
Adjuvant Whole Breast Radiotherapy Improve Survival in Women with Heart Failure with Reduced Ejection Fraction Receiving Breast-Conserving Surgery

 , , and
, , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Inclusion and Exclusion Criteria
2.3. Study Covariates and Statistical Analysis
3. Results
3.1. Study Cohort
3.2. Effects of Adjuvant Whole Breast Radiotherapy (WBRT) on Oncologic Outcomes in Women with Left-Side Invasive Ductal Carcinoma (IDC) and Heart Failure with Reduced Ejection Fraction (HFrEF) Receiving Breast-Conserving Surgery (BCS)
3.3. Other Independent Predictors of All-Cause Death, Locoregional Recurrence (LRR), and Distant Metastasis (DM) in the Women with Left IDC and HFrEF Receiving BCS
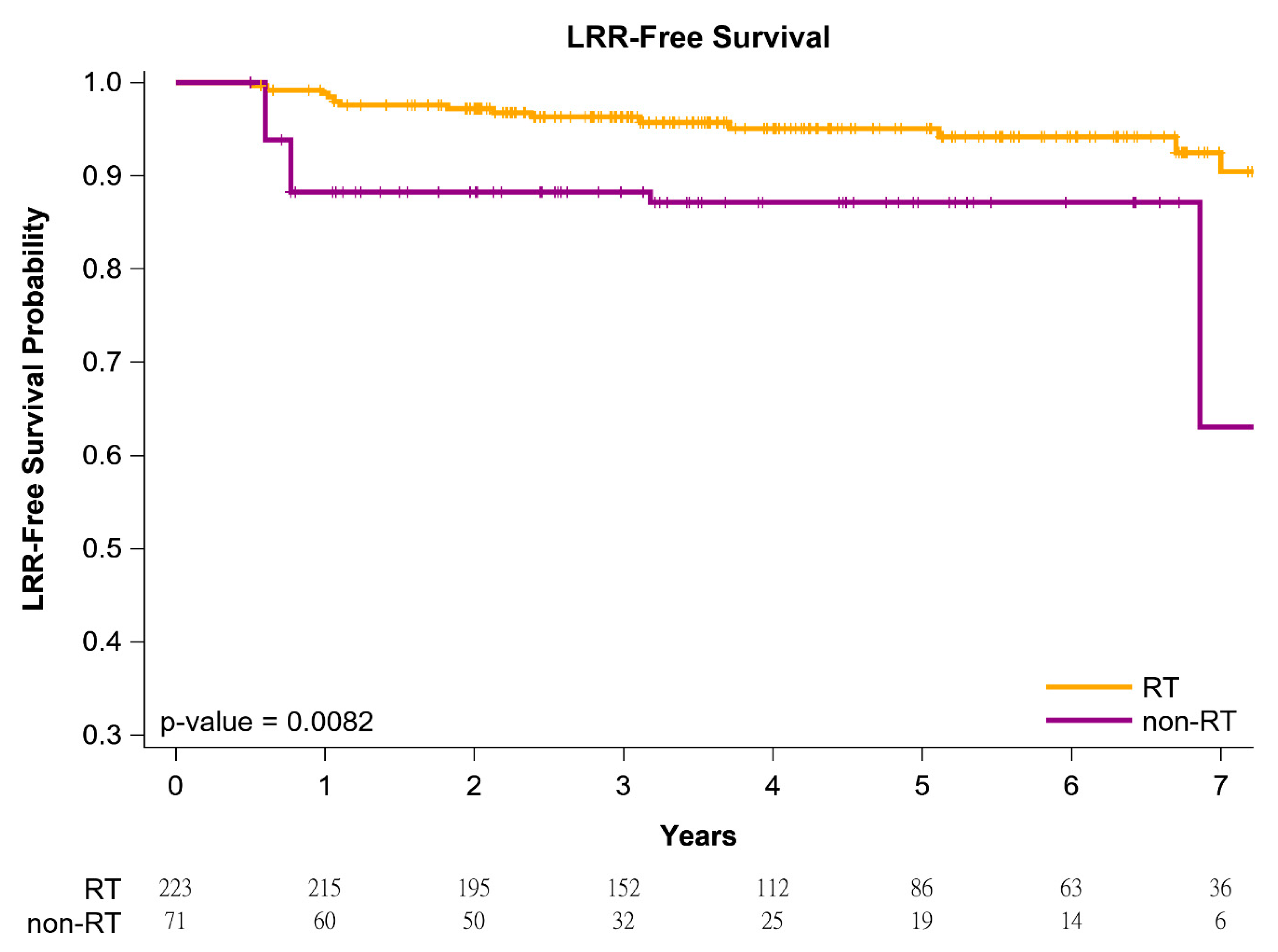
3.4. Survival Curves of Adjuvant WBRT or Non-Adjuvant WBRT in Women with Left IDC and HFrEF Receiving BCS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| WBRT | whole breast radiotherapy |
| LRR | locoregional recurrence |
| DM | distant metastasis |
| IDC | invasive ductal carcinoma |
| HFrEF | heart failure with reduced ejection fraction |
| BCS | breast-conserving surgery |
| OS | overall survival |
| aHR | adjusted hazard ratio |
| HR | hazard ratio |
| IPTW | inverse probability of treatment weighting |
| CI | confidence interval |
| AJCC | American Joint Committee on Cancer |
| TCRD | Taiwan Cancer Registry Database |
| SD | standard deviation |
| Her-2 | human epidermal growth factor receptor-2 |
| SLNB | sentinel lymph node biopsy |
| ALND | axillary lymph node dissection |
| CKD | chronic kidney disease |
| CCI | Charlson comorbidity index |
| ICD-10-CM | International Classification of Diseases, 10th Revision, Clinical Modification |
| NCCN | National Comprehensive Cancer Network |
| RT | radiotherapy |
| RICT | radiotherapy-related cardiotoxicity |
| TM | total mastectomy |
| HF | heart failure |
| LV | left ventricular |
| LVEF | left ventricular ejection fraction |
| T | tumor |
| N | nodal |
| pT | pathologic tumor stage |
| pN | pathologic nodal stage |
| NHIRD | National Health Insurance Research Database |
References
