
Risk of Dementia in Patients Who Underwent Surgery under Neuraxial Anesthesia: A Nationwide Cohort Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
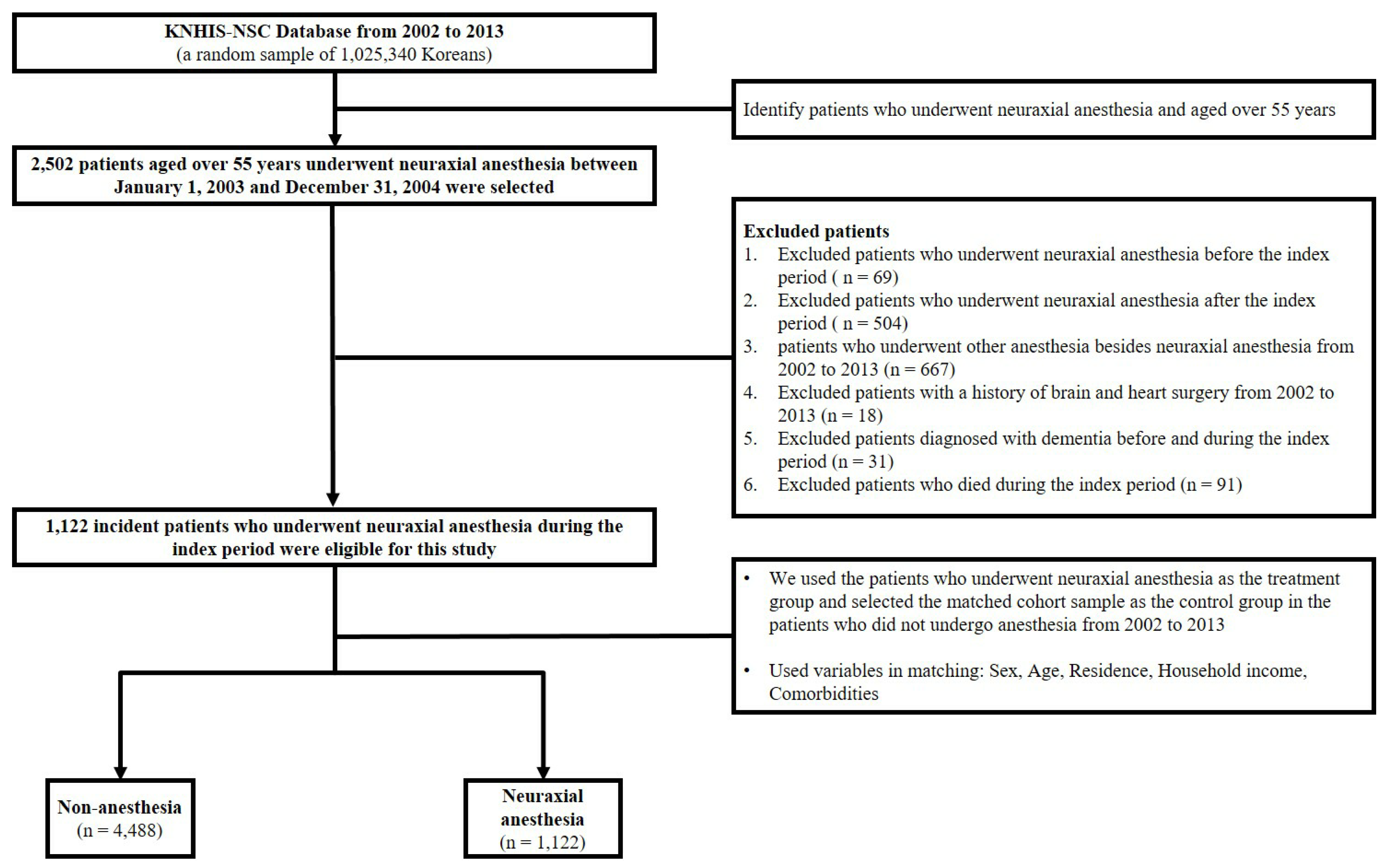
2.1. National Sample Cohort
2.2. Study Setting and Participants
2.3. Predictor and Outcome Variables
2.4. Statistical Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Comparison (n = 4488) | Surgery under Neuraxial Anesthesia (n = 1122) | p Value | |
|---|---|---|---|---|
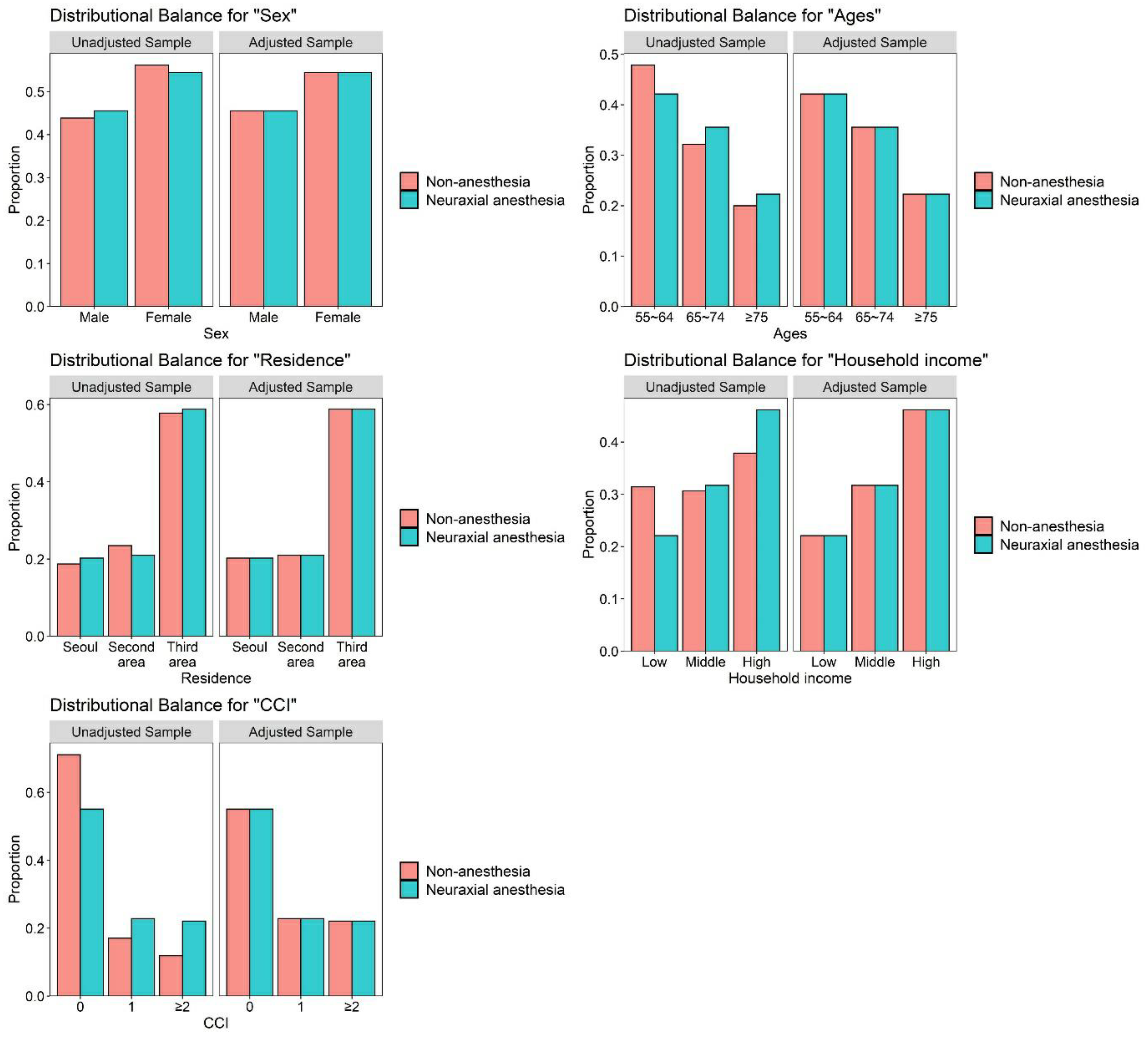
| Sex | Male | 2044 (45.5%) | 511 (45.5%) | 1.000 |
| Female | 2444 (54.5%) | 611 (54.5%) | ||
| Ages | 55–64 | 1892 (42.2%) | 473 (42.2%) | 1.000 |
| 65–74 | 1596 (35.6%) | 399 (35.6%) | ||
| ≥75 | 1000 (22.3%) | 250 (22.3%) | ||
| Residence | Seoul | 908 (20.2%) | 227 (20.2%) | 1.000 |
| Second area | 940 (20.9%) | 235 (20.9%) | ||
| Third area | 2640 (58.8%) | 660 (58.8%) | ||
| Household | Low (0–30%) | 992 (22.1%) | 248 (22.1%) | 1.000 |
| Middle (30–70%) | 1424 (31.7%) | 356 (31.7%) | ||
| High (70–100%) | 2072 (46.2%) | 518 (46.2%) | ||
| CCI | 0 | 2472 (55.1%) | 618 (55.1%) | 1.000 |
| 1 | 1024 (22.8%) | 256 (22.8%) | ||
| ≥2 | 992 (22.1%) | 248 (22.1%) |
3. Results
3.1. Effects of the Surgery under Neuraxial Anesthesia on the Incidence of Dementia among Patients Aged over 55 Years
3.2. Hazard Ratios of Dementia in Patients Aged over 55 Years and Who Underwent Surgery under Neuraxial Anesthesia

| Variables | N | Case | Incidence | Unadjusted HR (95% CI) | Adjusted HR (95% CI) | p Value |
|---|---|---|---|---|---|---|
| Group | ||||||
| Comparison | 4488 | 442 | 11.49 | 1.00 (ref) | 1.00 (ref) | |
| Surgery under neuraxial anesthesia | 1122 | 121 | 14.78 | 1.40 (1.14–1.72) ** | 1.44 (1.17–1.76) *** | <0.001 |
| Sex | ||||||
| Male | 2555 | 192 | 9.33 | 1.00 (ref) | 1.00 (ref) | |
| Female | 3055 | 371 | 14.23 | 1.51 (1.27–1.80) *** | 1.32 (1.10–1.57) ** | 0.002 |
| Ages (years) | ||||||
| 55–64 | 2365 | 77 | 3.40 | 1.00 (ref) | 1.00 (ref) | |
| 65–74 | 1995 | 240 | 14.35 | 4.44 (3.43–5.74) *** | 4.26 (3.29–5.51) *** | <0.001 |
| ≥75 | 1250 | 246 | 33.66 | 11.90 (9.20–15.40) *** | 11.36 (8.77–14.72) *** | <0.001 |
| Residence | ||||||
| Seoul | 1135 | 99 | 9.99 | 1.00 (ref) | 1.00 (ref) | |
| Second area | 1175 | 126 | 12.92 | 1.31 (1.01–1.70) * | 1.19 (0.92–1.56) | 0.188 |
| Third area | 3300 | 338 | 12.52 | 1.27 (1.02–1.59) * | 1.0aq7 (0.85–1.34) | 0.573 |
| Household income | ||||||
| Low (0–30%) | 1240 | 132 | 13.12 | 1.00 (ref) | 1.00 (ref) | |
| Middle (30–70%) | 1780 | 151 | 10.09 | 0.76 (0.60–0.96) * | 0.87 (0.69–1.10) | 0.239 |
