
Genetic Determinants in HLA and Cytochrome P450 Genes in the Risk of Aromatic Antiepileptic-Induced Severe Cutaneous Adverse Reactions

 , ,
, ,
Abstract
:1. Introduction
2. Severe Cutaneous Adverse Drug Reactions (SCARs) and AEDs Use
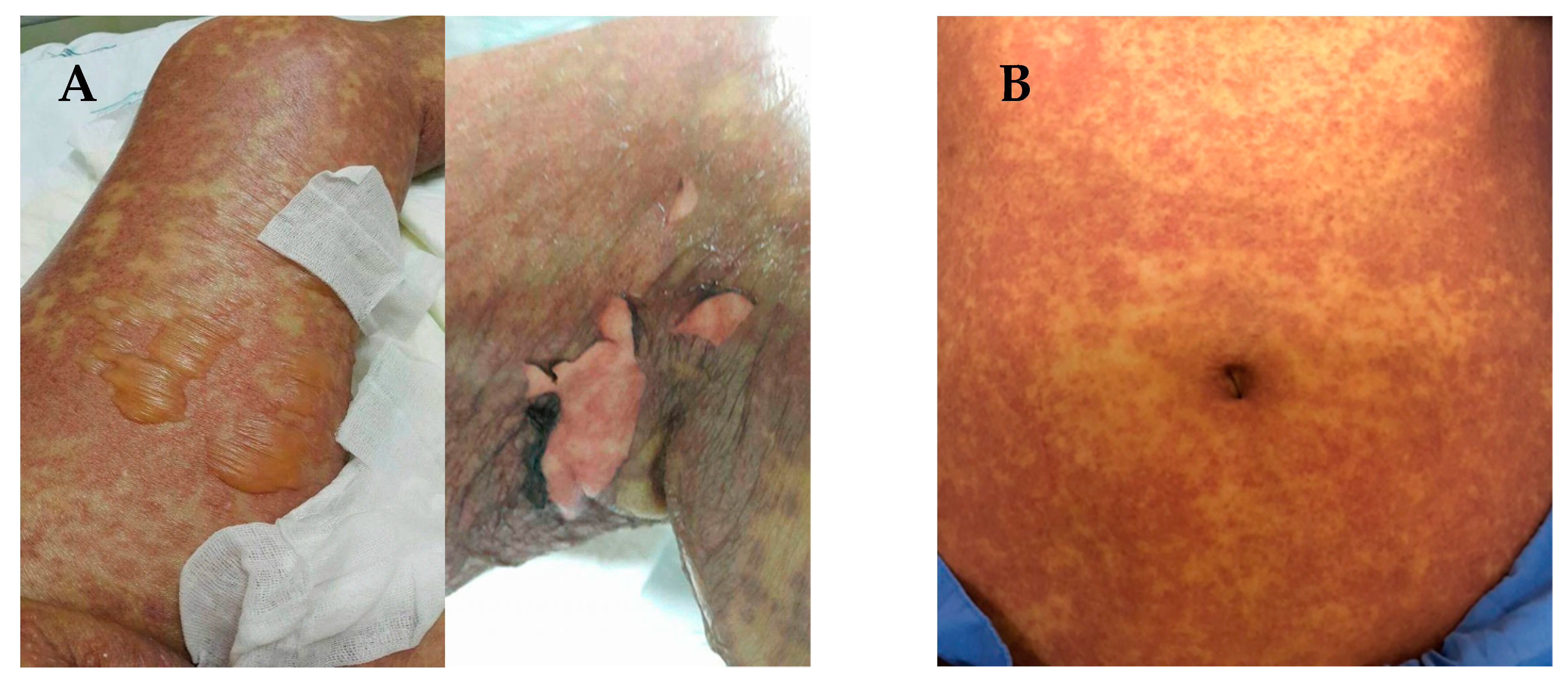
3. Clinical Manifestations of SCARs
4. Phenotyping and Causality of SCARs
5. Human Leukocyte Antigen (HLA) and Its Role in ADRs
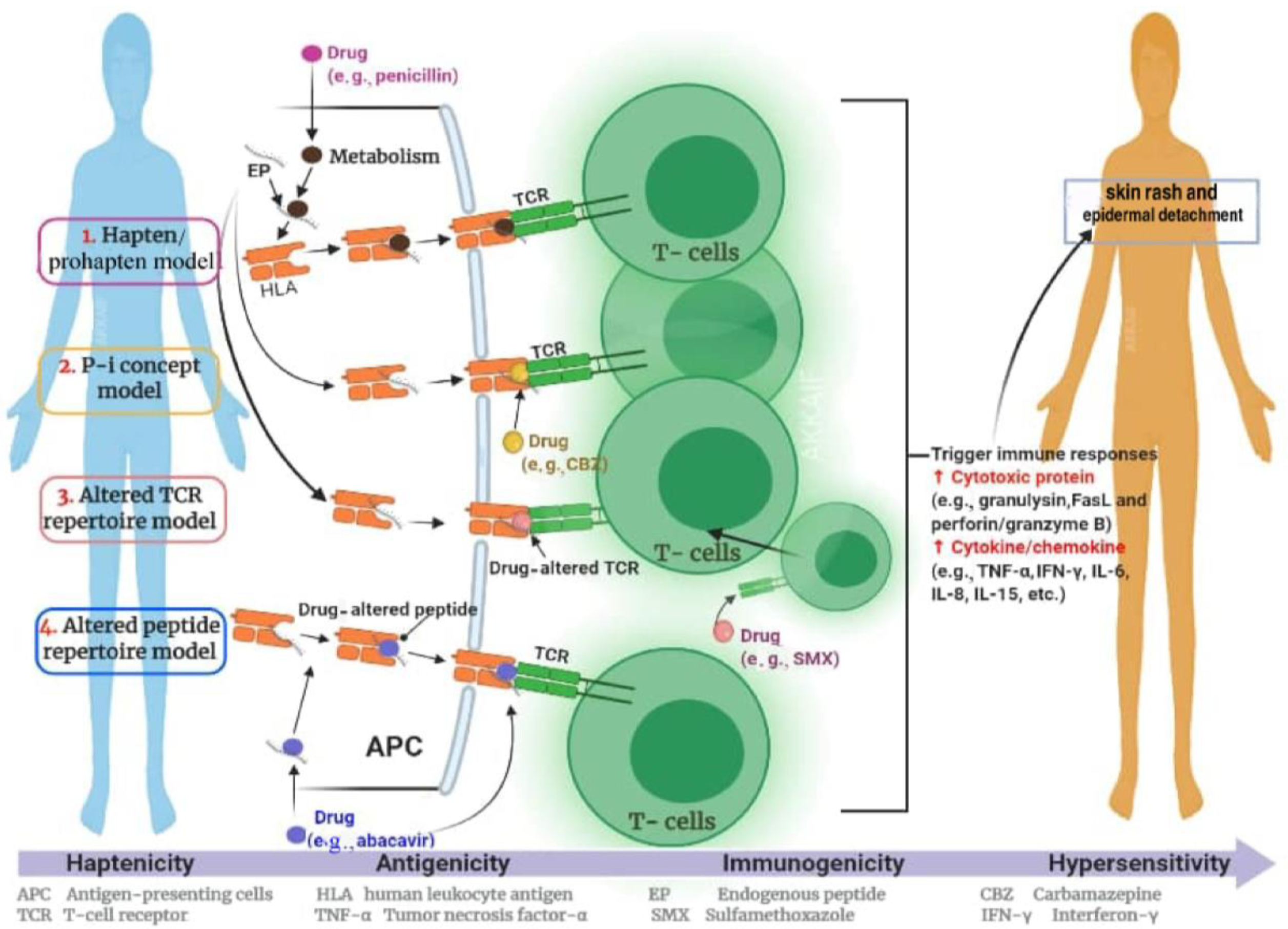
6. The Hypothesis of Immune Response in SCARs
7. Genetic Polymorphisms of HLA Genes
8. HLA Alleles and SCARs Induced by AEDs
8.1. Carbamazepine-Induced SCARs
8.2. Phenytoin-Induced SCAR
8.3. Lamotrigine-Induced SJS/TEN SCARs
8.4. Phenobarbital-Induced SJS/TEN SCARs
9. Cytochrome P450 Enzymes and the Risk of SCAR

{kind=link}
{kind=link}
{kind=link}
| AEDs | Population/Ethnicity | Genetic Variation | Allele Frequency | References |
|---|---|---|---|---|
| Carbamazepine | Thai | CYP2C19*2 | 0.29 | [11] |
| Korean | CYP3A5*3 | 0.237 | [131,132] | |
| Japanese | CYP3A5 | 7 | [128,133] | |
| Phenytoin | Japanese | CYP2C9 | 0 | [134] |
| Caucasian | CYP2C9*2 | 0.15 | [127] | |
| Caucasian | CYP2C9*3 | 0.07 | [127] | |
| Indian | CYP2C19*2 | 4.5 | [135,136] | |
| CYP2C19*3 | 10.1 | |||
| Thai | CYP2C 19*2 | 0.27 | [102,137] | |
| Thai | CYP2C19*3 | 0.02 | [102,137] | |
| Malay | CYP2C9*1 | 0.9407 | [134,138] | |
| Phenobarbital | Japanese | CYP2C19 | 0.26 | [139] |
| Japanese | CYP2C9 | 0.966 | [140] |
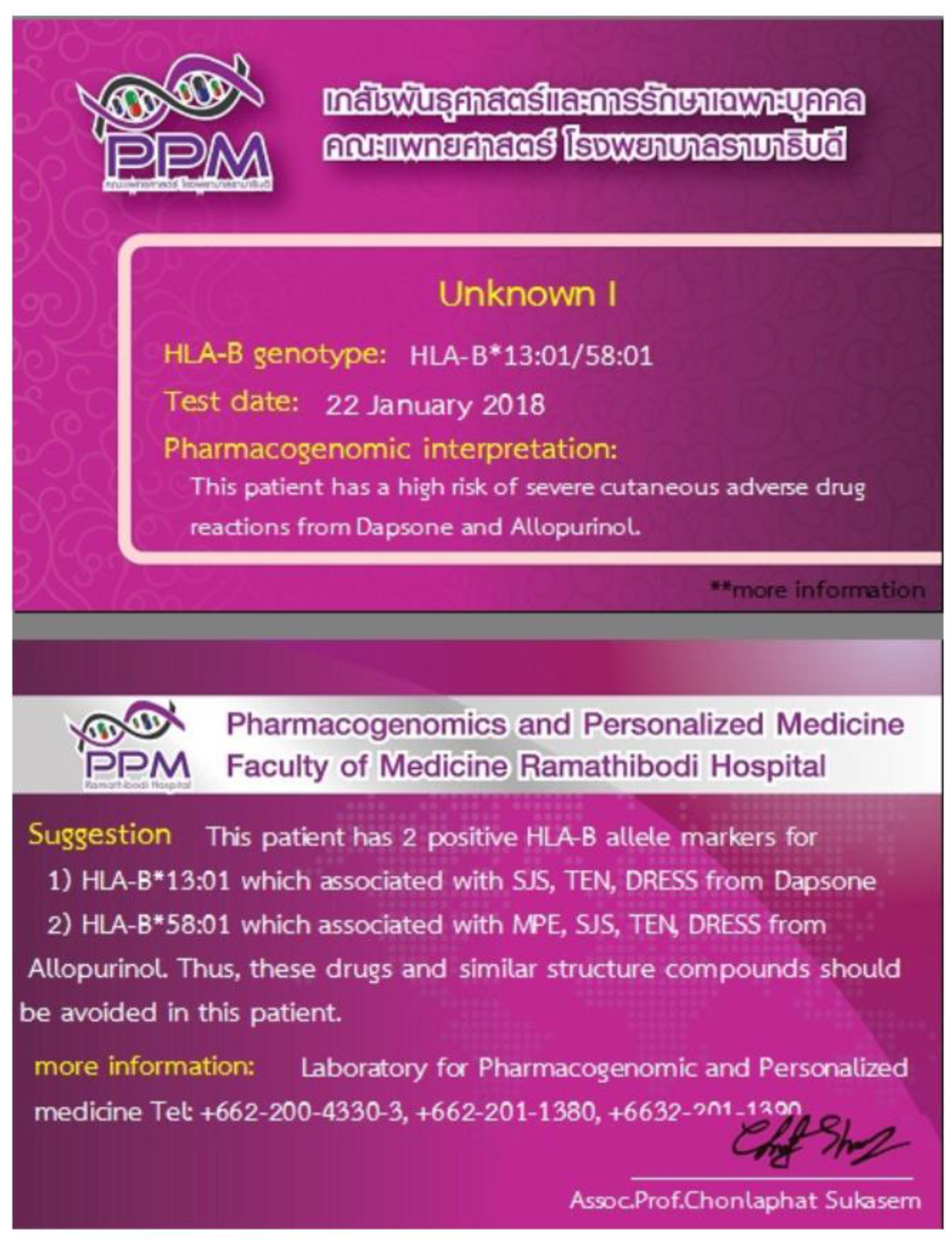
10. Clinical Application of Pharmacogenetic Testing in the Prevention of SCARs
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. International Drug Monitoring: The Role of National Centres, Report of a WHO Meeting [Held in Geneva from 20 to 25 September 1971]; World Health Organization Technical Report Series No. 498; World Health Organization: Geneva, Switzerland, 1972. [Google Scholar]
- Lazarou, J.; Pomeranz, B.H.; Corey, P.N. Incidence of adverse drug reactions in hospitalized patients: A meta-analysis of prospective studies. JAMA 1998, 279, 1200–1205. [Google Scholar] [CrossRef]
- Pirmohamed, M.; James, S.; Meakin, S.; Greene, C.; Scott, A.K.; Walley, T.J.; Farrar, K.; Parks, B.K.; Breckenridge, A.M. Adverse drug reactions as cause of admission to hospital: Prospective analysis of 18 820 patients. BMJ 2004, 329, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Mori, F.; Blanca-Lopez, N.; Caubet, J.; Demoly, P.; Du Toit, G.; Gomes, E.R.; Kuyucu, S.; Romano, A.; Soyer, O.; Tsabouri, S.; et al. Delayed hypersensitivity to antiepileptic drugs in children. Pediatr. Allergy Immunol. 2021, 32, 425–436. [Google Scholar] [CrossRef]
- Alfares, I.; Javaid, M.S.; Chen, Z.; Anderson, A.; Antonic-Baker, A.; Kwan, P. Sex Differences in the Risk of Cutaneous Adverse Drug Reactions Induced by Antiseizure Medications: A Systematic Review and Me-ta-analysis. CNS Drugs 2021, 35, 161–176. [Google Scholar] [CrossRef] [PubMed]
- Chia, F.L.; Leong, K.P. Severe cutaneous adverse reactions to drugs. Curr. Opin. Allergy Clin. Immunol. 2007, 7, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Roujeau, J.-C.; Kelly, J.P.; Naldi, L.; Rzany, B.; Stern, R.S.; Anderson, T.; Auquier, A.; Bastuji-Garin, S.; Correia, O.; Locati, F.; et al. Medication Use and the Risk of Stevens–Johnson Syndrome or Toxic Epidermal Necrolysis. N. Engl. J. Med. 1995, 333, 1600–1608. [Google Scholar] [CrossRef]
- Iriki, H.; Adachi, T.; Mori, M.; Tanese, K.; Funakoshi, T.; Karigane, D.; Shimizu, T.; Okamoto, S.; Keisuke, N. Toxic epidermal necrolysis in the absence of circulating T cells: A possi-ble role for resident memory T cells. J. Am. Acad. Dermatol. 2014, 71, e214–e216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sukasem, C.; Pratoomwun, J.; Satapornpong, P.; Klaewsongkram, J.; Rerkpattanapipat, T.; Reknimitr, P.; Lertpichiktul, P.; Puangpetch, A.; Nakkam, N.; Konyoung, P.; et al. Genetic association of co--trimoxazole--induced se-vere cutaneous adverse reactions is phenotype--specific: HLA class I genotypes and haplotypes. Clin. Pharmacol. Ther. 2020, 108, 1078–1089. [Google Scholar] [CrossRef]
- Tong, H.; Phan, N.V.T.; Nguyen, T.T.; Nguyen, D.V.; Vo, N.S.; Le, L. Review on Databases and Bioinformatic Approaches on Pharmacogenomics of Adverse Drug Reactions. Pharmacogenomics Pers. Med. 2021, 14, 61–75. [Google Scholar] [CrossRef]
- Manuyakorn, W.; Siripool, K.; Kamchaisatian, W.; Pakakasama, S.; Visudtibhan, A.; Vilaiyuk, S.; Rujirawat, T.; Benjaponpitak, S. Phenobarbital--induced severe cutaneous ad-verse drug reactions are associated with CYP2C19* 2 in Thai children. Pediatr. Allergy Immunol. 2013, 24, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Chan, F.L.; Dodiuk-Gad, R.P. Implementation of Genetic Screening to Prevent Severe Cutaneous Ad-verse Drug Reactions Is Crucial—Rebuttal from the Devil’s Antagonist. JAMA Dermatol. 2020, 156, 220–221. [Google Scholar] [CrossRef]
