
Tumor Infiltrating Neutrophils Are Frequently Found in Adenocarcinomas of the Biliary Tract and Their Precursor Lesions with Possible Impact on Prognosis

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients and Tissues
2.1.1. Patients with Surgically Resected Sporadic Biliary Tract Cancer (spBTC Cohort)
2.1.2. Patients with Primary Sclerosing Cholangitis and BTC (PSC-BTC Cohort)
2.1.3. Patients with PSC Who Underwent Liver Transplantation (PSC-LTX Cohort)
2.2. Tissue Microarray Construction and Tumor-Infiltrating Neutrophil (TIN) Density Score Analysis in Sporadic BTC
2.3. Neutrophils Density Analysis in Biliary Intraepithelial Neoplasia (BilIN)
2.4. BTC and BilIN Classification
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Correlation of TIN Density with Clinicopathologic Parameters
3.3. Correlation of TIN Density with Outcome
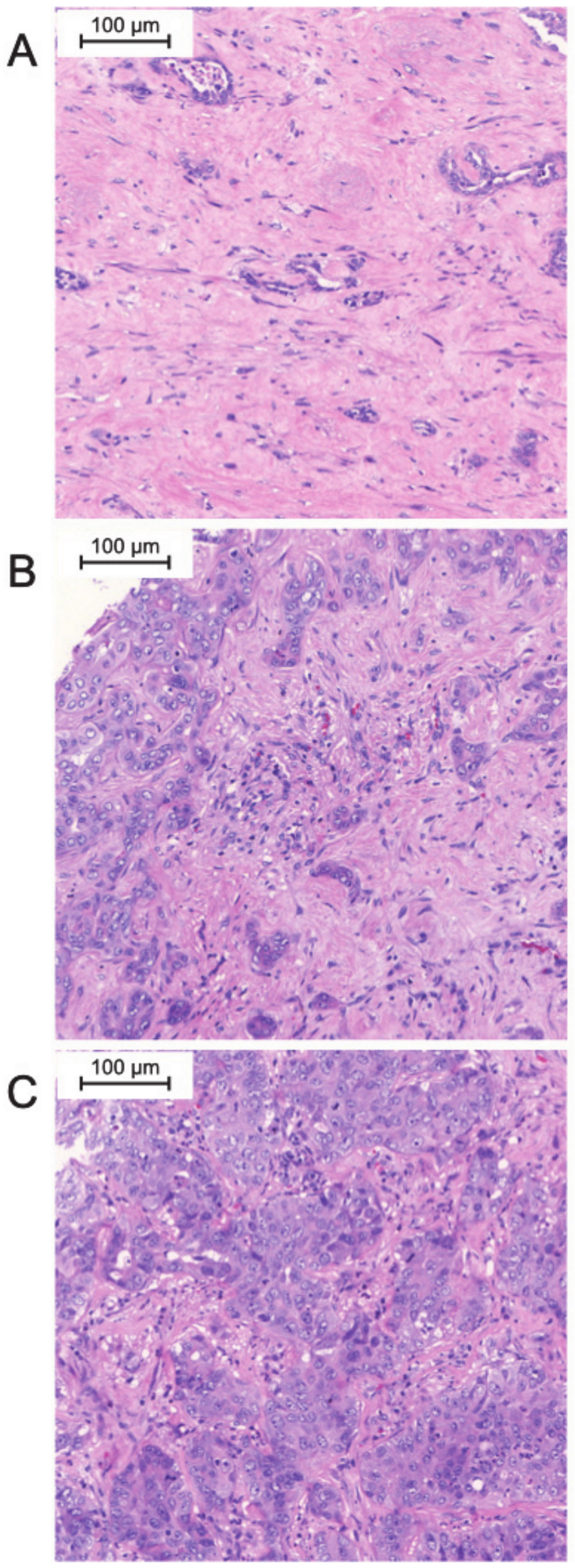
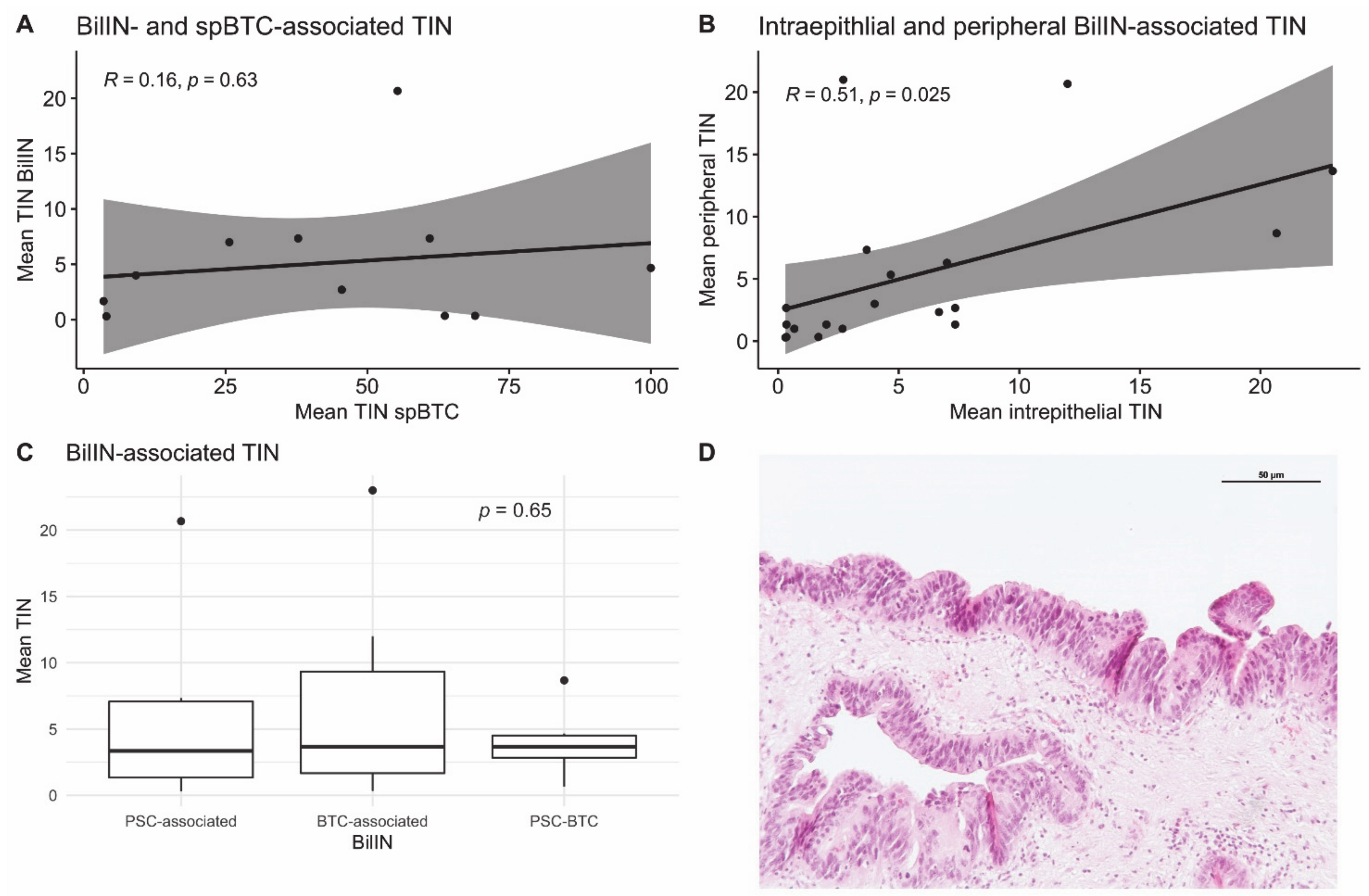
3.4. Neutrophil Infiltration in BTC-Associated BilIN
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C.; et al. The global burden of cancer 2013. JAMA Oncol. 2015, 1, 505. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Zhu, A.X.; Fuchs, C.S.; Brook, S.G.A. Forty-year trends in cholangiocarcinoma incidence in the U.S.: Intrahepatic disease on the rise. Oncologist 2016, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D. ESMO guidelines committee biliary cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, v28–v37. [Google Scholar] [CrossRef]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [Green Version]
- Endo, I.; Gonen, M.; Yopp, A.C.; Dalal, K.M.; Zhou, Q.; Klimstra, D.; D’Angelica, M.; DeMatteo, R.P.; Fong, Y.; Schwartz, L.; et al. Intrahepatic cholangiocarcinoma: Rising frequency, improved survival, and determinants of outcome after resection. Ann. Surg. 2008, 248, 84–96. [Google Scholar] [CrossRef]