| High (70–100%) | 2590 | 280 | 12.94 | 0.98 (0.79–1.20) | 0.99 (0.80–1.21) | 0.894 |
| CCI | ||||||
| 0 | 3090 | 283 | 10.54 | 1.00 (ref) | 1.00 (ref) | |
| 1 | 1280 | 163 | 15.24 | 1.47 (1.21–1.78) *** | 1.37 (1.13–1.66) ** | 0.001 |
| ≥2 | 1240 | 117 | 12.82 | 1.25 (1.01–1.55) * | 1.21 (0.97–1.50) | 0.091 |


4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Comorbidities | International Classification of Disease, 10th Revision Code | Original Weight | Updated Weight |
|---|---|---|---|
| Myocardial infarction | I21.x, I22.x, I25.2 | 1 | 0 |
| Congestive heart failure | I09.9, I11.0, I13.0, I13.2, I25.5, I42.0, I42.5–I42.9, I43.x, I50.x, P29.0 | 1 | 2 |
| Peripheral vascular disease | I70.x, I71.x, I73.1, I73.8, I73.9, I77.1, I79.0, I79.2, K55.1, K55.8, K55.9, Z95.8, Z95.9 | 1 | 0 |
| Cerebrovascular disease | G45.x, G46.x, H34.0, I60.x–I69.x | 1 | 0 |
| Chronic pulmonary disease | I27.8, I27.9, J40.x–J47.x, J60.x–J67.x, J68.4, J70.1, J70.3 | 1 | 1 |
| Rheumatologic disease | M05.x, M06.x, M31.5, M32.x–M34.x, M35.1, M35.3, M36.0 | 1 | 1 |
| Peptic ulcer disease | K25.x–K28.x | 1 | 0 |
| Mild liver disease | B18.x, K70.0–K70.3, K70.9, K71.3–K71.5, K71.7, K73.x, K74.x, K76.0, K76.2–K76.4, K76.8, K76.9, Z94.4 | 1 | 2 |
| Diabetes without chronic complication | E10.0, E10.1, E10.6, E10.8, E10.9, E11.0, E11.1, E11.6, E11.8, E11.9, E12.0, E12.1, E12.6, E12.8, E12.9, E13.0, E13.1, E13.6, E13.8, E13.9, E14.0, E14.1, E14.6, E14.8, E14.9 | 1 | 0 |
| Diabetes with chronic complication | E10.2–E10.5, E10.7, E11.2–E11.5, E11.7, E12.2–E12.5, E12.7, E13.2–E13.5, E13.7, E14.2–E14.5, E14.7 | 2 | 1 |
| Hemiplegia or paraplegia | G04.1, G11.4, G80.1, G80.2, G81.x, G82.x, G83.0–G83.4, G83.9 | 2 | 2 |
| Renal disease | I12.0, I13.1, N03.2–N03.7, N05.2–N05.7, N18.x, N19.x, N25.0, Z49.0–Z49.2, Z94.0, Z99.2 | 2 | 1 |
| Any malignancy including leukemia and lymphoma | C00.x–C26.x, C30.x–C34.x, C37.x–C41.x, C43.x, C45.x–C58.x, C60.x–C76.x, C81.x–C85.x, C88.x, C90.x–C97.x | 2 | 2 |
| Moderate or severe liver disease | I85.0, I85.9, I86.4, I98.2, K70.4, K71.1, K72.1, K72.9, K76.5, K76.6, K76.7 | 3 | 4 |
| Metastatic solid tumor | C77.x–C80.x | 6 | 6 |
| Acquired immune deficiency syndrome/human immunodeficiency virus | B20.x–B22.x, B24.x | 6 | 4 |
| The Number of Dementia Event | |
|---|---|
| Event | 563 |
| Non-anesthesia | 442 |
| Neuraxial anesthesia | 121 |
| Total censored (No event) | 5047 |
| Non-anesthesia | 4046 |
| Neuraxial anesthesia | 1001 |
| Termination of study | 3679 |
| Non-anesthesia | 2942 |
| Neuraxial anesthesia | 737 |
| Loss to follow up/Drop-out | 1368 |
