
A Low-Protein Diet with a Renal-Specific Oral Nutrition Supplement Helps Maintain Nutritional Status in Patients with Advanced Chronic Kidney Disease

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
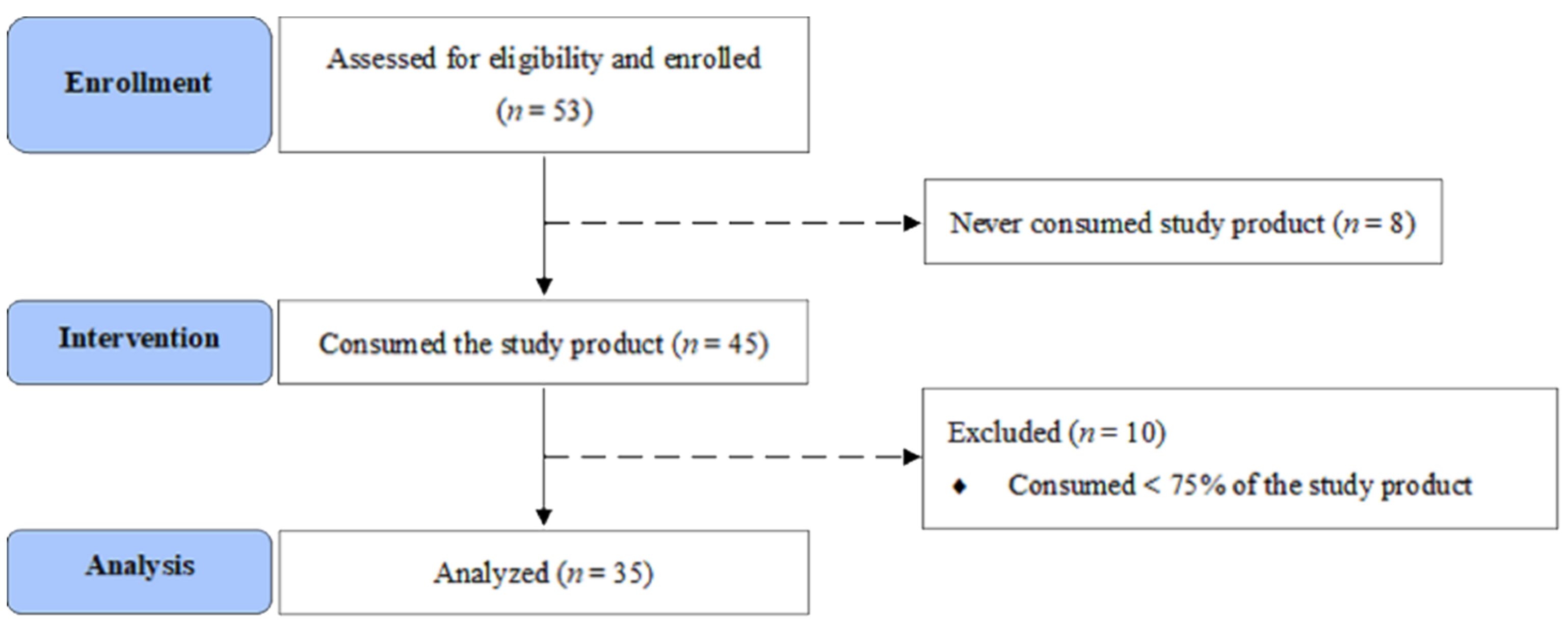
2.1. Participants and Study Design
2.2. Sample Size Calculation
2.3. Nutrition Intervention
2.4. Anthropometric Measurements
2.5. Laboratory Tests
2.6. Nutrition-Related Parameters
2.7. Quality of Life
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| BUN | Blood Urea Nitrogen |
| CKD | Chronic Kidney Disease |
| CRP | C-reactive protein |
| DEI | Dietary Energy Intake |
| DPI | Dietary Protein Intake |
| eGFR | estimated Glomerular Filtration Rate |
| HbA1c | glycated Hemoglobin |
| HOMA-IR | Homeostatic Model Assessment for Insulin Resistance |
| ITT | Intention-To-Treat |
| KDOQI | Kidney Disease Outcomes Quality Initiative |
| LDL | Low-Density Lipoprotein |
| LPD | Low-Protein Diet |
| MDRD | Modification of Diet in Renal Disease |
| MPE | Multidisciplinary Pre-ESRD Educational Program |
| NHANES | National Health and Nutrition Examination Survey |
| ONS | Oral Nutrition Supplements |
| PEW | Protein–Energy Wasting |
| RONS | Renal-Specific Oral Nutrition Supplement |
| QoL | Quality of Life |
| SD | Standard Deviation |
| SGA | Subjective Global Assessment |
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D. Global prevalence of chronic kidney disease—A systematic review and meta-analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.P.; Cheng, T.Y.; Tsai, M.K.; Chang, Y.C.; Chan, H.T.; Tsai, S.P.; Chiang, P.H.; Hsu, C.C.; Sung, P.K.; Hsu, Y.H.; et al. All-cause mortality attributable to chronic kidney disease: A prospective cohort study based on 462,293 adults in Taiwan. Lancet 2008, 371, 2173–2182. [Google Scholar] [CrossRef]
- Hwang, S.J.; Tsai, J.C.; Chen, H.C. Epidemiology, impact and preventive care of chronic kidney disease in Taiwan. Nephrology 2010, 15 (Suppl. 2), 3–9. [Google Scholar] [CrossRef]
- Wu, M.Y.; Wu, M.S. Taiwan renal care system: A learning health-care system. Nephrology 2018, 23 (Suppl. 4), 112–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Ko, G.J.; Obi, Y.; Tortorici, A.R.; Kalantar-Zadeh, K. Dietary protein intake and chronic kidney disease. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 77–85. [Google Scholar] [CrossRef]
- Fouque, D.; Laville, M. Low protein diets for chronic kidney disease in non diabetic adults. Cochrane Database Syst. Rev. 2009, CD001892. [Google Scholar] [CrossRef]
- Kovesdy, C.P.; Kopple, J.D.; Kalantar-Zadeh, K. Management of protein-energy wasting in non-dialysis-dependent chronic kidney disease: Reconciling low protein intake with nutritional therapy. Am. J. Clin. Nutr. 2013, 97, 1163–1177. [Google Scholar] [CrossRef] [Green Version]
