (9+) | 10 (0+) |
| Guerrero-Preston 2011 | HNC | Oral rinse (NaCl) | qMSP | HOXA9 | 32 (20+) | 19 (9+) |
| NID2 | 32 (23+) | 19 (12+) | ||||
| HOXA9+NID2 | 32 (25+) | 19 (6+) | ||||
| OC | HOXA9 | 16 (11+) | 19 (9+) | |||
| NID2 | 16 (14+) | 19 (12+) | ||||
| HOXA9+NID2 | 16 (14+) | 19 (6+) | ||||
| OPC | HOXA9 | 16 (9+) | 19 (9+) | |||
| NID2 | 16 (9+) | 19 (12+) | ||||
| HOXA9+NID2 | 16 (11+) | 19 (6+) | ||||
| Nagata 2011 | OC | Oral rinse (NaCl) | MSP | ECAD | 34 (32+) | 24 (5+) |
| TMEFF2 | 34 (29+) | 24 (3+) | ||||
| RARβ | 34 (28+) | 24 (2+) | ||||
| MGMT | 34 (26+) | 24 (5+) | ||||
| FHIT | 34 (27+) | 24 (8+) | ||||
| WIF1 | 34 (24+) | 24 (5+) | ||||
| DAPK | 34 (19+) | 24 (6+) | ||||
| p16 | 34 (13+) | 24 (2+) | ||||
| HIN | 34 (10+) | 24 (2+) | ||||
| TIMP3 | 34 (8+) | 24 (1+) | ||||
| p15 | 34 (22+) | 24 (9+) | ||||
| APC | 34 (18+) | 24 (9+) | ||||
| SPARC | 34 (14+) | 24 (8+) | ||||
| ECAD+TMEFF2+RARβ+MGMT | 34 (34+) | 24 (3+) | ||||
| ECAD+TMEFF2+MGMT | 34 (33+) | 24 (2+) | ||||
| ECAD+TMEFF2+RARβ | 34 (32+) | 24 (1+) | ||||
| ECAD+RARβ+MGMT | 34 (31+) | 24 (2+) | ||||
| Ovchinnikov 2012 | OC | Saliva | Nested MSP | p16+RASSF1A+DAPK1 | 143 (117+) | 46 (6+) |
| Rettori 2012 | HNC | Oral rinse (NaCl) | qMSP | DCC | 143 (75+) | 50 (5+) |
| CCNA1 | 146 (17+) | 60 (2+) | ||||
| DAPK | 146 (12+) | 39 (1+) | ||||
| MGMT | 146 (11+) | 57 (2+) | ||||
| TIMP3 | 146 (7+) | 60 (2+) | ||||
| MINT31 | 68 (3+) | 20 (0+) | ||||
| AIM1 | 71 (2+) | 41 (0+) | ||||
| SFRP1 | 71 (2+) | 20 (0+) | ||||
| APC | 62 (2+) | 20 (0+) | ||||
| CDKN2A | 69 (1+) | 20 (0+) | ||||
| HIN1 | 134 (16+) | 57 (11+) | ||||
| CCNA1+DAPK+DCC+MGMT+TIMP3 | NA | NA | ||||
| CCNA1+DAPK+MGMT+TIMP3 | NA | NA | ||||
| CCNA1+DAPK+MGMT | NA | NA | ||||
| CCNA1+MGMT+TIMP3 | NA | NA | ||||
| CCNA1+DAPK+TIMP3 | NA | NA | ||||
| DAPK+MGMT+TIMP3 | NA | NA | ||||
| CCNA1+MGMT | NA | NA | ||||
| CCNA1+DAPK | NA | NA | ||||
| CCNA1+TIMP3 | NA | NA | ||||
| Ksumoto 2012 | OC | Oral rinse | MSP | p16 | 10 (4+) | 3 (0+) |
| Ovchinnikov 2014 | HNC | Saliva | MSP | PCQAP5’ | 62 (42+) | 49 (17+) |
| PCQAP3’ | 60 (41+) | 45 (19+) | ||||
| Gaykalova 2015 | HNC | Oral rinse | qMSP | ZNF14 | 59 (5+) | 35 (0+) |
| ZNF160 | 59 (10+) | 35 (0+) | ||||
| ZNF420 | 59 (8+) | 35 (0+) | ||||
| ZNF14+ZNF160+ZNF420 | 59 (13+) | 35 (0+) | ||||
| Lim 2016 | HNC | Saliva | MSP | RASSF1α | 88 (36+) | 122 (10+) |
| p16 | 88 (41+) | 122 (38+) | ||||
| TIMP3 | 88 (33+) | 122 (22+) | ||||
| PCQAP5’ | 88 (72+) | 122 (66+) | ||||
| PCQAP3’ | 88 (30+) | 122 (18+) | ||||
| RASSF1α+p16+TIMP3+PCQAP5’+PCQAP3’ | 88 (62+) | 122 (24+) | ||||