| Non-anesthesia | 1104 |
| Neuraxial anesthesia | 264 |
References
- Morgan, G.E.; Mikhail, M.S. Morgan & Mikhail’s Clinical Anesthesiology; McGraw-Hill Education: New York, NY, USA, 2018. [Google Scholar]
- Elsharydah, A.; Li, F.C.; Minhajuddin, A.; Gabriel, R.A.; Joshi, G.P. Risk score for major complications after total hip arthroplasty: The beneficial effect of neuraxial anesthesia. A retrospective observational study. Curr. Orthop. Pract. 2020, 31, 156–161. [Google Scholar] [CrossRef]
- Basques, B.; Bohl, D.; Golinvaux, N.; Samuel, A.; Grauer, J. General versus spinal anaesthesia for patients aged 70 years and older with a fracture of the hip. Bone Jt. J. 2015, 97, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.M.; Cozowicz, C.; Uda, Y.; Memtsoudis, S.G.; Barrington, M.J. Neuraxial and combined neuraxial/general anesthesia compared to general anesthesia for major truncal and lower limb surgery: A systematic review and meta-analysis. Anesth. Analg. 2017, 125, 1931–1945. [Google Scholar] [CrossRef] [PubMed]
- Gasparini, M.; Vanacore, N.; Schiaffini, C.; Brusa, L.; Panella, M.; Talarico, G.; Bruno, G.; Meco, G.; Lenzi, G.L. A case-control study on Alzheimer’s disease and exposure to anesthesia. Neurol. Sci. 2002, 23, 11–14. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.M.; Grega, M.A.; Borowicz, L.M.; Bailey, M.M.; Barry, S.J.E.; Zeger, S.L.; Baumgartner, W.A.; Selnes, O.A. Is there cognitive decline 1 year after CABG? Comparison with surgical and nonsurgical controls. Neurology 2006, 65, 991–999. [Google Scholar] [CrossRef]
- Knopman, D.; Petersen, R.; Cha, R.; Edland, S.; Rocca, W. Coronary artery bypass grafting is not a risk factor for dementia or Alzheimer disease. Neurology 2005, 65, 986–990. [Google Scholar] [CrossRef]
- Tang, J.; Eckenhoff, M.F.; Eckenhoff, R.G. Anesthesia and the Old Brain. Anesth. Analg. 2010, 110, 421–426. [Google Scholar] [CrossRef]
- Aiello Bowles, E.J.; Larson, E.B.; Pong, R.P.; Walker, R.L.; Anderson, M.L.; Yu, O.; Gray, S.L.; Crane, P.K.; Dublin, S. Anesthesia Exposure and Risk of Dementia and Alzheimer’s Disease: A Prospective Study. J. Am. Geriatr. Soc. 2016, 64, 602–607. [Google Scholar] [CrossRef] [Green Version]
- Fong, H.K.; Sands, L.P.; Leung, J.M. The role of postoperative analgesia in delirium and cognitive decline in elderly patients: A systematic review. Anesth. Analg. 2006, 102, 1255–1266. [Google Scholar] [CrossRef]