- Boonstra, K.; Weersma, R.K.; van Erpecum, K.J.; Rauws, E.A.; Spanier, B.W.M.; Poen, A.C.; van Nieuwkerk, K.M.; Drenth, J.P.; Witteman, B.J.; Tuynman, H.A.; et al. Population-based epidemiology, malignancy risk, and outcome of primary sclerosing cholangitis. Hepatology 2013, 58, 2045–2055. [Google Scholar] [CrossRef]
- Hasita, H.; Komohara, Y.; Okabe, H.; Masuda, T.; Ohnishi, K.; Lei, X.F.; Beppu, T.; Baba, H.; Takeya, M. Significance of alternatively activated macrophages in patients with intrahepatic cholangiocarcinoma. Cancer Sci. 2010, 101, 1913–1919. [Google Scholar] [CrossRef]
- Cadamuro, M.; Morton, S.D.; Strazzabosco, M.; Fabris, L. Unveiling the role of tumor reactive stroma in cholangiocarcinoma: An opportunity for new therapeutic strategies. Transl. Gastrointest. Cancer 2013, 2, 130–144. [Google Scholar] [CrossRef]
- McNamara, M.G.; Templeton, A.J.; Maganti, M.; Walter, T.; Horgan, A.M.; McKeever, L.; Min, T.; Amir, E.; Knox, J.J. Neutrophil/lymphocyte ratio as a prognostic factor in biliary tract cancer. Eur. J. Cancer Oxf. Engl. 1990 2014, 50, 1581–1589. [Google Scholar] [CrossRef]
- Chen, Q.; Yang, L.-X.; Li, X.-D.; Yin, D.; Shi, S.-M.; Chen, E.-B.; Yu, L.; Zhou, Z.-J.; Zhou, S.-L.; Shi, Y.-H.; et al. The elevated preoperative neutrophil-to-lymphocyte ratio predicts poor prognosis in intrahepatic cholangiocarcinoma patients undergoing hepatectomy. Tumour Biol. J. Int. Soc. Oncodev. Biol. Med. 2015, 36, 5283–5289. [Google Scholar] [CrossRef]
- Zhang, Y.; Jiang, C.; Li, J.; Sun, J.; Qu, X. Prognostic significance of preoperative neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in patients with gallbladder carcinoma. Clin. Transl. Oncol. Off. Publ. Fed. Span. Oncol. Soc. Natl. Cancer Inst. Mex. 2015, 17, 810–818. [Google Scholar] [CrossRef]
- Lin, G.; Liu, Y.; Li, S.; Mao, Y.; Wang, J.; Shuang, Z.; Chen, J.; Li, S. Elevated neutrophil-to-lymphocyte ratio is an independent poor prognostic factor in patients with intrahepatic cholangiocarcinoma. Oncotarget 2016, 7, 50963–50971. [Google Scholar] [CrossRef] [Green Version]
