
Machine Learning Approaches for Predicting Bisphosphonate-Related Osteonecrosis in Women with Osteoporosis Using VEGFA Gene Polymorphisms

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Genotyping
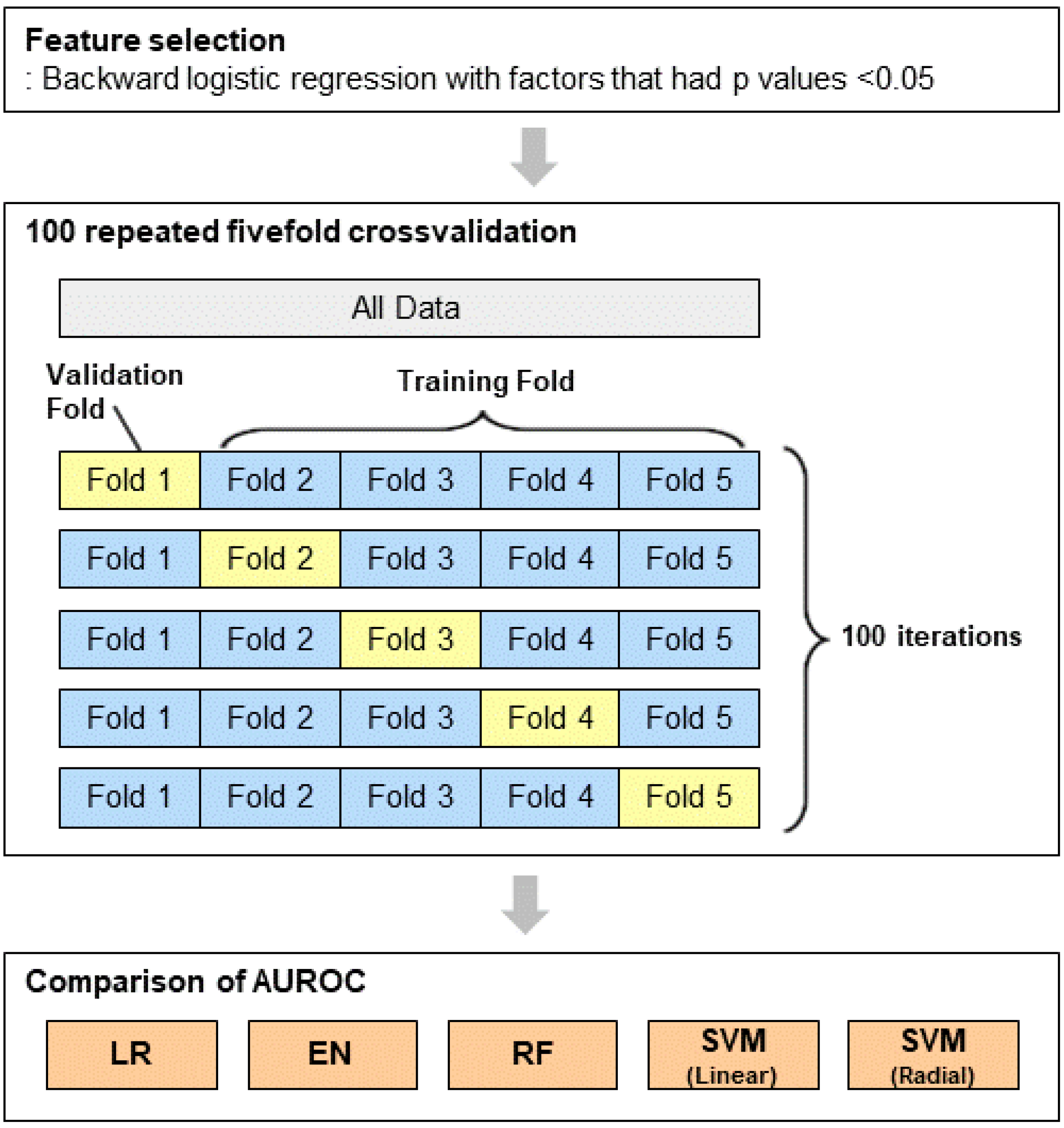
2.3. Statistical Analysis and Machine Learning Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AUROC | Area under the receiver-operating curve |
| BRONJ | Bisphosphonate-related osteonecrosis |
| CI | Confidence interval |
| ONJ | Osteonecrosis of the jaw |
| OR | Odds ratio |
| RF | Random forest |
| SNP | Single nucleotide polymorphism |
| SVM | Support vector machine |
| VEGF-A | Vascular endothelial growth factor A |
References
- Marx, R.E.; Sawatari, Y.; Fortin, M.; Broumand, V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: Risk factors, recognition, prevention, and treatment. J. Oral Maxillofac. Surg. 2005, 63, 1567–1575. [Google Scholar] [CrossRef]
- Khan, A.A.; Morrison, A.; Hanley, D.A.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; Taguchi, A.; Tetradis, S.; et al. Diagnosis and management of osteonecrosis of the jaw: A systematic review and international consensus. J. Bone Miner. Res. 2015, 30, 3–23. [Google Scholar] [CrossRef] [PubMed]
- King, R.; Tanna, N.; Patel, V. Medication-related osteonecrosis of the jaw unrelated to bisphosphonates and denosumab-a review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 289–299. [Google Scholar] [CrossRef]
- Aghaloo, T.; Hazboun, R.; Tetradis, S. Pathophysiology of Osteonecrosis of the Jaws. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 489–496. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.; Hakam, A.E.; McCauley, L.K. Current Understanding of the Pathophysiology of Osteonecrosis of the Jaw. Curr. Osteoporos. Rep. 2018, 16, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Mehrotra, B.; Rosenberg, T.J.; Engroff, S.L. Osteonecrosis of the jaws associated with the use of bisphosphonates: A review of 63 cases. J. Oral Maxillofac. Surg. 2004, 62, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Govaerts, D.; Piccart, F.; Ockerman, A.; Coropciuc, R.; Politis, C.; Jacobs, R. Adjuvant therapies for MRONJ: A systematic review. Bone 2020, 141, 115676. [Google Scholar] [CrossRef]
- Fortunato, L.; Bennardo, F.; Buffone, C.; Giudice, A. Is the application of platelet concentrates effective in the prevention and treatment of medication-related osteonecrosis of the jaw? A systematic review. J. Craniomaxillofac. Surg. 2020, 48, 268–285. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, F.; Bennardo, L.; Del Duca, E.; Patruno, C.; Fortunato, L.; Giudice, A.; Nistico, S.P. Autologous platelet-rich fibrin injections in the management of facial cutaneous sinus tracts secondary to medication-related osteonecrosis of the jaw. Dermatol. Ther. 2020, 33, e13334. [Google Scholar] [CrossRef]