- Thong, B.Y.-H.; Tan, T.-C. Epidemiology and risk factors for drug allergy. Br. J. Clin. Pharmacol. 2011, 71, 684–700. [Google Scholar] [CrossRef] [PubMed]
- Krivoy, N.; Taer, M.; Neuman, M.G. Antiepileptic drug-induced hypersensitivity syndrome reactions. Curr. Drug Saf. 2006, 1, 289–299. [Google Scholar] [CrossRef]
- Mehta, M.; Shah, J.; Khakhkhar, T.; Shah, R.; Hemavathi, K.G. Anticonvulsant hypersensitivity syn-drome associated with carbamazepine administration: Case series. J. Pharmacol. Pharmacother. 2014, 5, 59. [Google Scholar]
- Anwar, T.M.; Faris, P.M. A Systematic Review on Lamotrigine Induced Skin Rashes. J. Drug Deliv. Ther. 2021, 11, 146–151. [Google Scholar] [CrossRef]
- Roujeau, J.-C. The Spectrum of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Clinical Classification. J. Investig. Dermatol. 1994, 102, 28S–30S. [Google Scholar] [CrossRef] [PubMed]
- Duong, T.A.; Valeyrie-Allanore, L.; Wolkenstein, P.; Chosidow, O. Severe cutaneous adverse reactions to drugs. Lancet 2017, 390, 1996–2011. [Google Scholar] [CrossRef]
- Pavlos, R.; Mallal, S.; Phillips, E. HLA and pharmacogenetics of drug hypersensitivity. Pharmacogenomics 2012, 13, 1285–1306. [Google Scholar] [CrossRef] [Green Version]
- Choudhary, S.; McLeod, M.; Torchia, D.; Romanelli, P. Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome. J. Clin. Aesthetic Dermatol. 2013, 6, 31–37. [Google Scholar]
- Auquier-Dunant, A.; Mockenhaupt, M.; Naldi, L.; Correia, O.; Schröder, W.; Roujeau, J.-C. Correlations Between Clinical Patterns and Causes of Erythema Multiforme Majus, Stevens-Johnson Syndrome, and Toxic Epidermal Necrolysis. Arch. Dermatol. 2002, 138, 1019–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, M.F.; Arthur, Z.E.; Klauss, W.K.; Frank, A.; Lowell, A.G.S.K. Fitzpatrick’s Dermatology in General Medicine, 5th ed.; McGraw Hill: New York, NY, USA, 1999. [Google Scholar]
- Hall, J.B.; Schmidt, G.A.; Wood, L.D.H. Principles of Critical Care, 4th ed.; McGraw-Hill: New York, NY, USA, 1999. [Google Scholar]
- Fritsch, P.O.; Sidoroff, A. Drug-Induced Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis. Am. J. Clin. Dermatol. 2000, 1, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Creamer, D.; Walsh, S.; Dziewulski, P.; Exton, L.; Lee, H.; Dart, J.; Setterfield, J.; Bunker, C.; Ardern-Jones, M.; Watson, K.; et al. UK guidelines for the management of Stevens–Johnson syndrome/toxic epidermal necrolysis in adults 2016. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, e119–e153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, L.E.; Trent, J.T.; Kerdel, F.A. Use of intravenous immunoglobulin in toxic epidermal necrolysis and Stevens–Johnson syndrome: Our current understanding. Int. Immunopharmacol. 2006, 6, 543–549. [Google Scholar] [CrossRef]
- Vanfleteren, I.; Van Gysel, D.; De Brandt, C. Stevens-Johnson Syndrome: A Diagnostic Challenge in the Absence of Skin Lesions. Pediatr. Dermatol. 2003, 20, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Tomy, M.; Hui, L.I. Severe cutaneous adverse drug reactions: A review on epidemiology, etiology, clinical manifestation and pathogenesis. Chin. Med. J. 2008, 121, 756–761. [Google Scholar] [CrossRef]
- Kardaun, S.; Sidoroff, A.; Valeyrie-Allanore, L.; Halevy, S.; Davidovici, B.; Mockenhaupt, M.; Roujeau, J. Variability in the clinical pattern of cutaneous side-effects of drugs with systemic symptoms: Does a DRESS syndrome really exist? Br. J. Dermatol. 2007, 156, 609–611. [Google Scholar] [CrossRef]
- Han, M.K.; Agusti, A.; Calverley, P.M.; Celli, B.R.; Criner, G.; Curtis, J.L.; Fabbri, L.M.; Goldin, J.G.; Jones, P.W.; Macnee, W.; et al. Chronic obstructive pulmonary disease phenotypes: The future of COPD. Am. J. Respir. Crit. Care Med. 2010, 182, 598–604. [Google Scholar] [CrossRef] [Green Version]
- Sassolas, B.; Haddad, C.; Mockenhaupt, M.; Dunant, A.; Liss, Y.; Bork, K.; Haustein, U.F.; Vieluf, D.; Roujeau, J.C.; Louet, H.L. ALDEN, an algorithm for assessment of drug causal-ity in Stevens–Johnson syndrome and toxic epidermal necrolysis: Comparison with case–control analysis. Clin. Pharmacol. Ther. 2010, 88, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Bastuji-Garin, S.; Rzany, B.; Stern, R.S.; Shear, N.H.; Naldi, L.; Roujeau, J.-C. Clinical Classification of Cases of Toxic Epidermal Necrolysis, Stevens-Johnson Syndrome, and Erythema Multiforme. Arch. Dermatol. 1993, 129, 92–96. [Google Scholar] [CrossRef]
- Bégaud, B.; Evreux, J.C.; Jouglard, J.; Lagier, G. Imputation of the unexpected or toxic effects of drugs. Actualization of the method used in France. Therapy 1985, 40, 111–118. [Google Scholar]
