
Systematic Identification of Familial Hypercholesterolaemia in Primary Care—A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Types of Study
2.1.2. Types of Participant
2.1.3. Types of Intervention
2.1.4. Types of Outcome Measure
Primary Outcomes:
- Diagnosis of definite FH (i.e., a positive genetic mutation or clinical characteristics of FH);
- Diagnosis of possible and probable FH (as defined by diagnostic criteria);
- Adverse events associated with the intervention.
Secondary Outcomes:
- Cholesterol levels;
- Cardiovascular mortality and morbidity (minimum of one-year follow-up);
- Lipid-lowering treatment;
- Referral to a specialist service;
- Adverse self-reported psychological effects.
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Synthesis
3. Results
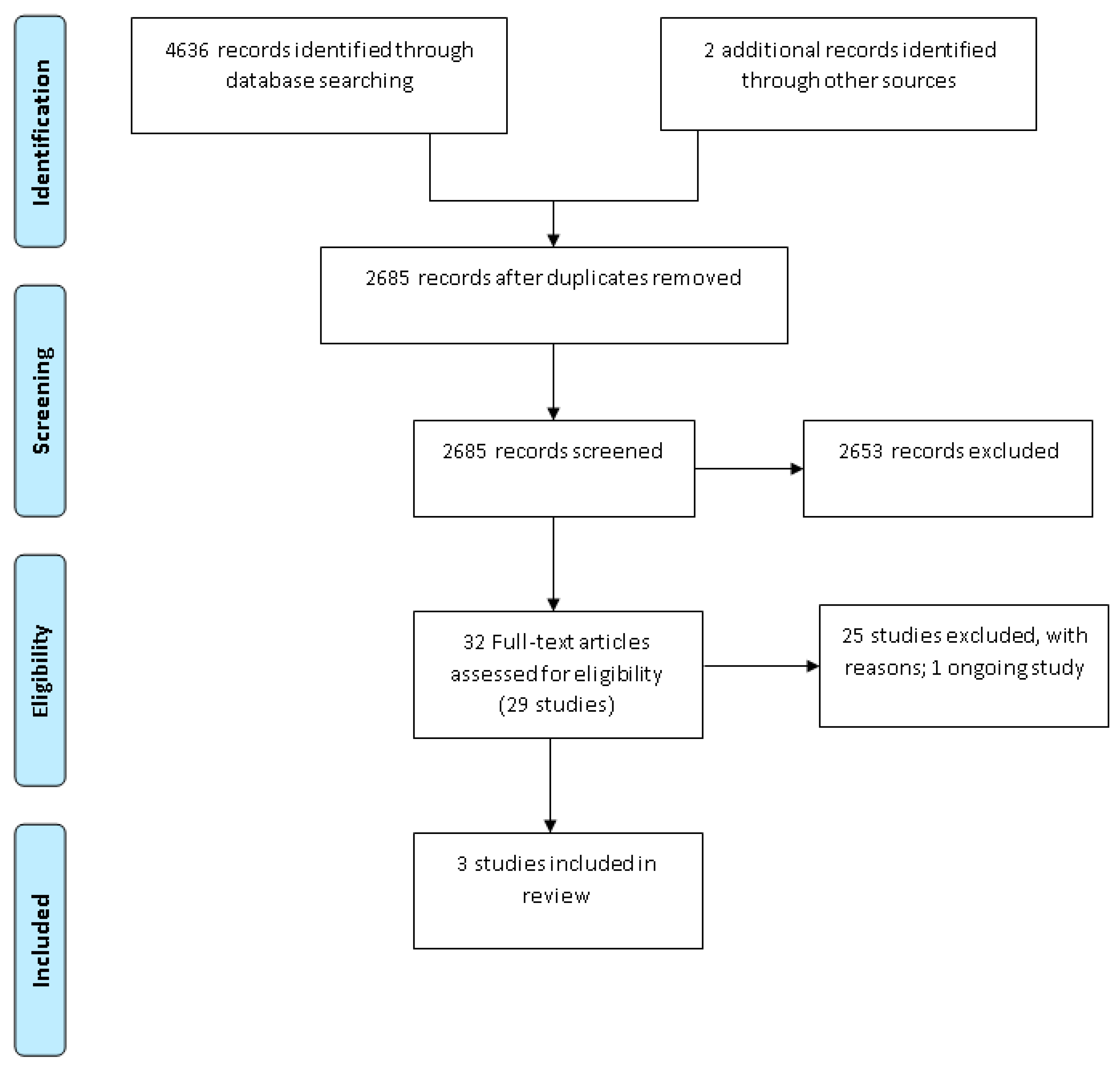
3.1. Study Selection
3.2. Characteristics of Included Studies
3.2.1. Diagnosis of Definite FH
3.2.2. Diagnosis of Possible and Probable FH
3.2.3. Adverse Events Associated with the Intervention
3.2.4. Cholesterol Levels
3.2.5. Cardiovascular Mortality and Morbidity
3.2.6. Lipid-Lowering Treatment
3.2.7. Referral to a Specialist Service
3.2.8. Adverse Self-Reported Psychological Effects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nordestgaard, B.G.; Chapman, M.J.; Humphries, S.E.; Ginsberg, H.N.; Masana, L.; Descamps, O.S.; Wiklund, O.; Hegele, R.A.; Raal, F.J.; Defesche, J.C.; et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: Guidance for clinicians to prevent coronary heart disease: Consensus statement of the European Atherosclerosis Society. Eur. Heart J. 2013, 34, 3478–3490. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Bittner, V. Familial Hypercholesterolaemia—Epidemiology, Diagnosis and Screening. Curr. Atheroscler. Rep. 2015, 17, 3. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Bestwick, J.P.; Morris, J.K.; Whyte, K.; Jenkins, L.; Wald, N.J. Child–Parent Familial Hypercholesterolemia Screening in Primary Care. N. Engl. J. Med. 2016, 375, 1628–1637. [Google Scholar] [CrossRef] [PubMed]
- Demott, K.; Nherera, L.; Shaw, E.J.; Minhas, R.; Humphries, S.E.; Kathoria, M.; Ritchie, G.; Nunes, V.; Davies, D.; Lee, P.; et al. Clinical Guidelines and Evidence Review for Familial Hypercholesterolaemia: The Identification and Management of Adults and Children with Familial Hypercholesterolaemia; National Collaborating Centre for Primary Care and Royal College of General Practitioners: London, UK, 2008. [Google Scholar]