- Allen, M.R.; Burr, D.B. The pathogenesis of bisphosphonate-related osteonecrosis of the jaw: So many hypotheses, so few data. J. Oral Maxillofac. Surg. 2009, 67, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Nissen, N.N.; Polverini, P.J.; Koch, A.E.; Volin, M.V.; Gamelli, R.L.; DiPietro, L.A. Vascular endothelial growth factor mediates angiogenic activity during the proliferative phase of wound healing. Am. J. Pathol. 1998, 152, 1445–1452. [Google Scholar]
- Ishtiaq, S.; Edwards, S.; Sankaralingam, A.; Evans, B.A.; Elford, C.; Frost, M.L.; Fogelman, I.; Hampson, G. The effect of nitrogen containing bisphosphonates, zoledronate and alendronate, on the production of pro-angiogenic factors by osteoblastic cells. Cytokine 2015, 71, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Bi, Y.; Gao, Y.; Ehirchiou, D.; Cao, C.; Kikuiri, T.; Le, A.; Shi, S.; Zhang, L. Bisphosphonates cause osteonecrosis of the jaw-like disease in mice. Am. J. Pathol. 2010, 177, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Bastos, P.; Patel, V.; Festy, F.; Hosny, N.; Cook, R.J. In-vivo imaging of the microvasculature of the soft tissue margins of osteonecrotic jaw lesions. Br. Dent. J. 2017, 223, 699–705. [Google Scholar] [CrossRef]
- Fung, P.L.; Nicoletti, P.; Shen, Y.; Porter, S.; Fedele, S. Pharmacogenetics of Bisphosphonate-associated Osteonecrosis of the Jaw. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 537–546. [Google Scholar] [CrossRef]
- Yang, G.; Singh, S.; Chen, Y.; Hamadeh, I.S.; Langaee, T.; McDonough, C.W.; Holliday, L.S.; Lamba, J.K.; Moreb, J.S.; Katz, J.; et al. Pharmacogenomics of osteonecrosis of the jaw. Bone 2019, 124, 75–82. [Google Scholar] [CrossRef]
- Nicoletti, P.; Cartsos, V.M.; Palaska, P.K.; Shen, Y.; Floratos, A.; Zavras, A.I. Genomewide pharmacogenetics of bisphosphonate-induced osteonecrosis of the jaw: The role of RBMS3. Oncologist 2012, 17, 279–287. [Google Scholar] [CrossRef] [Green Version]
- Bastida-Lertxundi, N.; Leizaola-Cardesa, I.O.; Hernando-Vazquez, J.; Muguerza-Iraola, R.; Aguilar-Salvatierra, A.; Gomez-Moreno, G.; Crettaz, J.S. Pharmacogenomics in medication-related osteonecrosis of the jaw: A systematic literature review. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 10184–10194. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Ko, Y.J.; Kim, J.Y.; Oh, Y.; Hwang, J.; Han, S.; Kim, S.; Lee, J.H.; Han, D.H. Genetic investigation of bisphosphonate-related osteonecrosis of jaw (BRONJ) via whole exome sequencing and bioinformatics. PLoS ONE 2015, 10, e0118084. [Google Scholar] [CrossRef]
- Sarasquete, M.E.; Garcia-Sanz, R.; Marin, L.; Alcoceba, M.; Chillon, M.C.; Balanzategui, A.; Santamaria, C.; Rosinol, L.; de la Rubia, J.; Hernandez, M.T.; et al. Bisphosphonate-related osteonecrosis of the jaw is associated with polymorphisms of the cytochrome P450 CYP2C8 in multiple myeloma: A genome-wide single nucleotide polymorphism analysis. Blood 2008, 112, 2709–2712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, G.; Hamadeh, I.S.; Katz, J.; Riva, A.; Lakatos, P.; Balla, B.; Kosa, J.; Vaszilko, M.; Pelliccioni, G.A.; Davis, N.; et al. SIRT1/HERC4 Locus Associated With Bisphosphonate-Induced Osteonecrosis of the Jaw: An Exome-Wide Association Analysis. J. Bone Min. Res. 2018, 33, 91–98. [Google Scholar] [CrossRef] [Green Version]