- Palmieri, T.L.; Greenhalgh, D.G.; Saffle, J.R.; Spence, R.J.; Peck, M.D.; Jeng, J.C.; Mozingo, D.W.; Yowler, C.J.; Sheridan, R.L.; Ahrenholz, D.H.; et al. A Multicenter Review of Toxic Epidermal Necrolysis Treated in U.S. Burn Centers at the End of the Twentieth Century. J. Burn. Care Rehabil. 2002, 23, 87–96. [Google Scholar] [CrossRef]
- Alfirevic, A.P.M. Genomics of adverse drug reactions. Trends Pharmacol. Sci. 2017, 38, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.W.W.C.S. Genetics of Adverse Drug Reactions; John Wiley Sons: Hoboken, NJ, USA, 2017. [Google Scholar]
- Lin, M.; Xu, H.; Shi, Y.; Da, L.-T. Antigenic Peptide Loading into Major Histocompatibility Complex Class I Is Driven by the Substrate N-Terminus. CCS Chem. 2021, 2021, 979–994. [Google Scholar] [CrossRef]
- Naranjo, A.C.; Busto, U.; Sellers, E.M.; Sandor, P.; Ruiz, I.; Roberts, A.E.; Janecek, E.; Domecq, C.; Greenblatt, D.J. A method for estimating the probability of adverse drug reactions. Clin. Pharmacol. Ther. 1981, 30, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.S.; Kwan, P.; Tan, C.T. Association of HLA-B* 1502 allele and carbamazepine-induced severe adverse cutaneous drug reaction among Asians, a review. Neurol. Asia 2008, 13, 15–21. [Google Scholar]
- Cresswell, P.; Ackerman, A.L.; Giodini, A.; Peaper, D.R.; Wearsch, P.A. Mechanisms of MHC class I-restricted antigen processing and cross-presentation. Immunol. Rev. 2005, 207, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Pirmohamed, M.; Naisbitt, D.J.; Gordon, F.; Park, B.K. The danger hypothesis—potential role in idiosyncratic drug reactions. Toxicology 2002, 181, 55–63. [Google Scholar] [CrossRef]
- Daly, K.A. Human leukocyte antigen (HLA) pharmacogenomic tests: Potential and pitfalls. Curr. Drug Metab. 2014, 15, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Zazzara, M.B.; Palmer, K.; Vetrano, D.L.; Carfì, A.; Graziano, O. Adverse drug reactions in older adults: A narrative review of the literature. Eur. Geriatr. Med. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Bharadwaj, M.; Illing, P.; Theodossis, A.; Purcell, A.W.; Rossjohn, J.; McCluskey, J. Drug Hypersensitivity and Human Leukocyte Antigens of the Major Histocompatibility Complex. Annu. Rev. Pharmacol. Toxicol. 2012, 52, 401–431. [Google Scholar] [CrossRef]
- Edwards, I.R.; Aronson, J.K. Adverse drug reactions: Definitions, diagnosis, and management. Lancet 2000, 356, 1255–1259. [Google Scholar] [CrossRef]
- Becquemont, L. HLA: A pharmacogenomics success story. Pharmacogenomics 2010, 11, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Karnes, J.H.; Miller, M.A.; White, K.D.; Konvinse, K.C.; Pavlos, R.K.; Redwood, A.J.; Peter, J.G.; Lehloenya, R.; Mallal, S.A.; Phillips, E.J.; et al. Applications of Immunopharmacogenomics: Predicting, Preventing, and Understanding Immune-Mediated Adverse Drug Reactions. Annu. Rev. Pharmacol. Toxicol. 2019, 59, 463–486. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; Barker, D.J.; Georgiou, X.; Cooper, A.M.; Flicek, P.; Marsh, E.S.G. IPD-IMGT/HLA Database. Nucleic Acids Res. 2019, 48, D948–D955. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; Halliwell, J.A.; Hayhurst, J.D.; Flicek, P.; Parham, P.; Marsh, S.G.E. The IPD and IMGT/HLA database: Allele variant databases. Nucleic Acids Res. 2015, 43, D423–D431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, L. Carbamazepine Therapy and HLA Genotype; NCBI: Bethesda, MD, USA, 2018. [Google Scholar]
- Pappas, D.J.; Lizee, A.; Paunic, V.; Beutner, K.R.; Motyer, A.; Vukcevic, D.; Leslie, S.; Biesiada, J.; Meller, J.; Taylor, K.D.; et al. Significant variation between SNP-based HLA imputations in diverse populations: The last mile is the hardest. Pharm. J. 2018, 18, 367–376. [Google Scholar] [CrossRef]
- Di, D.; Sanchez-Mazas, A. Challenging views on the peopling history of East Asia: The story according to HLA markers. Am. J. Phys. Anthr. 2011, 145, 81–96. [Google Scholar] [CrossRef]
- Solberg, O.D.; Mack, S.J.; Lancaster, A.K.; Single, R.M.; Tsai, Y.; Sanchez-Mazas, A.; Thomson, G. Balancing selection and heterogeneity across the classical human leukocyte antigen loci: A meta-analytic review of 497 population studies. Hum. Immunol. 2008, 69, 443–464. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.-C.; Too, C.-L.; Murad, S.; Hussein, S.H. Association of HLA-B*1502 allele with carbamazepine-induced toxic epidermal necrolysis and Stevens-Johnson syndrome in the multi-ethnic Malaysian population. Int. J. Dermatol. 2011, 50, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilzadeh, H.; Farjadian, S.; Alyasin, S.; Nemati, H.; Nabavizadeh, H.; Esmaeilzadeh, E. Epidemiology of Severe Cutaneous Adverse Drug Reaction and Its HLA Association among Pediatrics. Iran. J. Pharm. Res. IJPR 2019, 18, 506–522. [Google Scholar]