- Besseling, J.; Reitsma, J.B.; Hovingh, G.K.; Hutten, A. Predicting the presence of a mutation resulting in familial hypercholesterolemia-development of a prediction model in a cohort of 64,000 subjects. Circulation 2014, 130 (Suppl. 2), A16172. [Google Scholar]
- Qureshi, N.; Humphries, S.E.; Seed, M.; Rowlands, P.; Minhas, R. Identification and management of familial hypercholesterolaemia: What does it mean to primary care? Br. J. Gen. Pr. 2009, 59, 773–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, A.; Hopkins, M.D.; Toth, P.; Ballantyne, C.M.; Rader, D.J.; Robinson, J.G.; Daniels, S.R.; Gidding, S.S.; De Ferranti, S.D.; Ito, M.K.; et al. Familial hypercholesterolemia: Screening, diagnosis and management of pediatric and adult patients: Clinical guidance from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J. Clin. Lipidol. 2011, 5 (Suppl. 3), 133–140. [Google Scholar] [CrossRef] [PubMed]
- Harada-Shiba, M.; Arai, H.; Okamura, T.; Yokote, K.; Oikawa, S.; Nohara, A.; Okada, T.; Ohta, T.; Bujo, H.; Watanabe, M.; et al. Multicenter study to determine the diagnosis criteria of heterozygous familial hypercholesterolemia in Japan. J. Atheroscler. Thromb. 2012, 19, 1019–1026. [Google Scholar] [CrossRef] [Green Version]
- Hata, Y.; Mabuchi, H.; Saito, Y.; Itakura, H.; Egusa, G.; Ito, H.; Teramoto, T.; Tsushima, M.; Tada, N.; Oikawa, S.; et al. Report of the Japan Atherosclerosis Society (JAS) Guideline for Diagnosis and Treatment of Hyperlipidemia in Japanese Adults. J. Atheroscler. Thromb. 2002, 9, 1–27. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. Familial Hypercholesterolaemia: Identification and Management: Update Clinical Guideline 71. 2019. Available online: www.niceorguk/guidance/cg71 (accessed on 17 June 2020).
- Simon Broome Register Group. Risk of fatal coronary heart disease in familial hypercholesterolaemia. Scientific Steering Committee on behalf of the Simon Broome Register Group. BMJ 1991, 303, 893. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, D.; Watts, G.; Hamilton, I. Guidelines for the Diagnosis and Management of Familial Hypercholesterolaemia; Cardiac Society of Australia and New Zealand: Sydney, Australia, 2013; Available online: https://csanz.edu.au/wp-content/uploads/2013/12/Familial_Hypercholesterolemia_2013.pdf (accessed on 27 September 2020).