- Carrero, J.J.; Thomas, F.; Nagy, K.; Arogundade, F.; Avesani, C.M.; Chan, M.; Chmielewski, M.; Cordeiro, A.C.; Espinosa-Cuevas, A.; Fiaccadori, E.; et al. Global prevalence of protein-energy wasting in kidney disease: A meta-analysis of contemporary observational studies from the international society of renal nutrition and metabolism. J. Ren. Nutr. 2018, 28, 380–392. [Google Scholar] [CrossRef]
- Liu, P.J.; Ma, F.; Wang, Q.Y.; He, S.L. The effects of oral nutritional supplements in patients with maintenance dialysis therapy: A systematic review and meta-analysis of randomized clinical trials. PLoS ONE 2018, 13, e0203706. [Google Scholar] [CrossRef] [Green Version]
- Huang, M.C.; Chen, M.E.; Hung, H.C.; Chen, H.C.; Chang, W.T.; Lee, C.H.; Wu, Y.Y.; Chiang, H.C.; Hwang, S.J. Inadequate energy and excess protein intakes may be associated with worsening renal function in chronic kidney disease. J. Ren. Nutr. 2008, 18, 187–194. [Google Scholar] [CrossRef]
- Chen, M.E.; Hwang, S.J.; Chen, H.C.; Hung, C.C.; Hung, H.C.; Liu, S.C.; Wu, T.J.; Huang, M.C. Correlations of dietary energy and protein intakes with renal function impairment in chronic kidney disease patients with or without diabetes. Kaohsiung J. Med. Sci. 2017, 33, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Krok-Schoen, J.L.; Archdeacon Price, A.; Luo, M.; Kelly, O.J.; Taylor, C.A. Low dietary protein intakes and associated dietary patterns and functional limitations in an aging population: A NHANES analysis. J. Nutr. Health Aging 2019, 23, 338–347. [Google Scholar] [CrossRef] [Green Version]
- Moore, L.W.; Byham-Gray, L.D.; Scott Parrott, J.; Rigassio-Radler, D.; Mandayam, S.; Jones, S.L.; Mitch, W.E.; Osama Gaber, A. The mean dietary protein intake at different stages of chronic kidney disease is higher than current guidelines. Kidney Int. 2013, 83, 724–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montes-Delgado, R.; Guerrero Riscos, M.A.; Garcia-Luna, P.P.; Martin Herrera, C.; Pereira Cunill, J.L.; Garrido Vazquez, M.; Lopez Munoz, I.; Suarez Garcia, M.J.; Martin-Espejo, J.L.; Soler Junco, M.L.; et al. Treatment with low-protein diet and caloric supplements in patients with chronic kidney failure in predialysis. Comparative study. Rev. Clin. Esp. 1998, 198, 580–586. [Google Scholar]
- Lin, M.-R. The WHOQOL-Taiwan Group: Introduction to the development of the WHOQOL-Taiwan version. Chin. Public Health 2000, 19, 315–324. [Google Scholar]
- Boutron, I.; Moher, D.; Altman, D.G.; Schulz, K.F.; Ravaud, P.; Group, C. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. Ann. Intern. Med. 2008, 148, 295–309. [Google Scholar] [CrossRef]
