Differences and Similarities in Neuropathy in Type 1 and 2 Diabetes: A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
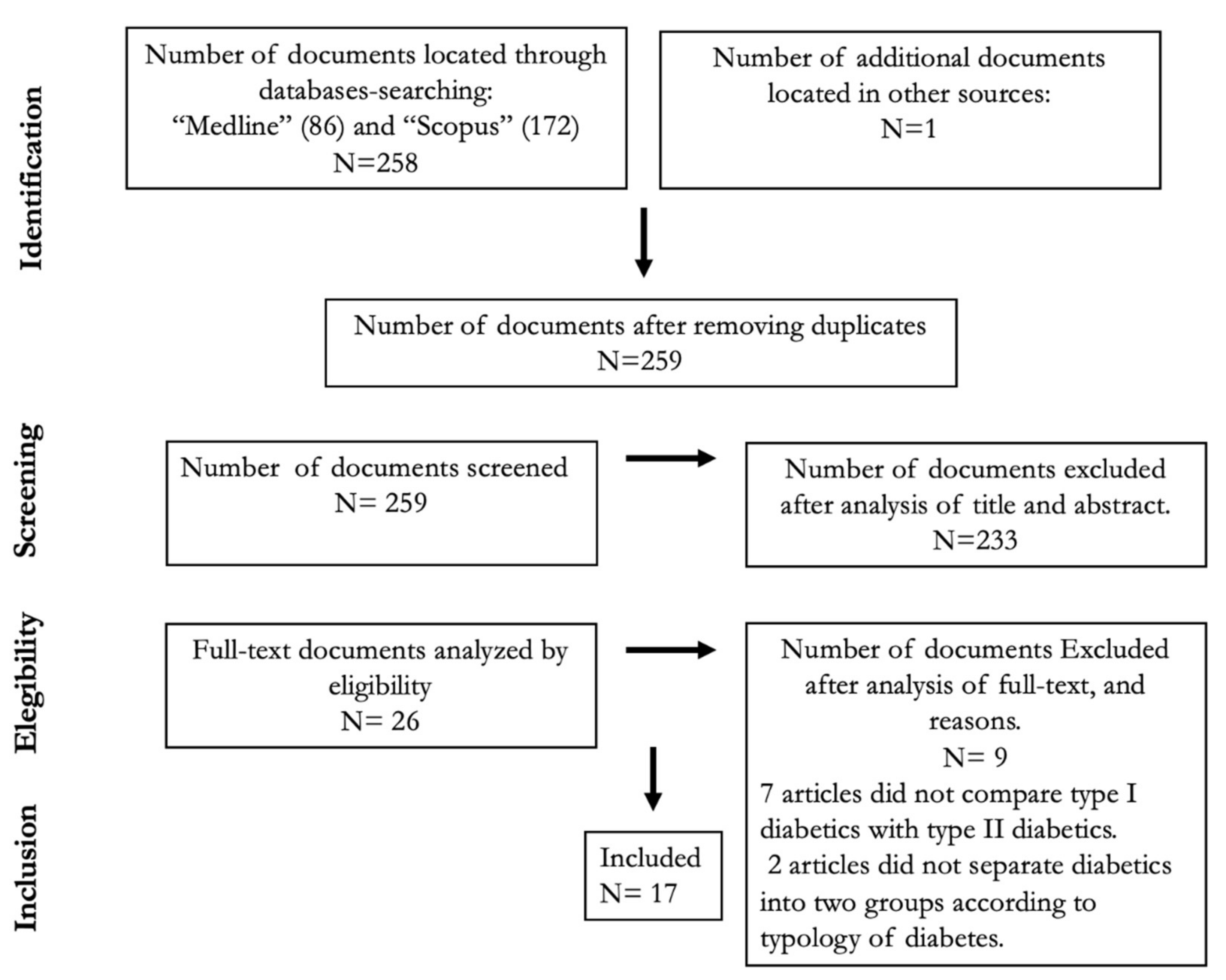
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Analysis
3. Results
3.1. Sensory Neuropathy
3.2. Motor Neuropathy
3.3. Autonomic Neuropathy
3.4. Differences in Molecular Markers Associated with Neuropathy in Type 1 and 2 Diabetes
3.5. Effect of Age and Sex on Neuropathy in Type 1 and 2 Diabetes Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Norris, J.M.; Johnson, R.K.; Stene, L.C. Type 1 diabetes—Early life origins and changing epidemiology. Lancet Diabetes Endocrinol. 2020, 8, 226–238. [Google Scholar] [CrossRef]
- Grulich-Henn, J.; Klose, D. Understanding childhood diabetes mellitus: New pathophysiological aspects. J. Inherit. Metab. Dis. 2018, 41, 19–27. [Google Scholar] [CrossRef]
- Peixoto-Barbosa, R.; Reis, A.F.; Giuffrida, F.M.A. Update on clinical screening of maturity-onset diabetes of the young (MODY). Diabetol. Metab. Syndr. 2020, 12, 1–14. [Google Scholar] [CrossRef]
- Zaccardi, F.; Webb, D.R.; Yates, T.; Davies, M.J. Pathophysiology of type 1 and type 2 diabetes mellitus: A 90-year perspective. Postgrad. Med. J. 2015, 92, 63–69. [Google Scholar] [CrossRef]
- Xia, Y.; Xie, Z.; Huang, G.; Zhou, Z. Incidence and trend of type 1 diabetes and the underlying environmental determinants. Diabetes/Metabolism Res. Rev. 2019, 35, e3075. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes–Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gherman, D.; Dumitrescu, C.I.; Ciocan, A.; Melincovici, C.S. Histopathological changes in major amputations due to diabetic foot—A review. Romanian J. Morphol. Embryol. = Rev. Roum. de Morphol. et Embryol. 2018, 59, 699–702. [Google Scholar]
- Rorive, M.; Scheen, A.J. [News in the management of diabetic foot]. J. News Manag. Diabetic Foot. Rev. Med. Suisse 2019, 15, 1448–1452. [Google Scholar]
- Tesfaye, S.; Selvarajah, D. Advances in the epidemiology, pathogenesis and management of diabetic peripheral neuropathy. Diabetes/Metabolism Res. Rev. 2012, 28, 8–14. [Google Scholar] [CrossRef]
- Azmi, S.; Petropoulos, I.N.; Ferdousi, M.; Ponirakis, G.; Alam, U.; Malik, R.A. An update on the diagnosis and treatment of diabetic somatic and autonomic neuropathy. F1000Research 2019, 8, 186. [Google Scholar] [CrossRef] [Green Version]
- Hicks, C.W.; Selvin, E. Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr. Diabetes Rep. 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Martin, C.L.; Albers, J.W.; Pop-Busui, R.; for the DCCT/EDIC Research Group. Neuropathy and Related Findings in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study. Diabetes Care 2014, 37, 31–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iqbal, Z.; Azmi, S.; Yadav, R.; Ferdousi, M.; Kumar, M.; Cuthbertson, D.J.; Lim, J.; Malik, R.A.; Alam, U. Diabetic Peripheral Neuropathy: Epidemiology, Diagnosis, and Pharmacotherapy. Clin. Ther. 2018, 40, 828–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urrútia, G.; Bonfill, X. Declaración PRISMA: Una propuesta para mejorar la publicación de revisiones sistemáticas y metaanálisis. Medicina Clínica 2010, 135, 507–511. [Google Scholar] [CrossRef]
- Balducci, S.; Sacchetti, M.; Orlando, G.; Salvi, L.; Pugliese, L.; Salerno, G.; D’Errico, V.; Iacobini, C.; Conti, F.; Zanuso, S.; et al. Correlates of muscle strength in diabetes. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 18–26. [Google Scholar] [CrossRef]