- McCormack, M.; Alfirevic, A.; Bourgeois, S.; Farrell, J.J.; Kasperavičiūtė, D.; Carrington, M.; Sills, G.J.; Marson, T.; Jia, X.; De Bakker, P.I.; et al. HLA-A*3101 and Carbamazepine-Induced Hypersensitivity Reactions in Europeans. N. Engl. J. Med. 2011, 364, 1134–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozeki, T.; Mushiroda, T.; Yowang, A.; Takahashi, A.; Kubo, M.; Shirakata, Y.; Ikezawa, Z.; Iijima, M.; Shiohara, T.; Hashimoto, K.; et al. Genome-wide association study identifies HLA-A*3101 allele as a genetic risk factor for carbamazepine-induced cutaneous adverse drug reactions in Japanese population. Hum. Mol. Genet. 2010, 20, 1034–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-H.; Lee, K.W.; Song, W.-J.; Kim, S.-H.; Jee, Y.-K.; Lee, S.-M.; Kang, H.-R.; Park, H.-W.; Cho, S.-H.; Park, S.-H.; et al. Carbamazepine-induced severe cutaneous adverse reactions and HLA genotypes in Koreans. Epilepsy Res. 2011, 97, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Genin, E.; Chen, D.-P.; Hung, S.-I.; Sekula, P.; Schumacher, A.M.; Chang, P.-Y.; Tsai, S.-H.; Wu, T.-L.; Bellón, T.; Tamouza, R.; et al. HLA-A*31:01 and different types of carbamazepine-induced severe cutaneous adverse reactions: An international study and meta-analysis. Pharmacogenomics J. 2014, 14, 281–288. [Google Scholar] [CrossRef]
- Hung, S.-I.; Chung, W.-H.; Jee, S.-H.; Chen, W.-C.; Chang, Y.-T.; Lee, W.-R.; Hu, S.-L.; Wu, M.-T.; Chen, G.-S.; Wong, T.-W.; et al. Genetic susceptibility to carbamazepine-induced cutaneous adverse drug reactions. Pharmacogenetics Genom. 2006, 16, 297–306. [Google Scholar] [CrossRef]
- Chung, W.-H.; Hung, S.-I.; Hong, H.-S.; Hsih, M.-S.; Yang, L.-C.; Ho, H.C.; Wu, J.Y.; Chen, Y.-T. A marker for Stevens–Johnson syndrome. Nature 2004, 428, 486. [Google Scholar] [CrossRef]
- Tassaneeyakul, W.; Tiamkao, S.; Jantararoungtong, T.; Chen, P.; Lin, S.-Y.; Chen, W.-H.; Konyoung, P.; Khunarkornsiri, U.; Auvichayapat, N.; Pavakul, K.; et al. Association between HLA-B*1502 and carbamazepine-induced severe cutaneous adverse drug reactions in a Thai population. Epilepsia 2010, 51, 926–930. [Google Scholar] [CrossRef]
- Nguyen, D.V.; Chu, H.C.; Nguyen, D.V.; Phan, M.H.; Craig, T.; Baumgart, K.; van Nunen, S. HLA-B* 1502 and carbamazepine-induced severe cutaneous adverse drug reactions in Vietnamese. Asia Pac. Allergy 2015, 5, 68–77. [Google Scholar] [CrossRef] [Green Version]
- Yuliwulandari, R.; Shin, J.G.; Kristin, E.; Suyatna, F.D.; Prahasto, I.D.; Prayuni, K.; Mahasirimongkol, S.; Cavallari, L.H.; Mitropoulou, C.; Patrinos, G.P.; et al. Cost-effectiveness analysis of genotyping for HLA-B*15:02 in Indonesian patients with epilepsy using a generic model. Pharm. J. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Hung, C.-C.; Chang, W.-L.; Ho, J.-L.; Tai, J.J.; Hsieh, T.-J.; Huang, H.-C.; Hsieh, Y.-W.; Liou, H.-H. Association of polymorphisms in EPHX1, UGT2B7, ABCB1, ABCC2, SCN1A and SCN2A genes with carbamazepine therapy optimization. Pharmacogenomics 2012, 13, 159–169. [Google Scholar] [CrossRef]
- Kaniwa, N.; Saito, Y.; Aihara, M.; Matsunaga, K.; Tohkin, M.; Kurose, K.; Furuya, H.; Takahashi, Y.; Muramatsu, M.; Kinoshita, S.; et al. HLA-B*1511 is a risk factor for carbamazepine-induced Stevens-Johnson syndrome and toxic epidermal necrolysis in Japanese patients. Epilepsia 2010, 51, 2461–2465. [Google Scholar] [CrossRef]
- Kaniwa, N.; Saito, Y.; Aihara, M.; Matsunaga, K.; Tohkin, M.; Kurose, K.; Sawada, J.-I.; Furuya, H.; Takahashi, Y.; Muramatsu, M.; et al. HLA-B locus in Japanese patients with anti-epileptics and allopurinol-related Stevens–Johnson syndrome and toxic epidermal necrolysis. Pharmacogenomics 2008, 9, 1617–1622. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ye, X.; Fan, Y.; Wang, L.; Luo, X.; Liu, H.; Gao, X.; Gong, Z.; Wang, Y.; Qiu, W.; et al. High Detection Rate of Copy Number Variations Using Capture Sequencing Data: A Retrospective Study. Clin. Chem. 2020, 66, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Cheung, Y.; Cheng, S.; Chan, E.J.M.; Lo, S.V.; Ng, M.H.L.; Kwan, P. HLA--B alleles associated with severe cutaneous reactions to antiepileptic drugs in Han Chinese. Epilepsia 2013, 54, 1307–1314. [Google Scholar] [CrossRef] [PubMed]
- Locharernkul, C.; Loplumlert, J.; Limotai, C.; Korkij, W.; Desudchit, T.; Tongkobpetch, S.; Kangwanshiratada, O.; Hirankarn, N.; Suphapeetiporn, K.; Shotelersuk, V. Carbamazepine and phenytoin induced Stevens-Johnson syndrome is associated with HLA-B*1502 allele in Thai population. Epilepsia 2008, 49, 2087–2091. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-C.; Ng, C.-C.; Too, C.-L.; Choon, S.-E.; Lee, C.-K.; Chung, W.-H.; Hussein, S.H.; Lim, K.-S.; Murad, S. Association of HLA-B*15:13 and HLA-B*15:02 with phenytoin-induced severe cutaneous adverse reactions in a Malay population. Pharm. J. 2016, 17, 170–173. [Google Scholar] [CrossRef]
- Zeng, T.; Long, Y.-S.; Min, F.-L.; Liao, W.-P.; Shi, Y.-W. Association ofHLA-B*1502allele with lamotrigine-induced Stevens-Johnson syndrome and toxic epidermal necrolysis in Han Chinese subjects: A meta-analysis. Int. J. Dermatol. 2014, 54, 488–493. [Google Scholar] [CrossRef]