- Seitz, D.P.; Shah, P.S.; Herrmann, N.; Beyene, J.; Siddiqui, N. Exposure to general anesthesia and risk of Alzheimer’s disease: A systematic review and meta-analysis. BMC Geriatr. 2011, 11, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ehsani, R.; Motlagh, S.D.; Zaman, B.; Kashani, S.S.; Ghodraty, M.R. Effect of general versus spinal anesthesia on postoperative delirium and early cognitive dysfunction in elderly patients. Anesthesiol. Pain Med. 2020, 10, e101815. [Google Scholar] [CrossRef]
- Zhang, B.; Tian, M.; Zhen, Y.; Yue, Y.; Sherman, J.; Zheng, H.; Li, S.; Tanzi, R.E.; Marcantonio, E.R.; Xie, Z. The effects of isoflurane and desflurane on cognitive function in humans. Anesth. Analg. 2012, 114, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silbert, B.; Evered, L.; Scott, D. Incidence of postoperative cognitive dysfunction after general or spinal anaesthesia for extracorporeal shock wave lithotripsy. Br. J. Anaesth. 2014, 113, 784–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langa, K.M.; Larson, E.B.; Crimmins, E.M.; Faul, J.D.; Levine, D.A.; Kabeto, M.U.; Weir, D.R. A Comparison of the Prevalence of Dementia in the United States in 2000 and 2012. JAMA Intern. Med. 2017, 177, 51–58. [Google Scholar] [CrossRef]
- Liu, C.C.; Liu, C.H.; Sun, Y.; Lee, H.J.; Tang, L.Y.; Chiu, M.J. Rural-urban disparities in the prevalence of mild cognitive impairment and dementia in Taiwan: A door-to-door nationwide study. J. Epidemiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.E. Potential Neurotoxicity of Spinal Anesthesia with Lidocaine Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2000; pp. 921–932. [Google Scholar]
- Werdehausen, R.; Braun, S.; Essmann, F.; Schulze-Osthoff, K.; Walczak, H.; Lipfert, P.; Stevens, M.F. Lidocaine induces apoptosis via the mitochondrial pathway independently of death receptor signaling. Anesthesiology 2007, 107, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Fathy, W.; Hussein, M.; Khalil, H. Effect of local anesthesia (with lidocaine vs. bupivacaine) on cognitive function in patients undergoing elective cataract surgery. Local Reg. Anesth. 2018, 12, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, Y.; Xu, J.; Ma, D.; Zeng, Y.; Cibelli, M.; Maze, M. Postoperative Impairment of Cognitive Function in Rats: A Possible Role for Cytokine-mediated Inflammation in the Hippocampus. Anesthesiology 2007, 106, 436–443. [Google Scholar] [CrossRef]
- Cibelli, M.; Fidalgo, A.R.; Terrando, N.; Ma, D.; Monaco, C.; Feldmann, M.; Takata, M.; Lever, I.J.; Nanchahal, J.; Fanselow, M.S. Role of interleukin-1β in postoperative cognitive dysfunction. Ann. Neurol. 2010, 68, 360–368. [Google Scholar] [CrossRef] [Green Version]