- Moghtaderi, A.; Bakhshipour, A.; Rashidi, H. Validation of Michigan neuropathy screening instrument for diabetic peripheral neuropathy. Clin. Neurol. Neurosurg. 2006, 108, 477–481. [Google Scholar] [CrossRef]
- Meyer, M.; Rose, C.; Hülsmann, J.-O.; Schatz, H.; Pfohl, M. Impaired 0.1-Hz vasomotion assessed by laser Doppler anemometry as an early index of peripheral sympathetic neuropathy in diabetes. Microvasc. Res. 2003, 65, 88–95. [Google Scholar] [CrossRef]
- Lautenbacher, S. PATH Tester MPI 100 - Pain and Thermal Sensitivity Tester; Gerät Zur Bestimmung Der Temperatur- Und Schmerzempfindlichkeit; Phywe Systeme GmbH: Göttingen, Germany, 1988; Available online: https://fis.uni-bamberg.de/handle/uniba/38723 (accessed on 18 March 2021).
- Aulich, J.; Cho, Y.H.; Januszewski, A.S.; Craig, M.E.; Selvadurai, H.; Wiegand, S.; Jenkins, A.J.; Donaghue, K.C. Associations between circulating inflammatory markers, diabetes type and complications in youth. Pediatr. Diabetes 2019, 20, 1118–1127. [Google Scholar] [CrossRef]
- NeuroSensory Analyzer TSA-II. Available online: http://www.intelimed.com.mx/tsaii.html (accessed on 18 March 2021).
- Schamarek, I.; Herder, C.; Nowotny, B.; Carstensen-Kirberg, M.; Strassburger, K.; Nowotny, P.; Strom, A.; Püttgen, S.; Müssig, K.; Szendroedi, J.; et al. Adiponectin, markers of subclinical inflammation and nerve conduction in individuals with recently diagnosed type 1 and type 2 diabetes. Eur. J. Endocrinol. 2016, 174, 433–443. [Google Scholar] [CrossRef] [Green Version]
- Chawla, A.; Bhasin, G.; Chawla, R. Validation Of Neuropathy Symptoms Score (NSS) And Neuropathy Disability Score (NDS) In The Clinical Diagnosis Of Peripheral Neuropathy In Middle Aged People With Diabetes. Internet J. Fam. Pract. 2013, 12, 1–5. [Google Scholar]
- Nybo, M.; Poulsen, M.K.; Grauslund, J.; Henriksen, J.E.; Rasmussen, L.M. Plasma osteoprotegerin concentrations in peripheral sensory neuropathy in Type 1 and Type 2 diabetic patients. Diabet. Med. 2010, 27, 289–294. [Google Scholar] [CrossRef]
- Arnold, R.; Kwai, N.; Lin, C.S.-Y.; Poynten, A.M.; Kiernan, M.C.; Krishnan, A.V. Axonal dysfunction prior to neuropathy onset in type 1 diabetes. Diabetes/Metabolism Res. Rev. 2013, 29, 53–59. [Google Scholar] [CrossRef]
- Cornblath, D.R.; Chaudhry, V.; Carter, K.; Lee, D.; Seysedadr, M.; Miernicki, M.; Joh, T. Total neuropathy score: Validation and reliability study. Neurol. 1999, 53, 1660. [Google Scholar] [CrossRef]
- Fedele, D.; Coscelli, C.; Santeusanio, F.; Bortolotti, A.; Chatenoud, L.; Colli, E.; Landoni, M.; Parazzini, F. Erectile dysfunction in diabetic subjects in Italy. Gruppo Italiano Studio Deficit Erettile nei Diabetici. Diabetes Care 1998, 21, 1973–1977. [Google Scholar] [CrossRef]
- Fedele, D.; Coscelli, C.; Cucinotta, D.; Forti, G.; Santeusanio, F.; Viaggi, S.; Fiori, G.; Velonà, T.; Lavezzari, M.; the Members of the Diade Study Group†. Incidence of Erectile Dysfunction in Italian Men with Diabetes. J. Urol. 2001, 166, 1368–1371. [Google Scholar] [CrossRef]
- Pan, Q.; Li, Q.; Deng, W.; Zhao, D.; Qi, L.; Huang, W.; Ma, L.; Li, H.; Li, Y.; Lyu, X.; et al. Prevalence and Diagnosis of Diabetic Cardiovascular Autonomic Neuropathy in Beijing, China: A Retrospective Multicenter Clinical Study. Front. Neurosci. 2019, 13, 1144. [Google Scholar] [CrossRef] [PubMed]
- Gulichsen, E.; Fleischer, J.; Ejskjaer, N.; Eldrup, E.; Tarnow, L. Screening for Diabetic Cardiac Autonomic Neuropathy Using a New Handheld Device. J. Diabetes Sci. Technol. 2012, 6, 965–972. [Google Scholar] [CrossRef] [Green Version]
- Medicus Engineering. Vagus. Available online: http://www.vagustm.com/ (accessed on 18 March 2021).