- Williams, R.R.; Hunt, S.C.; Schumacher, M.; Hegele, R.A.; Leppert, M.F.; Ludwig, E.H.; Hopkins, P.N. Diagnosing heterozygous familial hypercholesterolemia using new practical criteria validated by molecular genetics. Am. J. Cardiol. 1993, 72, 171–176. [Google Scholar] [CrossRef]
- Defesche, J.C.; Lansberg, P.J.; Umans-Eckenhausen, M.A.; Kastelein, J.J. Advanced method for the identification of patients with familial hypercholesterolaemia. Semin. Vasc. Med. 2004, 4, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Reiner, Z.; Catapano, A.L.; De Backer, G.; Graham, I.; Taskinen, M.R.; Wilkund, O.; Agewall, S.; Alegria, E.; Chapman, M.J.; Durrington, P.; et al. ESC/EAS Guidelines for management of dyslipidaemias. Eur. Heart J. 2011, 32, 1769–1818. [Google Scholar] [CrossRef]
- Watts, G.F.; Sullivan, D.R.; Poplawski, N.; van Bockxmeer, F.; Hamilton-Craig, I.; Clifton, P.M.; O’Brien, R.; Bishop, W.; George, P.; Barter, P.J.; et al. Familial hypercholesterolaemia: A model of care for Australasia. Atheroscler. Suppl. 2011, 12, 221–263. [Google Scholar] [CrossRef]
- Gidding, S.S.; Champagne, M.A.; de Ferranti, S.D.; Defesche, J.; Ito, M.K.; Knowles, J.W.; McCrindle, B.; Raal, F.; Rader, D.; Santos, R.D.; et al. The agenda for familial hypercholesterolaemia: A scientific statement from the American Heart Association. Circulation 2015, 132, 2167–2192. [Google Scholar] [CrossRef]
- Vallejo-Vaz, A.J.; Kondapally Seshasai, S.R.; Cole, D.; Hovingh, G.K.; Kastelein, J.J.; Mata, P.; Raal, F.J.; Santos, R.D.; Soran, H.; Watts, G.F.; et al. Familial hypercholesterolaemia: A global call to arms. Atherosclerosis 2015, 243, 257–259. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.1 (Updated September 2020); Cochrane: London, UK, 2020; Available online: www.training.cochrane.org/handbook (accessed on 12 February 2021).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qureshi, N.; Weng, S.F.; Tranter, J.A.; Da Silva, M.L.; Kai, J.; Leonardi-Bee, J. Strategies for identifying familial hypercholesterolaemia in non-specialist clinical settings (protocol). Cochrane Database Syst. Rev. 2018, CD012985. [Google Scholar] [CrossRef]
- Reeves, M.M.; Terranova, C.O.; Erickson, J.M.; Job, J.R.; Brookes, D.S.K.; McCarthy, N.; Hickman, I.J.; Lawler, S.P.; Fjeldsoe, B.S.; Healy, G.N.; et al. Living well after breast cancer randomized controlled trial protocol: Evaluating a telephone-delivered weight loss intervention versus usual care in women following treatment for breast cancer. BMC Cancer 2016, 16, 830. [Google Scholar] [CrossRef]
- Heart UK—The Cholesterol Charity. Available online: https://www.heartuk.org.uk (accessed on 27 September 2020).
- The British Heart Foundation. Available online: https://thefhfoundation.org/ (accessed on 27 September 2020).
- Scottish Intercollegiate Guidelines Network. Available online: www.sign.ac.uk (accessed on 27 September 2020).
- Sterne, J.A.; Higgins, J.P.; Reeves, B.C.; on behalf of the development group for ROBINS-1. ROBINS-1: A Tool for Assessing Risk of Bias in Non-Randomized Studies of Interventions (Version 7). Available online: www.riskofbias.info (accessed on 5 January 2017).