- La Ferla, F.; Paolicchi, E.; Crea, F.; Cei, S.; Graziani, F.; Gabriele, M.; Danesi, R. An aromatase polymorphism (g.132810C>T) predicts risk of bisphosphonate-related osteonecrosis of the jaw. Biomark. Med. 2012, 6, 201–209. [Google Scholar] [CrossRef]
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machoy, M.E.; Szyszka-Sommerfeld, L.; Vegh, A.; Gedrange, T.; Wozniak, K. The ways of using machine learning in dentistry. Adv. Clin. Exp. Med. 2020, 29, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, J.; de Oliveira Ruellas, A.C.; Goncalves, J.R.; Paniagua, B.; Prieto, J.C.; Styner, M.; Li, T.; Zhu, H.; Sugai, J.; Giannobile, W.; et al. Osteoarthritis of the Temporomandibular Joint can be diagnosed earlier using biomarkers and machine learning. Sci. Rep. 2020, 10, 8012. [Google Scholar] [CrossRef]
- Hung, K.; Yeung, A.W.K.; Tanaka, R.; Bornstein, M.M. Current Applications, Opportunities, and Limitations of AI for 3D Imaging in Dental Research and Practice. Int. J. Environ. Res. Public Health 2020, 17, 4424. [Google Scholar] [CrossRef] [PubMed]
- Hung, K.; Montalvao, C.; Tanaka, R.; Kawai, T.; Bornstein, M.M. The use and performance of artificial intelligence applications in dental and maxillofacial radiology: A systematic review. Dentomaxillofac. Radiol. 2020, 49, 20190107. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef]
- Sherry, S.T.; Ward, M.H.; Kholodov, M.; Baker, J.; Phan, L.; Smigielski, E.M.; Sirotkin, K. dbSNP: The NCBI database of genetic variation. Nucleic. Acids Res. 2001, 29, 308–311. [Google Scholar] [CrossRef] [Green Version]
- Ward, L.D.; Kellis, M. HaploReg v4: Systematic mining of putative causal variants, cell types, regulators and target genes for human complex traits and disease. Nucleic Acids Res. 2016, 44, D877–D881. [Google Scholar] [CrossRef]
- Rogers, M.S.; D’Amato, R.J. Common polymorphisms in angiogenesis. Cold Spring Harb. Perspect Med. 2012, 2. [Google Scholar] [CrossRef] [Green Version]
- Jain, L.; Vargo, C.A.; Danesi, R.; Sissung, T.M.; Price, D.K.; Venzon, D.; Venitz, J.; Figg, W.D. The role of vascular endothelial growth factor SNPs as predictive and prognostic markers for major solid tumors. Mol. Cancer Ther. 2009, 8, 2496–2508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Mendonca, G.R.; Brito, A.B.; Rocha, R.M.; Delamain, M.T.; de Andrade Natal, R.; Soares, F.A.; Colleoni, G.W.; Souza, C.A.; Vassallo, J.; Lima, C.S. Association of VEGFA-2578 C>A polymorphism with clinicopathological aspects and outcome in follicular lymphoma patients. Blood Cancer J. 2016, 6, e464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben Salem, A.; Megdich, F.; Kacem, O.; Souayeh, M.; Hachani Ben Ali, F.; Hizem, S.; Janhai, F.; Ajina, M.; Abu-Elmagd, M.; Assidi, M.; et al. Vascular endothelial growth factor (VEGFA) gene variation in polycystic ovary syndrome in a Tunisian women population. BMC Genom. 