- Ayad, F.; Belhadj, M.; Pariès, J.; Attali, J.R.; Valensi, P. Association between cardiac autonomic neuropathy and hypertension and its potential influence on diabetic complications. Diabet. Med. 2010, 27, 804–811. [Google Scholar] [CrossRef]
- Pappachan, J.M.; Sebastian, J.; Bino, B.C.; Jayaprakash, K.; Vijayakumar, K.; Sujathan, P.; A Adinegara, L. Cardiac autonomic neuropathy in diabetes mellitus: Prevalence, risk factors and utility of corrected QT interval in the ECG for its diagnosis. Postgrad. Med J. 2008, 84, 205–210. [Google Scholar] [CrossRef]
- Koçkar, M.C.; Kayahan, I.K.; Bavbek, N. Diabetic gastroparesis in association with autonomic neuropathy and microvasculopathy. Acta Med. Okayama 2002, 56, 237–243. [Google Scholar]
- Palasciano, G.; Portincasa, P.; Belfiore, A.; Baldassarre, G.; Cignarelli, M.; Paternostro, A.; Albano, O.; Giorgino, R. Gallbladder volume and emptying in diabetics: The role of neuropathy and obesity. J. Intern. Med. 1992, 231, 123–127. [Google Scholar] [CrossRef]
- Kramer, C.; Leitão, C.; Azevedo, M.; Valiatti, F.; Rodrigues, T.; Canani, L.; Gross, J. Diabetic retinopathy is associated with early autonomic dysfunction assessed by exercise-related heart rate changes. Braz. J. Med Biol. Res. 2008, 41, 1110–1115. [Google Scholar] [CrossRef] [Green Version]
- Duque, M.; Díaz, J.C.; Molina, D.I.; Gómez, E.; Márquez, G.; López, P.; Melgarejo, E.; Duque, L. Diabetic Autonomic Cardiovascular Neuropathy. Rev. Colomb. Cardiol. 2013, 20, 80–87. [Google Scholar]
- Cygankiewicz, I.; Zareba, W. Heart Rate Variability, 1st ed.; Buijs, R.M., Swaab, D.F., Eds.; Elsevier: Amsterdam, The Netherlands, 2013; Volume 117. [Google Scholar]
- Fidanci, M.K.; Gulgun, M.; Genc, A. Analysis of heart rate variability seems to be one step ahead of cardiac reflex tests for investigating cardiovascular autonomic neuropathy. Anatol. J. Cardiol. 2015, 15, 849–850. [Google Scholar] [CrossRef]
- Valensi, P.; Pariès, J.; Attali, J.R.; Cathelineau, G.; Fossati, P.; Verier-Mine, O.; Monnier, L.; Pouget, J.Y.; Vague, P.; Leutenegger, M.; et al. Cardiac Autonomic Neuropathy in Diabetic Patients: Influence of Diabetes Duration, Obesity, and Microangiopathic Complications - The French Multicenter Study. Metabolism 2003, 52, 815–820. [Google Scholar] [CrossRef]
- Fisher, V.L.; A Tahrani, A. Cardiac autonomic neuropathy in patients with diabetes mellitus: Current perspectives. Diabetes Metab. Syndr. Obesity: Targets Ther. 2017, 10, 419–434. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, D. Diabetic cardiovascular autonomic neuropathy: Prognosis, diagnosis and treatment. Diabetes/Metab. Rev. 1994, 10, 339–383. [Google Scholar] [CrossRef] [PubMed]
- Paneerselvam, D.; Saravanan, P.; Malini, P.; Vasuki, R. Prevalence of cardiac autonomic neuropathy in type 2 diabetes mellitus and its correlation with other microvascular complications in South Indian population. Int. J. Adv. Med. 2019, 6, 611. [Google Scholar] [CrossRef]
- Calogero, A.E.; Burgio, G.; Condorelli, R.A.; Cannarella, R.; La Vignera, S. Epidemiology and risk factors of lower urinary tract symptoms/benign prostatic hyperplasia and erectile dysfunction. Aging Male 2019, 22, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Pozzo, M.J.; Mociulsky, J.; Martinez, E.T.; Senatore, G.; Farias, J.M.; Sapetti, A.; Sanzana, M.G.; Gonzalez, P.; Cafferata, A.; Peloche, A.; et al. Diabetes and Quality of Life. Am. J. Ther. 2016, 23, e159–e171. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, D.K.; Campbell, I.W.; Wu, F.C.; Prescott, R.J.; Clarke, B.F. The prevalence of diabetic impotence. Diabetology 1980, 18, 279–283. [Google Scholar] [CrossRef]
- Azmi, S.; Ferdousi, M.; Alam, U.; Petropoulos, I.N.; Ponirakis, G.; Marshall, A.; Asghar, O.; Fadavi, H.; Jones, W.; Tavakoli, M.; et al. Small-fibre neuropathy in men with type 1 diabetes and erectile dysfunction: A cross-sectional study. Diabetology 2017, 60, 1094–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furukawa, S.; Sakai, T.; Niiya, T.; Miyaoka, H.; Miyake, T.; Yamamoto, S.; Maruyama, K.; Ueda, T.; Senba, H.; Todo, Y.; et al. Diabetic peripheral neuropathy and prevalence of erectile dysfunction in Japanese patients aged <65 years with type 2 diabetes mellitus: The Dogo Study. Int. J. Impot. Res. 2017, 29, 30–34. [Google Scholar]
- Kumar, M.; Chapman, A.; Javed, S.; Alam, U.; A Malik, R.; Azmi, S. The Investigation and Treatment of Diabetic Gastroparesis. Clin. Ther. 2018, 40, 850–861. [Google Scholar] [CrossRef]
- Agarwal, A.K.; Miglani, S.; Singla, S.; Garg, U.; Dudeja, R.K.; Goel, A. Ultrasonographic evaluation of gallbladder volume in diabetics. J. Assoc. Physicians India 2004, 52, 962–965. [Google Scholar] [PubMed]
- Ferrer Cañabate, J.; Tovar, I.; Martínez, P. Osteoprotegerina y Sistema RANKL/RANK: El Futuro Del Metabolismo Óseo? An. Med. Interna 2002, 19, 385–388. [Google Scholar] [CrossRef] [Green Version]