- Bell, D.A.; Bender, R.; Hooper, A.J.; McMahon, J.; Edwards, G.; Van Bockxmeer, F.M.; Watts, G.F.; Burnett, J.R. Impact of interpretative commenting on lipid profiles in people at high risk of familial hypercholesterolaemia. Clin. Chim. Acta 2013, 422, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Green, P.H.; Neely, D.; Humphries, S.E.; Saunders, T.; Gray, V.; Gordon, L.; Payne, J.; Carter, S.; Neuwirth, C.; Rees, A.; et al. Improving detection of familial hypercholesterolaemia in primary care using electronic audit and nurse-led clinics. J. Eval. Clin. Pr. 2016, 22, 341–348. [Google Scholar] [CrossRef]
- Weng, S.; Kai, J.; Tranter, J.; Leonardi-Bee, J.; Qureshi, N. Improving identification and management of familial hypercholesterolaemia in primary care: Pre- and post-intervention study. Atherosclerosis 2018, 274, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, D.A.; Hooper, A.J.; Bender, R.; McMahon, J.; Edwards, G.; Van Bockxmeer, F.M.; Watts, G.F.; Burnett, J.R. Opportunistic screening for familial hypercholesterolaemia via a community laboratory. Ann. Clin. Biochem. Int. J. Lab. Med. 2012, 49, 534–537. [Google Scholar] [CrossRef]
- Bell, D.; Hooper, A.; Edwards, G.; Southwell, L.; Pang, J.; Van Bockxmeer, F.; Watts, G.; Burnett, J. Impact of Telephoning the Requestors of Individuals Found to be at High Risk of Familial Hypercholesterolaemia. Hear. Lung Circ. 2013, 22, S230. [Google Scholar] [CrossRef] [Green Version]
- Bell, D.A.; Kirke, A.B.; Barbour, R.; Southwell, L.; Pang, J.; Burrows, S.; Watts, G.F. Can Patients be Accurately Assessed for Familial Hypercholesterolaemia in Primary Care? Hear. Lung Circ. 2014, 23, 1153–1157. [Google Scholar] [CrossRef]
- Bell, D.A.; Edwards, G.; Hooper, A.J.; McMahon, J.; Van Bockxmeer, F.M.; Watts, G.F.; Burnett, J.R. The potential role of an expert computer system to augment the opportunistic detection of individuals with familial hypercholesterolaemia from a community laboratory. Clin. Chim. Acta 2015, 448, 18–21. [Google Scholar] [CrossRef]
- Bender, R.; Edwards, G.; McMahon, J.; Hooper, A.J.; Watts, G.F.; Burnett, J.R.; Bell, D.A. Interpretative comments specifically suggesting specialist referral increase the detection of familial hypercholesterolaemia. Pathology 2016, 48, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Benn, M.; Watts, G.F.; Tybjaerg-Hansen, A.; Nordestgaard, B.G. Familial hypercholesterolaemia in the Danish general population: Prevalence, coronary artery disease, and cholesterol-lowering medication. J. Clin. Endocrinol. Metab. 2012, 97, 3956–3964. [Google Scholar] [CrossRef]
- Casula, M.; Catapano, A.L.; Bernardi, L.R.; Visconti, M.; Aronica, A. Detection of familial hypercholesterolaemia in patients from a general practice database. Atheroscler. Suppl. 2017, 29, 25–30. [Google Scholar] [CrossRef]
- Elis, A.; Leventer-Roberts, M.; Bachrach, A.; Lieberman, N.; Durst, R.; Knobler, H.; Balicer, R. The characteristics of patients with possible familial hypercholesterolemia—screening a large payer/provider healthcare delivery system. QJM 2020, 113, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.; Jaiyeola, A.; Whiting, M.; Modell, M.; Wierzbicki, A.S. Identifying patients with familial hypercholesterolaemia in primary care: An informatics-based approach in one primary care centre. Heart 2008, 94, 754–758. [Google Scholar] [CrossRef]
- Jayne, Z.; Lungley, J.; Harvey, D.; Stuart, A.; Nair, D. Specialist Familial Hypercholesterolaemia (FH) nurses in primary care for identification of FH index cases. Atherosclerosis 2016, 245, e250. [Google Scholar] [CrossRef]
- Kirke, A.B.; Barbour, R.A.; Burrows, S.; Bell, D.A.; Vickery, A.W.; Emery, J.; Watts, G.F. Systematic Detection of Familial Hypercholesterolaemia in Primary Health Care: A Community Based Prospective Study of Three Methods. Hear. Lung Circ. 2015, 24, 250–256. [Google Scholar] [CrossRef]