- Stratton, R.J.; Bircher, G.; Fouque, D.; Stenvinkel, P.; de Mutsert, R.; Engfer, M.; Elia, M. Multinutrient oral supplements and tube feeding in maintenance dialysis: A systematic review and meta-analysis. Am. J. Kidney Dis. 2005, 46, 387–405. [Google Scholar] [CrossRef] [PubMed]
- Sezer, S.; Bal, Z.; Tutal, E.; Uyar, M.E.; Acar, N.O. Long-Term oral nutrition supplementation improves outcomes in malnourished patients with chronic kidney disease on hemodialysis. JPEN J. Parenter Enteral. Nutr. 2014, 38, 960–965. [Google Scholar] [CrossRef] [Green Version]
- Chao, C.T.; Tang, C.H.; Cheng, R.W.; Wang, M.Y.; Hung, K.Y. Protein-Energy wasting significantly increases healthcare utilization and costs among patients with chronic kidney disease: A propensity-score matched cohort study. Curr. Med. Res. Opin. 2017, 33, 1705–1713. [Google Scholar] [CrossRef]
- Mah, J.Y.; Choy, S.W.; Roberts, M.A.; Desai, A.M.; Corken, M.; Gwini, S.M.; McMahon, L.P. Oral protein-based supplements versus placebo or no treatment for people with chronic kidney disease requiring dialysis. Cochrane Database Syst. Rev. 2020, 5, CD012616. [Google Scholar] [CrossRef]
- Satirapoj, B.; Prapakorn, J.; Punpanich, D.; Pongsuparbchon, C.; Supasyndh, O. The effect of ONCE Renal on minerals and electrolytes in predialysis patients with chronic kidney disease. Int. J. Nephrol. Renovasc. Dis. 2016, 9, 81–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, P.-Y.; Su, C.-T.; Chang, H.-W.; Lan, A.; Yang, S.-H. The effect of a nutritional supplement on chronic kidney disease patients. J. Food Nutr. Res. 2016, 4, 115–120. [Google Scholar]
- Chen, S.I.; Chiang, C.L.; Chao, C.T.; Chiang, C.K.; Huang, J.W. Gustatory dysfunction is closely associated with frailty in patients with chronic kidney disease. J. Ren. Nutr. 2021, 31, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Sung, C.C.; Liao, M.T.; Chao, C.T. Independent determinants of appetite impairment among patients with stage 3 or higher chronic kidney disease: A prospective study. Nutrients 2021, 13, 2863. [Google Scholar] [CrossRef]
- Hunsicker, L.G.; Adler, S.; Caggiula, A.; England, B.K.; Greene, T.; Kusek, J.W.; Rogers, N.L.; Teschan, P.E. Predictors of the progression of renal disease in the modification of diet in renal disease study. Kidney Int. 1997, 51, 1908–1919. [Google Scholar] [CrossRef] [Green Version]
- Kalantar-Zadeh, K.; Fouque, D. Nutritional management of chronic kidney disease. N. Engl. J. Med. 2017, 377, 1765–1776. [Google Scholar] [CrossRef]