- Miyashita, T.; Kawakami, A.; Nakashima, T.; Yamasaki, S.; Tamai, M.; Tanaka, F.; Kamachi, M.; Ida, H.; Migita, K.; Origuchi, T.; et al. Osteoprotegerin (OPG) acts as an endogenous decoy receptor in tumour necrosis factor-related apoptosis-inducing ligand (TRAIL)-mediated apoptosis of fibroblast-like synovial cells. Clin. Exp. Immunol. 2004, 137, 430–436. [Google Scholar] [CrossRef]
- Boyce, B.F.; Xing, L. Biology of RANK, RANKL, and osteoprotegerin. Arthritis Res. 2007, 9, S1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeffcoate, W. Vascular calcification and osteolysis in diabetic neuropathy?is RANK-L the missing link? Diabetology 2004, 47, 1488–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palsson-McDermott, E.M.; O’Neill, L.A.J. Signal transduction by the lipopolysaccharide receptor, Toll-like receptor-4. Immunology 2004, 113, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Rudofsky, G.; Reismann, P.; Witte, S.; Humpert, P.M.; Isermann, B.; Chavakis, T.; Tafel, J.; Nosikov, V.V.; Hamann, A.; Nawroth, P.; et al. Asp299Gly and Thr399Ile genotypes of the TLR4 gene are associated with a reduced prevalence of diabetic neuropathy in patients with type 2 diabetes. Diabetes Care 2003, 27, 179–183. [Google Scholar] [CrossRef] [Green Version]
- Pickup, J.C.; Crook, M.A. Is Type II diabetes mellitus a disease of the innate immune system? Diabetol. 1998, 41, 1241–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peltier, A.; A Goutman, S.; Callaghan, B.C. Painful diabetic neuropathy. BMJ 2014, 348, g1799. [Google Scholar] [CrossRef] [Green Version]
- Sima, A.A.; Kamiya, H. Diabetic Neuropathy Differs in Type 1 and Type 2 Diabetes. Ann. N. Y. Acad. Sci. 2006, 1084, 235–249. [Google Scholar] [CrossRef] [PubMed]
- Sima, A.A.; Zhang, W. Mechanisms of diabetic neuropathy. Handb. Clin. Neurol. 2014, 126, 429–442. [Google Scholar] [CrossRef]
- Hyllienmark, L.; Jönsson, B.; Ekberg, K.; Lindström, P. Abnormal cold perception in the lower limbs: A sensitive indicator for detection of polyneuropathy in patients with type 1 diabetes mellitus. Diabetes Res. Clin. Pr. 2009, 85, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Rolim, L.C.; de Sá, J.R.; Chacra, A.R.; Dib, S.A. Clinical Heterogeneity and Coexistence of Diabetic Neuropathies: Difference and Similarities between Types 1 and 2 Diabetes Mellitus. Arq. Bras. Endocrinol. Metabol. 2009, 53, 818–824. [Google Scholar] [CrossRef] [Green Version]
- Partanen, J.; Niskanen, L.; Lehtinen, J.; Mervaala, E.; Siitonen, O.; Uusitupa, M. Natural History of Peripheral Neuropathy in Patients with Non-Insulin-Dependent Diabetes Mellitus. N. Engl. J. Med. 1995, 333, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Silverthorn, D.U.; Johnson, B.R.; Ober, W.C.; Garrison, C.W.; Silverthorn, A.C. Chapter 10: Sensitive Physiology. In Human Physiology An Integrated Approach Edition, 8th ed.; Silverthorn, D.U., Ed.; Pearson Education: New York, NY, USA; Editorial Médica Panamerciana: Mexico City, Mexico, 2019. [Google Scholar]
- Chekka, K.; Moore, J.D.; Benzon, H.T. Physical Examination of the Patient with Pain. In Essentials of Pain Medicine; Benzon, H.T., Raja, S.N., Liu, S.S., Fishman, S.M., Cohen, S.P., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2011; pp. 19–27. [Google Scholar]
- Hogan, Q.; McCollister, K.; Harmelink, M.; Kohl, L.; Collins, M. Evaluation of Neurologic Injury Following Regional Anesthesia. In Complications of Regional Anesthesia; J.B. Metzler: Wien, Austria, 2017; pp. 113–137. [Google Scholar]
- Hebl, J.R. Peripheral Nerve Injury. In Complications in Regional Anesthesia and Pain Medicine; M. Neal, J., P. Rathmell, J., Eds.; Saunders: Philadelphia, PA, USA, 2007; pp. 125–140. [Google Scholar]
- Bajwa, H.; Al Khalili, Y. Physiology, Vibratory Sense; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Andersen, H.; Nielsen, S.; Mogensen, C.E.; Jakobsen, J. Muscle Strength in Type 2 Diabetes. Diabetes 2004, 53, 1543–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, H.; Poulsen, P.L.; Mogensen, C.E.; Jakobsen, J. Patients in Relation to Diabetic Complications. Diabetes 1996, 45, 440–445. [Google Scholar] [CrossRef]
- Andreassen, C.S.; Jakobsen, J.; Ringgaard, S.; Ejskjaer, N.; Andersen, H. Accelerated atrophy of lower leg and foot muscles—A follow-up study of long-term diabetic polyneuropathy using magnetic resonance imaging (MRI). Diabetology 2009, 52, 1182–1191. [Google Scholar] [CrossRef]
- Harati, Y. Frequently Asked Questions About Diabetic Peripheral Neuropathies. Neurol. Clin. 1992, 10, 783–807. [Google Scholar] [CrossRef]
- Cameron, N.E.; Cotter, M.A. The relationship of vascular changes to metabolic factors in diabetes mellitus and their role in the development of peripheral nerve complications. Diabetes/Metab. Rev. 1994, 10, 189–224. [Google Scholar] [CrossRef] [PubMed]
- Scarpini, E.; Bianchi, R.; Moggio, M.; Sciacco, M.; Fiori, M.G.; Scarlato, G. Decrease of nerve Na+,K+-ATPase activity in the pathogenesis of human diabetic neuropathy. J. Neurol. Sci. 1993, 120, 159–167. [Google Scholar] [CrossRef]