- Yeh, Y.-C.; Lei, H.-J.; Chen, M.-H.; Ho, H.-L.; Chiu, L.-Y.; Li, C.-P.; Wang, Y.-C. C-Reactive Protein (CRP) is a promising diagnostic immunohistochemical marker for intrahepatic cholangiocarcinoma and is associated with better prognosis. Am. J. Surg. Pathol. 2017, 41, 1630–1641. [Google Scholar] [CrossRef]
- Rapoport, B.L.; Steel, H.C.; Theron, A.J.; Smit, T.; Anderson, R. Role of the neutrophil in the pathogenesis of advanced cancer and impaired responsiveness to therapy. Molecules 2020, 25, 1618. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Liu, H.; Shen, Z.; Lin, C.; Wang, X.; Qin, J.; Qin, X.; Xu, J.; Sun, Y. Tumor-infiltrating neutrophils is prognostic and predictive for postoperative adjuvant chemotherapy benefit in patients with gastric cancer. Ann. Surg. 2018, 267, 311–318. [Google Scholar] [CrossRef]
- Zeindler, J.; Angehrn, F.; Droeser, R.; Däster, S.; Piscuoglio, S.; Ng, C.K.Y.; Kilic, E.; Mechera, R.; Meili, S.; Isaak, A.; et al. Infiltration by myeloperoxidase-positive neutrophils is an independent prognostic factor in breast cancer. Breast Cancer Res. Treat. 2019, 177, 581–589. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2017; ISBN 978-1-119-26354-8. [Google Scholar]
- Zen, Y.; Adsay, N.V.; Bardadin, K.; Colombari, R.; Ferrell, L.; Haga, H.; Hong, S.-M.; Hytiroglou, P.; Klöppel, G.; Lauwers, G.Y.; et al. Biliary intraepithelial neoplasia: An international interobserver agreement study and proposal for diagnostic criteria. Mod. Pathol. 2007, 20, 701–709. [Google Scholar] [CrossRef]
- Basturk, O.; Aishima, S.; Esposito, I. Biliary intraepithelial neoplasia. In WHO Classification of Tumours: Digestive System Tumours; WHO Classification of Tumours Editorial Board, International Agency for Research on Cancer: Lyon, France, 2019; Volume 1, ISBN 978-92-832-4499-8. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2020. [Google Scholar]
- Kassambara, A.; Kosinski, M.; Biecek, P. Survminer: Drawing Survival Curves Using “Ggplot2”, 2020.