- Roscioni, S.S.; Heerspink, H.J.; de Zeeuw, D. The effect of RAAS blockade on the progression of diabetic nephropathy. Nat. Rev. Nephrol. 2014, 10, 77–87. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Chang, Y.T.; Wu, H.L.; Guo, H.R.; Cheng, Y.Y.; Tseng, C.C.; Wang, M.C.; Lin, C.Y.; Sung, J.M. Handgrip strength is an independent predictor of renal outcomes in patients with chronic kidney diseases. Nephrol. Dial. Transpl. 2011, 26, 3588–3595. [Google Scholar] [CrossRef] [Green Version]
- Speeckaert, M.; Van Biesen, W.; Delanghe, J.; Slingerland, R.; Wiecek, A.; Heaf, J.; Drechsler, C.; Lacatus, R.; Vanholder, R.; Nistor, I.; et al. Are there better alternatives than haemoglobin A1c to estimate glycaemic control in the chronic kidney disease population? Nephrol. Dial. Transpl. 2014, 29, 2167–2177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spoto, B.; Pisano, A.; Zoccali, C. Insulin resistance in chronic kidney disease: A systematic review. Am. J. Physiol. Renal. Physiol. 2016, 311, F1087–F1108. [Google Scholar] [CrossRef] [Green Version]
- Bloomgarden, Z.; Handelsman, Y. How does CKD affect HbA1c? J. Diabetes 2018, 10, 270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonora, E.; Tuomilehto, J. The pros and cons of diagnosing diabetes with A1C. Diabetes Care 2011, 34 (Suppl. 2), S184–S190. [Google Scholar] [CrossRef] [Green Version]
- Perlman, R.L.; Finkelstein, F.O.; Liu, L.; Roys, E.; Kiser, M.; Eisele, G.; Burrows-Hudson, S.; Messana, J.M.; Levin, N.; Rajagopalan, S.; et al. Quality of life in chronic kidney disease (CKD): A cross-sectional analysis in the Renal Research Institute-CKD study. Am. J. Kidney Dis. 2005, 45, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Pagels, A.A.; Soderkvist, B.K.; Medin, C.; Hylander, B.; Heiwe, S. Health-Related quality of life in different stages of chronic kidney disease and at initiation of dialysis treatment. Health Qual. Life Outcomes 2012, 10, 71. [Google Scholar] [CrossRef] [Green Version]
- Venkateswaramurthy, N.; Islam, M.S.; Habeeba, R.C.; Sambathkumar, R. Assessment of quality of life in dialysis and non-dialysis chronic kidney disease patients. Int. J. Pharm. Sci. Res. 2019, 10, 2970–2974. [Google Scholar] [CrossRef]


{kind=link}
| Baseline (n = 35) | 3rd Month (n = 35) | p-Value ‡ | 6th Month (n = 35) | p-Value § | |
|---|---|---|---|---|---|
| Blood chemistry | |||||
| Albumin (g/dL) | 4.13 ± 0.31 (4.10) | 4.12 ± 0.32 (4.10) | 0.429 | 4.12 ± 0.32 (4.10) | 0.407 |
| Blood urea nitrogen (mg/dL) | 34.49 ± 12.58 (32.00) | 35.83 ± 11.80 (37.00) | 0.245 | 34.94 ± 12.67 (34.00) | 0.749 |
| Creatinine (mg/dL) | 2.34 ± 0.76 (2.20) | 2.45 ± 0.81 (2.30) | 0.037 * | 2.51 ± 0.96 (2.30) | 0.016 *,† |
| eGFR (ml/min/1.73 m2) | 27.77 ± 10.02 (28.00) | 26.40 ± 9.54 (25.00) | 0.044 * | 26.11 ± 9.97 (26.00) | 0.031 * |