2016, 17, 748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.; Ning, L.; Liu, X.; Zhang, H.; Yu, Y.; Zhang, S.; Rao, W.; Shi, J.; Sun, H.; Yu, Q. Association between single nucleotide variants of vascular endothelial growth factor A and the risk of thyroid carcinoma and nodular goiter in a Han Chinese population. Oncotarget 2017, 8, 15838–15845. [Google Scholar] [CrossRef] [Green Version]
- Ahluwalia, T.S.; Troelsen, J.T.; Balslev-Harder, M.; Bork-Jensen, J.; Thuesen, B.H.; Cerqueira, C.; Linneberg, A.; Grarup, N.; Pedersen, O.; Hansen, T.; et al. Carriers of a VEGFA enhancer polymorphism selectively binding CHOP/DDIT3 are predisposed to increased circulating levels of thyroid-stimulating hormone. J. Med. Genet. 2017, 54, 166–175. [Google Scholar] [CrossRef]
- Hoeben, A.; Landuyt, B.; Highley, M.S.; Wildiers, H.; Van Oosterom, A.T.; De Bruijn, E.A. Vascular endothelial growth factor and angiogenesis. Pharmacol. Rev. 2004, 56, 549–580. [Google Scholar] [CrossRef] [PubMed]
- Lohela, M.; Bry, M.; Tammela, T.; Alitalo, K. VEGFs and receptors involved in angiogenesis versus lymphangiogenesis. Curr. Opin. Cell Biol. 2009, 21, 154–165. [Google Scholar] [CrossRef]
- Hu, K.; Olsen, B.R. Osteoblast-derived VEGF regulates osteoblast differentiation and bone formation during bone repair. J. Clin. Investig. 2016, 126, 509–526. [Google Scholar] [CrossRef] [Green Version]
- Street, J.; Bao, M.; deGuzman, L.; Bunting, S.; Peale, F.V., Jr.; Ferrara, N.; Steinmetz, H.; Hoeffel, J.; Cleland, J.L.; Daugherty, A.; et al. Vascular endothelial growth factor stimulates bone repair by promoting angiogenesis and bone turnover. Proc. Natl. Acad. Sci. USA 2002, 99, 9656–9661. [Google Scholar] [CrossRef] [Green Version]
- Vincenzi, B.; Santini, D.; Rocci, L.; Tonini, G. Bisphosphonates: New antiangiogenic molecules in cancer treatment? Ann. Oncol. 2003, 14, 806–807. [Google Scholar] [CrossRef]
- Ainsworth, H.C.; Langefeld, C.D.; Freedman, B.I. Genetic epidemiology in kidney disease. Nephrol. Dial. Transplant. 2017, 32, ii159–ii169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kottgen, A.; Pattaro, C.; Boger, C.A.; Fuchsberger, C.; Olden, M.; Glazer, N.L.; Parsa, A.; Gao, X.; Yang, Q.; Smith, A.V.; et al. New loci associated with kidney function and chronic kidney disease. Nat. Genet. 2010, 42, 376–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elias, I.; Franckhauser, S.; Ferre, T.; Vila, L.; Tafuro, S.; Munoz, S.; Roca, C.; Ramos, D.; Pujol, A.; Riu, E.; et al. Adipose tissue overexpression of vascular endothelial growth factor protects against diet-induced obesity and insulin resistance. Diabetes 2012, 61, 1801–1813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, L.X.; Ye, X.J.; Wang, Y.G.; Zhu, J.J.; Xie, W.Z.; Zhao, Y.M.; Lai, X.Y. 3′-UTR polymorphism (rs10434) in the VEGF gene is associated with B-CLL in a Chinese population. Genet. Mol. Res. 2015, 14, 4085–4089. [Google Scholar] [CrossRef] [PubMed]