| Ferlazzo 2017 | OC | Saliva (Oragene DNA kit) | MSP | P16 | 58 (10+) | 90 (5+) |
| MGMT | 58 (16+) | 90 (7+) | ||||
| P16 + MGMT | 58 (12+) | 90 (0+) | ||||
| Cheng 2017 | OC | Oral rinse (0.12% clorhexidine) | qMSP | ZNF582 | 94 (62+) | 65 (10+) |
| PAX1 | 94 (64+) | 65 (7+) | ||||
| ZNF582+PAX1 | 94 (75+) | 65 (14+) | ||||
| Puttipanyalears 2018 | HNC | Oral rinse (NaCl) | qMSP | TRH | 66 (57+) | 54 (4+) |
| OC | 42 (37+) | |||||
| OPC | 24 (20+) | |||||
| Liyanage 2020 | HNC | Saliva | MSP | p16 | 88 (62+) | NA |
| RASSF1 α | 88 (59+) | NA | ||||
| TIMP3 | 88 (68+) | NA | ||||
| PCQAP/MED15 | 88 (66+) | NA | ||||
| p16+RASSF1α+TIMP3+PCQAP | 84 (80+) | 60 (5+) | ||||
| OC | p16 | 54 (39+) | NA | |||
| RASSF1α | 54 (37+) | NA | ||||
| TIMP3 | 54 (43+) | NA | ||||
| PCQAP/MED15 | 54 (43+) | NA | ||||
| p16+RASSF1α+TIMP3+PCQAP | 54 (46+) | 60 (5+) | ||||
| OPC | p16 | 34 (23+) | NA | |||
| RASSF1α | 34 (22+) | NA | ||||
| TIMP3 | 34 (25+) | NA | ||||
| PCQAP/MED15 | 34 (23+) | NA | ||||
| p16+RASSF1α+TIMP3+PCQAP | 34 (34+) | 60 (5+) | ||||
| Srisuttee 2020 | OC | Oral rinse (NaCl) | qMSP | NID2 | 43 (34+) | 90 (0+) |
| Shen 2020 | OPC | Oral rinse (NaCl) | qMSP | EDNRB | 21 (15+) | 40 (2+) |
| PAX5 | 21 (15+) | 40 (4+) | ||||
| p16 | 21 (3+) | 40 (0+) | ||||
| González-Pérez 2020 | OC | Saliva | MSP | p16 | 43 (19+) | 40 (4+) |
| RASSF1A | 43 (10+) | 40 (2+) | ||||
| p16+RASSF1A | 43 (23+) | 40 (5+) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rapado-González, Ó.; Martínez-Reglero, C.; Salgado-Barreira, Á.; Muinelo-Romay, L.; Muinelo-Lorenzo, J.; López-López, R.; Díaz-Lagares, Á.; Suárez-Cunqueiro, M.M. Salivary DNA Methylation as an Epigenetic Biomarker for Head and Neck Cancer. Part I: A Diagnostic Accuracy Meta-Analysis. J. Pers. Med. 2021, 11, 568. https://doi.org/10.3390/jpm11060568
Rapado-González Ó, Martínez-Reglero C, Salgado-Barreira Á, Muinelo-Romay L, Muinelo-Lorenzo J, López-López R, Díaz-Lagares Á, Suárez-Cunqueiro MM. Salivary DNA Methylation as an Epigenetic Biomarker for Head and Neck Cancer. Part I: A Diagnostic Accuracy Meta-Analysis. Journal of Personalized Medicine. 2021; 11(6):568. https://doi.org/10.3390/jpm11060568
Chicago/Turabian StyleRapado-González, Óscar, Cristina Martínez-Reglero, Ángel Salgado-Barreira, Laura Muinelo-Romay, Juan Muinelo-Lorenzo, Rafael López-López, Ángel Díaz-Lagares, and María Mercedes Suárez-Cunqueiro. 2021. "Salivary DNA Methylation as an Epigenetic Biomarker for Head and Neck Cancer. Part I: A Diagnostic Accuracy Meta-Analysis" Journal of Personalized Medicine 11, no. 6: 568. https://doi.org/10.3390/jpm11060568