| Nondiabetic group (n = 26) | 25.69 ± 10.12 (25.00) | 24.50 ± 9.73 (21.50) | 0.161 | 24.00 ± 9.84 (23.00) | 0.042 * |
| Diabetic group (n = 5) | 33.78 ± 7.24 (33.00) | 31.89 ± 6.75 (32.00) | 0.092 | 32.22 ± 7.98 (32.00) | 0.403 |
| Uric acid (mg/dL) | 6.52 ± 1.62 (6.20) | 6.39 ± 1.56 (6.30) | 0.277 | 6.50 ± 1.61 (6.30) | 0.931 |
| HbA1c (%) | 5.77 ± 0.75 (5.60) | 5.87 ± 0.70 (5.70) | 0.079 | 5.91 ± 0.78 (5.70) | 0.021 *,† |
| Glucose (mg/dL) | 103.46 ± 25.06 (99.00) | 100.54 ± 12.76 (102.00) | 0.627 † | 103.54 ± 24.68 (103.00) | 0.107 † |
| Insulin (µIU/mL) | 6.55 ± 4.61 (5.40) | 8.77 ± 10.20 (5.70) | 0.311 † | 8.63 ± 10.83 (6.00) | 0.119 † |
| HOMA-IR | 1.74 ± 1.46 (1.25) | 2.05 ± 2.32 (1.35) | 0.563 † | 2.51 ± 4.49 (1.61) | 0.023 *,† |
| Cholesterol (mg/dL) | 190.74 ± 36.20 (191.00) | 180.43 ± 40.93 (173.00) | 0.187 | 180.77 ± 48.69 (176.00) | 0.203 |
| Triglycerides (mg/dL) | 124.69 ± 55.65 (116.00) | 136.00 ± 77.36 (110.00) | 0.182 | 146.43 ± 99.64 (133.00) | 0.098 † |
| LDL (mg/dL) | 108.74 ± 28.46 (109.00) | 98.09 ± 30.68 (88.00) | 0.072 | 95.57 ± 36.37 (89.00) | 0.026 * |
| Sodium (mmol/L) | 140.77 ± 2.56 (141.00) | 140.54 ± 2.31 (141.00) | 0.481 | 140.29 ± 2.70 (141.00) | 0.155 |
| Potassium (mmol/L) | 4.38 ± 0.58 (4.30) | 4.43 ± 0.49 (4.40) | 0.382 | 4.42 ± 0.65 (4.40) | 0.583 |
| Calcium (mg/dL) | 9.26 ± 0.33 (9.20) | 9.21 ± 0.38 (9.20) | 0.362 | 9.18 ± 0.41 (9.20) | 0.205 |
| Phosphorus (mg/dL) | 3.85 ± 0.67 (3.70) | 3.84 ± 0.68 (3.70) | 0.943 | 3.95 ± 0.67 (4.00) | 0.148 |
| CRP (mg/L) | 1.13 ± 1.43 (0.50) | 2.22 ± 4.23 (0.50) | 0.099 | 2.12 ± 4.09 (0.50) | 0.166 † |
| Baseline (n = 35) | 3rd Month (n = 35) | p-Value ‡ | 6th Month (n = 35) | p-Value § | |
|---|---|---|---|---|---|
| Nutritional status and intakes | |||||
| Body weight (kg) | 61.67 ± 11.35 (63.30) | 62.76 ± 10.93 (64.75) | < 0.001 * | 62.98 ± 10.85 (65.00) | < 0.001 * |
| Body Mass Index (kg/m2) | 23.58 ± 3.43 (24.02) | 24.01 ± 3.27 (24.84) | < 0.001 * | 24.10 ± 3.26 (24.55) | < 0.001 * |
| Daily energy intake (kcal/d) | 1470.77 ± 330.69 (1486.67) | 1654.12 ± 251.59 (1630.00) | < 0.001 * | 1659.75 ± 245.40 (1595.67) | < 0.001 * |
| Total energy intake (kcal/kg/d) | 24.14 ± 5.11 (24.35) | 26.81 ± 4.68 (26.78) | < 0.001 * | 26.82 ± 4.79 (25.98) | < 0.001 * |
| Total protein intake (g/d) | 47.98 ± 12.81 (48.33) | 49.90 ± 11.64 (48.10) | 0.277 | 50.79 ± 11.63 (48.60) | 0.140 |
| Total protein intake (g/kg/d) | 0.78 ± 0.19 (0.81) | 0.80 ± 0.16 (0.80) | 0.612 | 0.81 ± 0.18 (0.77) | 0.358 |
| Body composition and handgrip strength | |||||
| Total body protein (kg) | 8.67 ± 1.54 (8.10) | 8.76 ± 2.01 (8.50) | 0.801 † | 8.76 ± 1.76 (8.55) | 0.379 † |
| Total body mineral (kg) | 2.95 ± 0.51 (2.88) | 2.98 ± 0.60 (2.87) | 0.230 † | 3.02 ± 0.52 (2.98) | 0.005 * |