- Qureshi, N.; Weng, S.; Tranter, J.; El-Kadiki, A.; Kai, J. Feasibility of improving identification of familial hypercholesterolaemia in general practice: Intervention development study. BMJ Open 2016, 6, e011734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safarova, M.S.; Liu, H.; Kullo, I.J. Rapid identification of familial hypercholesterolaemia from electronic health records: The SEARCH study. J. Clin. Lipidol. 2016, 10, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Shipman, K.; Ganeshamoorthy, S.; Labib, M. Audit of the diagnosis of familial hypercholesterolaemia in primary care. Atherosclerosis 2014, 236, e306. [Google Scholar] [CrossRef]
- Troeung, L.; Arnold-Reed, D.; Ping-Delfos, W.C.S.; Watts, G.F.; Pang, J.; Lugonja, M.; Bulsara, M.; Mortley, D.; James, M.; Brett, T. A new electronic screening tool for identifying risk of familial hypercholesterolaemia in general practice. Heart 2016, 102, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Vickery, A.W.; Ryan, J.; Pang, J.; Garton-Smith, J.; Watts, G.F. Increasing the Detection of Familial Hypercholesterolaemia Using General Practice Electronic Databases. Hear. Lung Circ. 2017, 26, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Zamora, A.; Masana, L.; Comas-Cufi, M.; Vila, A.; Plana, N.; Garcia-Gil, M.; Alves-Cabratosa, L.; Marrugat, J.; Roman, I.; Ramos, R. Familial hypercholesterolaemia in a European Mediterranean population—Prevalence and clinical data from 2.5 million primary care patients. J. Clin. Lipidol. 2017, 11, 1013–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amor-Salamanca, A.; Castillo, S.; Gonzalez-Vioque, E.; Dominguez, F.; Quintana, L.; Lluís-Ganella, C.; Escudier, J.M.; Ortega, J.; Lara-Pezzi, E.; Alonso-Pulpon, L.; et al. Genetically Confirmed Familial Hypercholesterolemia in Patients with Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2017, 70, 1732–1740. [Google Scholar] [CrossRef]
- Benlian, P.; Turquet, A.; Carrat, F.; Amsellem, S.; Sanchez, L.; Briffaut, D.; Girardet, J.P. Diagnosis scoring for clinical identification of children with heterozygous familial hypercholesterolaemia. J. Pediatr. Gastroenterol. Nutr. 2009, 48, 456–463. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. IN-TANDEM Familial Hypercholesterolemia Pilot Study; National Library of Medicine (US): Bethesda, MD, USA, 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT03253432 (accessed on 27 September 2020).
- ClinicalTrials.gov. Prevalence of Familial Hypercholesterolaemia (FH) in Italian Patients with Coronary Artery Disease; National Library of Medicine (US): Bethesda, MD, USA, 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT03520140 (accessed on 27 September 2020).
- ClinicalTrials.gov. A Prospective Pilot Study of Screening out Rate and Clinical Management of Familial Hypercholesterolemia; National Library of Medicine (US): Bethesda, MD, USA, 2019. Available online: https://clinicaltrials.gov/ct2/show/NCT03398954 (accessed on 27 September 2020).
- Nanchen, D.; Gencer, B.; Auer, R.; Räber, L.; Stefanini, G.G.; Klingenberg, R.; Schmied, C.M.; Cornuz, J.; Muller, O.; Vogt, P.; et al. Prevalence and management of familial hypercholesterolaemia in patients with acute coronary syndromes. Eur. Hear. J. 2015, 36, 2438–2445. [Google Scholar] [CrossRef]
- Steyn, K.; Fourie, J.M.; Shepherd, J. Detection and measurement of hypercholesterolaemia in South Africans attending general practitioners in private practice—The cholesterol monitor. S. Afr. Med. J. 1998, 88, 1569–1574. [Google Scholar]
- Aref-Eshghi, E.; Oake, J.; Godwin, M.; Aubrey-Bassler, K.; Duke, P.; Mahdavian, M.; Asghari, S. Identification of Dyslipidemic Patients Attending Primary Care Clinics Using Electronic Medical Record (EMR) Data from the Canadian Primary Care Sentinel Surveillance Network (CPCSSN) Database. J. Med. Syst. 2017, 41, 45. [Google Scholar] [CrossRef] [PubMed]
- E Arnold-Reed, D.; Brett, T.; Troeung, L.; Vickery, A.; Garton-Smith, J.; Bell, D.; Pang, J.; Grace, T.; Bulsara, C.; Li, I.; et al. Detection and management of familial hypercholesterolaemia in primary care in Australia: Protocol for a pragmatic cluster intervention study with pre-post intervention comparisons. BMJ Open 2017, 7, e017539. [Google Scholar]