- Terrando, N.; Monaco, C.; Ma, D.; Foxwell, B.M.J.; Feldmann, M.; Maze, M. Tumor necrosis factor-α triggers a cytokine cascade yielding postoperative cognitive decline. Proc. Natl. Acad. Sci. USA 2010, 107, 20518–20522. [Google Scholar] [CrossRef] [Green Version]
- Alam, A.; Hana, Z.; Jin, Z.; Suen, K.C.; Ma, D. Surgery, neuroinflammation and cognitive impairment. EBioMedicine 2018, 37, 547–556. [Google Scholar] [CrossRef] [Green Version]
- Wan, Y.; Xu, J.; Meng, F.; Bao, Y.; Ge, Y.; Lobo, N.; Vizcaychipi, M.P.; Zhang, D.; Gentleman, S.M.; Maze, M.; et al. Cognitive decline following major surgery is associated with gliosis, β-amyloid accumulation, and τ phosphorylation in old mice. Crit. Care Med. 2010, 38, 2190–2198. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhou, M.; Jia, X.; Zhang, W.; Shi, Y.; Bai, S.; Rampes, S.; Vizcaychipi, M.P.; Wu, C.; Wang, K.; et al. Inflammation Disrupts the Brain Network of Executive Function After Cardiac Surgery. Ann. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Edmondson, M.; Sakamoto, A.; Ma, D. Anesthesia, surgical stress, and “long-term” outcomes. Acta Anaesthesiol. Taiwanica 2015, 53, 99–104. [Google Scholar] [CrossRef]
- Guo, Y.; Li, Y.; Zhang, Y.; Fang, S.; Xu, X.; Zhao, A.; Zhang, J.; Li, J.V.; Ma, D.; Jia, W.; et al. Post-operative delirium associated with metabolic alterations following hemi-arthroplasty in older patients. Age Ageing 2019, 49, 88–95. [Google Scholar] [CrossRef]
- Jin, Z.; Hu, J.; Ma, D. Postoperative delirium: Perioperative assessment, risk reduction, and management. Br. J. Anaesth. 2020, 125, 492–504. [Google Scholar] [CrossRef]
- Alam, A.; Ma, D. Is it time to Assess Neurological Status before Surgery to Improve Postoperative Outcomes? Ann. Surg. 2021. Available online: https://journals.lww.com/annalsofsurgery/Citation/9000/Is_it_time_to_Assess_Neurological_Status_before.93207.aspx (accessed on 13 December 2021). [CrossRef]
- Kwak, K.-H. Postdural puncture headache. Korean J. Anesth. 2017, 70, 136–143. [Google Scholar] [CrossRef]
- Fleischman, D.; Berdahl, J.P.; Zaydlarova, J.; Stinnett, S.; Fautsch, M.P.; Allingham, R.R. Cerebrospinal fluid pressure decreases with older age. PLoS ONE 2012, 7, e52664. [Google Scholar] [CrossRef] [PubMed]
- Attier-Zmudka, J.; Sérot, J.-M.; Valluy, J.; Saffarini, M.; Macaret, A.-S.; Diouf, M.; Dao, S.; Douadi, Y.; Malinowski, K.P.; Balédent, O. Decreased Cerebrospinal Fluid Flow Is Associated With Cognitive Deficit in Elderly Patients. Front. Aging Neurosci. 2019, 11, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leffert, L.R.; Schwamm, L.H. Neuraxial Anesthesia in Parturients with Intracranial Pathology: A Comprehensive Review and Reassessment of Risk. Anesthesiology 2013, 119, 703–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yri, H.M.; Fagerlund, B.; Forchhammer, H.B.; Jensen, R.H. Cognitive function in idiopathic intracranial hypertension: A prospective case-control study. BMJ Open 2014, 4, e004376. [Google Scholar] [CrossRef] [Green Version]