- Tempark, T.; Satapornpong, P.; Rerknimitr, P.; Nakkam, N.; Saksit, N.; Wattankrai, P.; Jantararoungtong, T.; Koomdee, N.; Mahakkanukrauh, A.; Tassaneeyakul, W.; et al. Dapsone-induced severe cutaneous adverse drug reactions are strongly linked with HLA-B* 13: 01 allele in the Thai population. Pharmacogenet. Genom. 2017, 27, 429–437. [Google Scholar] [CrossRef]
- Allele Frequency Net Database. Available online: http://www.allelefrequencies.net/pop6001c.asp?pop_id=1801 (accessed on 30 April 2021).
- Hagenlocher, Y.; Willburger, B.; Behrens, G.A.; Schmidt, A.H.; Ioffe, Y.; Sauter, J. 6-Locus HLA allele and haplotype frequencies in a population of 1075 Russians from Karelia. Hum. Immunol. 2019, 80, 95–96. [Google Scholar] [CrossRef]
- Ikeda, N.; Kojima, H.; Nishikawa, M.; Hayashi, K.; Futagami, T.; Tsujino, T.; Kusunoki, Y.; Fujii, N.; Suegami, S.; Miyazaki, Y.; et al. Determination of HLA-A, -C, -B, -DRB1 allele and haplotype frequency in Japanese population based on family study. Tissue Antigens 2015, 85, 252–259. [Google Scholar] [CrossRef] [Green Version]
- Huh, J.Y.; Yi, D.Y.; Eo, S.; Cho, H.; Park, M.H.; Kang, M.S. HLA--A,--B and--DRB 1 polymorphism in K oreans defined by sequence--based typing of 4128 cord blood units. Int. J. Immunogenet. 2013, 40, 515–523. [Google Scholar] [CrossRef]
- Qin, Q.P.; Su, F.; Yan, X.W.; Xing, Z.; Meng, P.; Chengya, W.; Jie, S. Distribution of human leucocyte antigen--A,--B and--DR alleles and haplotypes at high resolution in the population from Jiangsu province of China. Int. J. Immunogenet. 2011, 38, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Chandanayingyong, D.; Stephens, H.A.; Klaythong, R.; Sirikong, M.; Udee, S.; Longta, P.; Chantangpol, R.; Bejrachandra, S.; Rungruang, E. HLA-A, -B, -DRB1, -DQA1, and -DQB1 polymorphism in thais. Hum. Immunol. 1997, 53, 174–182. [Google Scholar] [CrossRef]
- Pimtanothai, N.; Charoenwongse, P.; Mutirangura, A.; Hurley, C. Distribution of HLA-B alleles in nasopharyngeal carcinoma patients and normal controls in Thailand. Tissue Antigens 2002, 59, 223–225. [Google Scholar] [CrossRef]
- Pan, Q.-Q.; Fan, S.; Wang, X.-Y.; Pan, M.; Zhao, X.; Zhou, X.-Y.; Wang, C.-Y.; Shen, J. The distribution of human leukocyte antigen-A, -B, and -DRB1 alleles and haplotypes based on high-resolution genotyping of 167 families from Jiangsu Province, China. Hum. Immunol. 2011, 72, 872–876. [Google Scholar] [CrossRef] [PubMed]
- Hong, W.; Fu, Y.; Chen, S.; Wang, F.; Ren, X.; Xu, A. Distributions of HLA class I alleles and haplotypes in Northern Han Chinese. Tissue Antigens 2005, 66, 297–304. [Google Scholar] [CrossRef]
- Yao, Y.; Shi, L.; Matsushita, M.; Yu, L.; Lin, K.; Tao, Y.; Huang, X.; Yi, W.; Oka, T.; Tokunaga, K.; et al. Distribution of HLA-A, -B, -Cw, and -DRB1 alleles and haplotypes in an isolated Han population in Southwest China. Tissue Antigens 2009, 73, 561–568. [Google Scholar] [CrossRef]
- Romphruk, A.V.; Romphruk, A.; Kongmaroeng, C.; Klumkrathok, K.; Paupairoj, C.; Leelayuwat, C. HLA class I and II alleles and haplotypes in ethnic Northeast Thais. Tissue Antigens 2010, 75, 701–711. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.-K.; Mohd-Farid, B.; Salsabil, S.; Heselynn, H.; Wahinuddin, S.; Lau, I.-S.; Gun, S.-C.; Nor-Suhaila, S.; Eashwary, M.; Mohd-Shahrir, M.S.; et al. HLA-A, -B, -C, -DRB1 and -DQB1 alleles and haplotypes in 951 Southeast Asia Malays from Peninsular Malaysia. Hum. Immunol. 2016, 77, 818–819. [Google Scholar] [CrossRef]
- Seshasubramanian, V.; Manisekar, N.K.; Sathishkannan, A.D.; Naganathan, C.; Nandakumar, Y.; Narayan, S. Malayalam speaking population from South India: Common five-locus haplotypes in Malayalam speaking population. HLA 2018, 92, 432–434. [Google Scholar] [CrossRef]
- Hoa, B.K.; Hang, N.T.L.; Kashiwase, K.; Ohashi, J.; Lien, L.T.; Horie, T.; Shojima, J.; Hijikata, M.; Sakurada, S.; Satake, M.; et al. HLA-A, -B, -C, -DRB1 and -DQB1 alleles and haplotypes in the Kinh population in Vietnam. Tissue Antigens 2007, 71, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Yuliwulandari, R.; Sachrowardi, Q.; Nakajima, H.; Kashiwase, K.; Hirayasu, K.; Mabuchi, A.; Sofro, A.S.M.; Tokunaga, K. Association of HLA-A, -B, and -DRB1 with pulmonary tuberculosis in western Javanese Indonesia. Hum. Immunol. 2010, 71, 697–701. [Google Scholar] [CrossRef]
- Itoh, Y.; Mizuki, N.; Shimada, T.; Azuma, F.; Itakura, M.; Kashiwase, K.; Kikkawa, E.; Kulski, J.K.; Satake, M.; Inoko, H. High-throughput DNA typing of HLA-A, -B, -C, and -DRB1 loci by a PCR–SSOP–Luminex method in the Japanese population. Immunogenetics 2005, 57, 717–729. [Google Scholar] [CrossRef]
- Available online: http://allelefrequencies.net/pop6001c.asp?pop_id=1231 (accessed on 30 April 2021).