- Lan, N.S.; Martin, A.C.; Brett, T.; Watts, G.F.; Bell, D.A. Improving the detection of familial hypercholesterolaemia. Pathology 2019, 51, 213–221. [Google Scholar] [CrossRef]
- Weng, S.; Kai, J.; Akyea, R.; Qureshi, N. Detection of familial hypercholesterolaemia: External validation of the FAMCAT clinical case-finding algorithm to identify patients in primary care. Lancet Public Health 2019, 4, e256–e264. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Study and Year | Design/ Setting | Participants | Intervention | Outcomes | Comparisons | Main Results | ||
|---|---|---|---|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | Absolute Difference (95% CI), n | ||||||
| Bell et al., 2013 | Uncontrolled BA study General practices in Western Australia | 96 Patients Gender: Female 68 (70.9%), Male 28 (29.1%) Age (years): mean ± SD [range]: 53.7 ± 10.7 [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57] | Interpretative comments added to lipid results | -FH diagnosis (Modified DLCN criteria) -LDL-c level -Referral to specialist | No comments added to lipid results (standard/usual care) | Definite FH: 0/96 (0%) Possible FH: 0/96 (0%) | Definite FH: 2/96 (2.08%) Possible FH: 2/96 (2.08%) | Definite FH: 2.08% (–2.05 to 7.28%), n = 96 Possible FH: 2.08% (–2.05 to 7.28%), n = 96 |
| Green et al., 2016 | Uncontrolled BA study with two sequential interventions. General practices in South East England | Approximately 290,000 patients Gender: not reported Age: In 2011, 37,200 people were aged >65 years and 4400 aged >85 years | 1: computer based reminder message 2: FH Nurse Advisor Programme—2-part process. Part 1 as above; Part 2 involved consultation with nurse to collect further information | -FH diagnosis (Baseline: S-B; Post-interv: S-B and/or DLCN criteria) | Baseline prevalence of FH | EHR Search and reminder | ||
| Definite FH: 331/262,030 (0.13%) Possible FH: 12/262,030 (0.005%) | Definite FH 354/199,346 (0.18%) Possible FH: 88/199,346 (0.04%) | Definite FH: 0.05% (0.03 to 0.07%), n = 262,030 Possible FH: 0.04% (–0.03 to 0.05%), n = 262,030 | ||||||
| EHR search and reminder + nurse intervention | ||||||||
| Definite FH: 331/262,030 (0.13%) Possible FH: 12/262,030 (0.005%) | Definite FH: 546/281,655 (0.19%) Possible FH: 147/281,655 (0.05%) | Definite FH: 0.07% (0.05 to 0.09%), n = 262,030 Possible FH: 0.05% (0.04 to 0.06%), n = 262,030 | ||||||
| Weng et al., 2018 | Uncontrolled BA study Six General Practices in Central England | 831 identified, 118 patients medical records accessed Gender: Female 46 (39%), Male 72 (61%) Age (years) mean (SD): male 58 (9.0), female 56 (7.5) | Combined approach: Opportunistic recruitment following computer-based reminder message with systematic postal recruitment of eligible patients | -FH diagnosis (S-B criteria) -Cholesterol -Statins prescribed | Same 118 participants with Cholesterol ≥ 7.5 mmol/L after the release of the NICE FH guidelines | Definite FH: 0/118 (0%) Possible FH: 0/118 (0%) | Definite FH: 2/118 (1.69%) Possible FH: 30/118 (25.42%) | Definite FH: 1.69% (–1.69 to 5.97%), n = 118 Possible FH: 25.42% (17.75 to 33.97%), n = 118 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, L.; Qureshi, N.; Abdul-Hamid, H.; Weng, S.; Kai, J.; Leonardi-Bee, J. Systematic Identification of Familial Hypercholesterolaemia in Primary Care—A Systematic Review. J. Pers. Med. 2021, 11, 302. https://doi.org/10.3390/jpm11040302
Silva L, Qureshi N, Abdul-Hamid H, Weng S, Kai J, Leonardi-Bee J. Systematic Identification of Familial Hypercholesterolaemia in Primary Care—A Systematic Review. Journal of Personalized Medicine. 2021; 11(4):302. https://doi.org/10.3390/jpm11040302
Chicago/Turabian StyleSilva, Luisa, Nadeem Qureshi, Hasidah Abdul-Hamid, Stephen Weng, Joe Kai, and Jo Leonardi-Bee. 2021. "Systematic Identification of Familial Hypercholesterolaemia in Primary Care—A Systematic Review" Journal of Personalized Medicine 11, no. 4: 302. https://doi.org/10.3390/jpm11040302