- Kleinerman, J.; Sancetta, S.M.; Hackel, D.B. Effects of high spinal anesthesia on cerebral circulation and metabolism in man. J. Clin. Investig. 1958, 37, 285–293. [Google Scholar] [CrossRef]
- Schmidt, B.; Czosnyka, M.; Schwarze, J.J.; Sander, D.; Gerstner, W.; Lumenta, C.B.; Pickard, J.D.; Klingelhöfer, J. Cerebral vasodilatation causing acute intracranial hypertension: A method for noninvasive assessment. J. Cereb. Blood Flow Metab. 1999, 19, 990–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarumi, T.; Zhang, R. Cerebral blood flow in normal aging adults: Cardiovascular determinants, clinical implications, and aerobic fitness. J. Neurochem. 2018, 144, 595–608. [Google Scholar] [CrossRef] [Green Version]
- Bennett, D.A.; Wilson, R.S.; Arvanitakis, Z.; Boyle, P.A.; de Toledo-Morrell, L.; Schneider, J.A. Selected findings from the religious orders study and rush memory and aging project. J. Alzheimer’s Dis. 2013, 33, S397–S403. [Google Scholar] [CrossRef]
- Chui, H.C.; Zarow, C.; Mack, W.J.; Ellis, W.G.; Zheng, L.; Jagust, W.J.; Mungas, D.; Reed, B.R.; Kramer, J.H.; DeCarli, C.C.; et al. Cognitive impact of subcortical vascular and Alzheimer’s disease pathology. Ann. Neurol. 2006, 60, 677–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toledo, J.B.; Arnold, S.E.; Raible, K.; Brettschneider, J.; Xie, S.X.; Grossman, M.; Monsell, S.E.; Kukull, W.A.; Trojanowski, J.Q. Contribution of cerebrovascular disease in autopsy confirmed neurodegenerative disease cases in the National Alzheimer’s Coordinating Centre. Brain 2013, 136, 2697–2706. [Google Scholar] [CrossRef]
- Groot, A.E.; Vermeij, J.-D.M.; Westendorp, W.F.; Nederkoorn, P.J.; van de Beek, D.; Coutinho, J.M. Continuation or discontinuation of anticoagulation in the early phase after acute ischemic stroke. Stroke 2018, 49, 1762–1765. [Google Scholar] [CrossRef]
- Vanga, S.R.; Satti, S.R.; Williams, J.; Weintraub, W.; Doorey, A. Discontinuation of oral anticoagulation preceding acute ischemic stroke–prevalence and outcomes: Comprehensive chart review. Postgrad. Med. 2015, 127, 791–795. [Google Scholar] [CrossRef] [Green Version]
- Das, A.S.; Regenhardt, R.W.; Vernooij, M.W.; Blacker, D.; Charidimou, A.; Viswanathan, A. Asymptomatic Cerebral Small Vessel Disease: Insights from Population-Based Studies. J. Stroke 2019, 21, 121–138. [Google Scholar] [CrossRef]