- Bannai, M.; Tokunaga, K.; Imanishi, T.; Harihara, S.; Fujisawa, K.; Juji, T.; Omoto, K. HLA class II alleles in Ainu living in Hidaka district, Hokkaido, northern Japan. Am. J. Phys. Anthr. 1996, 101, 1–9. [Google Scholar] [CrossRef]
- Cruccu, G.; Gronseth, G.; Alksne, J.; Argoff, C.; Brainin, M.; Burchiel, K.; Nurmikko, T.; Zakrewska, J.M.; American Academy of Neurology Society; European Federation of Neurological Society. AAN-EFNS guidelines on trigeminal neuralgia management. Eur. J. Neurol. 2008, 15, 1013–1028. [Google Scholar] [CrossRef]
- Marson, A.G.; Al-Kharusi, A.M.; Alwaidh, M.; Appleton, R.; Baker, A.G.; Chadwick, D.W.; Cramp, C.; Cockerell, O.C.; Cooper, P.N.; Doughty, J.; et al. The SANAD study of effectiveness of carbamazepine, gabapentin, lamotrigine, oxcarbazepine, or topiramate for treatment of partial epilepsy: An unblinded randomised controlled trial. Lancet 2007, 369, 1000–1015. [Google Scholar] [CrossRef] [Green Version]
- Fan, W.-L.; Shiao, M.-S.; Hui, R.C.-Y.; Su, S.-C.; Wang, C.-W.; Chang, Y.-C.; Chung-Yee, H.R. HLA Association with Drug-Induced Adverse Reactions. J. Immunol. Res. 2017, 2017, 3186328. [Google Scholar] [CrossRef] [PubMed]
- Khosama, H.; Budikayanti, A.; Khor, A.H.P.; Lim, K.S.; Ng, C.-C.; Mansyur, I.G.; Harahap, A.; Ranakusuma, T.A.R.; Tan, C.T. HLA-B* 1502 and carbamazepine induced Stevens-Johnson syndrome/toxic epidermal necrolysis in Indonesia. Neurol. Asia 2017, 22, 113–116. [Google Scholar]
- Yip, V.L.; Marson, A.G.; Jorgensen, A.L.; Pirmohamed, M.; Alfirevic, A. HLA Genotype and Carbamazepine-Induced Cutaneous Adverse Drug Reactions: A Systematic Review. Clin. Pharmacol. Ther. 2012, 92, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Van Nguyen, D.; Vidal, C.; Chu, H.C.; van Nunen, S. Developing pharmacogenetic screening methods for an emergent country: Vietnam. World Allergy Organ. J. 2019, 12, 100037. [Google Scholar] [CrossRef] [Green Version]
- Jaruthamsophon, K.; Tipmanee, V.; Sangiemchoey, A.; Sukasem, C.; Limprasert, P. HLA-B*15:21 and carbamazepine-induced Stevens-Johnson syndrome: Pooled-data and in silico analysis. Sci. Rep. 2017, 7, 45553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, T.Y.; Prajapati, L.M.; Mittal, B.; Joshi, C.G.; Sheth, J.J.; Patel, D.B.; Dave, D.M.; Goyal, R.K. Association of HLA-B* 1502 allele and carbamazepine-induced Stevens-Johnson syndrome among Indians. Indian J. Dermatol. Venereol. Leprol. 2009, 75, 579. [Google Scholar] [CrossRef] [PubMed]
- Man, C.B.; Kwan, P.; Baum, L.; Yu, E.; Lau, K.; Cheng, A.S.; Ng, M.H. Association between HLA-B*1502 Allele and Antiepileptic Drug-Induced Cutaneous Reactions in Han Chinese. Epilepsia 2007, 48, 1015–1018. [Google Scholar] [CrossRef] [PubMed]
- Kano, Y.; Hirahara, K.; Asano, Y.; Shiohara, T. HLA-B allele associations with certain drugs are not confirmed in Japanese patients with severe cutaneous drug reactions. Acta Derm. Venereol. 2008, 88, 616–618. [Google Scholar] [PubMed]
- Sukasem, C.; Chaichan, C.; Nakkrut, T.; Satapornpong, P.; Jaruthasopom, K.; Janatraroungtong, T.; Koomdee, N.; Sririttha, S.; Medhasi, S.; Oo-Puthinan, S.; et al. Association between HLA-B alleles and carbamazepine-induced macu-lopapular exanthema and severe cutaneous reactions in Thai patients. J. Immunol. Res. 2018, 2018, 2780272. [Google Scholar] [CrossRef] [Green Version]
- Tangamornsuksan, W.; Chaiyakunapruk, N.; Somkrua, R.; Lohitnavy, M.; Tassaneeyakul, W. Relationship between the HLA-B* 1502 allele and carbamazepine-induced Stevens-Johnson syndrome and toxic epidermal necrolysis: A systematic re-view and meta-analysis. JAMA Dermatol. 2013, 149, 1025–1032. [Google Scholar] [CrossRef] [Green Version]
- Ferrell, P.B.; McLeod, H.L. Carbamazepine, HLA-B* 1502 and risk of Stevens–Johnson syndrome and toxic epidermal necrolysis: US FDA recommendations. Pharmacogenomics 2008, 9, 1543–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.; Zhou, J.-Q.; Zhou, L.-M.; Chen, Z.-Y.; Fang, Z.-Y.; Chen, S.-D.; Yang, L.-B.; Cai, X.-D.; Dai, Q.-L.; Hong, H.; et al. Association between HLA-B*1502 allele and carbamazepine-induced severe cutaneous adverse reactions in Han people of southern China mainland. Seizure 2011, 20, 446–448. [Google Scholar] [CrossRef] [Green Version]
- Yip, V.L.M.; Alfirevic, A.; Pirmohamed, M. Genetics of Immune-Mediated Adverse Drug Reactions: A Comprehensive and Clinical Review. Clin. Rev. Allergy Immunol. 2015, 48, 165–175. [Google Scholar] [CrossRef]
- Locharernkul, C.; Shotelersuk, V.; Hirankarn, N. HLA-B* 1502 screening: Time to clinical practice. Epilepsia 2010, 51, 936–938. [Google Scholar] [CrossRef]
- Tassaneeyakul, W.; Prabmeechai, N.; Sukasem, C.; Kongpan, T.; Konyoung, P.; Chumworathayi, P.; Tiamkao, S.; Khunarkornsiri, U.; Kulkantrakorn, K.; Saksit, N.; et al. Associations between HLA class I and cytochrome P450 2C9 genetic polymorphisms and phenytoin-related severe cutaneous adverse reactions in a Thai population. Pharm. Genom. 2016, 26, 225–234. [Google Scholar] [CrossRef] [PubMed]