| Skeletal muscle mass (kg) | 24.12 ± 4.65 (22.50) | 24.41 ± 6.02 (23.70) | 0.586 † | 24.99 ± 6.33 (23.80) | 0.216 † |
| Fat-free mass (%) | 62.19 ± 15.78 (64.30) | 60.24 ± 17.10 (61.60) | 0.682 † | 58.99 ± 17.64 (61.85) | 0.854 † |
| Total body fat mass (kg) | 16.93 ± 7.16 (17.70) | 17.58 ± 6.84 (17.10) | 0.070 † | 18.09 ± 6.56 (18.00) | 0.011 *,† |
| Body fat (%) | 27.47 ± 10.77 (28.10) | 28.71 ± 12.59 (26.60) | 0.175 † | 28.39 ± 11.10 (26.65) | 0.707 † |
| Handgrip strength (kg) | 26.97 ± 7.71 (27.50) | 27.54 ± 7.54 (27.32) | 0.038 * | 28.00 ± 7.87 (28.50) | 0.036 *,† |
| Baseline | 3rd Month | p-Value ‡ | 6th Month | p-Value § | p-Value ¶ | ||||
|---|---|---|---|---|---|---|---|---|---|
| Nondiabetic (n = 26) | Diabetic (n = 9) | Nondiabetic (n = 26) | Diabetic (n = 9) | Nondiabetic (n = 26) | Diabetic (n = 9) | ||||
| Glucose (mg/dL) | 99.42 ± 8.86 (99.50) | 115.11 ± 47.10 (96.00) | 99.27 ± 10.50 (101.50) | 104.22 ± 18.07 (110.00) | 0.408 | 96.46 ± 20.96 (102.00) | 124.00 ± 24.14 (120.00) | 0.820 | 0.012 * |
| HOMA-IR | 1.50 ± 1.13 (1.19) | 2.44 ± 2.10 (1.64) | 1.73 ± 1.40 (1.37) | 2.95 ± 3.89 (1.28) | 0.549 | 1.69 ± 1.23 (1.48) | 4.90 ± 8.49 (1.76) | 0.128 † | 0.092 |
| HbA1c (%) | 5.48 ± 0.23 (5.50) | 6.62 ± 1.08 (6.40) | 5.60 ± 0.30 (5.60) | 6.63 ± 0.94 (6.60) | 0.408 | 5.63 ± 0.42 (5.55) | 6.73 ± 1.02 (6.60) | 0.649 | 0.985 † |
| Insulin (µIU/mL) | 5.93 ± 4.10 (5.05) | 8.34 ± 5.73 (6.90) | 7.45 ± 5.77 (5.85) | 12.59 ± 17.78 (4.70) | 0.162 | 6.89 ± 4.49 (6.00) | 13.67 ± 19.92 (6.00) | 0.327 | 0.365 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kelly, O.J.; Huang, M.-C.; Liao, H.-Y.; Lin, C.-C.; Tung, T.-Y.; Cheng, R.W.-Y.; Wang, M.Y.-H.; Yalawar, M.; Hwang, S.-J. A Low-Protein Diet with a Renal-Specific Oral Nutrition Supplement Helps Maintain Nutritional Status in Patients with Advanced Chronic Kidney Disease. J. Pers. Med. 2021, 11, 1360. https://doi.org/10.3390/jpm11121360
Kelly OJ, Huang M-C, Liao H-Y, Lin C-C, Tung T-Y, Cheng RW-Y, Wang MY-H, Yalawar M, Hwang S-J. A Low-Protein Diet with a Renal-Specific Oral Nutrition Supplement Helps Maintain Nutritional Status in Patients with Advanced Chronic Kidney Disease. Journal of Personalized Medicine. 2021; 11(12):1360. https://doi.org/10.3390/jpm11121360
Chicago/Turabian StyleKelly, Owen J., Meng-Chuan Huang, Hsin-Yin Liao, Chih-Ching Lin, Tsui-Yin Tung, Rhoda Wen-Yi Cheng, Michael Yao-Hsien Wang, Menaka Yalawar, and Shang-Jyh Hwang. 2021. "A Low-Protein Diet with a Renal-Specific Oral Nutrition Supplement Helps Maintain Nutritional Status in Patients with Advanced Chronic Kidney Disease" Journal of Personalized Medicine 11, no. 12: 1360. https://doi.org/10.3390/jpm11121360