- Hamer, M.; Chida, Y. Physical activity and risk of neurodegenerative disease: A systematic review of prospective evidence. Psychol. Med. 2009, 39, 3–11. [Google Scholar] [CrossRef]
- Dementia. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 23 August 2021).
- Tschanz, J.T.; Corcoran, C.D.; Schwartz, S.; Treiber, K.; Green, R.C.; Norton, M.C.; Mielke, M.M.; Piercy, K.; Steinberg, M.; Rabins, P.V.; et al. Progression of cognitive, functional, and neuropsychiatric symptom domains in a population cohort with Alzheimer dementia: The Cache County Dementia Progression study. Am. J. Geriatr. Psychiatry 2011, 19, 532–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turrentine, F.E.; Wang, H.; Simpson, V.B.; Jones, R.S. Surgical risk factors, morbidity, and mortality in elderly patients. J. Am. Coll. Surg. 2006, 203, 865–877. [Google Scholar] [CrossRef]
- Cornellà, N.; Sancho, J.; Sitges-Serra, A. Short and Long-Term Outcomes After Surgical Procedures Lasting for More Than Six Hours. Sci. Rep. 2017, 7, 9221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGee, D.L. Local and topical anesthesia. In: Clinical Procedures. In Emergency Medicine, 5th ed.; Roberts, J.R., Hedges, J.R., Eds.; Saunders: Philadelphia, PA, USA, 2010; p. 481. [Google Scholar]
- Hruza, G.J. Anesthesia. In Dermatology, 2nd ed.; Bolognia, J.L., Jorizzo, J.L., Rapini, R.P., Eds.; Mosby: St. Louis, MO, USA, 2008; Volume 2, p. 2173. [Google Scholar]
- Bahl, R. Local anesthesia in dentistry. Anesth. Prog. 2004, 51, 138–142. [Google Scholar]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]

| Sex | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|
| Comparison | Surgery under Neuraxial Anesthesia | Comparison | Surgery under Neuraxial Anesthesia | |||||
| Unadjusted HR (95% CI) | 1.00 (ref) | 1.54 (1.09–2.17) * | 1.00 (ref) | 1.33 (1.03–1.71) * | ||||
| Adjusted HR (95% CI) | 1.00 (ref) | 1.60 (1.13–2.25) ** | 1.00 (ref) | 1.36 (1.05–1.75) * | ||||
| Ages | 55–64 | 65–74 | ≥75 | |||||
| Comparison | Surgery under neuraxial anesthesia | Comparison | Surgery under neuraxial anesthesia | Comparison | Surgery under neuraxial anesthesia | |||
| Unadjusted HR (95% CI) | 1.00 (ref) | 1.32 (0.74–2.35) | 1.00 (ref) | 1.30 (0.94–1.80) | 1.00 (ref) | 1.60 (1.19–2.16) ** | ||
| Adjusted HR (95% CI) | 1.00 (ref) | 1.33 (0.75–2.37) | 1.00 (ref) | 1.31 (0.95–1.81) | 1.00 (ref) | 1.60 (1.19–2.15) ** | ||
| CCI | 0 | 1 | ≥2 | |||||