- McCormack, M.; Urban, T.J.; Shianna, K.V.; Walley, N.; Pandolfo, M.; Depondt, C.; Chaila, E.; O’Conner, G.; Kasperaviciute, D.; Radtke, R.A.; et al. Genome-wide mapping for clinically relevant predictors of lamotrigine-and phenytoin-induced hypersensitivity reactions. Pharmacogenomics 2012, 13, 399–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koomdee, N.; Pratoomwun, J.; Jantararoungtong, T.; Teeramoke, V.; Tassaneeyakul, W.; Klaewsongkram, J.; Rerkpattanpipat, T.; Santon, S.; Puangpetch, A.; Intusome, U.; et al. Association of HLA-A and HLA-B alleles with lamotrigi-ne-induced cutaneous adverse drug reactions in the Thai population. Front. Pharmacol. 2017, 8, 879. [Google Scholar] [CrossRef]
- Gerogianni, K.; Tsezou, A.; Dimas, K. Drug-induced skin adverse reactions: The role of pharmacogenomics in their pre-vention. Mol. Diagn. Ther. 2018, 22, 297–314. [Google Scholar] [CrossRef]
- Lonjou, C.; Borot, N.; Sekula, P.; Ledger, N.; Thomas, L.; Halevy, S.; Naldi, L.; Bouwes-Bavinck, J.-N.; Sidoroff, A.; de Toma, C.; et al. A European study of HLA-B in Stevens–Johnson syndrome and toxic epidermal necrolysis related to five high-risk drugs. Pharmacogenetics Genom. 2008, 18, 99–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazeem, G.R.; Cox, C.; Aponte, J.; Messenheimer, J.; Brazell, C.; Nelsen, A.C.; Nelson, M.R.; Foot, E. High-resolution HLA genotyping and severe cutaneous adverse reactions in lamotrigine-treated patients. Pharm. Genom. 2009, 19, 661–665. [Google Scholar] [CrossRef]
- Park, H.J.; Kim, S.R.; Leem, D.W.; Moon, I.J.; Koh, S.B.; Park, K.H.; Park, J.-W.; Lee, J.-H. Clinical features of and genetic predisposition to drug-induced Stevens–Johnson syndrome and toxic epidermal necrolysis in a single Korean tertiary institution patients—investigating the relation between the HLA-B* 4403 allele and lamotrigine. Eur. J. Clin. Pharmacol. 2015, 71, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Knowles, S.R.; Dewhurst, N.; Shear, N.H. Anticonvulsant hypersensitivity syndrome: An update. Expert Opin. Drug Saf. 2012, 11, 767–778. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Dao, R.-L.; Lee, T.-J.; Lu, C.-W.; Hung, S.-I.; Chung, W.-H. Severe cutaneous adverse reactions to antiepileptic drugs in Asians. Neurology 2011, 77, 2025–2033. [Google Scholar] [CrossRef]
- Kaniwa, N.; Sugiyama, E.; Saito, Y.; Kurose, K.; Maekawa, K.; Hasegawa, R.; Furuya, H.; Ikeda, H.; Takahashi, Y.; Muramatsu, M.; et al. Specific HLA types are associated with antiepileptic drug-induced Stevens–Johnson syndrome and toxic epidermal necrolysis in Japanese subjects. Pharmacogenomics 2013, 14, 1821–1831. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, J.; Wu, X.; Yu, P.; Hong, Z. HLA-B*1502 allele is associated with a cross-reactivity pattern of cutaneous adverse reactions to antiepileptic drugs. J. Int. Med. Res. 2012, 40, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Akkaif, M.A.; Sha’aban, A.; Daud, N.A.A.; Ng, M.L.; Ibrahim, B. Investigate the Strategy of Using Pharmacogenetics and Pharmacometabonomics to the Personalization of Ticagrelor Antiplatelet Therapy. Syst. Rev. Pharm. 2020, 11, 1100–1107. [Google Scholar]
- Nebert, D.W.; Russell, D.W. Clinical importance of the cytochromes P450. Lancet 2002, 360, 1155–1162. [Google Scholar] [CrossRef]
- Akkaif, M.A.; Daud, N.A.A.; Sha’aban, A.; Ng, M.L.; Kader, M.A.S.A.; Noor, D.A.M.; Ibrahim, B. The Role of Genetic Polymorphism and Other Factors on Clopidogrel Re-sistance (CR) in an Asian Population with Coronary Heart Disease (CHD). Molecules 2021, 26, 1987. [Google Scholar] [CrossRef]
- Gaedigk, A.; Ingelman--Sundberg, M.; Miller, N.A.; Leeder, J.S.; Whirl-Carillo, M.; Klein, T.E.; PharmVar Steering Committee. The Pharmacogene Variation (PharmVar) Consortium: Incorporation of the human cytochrome P450 (CYP) allele nomenclature database. Clin. Pharmacol. Ther. 2018, 103, 399–401. [Google Scholar] [CrossRef] [Green Version]
- Aithal, G.P.; Day, C.P.; Kesteven, P.J.; Daly, A.K. Association of polymorphisms in the cytochrome P450 CYP2C9 with warfarin dose requirement and risk of bleeding complications. Lancet 1999, 353, 717–719. [Google Scholar] [CrossRef]
- Miners, J.O.; Birkett, D.J. Cytochrome P4502C9: An enzyme of major importance in human drug metabolism. Br. J. Clin. Pharmacol. 1998, 45, 525–538. [Google Scholar] [CrossRef] [Green Version]
- Odani, A.; Hashimoto, Y.; Otsuki, Y.; Uwai, Y.; Hattori, H.; Furusho, K.; Inui, K. Genetic polymorphism of the CYP2C subfamily and its effect on the pharma-cokinetics of phenytoin in Japanese patients with epilepsy. Clin. Pharmacol. Ther. 1997, 62, 287–292. [Google Scholar] [CrossRef]
- Aynacioglu, A.S.; Brockmöller, J.; Bauer, S.; Sachse, C.; Güzelbey, P.; Öngen, Z.; Nacak, M.; Roots, I. Frequency of cytochrome P450 CYP2C9 variants in a Turkish population and functional relevance for phenytoin. Br. J. Clin. Pharmacol. 1999, 48, 409–415. [Google Scholar] [CrossRef] [Green Version]
- van der Weide, J.; Steijns, L.S.W.; van Weelden, M.J.M.; de Haan, K. The effect of genetic polymorphism of cytochrome P450 CYP2C9 on phenytoin dose requirement. Pharmacogenet. Genom. 2001, 11, 287–291. [Google Scholar] [CrossRef]
- Saruwatari, J.; Ishitsu, T.; Nakagawa, K. Update on the genetic polymorphisms of drug-metabolizing enzymes in an-tiepileptic drug therapy. Pharmaceuticals 2010, 3, 2709–2732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morton Grove IMGPI. PHENYTOIN Suspension. Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=efd93f07-818b-41ae-abd6-49ec5175311a (accessed on 30 April 2021).