- Masucci, M.T.; Minopoli, M.; Carriero, M.V. Tumor associated neutrophils. Their role in tumorigenesis, metastasis, prognosis and therapy. Front. Oncol. 2019, 9, 1146. [Google Scholar] [CrossRef] [Green Version]
- Powell, D.R.; Huttenlocher, A. Neutrophils in the tumor microenvironment. Trends Immunol. 2016, 37, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Fridlender, Z.G.; Sun, J.; Kim, S.; Kapoor, V.; Cheng, G.; Ling, L.; Worthen, G.S.; Albelda, S.M. Polarization of tumor-associated neutrophil phenotype by TGF-β: “N1” versus “N2” TAN. Cancer Cell 2009, 16, 183–194. [Google Scholar] [CrossRef] [Green Version]
- Flavell, R.A.; Sanjabi, S.; Wrzesinski, S.H.; Licona-Limón, P. The polarization of immune cells in the tumour environment by TGFβ. Nat. Rev. Immunol. 2010, 10, 554–567. [Google Scholar] [CrossRef] [Green Version]
- Eruslanov, E.B.; Singhal, S.; Albelda, S.M. Mouse versus human neutrophils in cancer: A major knowledge gap. Trends Cancer 2017, 3, 149–160. [Google Scholar] [CrossRef] [Green Version]
- Roy, S.; Glaser, S.; Chakraborty, S. Inflammation and progression of cholangiocarcinoma: Role of angiogenic and lymphangiogenic mechanisms. Front. Med. 2019, 6, 293. [Google Scholar] [CrossRef] [Green Version]
- Schottenfeld, D.; Beebe-Dimmer, J. Chronic inflammation: A common and important factor in the pathogenesis of Neoplasia. CA Cancer J. Clin. 2006, 56, 69–83. [Google Scholar] [CrossRef]
- Posabella, A.; Köhn, P.; Lalos, A.; Wilhelm, A.; Mechera, R.; Soysal, S.; Muenst, S.; Güth, U.; Stadlmann, S.; Terracciano, L.; et al. High density of CD66B in primary high-grade ovarian cancer independently predicts response to chemotherapy. J. Cancer Res. Clin. Oncol. 2020, 146, 127–136. [Google Scholar] [CrossRef]
- Stenzel, P.J.; Schindeldecker, M.; Tagscherer, K.E.; Foersch, S.; Herpel, E.; Hohenfellner, M.; Hatiboglu, G.; Alt, J.; Thomas, C.; Haferkamp, A.; et al. Prognostic and predictive value of tumor-infiltrating leukocytes and of immune checkpoint molecules PD1 and PDL1 in clear cell renal cell carcinoma. Transl. Oncol. 2020, 13, 336–345. [Google Scholar] [CrossRef]
- Li, Y.-W.; Qiu, S.-J.; Fan, J.; Zhou, J.; Gao, Q.; Xiao, Y.-S.; Xu, Y.-F. Intratumoral neutrophils: A Poor prognostic factor for hepatocellular carcinoma following resection. J. Hepatol. 2011, 54, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Kuang, D.-M.; Zhao, Q.; Wu, Y.; Peng, C.; Wang, J.; Xu, Z.; Yin, X.-Y.; Zheng, L. Peritumoral neutrophils link inflammatory response to disease progression by fostering angiogenesis in hepatocellular carcinoma. J. Hepatol. 2011, 54, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.-L.; Dai, Z.; Zhou, Z.-J.; Wang, X.-Y.; Yang, G.-H.; Wang, Z.; Huang, X.-W.; Fan, J.; Zhou, J. Overexpression of CXCL5 mediates neutrophil infiltration and indicates poor prognosis for hepatocellular carcinoma. Hepatology 2012, 56, 2242–2254. [Google Scholar] [CrossRef] [PubMed]