- Agashe, S.; Petak, S. Cardiac Autonomic Neuropathy in Diabetes Mellitus. Methodist DeBakey Cardiovasc. J. 2019, 14, 251–256. [Google Scholar] [CrossRef]
- Vinik, A.I.; Ziegler, D. Diabetic Cardiovascular Autonomic Neuropathy. Circulation 2007, 115, 387–397. [Google Scholar] [CrossRef]
- Pourmoghaddas, A.; Hekmatnia, A. The relationship between QTc interval and cardiac autonomic neuropathy in diabetes mellitus. Mol. Cell. Biochem. 2003, 249, 125–128. [Google Scholar] [CrossRef]
- Traon, A.P.-L.; Fontaine, S.; Tap, G.; Guidolin, B.; Senard, J.-M.; Hanaire, H. Cardiovascular autonomic neuropathy and other complications in type 1 diabetes. Clin. Auton. Res. 2010, 20, 153–160. [Google Scholar] [CrossRef]
- Mehta, S.; Mathur, D.; Chaturvedi, M.; Verma, K. Incidence of cardiac autonomic neuropathy and its correlation with retinopathy, micro-albuminuria and glycated haemoglobin in non-insulin dependent diabetes mellitus. J. Indian Med Assoc. 2002, 100, 141–143. [Google Scholar]
- Perin, P.C.; Maule, S.; Quadri, R. SYMPATHETIC NERVOUS SYSTEM, DIABETES, AND HYPERTENSION. Clin. Exp. Hypertens. 2001, 23, 45–55. [Google Scholar] [CrossRef]
- Istenes, I.; Keresztes, K.; Hermányi, Z.; Putz, Z.; Vargha, P.; Gandhi, R.; Tesfaye, S.; Kempler, P. Relationship between Autonomic Neuropathy and Hypertension-Are We Underestimating the Problem? Medicine 2008, 25, 863–866. [Google Scholar]
- Straub, R.H.; Thum, M.; Hollerbach, C.; Palitzsch, K.-D.; Schölmerich, J. Impact of Obesity on Neuropathic Late Complications in NIDDM. Diabetes Care 1994, 17, 1290–1294. [Google Scholar] [CrossRef] [PubMed]
- Vinik, A.I.; Casellini, C.; Parson, H.K.; Colberg, S.R.; Nevoret, M.-L. Cardiac Autonomic Neuropathy in Diabetes: A Predictor of Cardiometabolic Events. Front. Neurosci. 2018, 12, 591. [Google Scholar] [CrossRef]
- Williams, S.M.; Eleftheriadou, A.; Alam, U.; Cuthbertson, D.J.; Wilding, J.P.H. Cardiac Autonomic Neuropathy in Obesity, the Metabolic Syndrome and Prediabetes: A Narrative Review. Diabetes Ther. 2019, 10, 1995–2021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doulgerakis, D.; Moyssakis, I.; Kapelios, C.J.; Eleftheriadou, I.; Chorepsima, S.; Michail, S.; Tentolouris, N. Cardiac Autonomic Neuropathy Predicts All-Cause and Cardiovascular Mortality in Patients With End-Stage Renal Failure: A 5-Year Prospective Study. Kidney Int. Rep. 2017, 2, 686–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moţăţăianu, A.; Maier, S.; Bajko, Z.; Voidazan, S.; Bălaşa, R.; Stoian, A. Cardiac autonomic neuropathy in type 1 and type 2 diabetes patients. BMC Neurol. 2018, 18, 1–9. [Google Scholar] [CrossRef]
- Spallone, V. Update on the Impact, Diagnosis and Management of Cardiovascular Autonomic Neuropathy in Diabetes: What Is Defined, What Is New, and What Is Unmet. Diabetes Metab. J. 2019, 43, 3–30. [Google Scholar] [CrossRef]
- Phe, V.; Rouprêt, M. Erectile dysfunction and diabetes: A review of the current evidence-based medicine and a synthesis of the main available therapies. Diabetes Metab. 2012, 38, 1–13. [Google Scholar] [CrossRef]
- Chu, N.V.; Edelman, S.V. Erectile Dysfunction and Diabetes. Curr. Diab. Rep. 2002, 2, 60–66. [Google Scholar] [CrossRef]
- Chitaley, K.; Kupelian, V.; Subak, L.; Wessells, H. Diabetes, Obesity and Erectile Dysfunction: Field Overview and Research Priorities. J. Urol. 2009, 182, S45–S50. [Google Scholar] [CrossRef] [Green Version]
- Varkonyi, T.T.; Kempler, P. Sexual dysfunction in diabetes. Neurocutaneous Syndromes 2014, 126, 223–232. [Google Scholar] [CrossRef]
- Guarino, D.; Nannipieri, M.; Iervasi, G.; Taddei, S.; Bruno, R.M. The Role of the Autonomic Nervous System in the Pathophysiology of Obesity. Front. Physiol. 2017, 8, 665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fidan-Yaylali, G.; Yaylali, Y.T.; Erdogan, Ç.; Can, B.; Senol, H.; Gedik-Topçu, B.; Topsakal, S. The Association between Central Adiposity and Autonomic Dysfunction in Obesity. Med Princ. Pr. 2016, 25, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.Y.; Park, T.S. Role of inflammatory biomarkers in diabetic peripheral neuropathy. J. Diabetes Investig. 2017, 9, 1016–1018. [Google Scholar] [CrossRef]
- Swarbrick, M.M.; Havel, P.J. Physiological, Pharmacological, and Nutritional Regulation of Circulating Adiponectin Concentrations in Humans. Metab. Syndr. Relat. Disord. 2008, 6, 87–102. [Google Scholar] [CrossRef] [Green Version]
- Boulton, A.J.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apelqvist, J. The global burden of diabetic foot disease. Lancet 2005, 366, 1719–1724. [Google Scholar] [CrossRef]
- Williams, R.; Colagiuri, S.; Almutairi, R.; Aschner Montoya, P.; Basit, A.; Beran, D. IDF Diabetes Atlas, 9th ed.; Suvi, K., Belma, M., Pouya, S., Paraskevi, S., Eds.; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- Grisold, A.; Callaghan, B.C.; Feldman, E.L. Mediators of diabetic neuropathy. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Reference | Population Characteristics | Measurement of Neuropathy | Main Outcomes | ||