- Niktalab, R.; Piravar, Z.; Behzadi, R. Different Polymorphisms of Vascular Endothelial Growth Factor Gene in Patients with Pre-Eclampsia among The Iranian Women Population. Int. J. Fertil. Steril. 2020, 14, 41–45. [Google Scholar] [CrossRef]
- Liu, F.; Wu, K.; Wu, W.; Chen, Y.; Wu, H.; Wang, H.; Zhang, W. miR203 contributes to preeclampsia via inhibition of VEGFA expression. Mol. Med. Rep. 2018, 17, 5627–5634. [Google Scholar] [CrossRef] [Green Version]
- Barasch, A.; Cunha-Cruz, J.; Curro, F.A.; Hujoel, P.; Sung, A.H.; Vena, D.; Voinea-Griffin, A.E.; Group, C.C.; Beadnell, S.; Craig, R.G.; et al. Risk factors for osteonecrosis of the jaws: A case-control study from the CONDOR dental PBRN. J. Dent. Res. 2011, 90, 439–444. [Google Scholar] [CrossRef]
- Thumbigere-Math, V.; Tu, L.; Huckabay, S.; Dudek, A.Z.; Lunos, S.; Basi, D.L.; Hughes, P.J.; Leach, J.W.; Swenson, K.K.; Gopalakrishnan, R. A retrospective study evaluating frequency and risk factors of osteonecrosis of the jaw in 576 cancer patients receiving intravenous bisphosphonates. Am. J. Clin. Oncol. 2012, 35, 386–392. [Google Scholar] [CrossRef]
- Badros, A.; Weikel, D.; Salama, A.; Goloubeva, O.; Schneider, A.; Rapoport, A.; Fenton, R.; Gahres, N.; Sausville, E.; Ord, R.; et al. Osteonecrosis of the jaw in multiple myeloma patients: Clinical features and risk factors. J. Clin. Oncol. 2006, 24, 945–952. [Google Scholar] [CrossRef]
- Hoff, A.O.; Toth, B.; Hu, M.; Hortobagyi, G.N.; Gagel, R.F. Epidemiology and risk factors for osteonecrosis of the jaw in cancer patients. Ann. N. Y. Acad. Sci. 2011, 1218, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Zou, H.; Hastie, T. Regularization and variable selection via the elastic net. J. R. Stat. Soc. B 2005, 67, 301–320. [Google Scholar] [CrossRef] [Green Version]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Breiman, L.; Friedman, J.; Stone, C.; Olshen, R. Classification and Regression Trees; Chapman and Hall: London, UK, 1984. [Google Scholar]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning: Data Mining, Inference and Prediction, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Cortes, C.; Vapnik, V. Support-Vector Networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Case (n = 58) | Control (n = 67) | p |
|---|---|---|---|
| Age (years) | 0.003 | ||
| <65 | 3 (5.2) | 16 (24.2) | |
| ≥65 | 55 (94.8) | 50 (75.8) | |
| Comorbidity | |||
| Hypertension | 36 (62.1) | 28 (41.8) | 0.024 |
| Diabetes mellitus | 18 (31.0) | 16 (23.9) | 0.370 |
| Cardiovascular disease | 8 (13.8) | 8 (11.9) | 0.757 |
| Rheumatoid arthritis | 7 (12.1) | 2 (3.0) | 0.080 |
| Thyroid disease | 4 (6.9) | 2 (3.0) | 0.415 |