- Ino, Y.; Yamazaki-Itoh, R.; Shimada, K.; Iwasaki, M.; Kosuge, T.; Kanai, Y.; Hiraoka, N. Immune cell infiltration as an indicator of the immune microenvironment of pancreatic cancer. Br. J. Cancer 2013, 108, 914–923. [Google Scholar] [CrossRef]
- Gu, F.-M.; Gao, Q.; Shi, G.-M.; Zhang, X.; Wang, J.; Jiang, J.-H.; Wang, X.-Y.; Shi, Y.-H.; Ding, Z.-B.; Fan, J.; et al. Intratumoral IL-17+ cells and neutrophils show strong prognostic significance in intrahepatic cholangiocarcinoma. Ann. Surg. Oncol. 2012, 19, 2506–2514. [Google Scholar] [CrossRef]
- Mao, Z.-Y.; Zhu, G.-Q.; Xiong, M.; Ren, L.; Bai, L. Prognostic value of neutrophil distribution in cholangiocarcinoma. World J. Gastroenterol. 2015, 21, 4961–4968. [Google Scholar] [CrossRef]
- Eruslanov, E.B.; Bhojnagarwala, P.S.; Quatromoni, J.G.; Stephen, T.L.; Ranganathan, A.; Deshpande, C.; Akimova, T.; Vachani, A.; Litzky, L.; Hancock, W.W.; et al. Tumor-associated neutrophils stimulate t cell responses in early-stage human lung cancer. J. Clin. Invest. 2014, 124, 5466–5480. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Wu, D.; Ni, C.; Ye, J.; Chen, W.; Hu, G.; Wang, Z.; Wang, C.; Zhang, Z.; Xia, W.; et al. ΓδT17 cells promote the accumulation and expansion of myeloid-derived suppressor cells in human colorectal cancer. Immunity 2014, 40, 785–800. [Google Scholar] [CrossRef] [Green Version]
- Singhal, S.; Bhojnagarwala, P.S.; O’Brien, S.; Moon, E.K.; Garfall, A.L.; Rao, A.S.; Quatromoni, J.G.; Stephen, T.L.; Litzky, L.; Deshpande, C.; et al. Origin and role of a subset of tumor-associated neutrophils with antigen-presenting cell features in early-stage human lung cancer. Cancer Cell 2016, 30, 120–135. [Google Scholar] [CrossRef] [Green Version]
- Ercolani, G.; Dazzi, A.; Giovinazzo, F.; Ruzzenente, A.; Bassi, C.; Guglielmi, A.; Scarpa, A.; D’Errico, A.; Pinna, A.D. Intrahepatic, peri-hilar and distal cholangiocarcinoma: Three different locations of the same tumor or three different tumors? Eur. J. Surg. Oncol. 2015, 41, 1162–1169. [Google Scholar] [CrossRef]
- Cardinale, V.; Renzi, A.; Carpino, G.; Torrice, A.; Bragazzi, M.C.; Giuliante, F.; DeRose, A.M.; Fraveto, A.; Onori, P.; Napoletano, C.; et al. Tumorigenesis and neoplastic progression profiles of cancer stem cell subpopulations in cholangiocarcinomas. Am. J. Pathol. 2015, 185. [Google Scholar] [CrossRef]