|---|---|---|---|---|---|
| Balducci et al. 2014 [15] | N | 400 | Questionnaire Michigan Neuropathy Screening Instrument [16] Diapason and biothesiometer Monofilament | The vibration perception threshold in the malleolus and hallux, was higher in type 1 diabetics than in type 2 diabetics. No differences were found in amplitude, conduction velocity and distal latency of sural sensory nerve, between type 1 and type 2 diabetics. | |
| Mean duration of DM | T1 | 22.1 ± 11.1 | |||
| T2 | 14.0 ± 9.0 | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 7.44 ± 1.38 | |||
| T2 | 7.08 ± 1.45 | ||||
| Gender (%) |  | 43% | |||
 | 57% | ||||
| Age (mean) | 61.9 ± 11.1 | ||||
| Meyer et al. 2003 [17] | N | 42 | Pain and thermal sensitivity tester [18] Diapason | The frequency of cold sensitivity impairment was higher in type 2 diabetics than in type 1 (60% vs. 40%) The impairment of heat sensitivity was only found in 10% of type 1 diabetics. The frequency of vibration sensitivity impairment was higher in type 2 diabetics than in type 1 (45% vs. 15%) The impairment of pain sensitivity was not found in neither group of diabetics. | |
| Mean duration of DM | T1 | 7.8 ± 2.3 | |||
| T2 | 10.4 ± 2.4 | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 9.4 ± 0.6 | |||
| T2 | 8.3 ± 0.3 | ||||
| Gender (%) | | 54.8% | |||
| | 45.2% | ||||
| Age (mean) | 46.3 ± 2 | ||||
| Aulich et al. 2019 [19] | N | 198 | Neurosensory Analyzer model TSA-II [20] →Thermal sensitivity for cold and hot at the left foot dorsum. →Vibratory sensitivity at the left malleolus and left great toe. | The prevalence of sensory neuropathy was higher in type 2 diabetics than in type 1 diabetics. | |
| Mean duration of DM | T1 | 8.1 | |||
| T2 | 1.8 | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 8.5 | |||
| T2 | 6.6 | ||||
| Gender (%) | | 49% | |||
| | 51% | ||||
| Age (mean) | 15.5 ± 2.4 | ||||
| Schamarek et al. 2016 [21] | N | 513 | Questionnaire Neuropathy Disability Score and Questionnaire Neuropathy Symptom Score [22] Electromyography | The prevalence of sensory neuropathy was higher in type 2 diabetics which was reflected in a lower sensory nerve conduction rate. Neuropathy Disability Score (NDS) and Neuropathy Symptom Score (NSS) were also more altered in type 2 diabetics. | |
| Mean duration of DM | T1 | Not reported | |||
| T2 | Not reported | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 6.91 ± 1.70 | |||
| T2 | 6.53 ± 1.09 | ||||
| Gender (%) | | 35.5% | |||
| | 64.5% | ||||
| Age (mean) | 47.4 ± 11.2 | ||||
| Nybo et al. 2009 [23] | N | 505 | Semmes–Weinstein monofilament | Neuropathy was more prevalent in type 1 diabetic patients. | |
| Mean duration of DM | T1 | 42–43 approx. | |||
| T2 | 4.2–5.7 approx. | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 7.5–7.8 approx. | |||
| T2 | 7.3–7.5 approx. | ||||
| Gender (%) | | 43% | |||
| | 57% | ||||
| Age (mean) | 58.3 ± 10.4 | ||||
| Reference | Population Characteristics | Measurement of Neuropathy | Main Outcomes | ||
|---|---|---|---|---|---|
| Balducci et al. 2014 [15] | N | 400 | Questionnaire Michigan Neuropathy Screening Instrument [16] Dynamometer: muscle contraction of shoulders and lower limbs. Electromyography: →Conduction velocity, amplitude, and distal latency of motor peroneal nerve and sensory sural nerve. | Muscle strength was higher in type 1 diabetics than in type 2 diabetics. | |
| Mean duration of DM | T1 | 80 | |||
| T2 | 14.0 ± 9.0 | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 7.44 ± 1.38 | |||
| T2 | 7.08 ± 1.45 | ||||
| Gender (%) | | 43% | |||
| | 57% | ||||
| Age (mean) | 61.9 ± 11.1 | ||||
| Schamarek et al. 2016 [21] | N | 513 | Questionnaire Neuropathy Disability Score and Questionnaire Neuropathy Symptom Score [22] Electromyography: →Conduction velocity of medium, ulnar, and peroneal motor nerves. | The prevalence of motor neuropathy was higher in type 2 diabetics. Neuropathy Disability Score (NDS) and Neuropathy Symptom Score (NSS) were also more altered in type 2 diabetics. | |
| Mean duration of DM | T1 | 161 | |||
| T2 | Not reported | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 6.91 ± 1.70 | |||
| T2 | 6.53 ± 1.09 | ||||
| Gender (%) | | 35.5% | |||
| | 64.5% | ||||
| Age (mean) | 47.4 ± 11.2 | ||||
| Arnold et al. 2013 [24] | N | 40 | Total Neuropathy Score [25] Electromyography: →Conduction velocity of motor nerves Nerve excitability testing: →Compound muscle action potentials of median motor nerve at the wrist | Abnormalities in nerve excitability parameters were found in type 1 diabetes patients. | |
| Mean duration of DM | T1 | 7.78 ± 1.33 | |||
| T2 | 8.07 ± 1.14 | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 7.64 ± 0.33 | |||
| T2 | 7.70 ± 0.39 | ||||
| Gender (%) | | 27.5% | |||
| | 72.5% | ||||
| Age (mean) | 41 | ||||