| Comparison | Surgery under neuraxial anesthesia | Comparison | Surgery under neuraxial anesthesia | Comparison | Surgery under neuraxial anesthesia | |||
| Unadjusted HR (95% CI) | 1.00 (ref) | 1.55 (1.17–2.05) ** | 1.00 (ref) | 1.33 (0.90–1.96) | 1.00 (ref) | 1.18 (0.73–1.88) | ||
| Adjusted HR (95% CI) | 1.00 (ref) | 1.62 (1.23–2.15) *** | 1.00 (ref) | 1.39 (0.94–2.05) | 1.00 (ref) | 1.11 (0.69–1.77) | ||
| Variables | N | Case | Incidence | Unadjusted HR (95% CI) | Adjusted HR (95% CI) | p Value |
|---|---|---|---|---|---|---|
| Alzheimer’s Disease | ||||||
| Comparison | 4488 | 328 | 8.45 | 1.00 (ref) | 1.00 (ref) | |
| Surgery under neuraxial anesthesia | 1122 | 92 | 11.13 | 1.48 (1.17–1.87) ** | 1.52 (1.20–1.92) *** | <0.001 |
| Vascular Dementia | ||||||
| Comparison | 4488 | 95 | 2.40 | 1.00 (ref) | 1.00 (ref) | |
| Surgery under neuraxial anesthesia | 1122 | 24 | 2.84 | 1.27 (0.81–2.01) | 1.29 (0.82–2.03) | 0.273 |
| Variables | N | Case | Incidence | Unadjusted HR (95% CI) | Adjusted HR (95% CI) | p Value |
|---|---|---|---|---|---|---|
| Dementia | ||||||
| Comparison | 4488 | 442 | 11.49 | 1.00 (ref) | 1.00 (ref) | |
| Minor | 1032 | 107 | 13.95 | 1.32 (1.06–1.63) * | 1.40 (1.13–1.74) ** | 0.002 |
| Major | 90 | 14 | 27.06 | 2.76 (1.62–4.71) *** | 1.78 (1.04–3.04) * | 0.036 |
| Alzheimer’s disease | ||||||
| Comparison | 4488 | 328 | 8.45 | 1.00 (ref) | 1.00 (ref) | |
| Minor | 1032 | 81 | 10.47 | 1.38 (1.08–1.77) * | 1.48 (1.16–1.90) ** | 0.002 |
| Major | 90 | 11 | 20.88 | 3.00 (1.64–5.48) *** | 1.87 (1.02–3.44) * | 0.043 |
| Vascular dementia | ||||||
| Comparison | 4488 | 95 | 2.40 | 1.00 (ref) | 1.00 (ref) | |
| Minor | 1032 | 23 | 2.91 | 1.30 (0.82–2.06) | 1.36 (0.86–2.17) | 0.188 |
| Major | 90 | 1 | 1.80 | 0.88 (0.12–6.31) | 0.57 (0.08–4.11) | 0.577 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, Y.-S.; Lee, J.-J.; Lee, S.-H.; Kim, C.; Yu, H.; Sohn, J.-H.; Kim, D.-K. Risk of Dementia in Patients Who Underwent Surgery under Neuraxial Anesthesia: A Nationwide Cohort Study. J. Pers. Med. 2021, 11, 1386. https://doi.org/10.3390/jpm11121386
Kwon Y-S, Lee J-J, Lee S-H, Kim C, Yu H, Sohn J-H, Kim D-K. Risk of Dementia in Patients Who Underwent Surgery under Neuraxial Anesthesia: A Nationwide Cohort Study. Journal of Personalized Medicine. 2021; 11(12):1386. https://doi.org/10.3390/jpm11121386
Chicago/Turabian StyleKwon, Young-Suk, Jae-Jun Lee, Sang-Hwa Lee, Chulho Kim, Hyunjae Yu, Jong-Hee Sohn, and Dong-Kyu Kim. 2021. "Risk of Dementia in Patients Who Underwent Surgery under Neuraxial Anesthesia: A Nationwide Cohort Study" Journal of Personalized Medicine 11, no. 12: 1386. https://doi.org/10.3390/jpm11121386