- Mayr, C.; Ocker, M.; Ritter, M.; Pichler, M.; Neureiter, D.; Kiesslich, T. Biliary tract cancer stem cells-Translational options and challenges. World J. Gastroenterol. 2017, 23, 2470–2482. [Google Scholar] [CrossRef]
- Andersen, J.B.; Spee, B.; Blechacz, B.R.; Avital, I.; Komuta, M.; Barbour, A.; Conner, E.A.; Gillen, M.C.; Roskams, T.; Roberts, L.R.; et al. Genomic and Genetic characterization of cholangiocarcinoma identifies therapeutic targets for tyrosine kinase inhibitors. Gastroenterology 2012, 142, 1021–1031.e15. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| TIN Density | ||||||
|---|---|---|---|---|---|---|
| All Patients N= 53 | Low N= 31 | Intermediate N= 12 | High N= 8 | |||
| n, mean, median (%, SD, or IQR) | n, mean, median (%, SD, or IQR) | n, mean, median (%, SD, or IQR) | n, mean, median (%, SD, or IQR) | p | ||
| Sex | W M | 29 (54.7) 24 (45.3) | 18 (58.1) 13 (41.9) | 5 (41.7) 7 (58.3) | 4 (50.0) 4 (50.0) | 0.624 |
| Age | ≤67 >67 | 28 (52.8) 25 (47.2) | 16 (51.6) 15 (48.4) | 7 (58.3) 5 (41.7) | 4 (50.0) 4 (50.0) | 0.925 |
| CA19-9 | 53.6 (26.9–359.0) | 53.6 (28.3–160.4) | 61.8 (20.3–360.4) | 36.4 (29.7–1164.6) | 0.325 | |
| CEA | 2.2 (1.2–3.0) | 2.4 (1.4–3.3) | 2.2 (1.1–4.6) | 1.2 (0.9–1.3) | 0.080 | |
| CRP | 17.2 (7.2–59.5) | 24.7 (9.50–75.50) | 11.0 (4.9–31.2) | 19.4 (6.2–26.7) | 0.396 | |
| Localization | IHC PHC DC GBC | 19 (35.8) 13 (24.5) 14 (26.4) 7 (13.2) | 10 (32.3) 6 (19.4) 8 (25.8) 7 (22.6) | 5 (41.7) 2 (16.7) 5 (41.7) 0 (0.0) | 4 (50.0) 3 (37.5) 1 (12.5) 0 (0.0) | 0.312 |
| T | T1 T2 T3 T4 | 15 (28.3) 19 (35.8) 19 (35.8) 0 (0) | 6 (19.4) 8 (25.8) 17 (54.8) 0 (0.0) | 4 (33.3) 6 (50.0) 2 (16.7) 0 (0.0) | 4 (50.0) 4 (50.0) 0 (0.0) 0 (0.0) | 0.012 |
| N | N0 N1 | 23 (43.4) 30 (56.6) | 9 (29.3) 22 (71.0) | 9 (75.0) 3 (25.0) | 4 (50) 4 (50) | 0.025 |
| M | M0 M1 | 49 (92.5) 4 (7.5) | 27 (87.1) 4 (12.9) | 12 (100.0) 0 (0.0) | 8 (100.0) 0 (0.0) | 0.462 |
| L | L0 L1 | 39 (73.6) 14 (26.4) | 22 (71.0) 9 (29.0) | 9 (75.0) 3 (25.0) | 7 (87.5) 1 (12.5) | 0.743 |
| V | V0 V1 | 44 (83.0) 9 (17.0) | 24 (77.4) 7 (22.6) | 11 (91.7) 1 (8.3) | 7 (87.5) 1 (12.5) | 0.671 |
| Pn | Pn0 Pn1 | 24 (45.3) 29 (54.7) | 13 (41.9) 18 (58.9) | 6 (50.0) 6 (50.0) | 3 (37.5) 5 (62.5) | 0.851 |
| G | G1 G2 G3 | 3 (5.7) 31 (58.5) 19 (35.8) | 2 (6.5) 18 (58.1) 11 (35.5) | 1 (8.3) 8 (66.7) 3 (25.0) | 0 (0.0) 3 (37.5) 5 (62.5) | 0.517 |
| R | R0 R+ | 42 (79.2) 11 (20.8) | 25 (80.6) 6 (19.4) | 11 (91.7) 1 (8.3) | 5 (62.5) 3 (37.5) | 0.285 |
| Stage | Stage I Stage II Stage III Stage IV | 9 (17.0) 19 (35.8) 20 (37.7) 5 (9.4) | 1 (3.2) 12 (38.7) 14 (45.2) 4 (12.9) | 4 (33.3) 6 (50.0) 1 (8.3) 1 (8.3) | 3 (37.5) 1 (12.5) 4 (50.0) 0 (0.0) | 0.010 |