| Reference | Population Study Characteristics | Measurement of Neuropathy | Main Outcomes | ||
|---|---|---|---|---|---|
| Balducci et al. 2014 [15] | N | 400 | CV autonomic reflex tests: heart rate variation during rest, to deep breathing, to cough test, to standing, systolic blood pressure falls on standing. | No differences were found for the systolic blood pressure response to standing, between type 1 diabetics and type 2 diabetics. Heart rate response to deep breathing was higher in type 1 diabetics than in type 2. Heart rate response to standing was higher in type 1 diabetics than in type 2. No differences were found between both groups of diabetics in heart rate variation during rest, and in cough test. | |
| Mean duration of DM | T1 | 22.1 ± 11.1 | |||
| T2 | 14.0 ± 9.0 | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 7.44 ± 1.38 | |||
| T2 | 7.08 ± 1.45 | ||||
| Gender (%) | | 43% | |||
| | 57% | ||||
| Age (mean) | 61.9 ± 11.1 | ||||
| Meyer et al. 2003 [17] | N | 42 | CV autonomic reflex tests: heart rate variation during rest, to deep breathing, to Valsalva maneuver. Peripheral sympathetic test: laser doppler anemometry for vasomotion assessment. | In type 1 diabetes patients, vasomotion impairment was more common in subjects with autonomous neuropathy than in those without it. In contrast, in type 2 diabetics group, no differences were found in deterioration of vasomotion between subjects with and subjects without autonomic neuropathy. Type 1 diabetics who did not suffer autonomic neuropathy had vasomotion amplitudes greater than those with autonomic neuropathy while in type 2 diabetics, no differences were observed. In both type 1 and type 2 diabetics, a positive association was found between vasomotion amplitudes and Valsalva ratio. There no was correlation between vasomotion amplitudes and variation heart rate during deep breathing test, in neither group. | |
| Mean duration of DM | T1 | 7.8 ± 2.3 | |||
| T2 | 10.4 ± 2.4 | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 9.4 ± 0.6 | |||
| T2 | 8.3 ± 0.3 | ||||
| Gender (%) | | 54.8% | |||
| | 45.2% | ||||
| Age (mean) | 46.3 ± 2 | ||||
| Fedele et al. 1998 [26] | N | 9868 | Interview about presence or absence of erectile dysfunction (achieving and maintaining a sufficient erection for a satisfactory sexual relationship). Review of the medical history | The prevalence of erectile dysfunction was much higher in type 2 diabetics than in type 1 diabetics. | |
| Mean duration of DM | T1 | Not reported | |||
| T2 | Not reported | ||||
| Level of glycemic control (HbA1c) (%) | T1 | Not reported | |||
| T2 | Not reported | ||||
| Gender (%) | | 0% | |||
| | 100% | ||||
| Age (range) | 20–69 | ||||
| Fedele et al. 2001 [27] | N | 1010 | Interview about presence or absence of erectile dysfunction (achieving and maintaining a sufficient erection for a satisfactory sexual relationship). | The incidence of erectile dysfunction over a follow-up period of 2.8 years was 1.6 times higher in type 2 diabetics than in type 1 diabetics. | |
| Mean duration of DM | T1 | Not reported | |||
| T2 | Not reported | ||||
| Level of glycemic control (HbA1c) (%) | T1 | Not reported | |||
| T2 | Not reported | ||||
| Gender (%) | | 0% | |||
| | 100% | ||||
| Age | 19–79 | ||||
| Aulich et al. 2019 [19] | N | 198 | Variability of basal heart rate during 10 minutes of supine decubitus by ECG. | The prevalence of cardiac autonomous neuropathy was higher in type 2 than in type 1 young diabetics. | |
| Mean duration of DM | T1 | 8.1 | |||
| T2 | 1.8 | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 8.5 | |||
| T2 | 6.6 | ||||
| Gender (%) | | 49% | |||
| | 51% | ||||
| Age (mean) | 15.5 ± 2.4 | ||||
| Pan et al. 2019 [28] | N | 2.048 | CV autonomic reflex tests: heart rate response to deep breathing, heart rate response to Valsalva maneuver, to standing systolic blood pressure response to standing | The prevalence of cardiac autonomous neuropathy was similar between type 1 and type 2 diabetics. In type 1 diabetics, the optimal diagnostic strategy for CAN was the combination of the variation in HR during the Valsalva maneuver and in response to standing. In contrast, in type 2 diabetics, the HR variation test in response to deep breathing had great sensitivity and the best combination was with the Valsalva maneuver. | |
| Mean duration of DM | T1 | Not reported | |||
| T2 | Not reported | ||||
| Level of glycemic control (HbA1c) (%) | T1 | Not reported | |||
| T2 | Not reported | ||||
| Gender (%) | | 50% | |||
| | 50% | ||||
| Age (mean) | 58.86 ± 10.8 | ||||
| Gulichsen et al. 2012 [29] | N | 323 | CV autonomic reflex tests using a new handheld device VagusTM [30]: heart rate variation during rest, heart rate response to deep breathing, to Valsalva maneuver, to standing. | The prevalence of cardiac autonomous neuropathy was higher in type 2 diabetics than in type 1 diabetics. | |
| Mean duration of DM | T1 | Not reported | |||
| T2 | Not reported | ||||