| Kidney disease | 2 (3.4) | 3 (4.5) | 1.000 |
| Liver disease | 0 (0) | 2 (3.0) | 0.499 |
| Cancer | 2 (3.5) | 6 (9.1) | 0.284 |
| Treatment duration (months) | |||
| <36 | 13 (25.5) | 30 (55.6) | 0.002 |
| ≥36 | 38 (74.5) | 24 (44.4) |
| Gene Polymorphism | Allele Change | Minor Allele Frequency | Grouped Genotypes | Case (n = 58) | Control (n = 67) | p |
|---|---|---|---|---|---|---|
| rs699947 | A > C | 0.253 | AA, AC | 22 (37.9) | 31 (46.3) | 0.347 |
| CC | 36 (62.1) | 36 (53.7) | ||||
| rs2010963 | C > G | 0.439 | CC | 14 (25.0) | 8 (12.5) | 0.077 |
| CG, GG | 42 (75.0) | 56 (87.5) | ||||
| rs25648 | C > T | 0.081 | CC | 51 (87.9) | 52 (77.6) | 0.131 |
| CT, TT | 7 (12.1) | 15 (22.4) | ||||
| rs3024987 | C > T | 0.211 | CC, CT | 56 (96.6) | 63 (94.0) | 0.685 |
| TT | 2 (3.4) | 4 (6.0) | ||||
| rs3025022 | C > T | 0.181 | CC, CT | 18 (31.0) | 23 (34.3) | 0.696 |
| TT | 40 (69.0) | 44 (65.7) | ||||
| rs3025035 | C > T | 0.202 | CC | 34 (59.6) | 49 (73.1) | 0.246 |
| CT, TT | 23 (40.4) | 18 (26.9) | ||||
| rs3025039 | C > T | 0.133 | CC | 42 (72.4) | 50 (74.6) | 1.000 |
| CT, TT | 16 (27.6) | 17 (25.4) | ||||
| rs10434 | A > G | 0.113 | AA, AG | 7 (12.1) | 18 (26.9) | 0.039 |
| GG | 51 (87.9) | 49 (73.1) | ||||
| rs998584 | C > A | 0.421 | CC | 7 (12.1) | 14 (21.2) | 0.176 |
| CA, AA | 51 (87.9) | 52 (78.8) | ||||
| rs6905288 | G > A | 0.240 | GG, GA | 21 (36.2) | 33 (49.3) | 0.142 |
| AA | 37 (63.8) | 34 (50.7) | ||||
| rs881858 | G > A | 0.133 | GG, GA | 18 (31.0) | 10 (14.9) | 0.031 |
| AA | 40 (69.0) | 57 (85.1) |
| Variables | Crude Odds Ratio (95% CI) | Adjusted Odds Ratio (95% CI) | Attributable Risk (%) |
|---|---|---|---|
| Age ≥ 65 years | 5.87 (1.61–21.34) ** | 16.05 (1.87–138.05) * | 93.8 |
| Treatment duration ≥ 36 months | 3.65 (1.60–8.36) ** | 3.67 (1.36–9.94) * | 72.8 |
| VEGFA | |||
| rs10434, GG | 2.68 (1.03–6.97) * | 3.16 (0.97–10.31) | 68.4 |
| rs881858, GG/GA | 2.56 (1.07–6.14) * | 6.45 (1.69–24.65) ** | 84.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-W.; Yee, J.; Oh, S.-H.; Kim, S.-H.; Kim, S.-J.; Chung, J.-E.; Gwak, H.-S. Machine Learning Approaches for Predicting Bisphosphonate-Related Osteonecrosis in Women with Osteoporosis Using VEGFA Gene Polymorphisms. J. Pers. Med. 2021, 11, 541. https://doi.org/10.3390/jpm11060541
Kim J-W, Yee J, Oh S-H, Kim S-H, Kim S-J, Chung J-E, Gwak H-S. Machine Learning Approaches for Predicting Bisphosphonate-Related Osteonecrosis in Women with Osteoporosis Using VEGFA Gene Polymorphisms. Journal of Personalized Medicine. 2021; 11(6):541. https://doi.org/10.3390/jpm11060541
Chicago/Turabian StyleKim, Jin-Woo, Jeong Yee, Sang-Hyeon Oh, Sun-Hyun Kim, Sun-Jong Kim, Jee-Eun Chung, and Hye-Sun Gwak. 2021. "Machine Learning Approaches for Predicting Bisphosphonate-Related Osteonecrosis in Women with Osteoporosis Using VEGFA Gene Polymorphisms" Journal of Personalized Medicine 11, no. 6: 541. https://doi.org/10.3390/jpm11060541