| Postoperative Complications | Yes No | 28 (52.8) 25 (47.2) | 16 (51.6) 15 (48.4) | 6 (50.0) 6 (50.0) | 5 (62.5) 3 (37.5) | 0.837 |
| Chemotherapy | Yes No | 33 (62.3) 20 (37.7) | 22 (71.0) 9 (29.0) | 6 (50.0) 6 (50.0) | 4 (50.0) 4 (50.0) | 0.356 |
| Endpoint | Subgroup | HR | CI 95% | p |
|---|---|---|---|---|
| Age > 67 vs. ≤67 | 1.17 | 0.55–2.47 | 0.678 | |
| Female vs. Male | 1.02 | 0.48–2.14 | 0.963 | |
| CEA high vs. low | 1.75 | 0.73–4.20 | 0.207 | |
| CA19.9 high vs. low | 1.78 | 0.82–3.84 | 0.145 | |
| TIN intermediate vs. high | 10.10 | 1.22–83.50 | 0.032 | |
| TIN low vs. high | 7.66 | 1.02–57.53 | 0.048 | |
| Complications Yes vs. No | 1.30 | 0.61–2.78 | 0.498 | |
| G2 vs. G1 | 1.63 | 0.22–12.34 | 0.636 | |
| G3 vs. G1 | 1.72 | 0.22–13.66 | 0.607 | |
| T2 vs. T1 | 0.83 | 0.31–2.23 | 0.706 | |
| T3 vs. T1 | 1.26 | 0.51–3.11 | 0.612 | |
| N1 vs. N0 | 1.69 | 0.79–3.62 | 0.179 | |
| M1 vs. M0 | 1.07 | 0.25–4.53 | 0.927 | |
| Stage 2 vs. Stage 1 | 3.23 | 0.71–14.66 | 0.128 | |
| Stage 3 vs. Stage 1 | 4.48 | 1.01–19.92 | 0.049 | |
| Stage4 vs. Stage 1 | 3.15 | 0.44–22.51 | 0.254 | |
| R1 vs. R0 | 1.30 | 0.52–3.25 | 0.579 | |
| V1 vs. V0 | 1.74 | 0.70–4.34 | 0.234 | |
| L1 vs. L0 | 0.82 | 0.33–2.05 | 0.676 | |
| Pn1 vs. Pn0 | 1.39 | 0.65–2.95 | 0.394 | |
| Chemotherapy Yes vs. No | 0.62 | 0.29–1.31 | 0.208 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Branchi, V.; Jürgensen, B.; Esser, L.; Gonzalez-Carmona, M.; Weismüller, T.J.; Strassburg, C.P.; Henn, J.; Semaan, A.; Lingohr, P.; Manekeller, S.; et al. Tumor Infiltrating Neutrophils Are Frequently Found in Adenocarcinomas of the Biliary Tract and Their Precursor Lesions with Possible Impact on Prognosis. J. Pers. Med. 2021, 11, 233. https://doi.org/10.3390/jpm11030233
Branchi V, Jürgensen B, Esser L, Gonzalez-Carmona M, Weismüller TJ, Strassburg CP, Henn J, Semaan A, Lingohr P, Manekeller S, et al. Tumor Infiltrating Neutrophils Are Frequently Found in Adenocarcinomas of the Biliary Tract and Their Precursor Lesions with Possible Impact on Prognosis. Journal of Personalized Medicine. 2021; 11(3):233. https://doi.org/10.3390/jpm11030233
Chicago/Turabian StyleBranchi, Vittorio, Benedict Jürgensen, Laura Esser, Maria Gonzalez-Carmona, Tobias J. Weismüller, Christian P. Strassburg, Jonas Henn, Alexander Semaan, Philipp Lingohr, Steffen Manekeller, and et al. 2021. "Tumor Infiltrating Neutrophils Are Frequently Found in Adenocarcinomas of the Biliary Tract and Their Precursor Lesions with Possible Impact on Prognosis" Journal of Personalized Medicine 11, no. 3: 233. https://doi.org/10.3390/jpm11030233