| Level of glycemic control (HbA1c) (%) | T1 | Not reported | |||
| T2 | Not reported | ||||
| Gender (%) | | 46.1% | |||
| | 53.9% | ||||
| Age (mean) | 56.1 ± 11.4 | ||||
| Ayad et al. 2010 [31] | N | 310 | Questionnaire of symptoms CV autonomic reflex tests: heart rate response to deep breathing, to standing, and to Valsalva maneuver. Systolic blood pressure response to standing. | No differences were found between the diabetic groups regarding the prevalence of postural hypotension. The prevalence of neuropathy did not show significant differences between type 1 diabetics and type 2 diabetics, although in this latter group, it was slightly higher. Among type 2 diabetics, neuropathy was more severe in those treated with insulin compared to those treated with oral antidiabetics. | |
| Mean duration of DM | T1 | 9.8 ± 7.7 | |||
| T2 | 7.4 ± 13.6 | ||||
| Level of glycemic control (HbA1c) (%) | T1 | 10.4 ± 2.7 | |||
| T2 | 9.8 2.5 | ||||
| Gender (%) | | 53.2% | |||
| | 46.8% | ||||
| Age (mean) | 41.7 ± 12.8 | ||||
| Pappachan et al. 2008 [32] | N | 100 | CV autonomic reflex tests: Heart rate during rest, to deep breathing, to Valsalva maneuver. Systolic blood pressure response to standing. Assessment of diastolic blood pressure response during sustained handgrip. Determination of QTc interval (ECG) | The maximum systolic and diastolic BP during exercise were not different between patients with retinopathy and patients without retinopathy, in neither diabetic group. Recovery of systolic and diastolic BP at 2 minutes post exercise was not different between those diabetics with retinopathy and those without, in the group of type 1 diabetics. In contrast, in type 2 diabetics, the recovery of SBP was higher in subjects with retinopathy, while this difference was not observed for DBP. In both groups of diabetics, univariate analysis showed a significant and positive correlation between severity of CAN and prolongation of QTc interval. | |
| Mean duration of DM | T1 | Not reported | |||
| T2 | Not reported | ||||
| Level of glycemic control (HbA1c) (%) | T1 | Not reported | |||
| T2 | Not reported | ||||
| Gender (%) | | 60% | |||
| | 40% | ||||
| Age (Median) | 53 | ||||
| Koçkar et al. 2002 [33] | N | 40 | Determination of QTc interval (ECG) | In both diabetic groups, QTc dispersion was longer than in healthy controls, but this difference only was significant in type 2 diabetics. Gastric emptying time was significantly higher in type 1 and type 2 diabetics than healthy controls. | |
| Mean duration of DM | T1 | Not reported | |||
| T2 | Not reported | ||||
| Level of glycemic control (HbA1c) (%) | T1 | Not reported | |||
| T2 | Not reported | ||||
| Gender (%) | | 35% | |||
| | 65% | ||||
| Age | 39.5 ± 9.3 | ||||
| Palasciano et al. 1992 [34] | N | 21 | Electromyography: Function of the striatum muscle. Conduction velocity and potential amplitude of deep peroneal motor nerves. Ultrasound for evaluate gallbladder volume and study motor function (motility), during fasting and after intake. | Motor function of gallbladder was not correlated with type of diabetes. | |
| Mean duration of DM | T1 | Not reported | |||
| T2 | Not reported | ||||
| Level of glycemic control (HbA1c) (%) | T1 | Not reported | |||
| T2 | Not reported | ||||
| Gender (%) | | 52% | |||
| | 48% | ||||
| Age (mean) | 50 ± 15 | ||||
| Kramer et al. 2008 [35] | N | 112 | Exercise electrocardiography (at different intervals): heart rate and blood pressure at rest and estimated workload in metabolic equivalents (METs). CV autonomic reflex tests: heart rate response to Valsalva maneuver, beat-to-beat heart rate variation. Heart rate response to standing. Postural fall in blood pressure. Assessment of diastolic blood pressure response during sustained handgrip. | Autonomous cardiac neuropathy, detected by tests of variability of HR with exercise, was related to the development of retinopathy in subjects with type I and type II diabetes. | |
| Mean duration of DM | T1 | 21.5–27 approx. | |||
| T2 | 8.7–10.7 approx. | ||||
| Level of glycemic control (HbA1c) (%) | T1 | Not reported | |||
| T2 | Not reported | ||||
| Gender (%) | | 43% | |||
| | 57% | ||||
| Age (mean) | 51.6 ± 9 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sempere-Bigorra, M.; Julián-Rochina, I.; Cauli, O. Differences and Similarities in Neuropathy in Type 1 and 2 Diabetes: A Systematic Review. J. Pers. Med. 2021, 11, 230. https://doi.org/10.3390/jpm11030230
Sempere-Bigorra M, Julián-Rochina I, Cauli O. Differences and Similarities in Neuropathy in Type 1 and 2 Diabetes: A Systematic Review. Journal of Personalized Medicine. 2021; 11(3):230. https://doi.org/10.3390/jpm11030230
Chicago/Turabian StyleSempere-Bigorra, Mar, Iván Julián-Rochina, and Omar Cauli. 2021. "Differences and Similarities in Neuropathy in Type 1 and 2 Diabetes: A Systematic Review" Journal of Personalized Medicine 11, no. 3: 230. https://doi.org/10.3390/jpm11030230