- Yang, Z.; Cui, H.; Hasi, T.; Jia, S.; Gong, M.; Su, X. Genetic polymorphisms of cytochrome P450 enzymes 2C9 and 2C19 in a healthy Mongolian population in China. Genet. Mol. Res. 2010, 9, 1844–1851. [Google Scholar] [CrossRef]
- Park, P.-W.; Seo, Y.H.; Ahn, J.Y.; Kim, K.-A.; Park, J.-Y. Effect ofCYP3A5*3genotype on serum carbamazepine concentrations at steady-state in Korean epileptic patients. J. Clin. Pharm. Ther. 2009, 34, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Cheong, H.S.; Kim, L.H.; Kim, J.O.; Seo, D.W.; Kim, Y.H.; Chung, M.W.; Han, S.Y.; Shin, H.D. Screening of Genetic Polymorphisms of CYP3A4 and CYP3A5 Genes. Korean J. Physiol. Pharmacol. 2013, 17, 479–484. [Google Scholar] [CrossRef] [Green Version]
- Seo, T.; Nakada, N.; Ueda, N.; Hagiwara, T.; Hashimoto, N.; Nakagawa, K.; Ishitsu, T. Effect of CYP3A5*3 on carbamazepine pharmacokinetics in Japanese patients with epilepsy. Clin. Pharmacol. Ther. 2006, 79, 509–510. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.-H.; Chang, W.-C.; Lee, Y.-S.; Wu, Y.-Y.; Yang, C.-H.; Ho, H.-C.; Chen, M.-J.; Lin, J.-Y.; Hui, R.C.-Y.; Ho, J.-C.; et al. Genetic Variants Associated With Phenytoin-Related Severe Cutaneous Adverse Reactions. JAMA 2014, 312, 525–534. [Google Scholar] [CrossRef] [Green Version]
- Samidorai, A.; Charles, N.S.C.; Babu, S.P.K.K.; Ramesh, V. Cytochrome P450 2C9 gene polymorphism in phenytoin induced gingival enlargement: A case report. J. Pharm. Bioallied Sci. 2013, 5, 237–239. [Google Scholar] [CrossRef]
- Silvado, C.E.; Terra, V.C.; Twardowschy, C.A. CYP2C9 polymorphisms in epilepsy: Influence on phenytoin treatment. Pharmacogenomics Pers. Med. 2018, 11, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phabphal, K.; Geater, A.; Limapichart, K.; Sathirapanya, P.; Setthawatcharawanich, S. Role of CYP2C9 polymorphism in phenytoin-related metabolic abnormalities and subclinical atherosclerosis in young adult epileptic patients. Seizure 2013, 22, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Seng, K.C.; Gin, G.G.; Sangkar, J.V.; Phipps, M.E. Frequency of cytochrome P450 2C9 (CYP2C9) alleles in three ethnic groups in Malaysia. Asia Pac. J. Mol. Biol. Biotechnol. 2003, 11, 83–91. [Google Scholar]
- Saruwatari, J.; Ishitsu, T.; Seo, T.; Shimomasuda, M.; Okada, Y.; Goto, S.; Nagata, R.; Takashima, A.; Yoshida, S.; Yoshida, S.; et al. The clinical impact of cytochrome P450 polymorphisms on anti-epileptic drug therapy. Epilepsy Seizure 2010, 3, 34–50. [Google Scholar] [CrossRef]
- Goto, S.; Seo, T.; Murata, T.; Nakada, N.; Ueda, N.; Ishitsu, T.; Nakagawa, K. Population Estimation of the Effects of Cytochrome P450 2C9 and 2C19 Polymorphisms on Phenobarbital Clearance in Japanese. Ther. Drug Monit. 2007, 29, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Toh, D.S.L.; Tan, L.L.; Aw, D.C.W.; Pang, S.M.; Lim, S.H.; Thirumoorthy, T.; Lee, H.Y.; Tay, Y.K.; Tan, S.K.; Vasudevan, A.; et al. Building pharmacogenetics into a pharmacovigilance program in Singapore: Using serious skin rash as a pilot study. Pharm. J. 2014, 14, 316–321. [Google Scholar] [CrossRef]
- White, K.D.; Abe, R.; Ardern-Jones, M.; Beachkofsky, T.; Bouchard, C.; Carleton, B.; Chodosh, J.; Cibotti, R.; Davis, R.; Denny, J.C.; et al. SJS/TEN 2017: Building Multidisciplinary Networks to Drive Science and Translation. J. Allergy Clin. Immunol. Pr. 2018, 6, 38–69. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Lin, J.-J.; Lu, C.-S.; Ong, C.-T.; Hsieh, P.F.; Yang, C.-C.; Tai, C.-T.; Wu, S.-L.; Lu, C.-H.; Hsu, Y.-C.; et al. Carbamazepine-Induced Toxic Effects and HLA-B*1502 Screening in Taiwan. New Engl. J. Med. 2011, 364, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.; Bousman, C.A. Commercial Pharmacogenetic Tests in Psychiatry: Do they Facilitate the Implementation of Pharmacogenetic Dosing Guidelines? Pharmacopsychiatry 2020, 53, 174–178. [Google Scholar] [CrossRef] [Green Version]



| AEDs | HLA Alleles | Population/Ethnicity | Phenotype | Reference |
|---|---|---|---|---|
| Carbamazepine | HLA-A*02:01 | Iranian | SJS | [55] |
| HLA-A*31:01 | DRESS | |||
| MPE | [56,57,58,59,60] | |||
| Caucasian | SJS/TEN | |||
| Japanese | ||||
| DRESS, | [60] | |||
| SJS/TEN | ||||
| Korean | ||||
| DRESS, | ||||
| MPE, | ||||
| Han Chinese | ||||
| HLA-A*51:01 | Iranian | SJS | [55] | |
| HLA-B*15:02 | Han Chinese | SJS/TEN | [9,51,61,62,63,64] | |
| Thai | ||||
| Malay | ||||
| Indian | ||||
| Vietnamese | ||||
| Indonesian | ||||
| HLA-B∗15:08 | Indian | SJS/TEN | [65] | |
| HLA-B*15:11 | Japanese | SJS/TEN | [66] | |
| Korean | [58] | |||
| HLA-B*15:18 | Japanese | SJS/TEN | [67] | |
| HLA-B*15:21 | Filipino | SJS/TEN | [68] | |
| Phenytoin | HLA-B*15:02 | Han Chinese | SJS/TEN | [69] |
| Thai | [70] | |||
| Malay | [71] | |||
| HLA-B*15:13 | Malay | SJS/TEN | [71] | |
| Lamotrigine | HLA-B*15:01 | Han Chinese | SJS/TEN | [69] |
| [72] | ||||
| Phenobarbital | HLA-B*13:01 | Thai | SJS/TEN | [73] |
| Han Chinese | ||||
| HLA--B*51:01 | Japanese | SJS/TEN | [11] |
| HLA Alleles | Population/Ethnicity | Allele Frequency | Reference |
|---|---|---|---|
| HLA-A | |||
| HLA-A*02:01 | Iranian | 0.202 | [74] |
| HLA-A*31:01 | Caucasian | 0.0214 | [75] |
| Japanese | 0.084 | [76] | |
| Korean | 0.0562 | [77] | |
| Han Chinese | 0.0307 | [78] | |
| HLA-B | |||
| HLA-B*13:01 | Thai | 0.210–0.0410 | [79,80] |
| Han Chinese | 0.0405 | [81] | |
| HLA-B*15:01 | Han Chinese | 0.038 | [82] |
| HLA-B*15:02 | Han Chinese | 0.0190–0.1240 | [82,83] |
| Thai | 0.084 | [84] | |
| Malay | 0.1225 | [85] | |
| Indian | 0.013 | [86] | |
| Vietnamese | 0.135 | [87] | |
| Indonesian | 0.122 | [88] | |
| HLA-B*15:11 | Japanese | 0.0088 | [76] |
| Korean | 0.0166 | [77] | |
| HLA-B*15:13 | Malay | 0.0599 | [85] |
| HLA-B*15:18 | Japanese | 0.0152 | [89] |
| HLA-B*15:21 | Filipino | 0.01 | [90] |
| HLA-B*51:01 | Japanese | 0.07–0.9 | [91] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, A.F.; Sukasem, C.; Sabbah, M.A.; Musa, N.F.; Mohamed Noor, D.A.; Daud, N.A.A. Genetic Determinants in HLA and Cytochrome P450 Genes in the Risk of Aromatic Antiepileptic-Induced Severe Cutaneous Adverse Reactions. J. Pers. Med. 2021, 11, 383. https://doi.org/10.3390/jpm11050383
Ahmed AF, Sukasem C, Sabbah MA, Musa NF, Mohamed Noor DA, Daud NAA. Genetic Determinants in HLA and Cytochrome P450 Genes in the Risk of Aromatic Antiepileptic-Induced Severe Cutaneous Adverse Reactions. Journal of Personalized Medicine. 2021; 11(5):383. https://doi.org/10.3390/jpm11050383
Chicago/Turabian StyleAhmed, Ali Fadhel, Chonlaphat Sukasem, Majeed Arsheed Sabbah, Nur Fadhlina Musa, Dzul Azri Mohamed Noor, and Nur Aizati Athirah Daud. 2021. "Genetic Determinants in HLA and Cytochrome P450 Genes in the Risk of Aromatic Antiepileptic-Induced Severe Cutaneous Adverse Reactions" Journal of Personalized Medicine 11, no. 5: 383. https://doi.org/10.3390/jpm11050383