- Hooning, M.J.; Botma, A.; Aleman, B.M.; Baaijens, M.H.; Bartelink, H.; Klijn, J.G.; Taylor, C.W.; van Leeuwen, F.E. Long-term risk of cardiovascular disease in 10-year survivors of breast cancer. J. Natl. Cancer Inst. 2007, 99, 365–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, L.B.; Ng, A.K.; Allan, J.M.; Pui, C.H.; Kennedy, A.R.; Xu, X.G.; Purdy, J.A.; Applegate, K.; Yahalom, J.; Constine, L.S.; et al. Second malignant neoplasms and cardiovascular disease following radiotherapy. J. Natl. Cancer Inst. 2012, 104, 357–370. [Google Scholar] [CrossRef]
- Moslehi, J. The cardiovascular perils of cancer survivorship. N. Engl. J. Med. 2013, 368, 1055–1056. [Google Scholar] [CrossRef] [Green Version]
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Bronnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B.; et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paszat, L.F.; Mackillop, W.J.; Groome, P.A.; Schulze, K.; Holowaty, E. Mortality from myocardial infarction following postlumpectomy radiotherapy for breast cancer: A population-based study in Ontario, Canada. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 755–762. [Google Scholar] [CrossRef]
- Hojris, I.; Overgaard, M.; Christensen, J.J.; Overgaard, J. Morbidity and mortality of ischaemic heart disease in high-risk breast-cancer patients after adjuvant postmastectomy systemic treatment with or without radiotherapy: Analysis of DBCG 82b and 82c randomised trials. Radiotherapy Committee of the Danish Breast Cancer Cooperative Group. Lancet 1999, 354, 1425–1430. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013, 128, 1810–1852. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, C.Y.; Chen, C.H.; Chen, H.M.; Wu, S.Y. Effect of pathologic stages on postmastectomy radiation therapy in breast cancer receiving neoadjuvant chemotherapy and total mastectomy: A Cancer Database Analysis. Breast 2020, 54, 70–78. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, C.Y.; Qin, L.; Chen, H.M.; Wu, S.Y. Breast-conserving surgery with or without irradiation in women with invasive ductal carcinoma of the breast receiving preoperative systemic therapy: A cohort study. Breast 2020, 54, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, C.Y.; Chen, H.M.; Wu, S.Y. Neoadjuvant Chemotherapy or Endocrine Therapy for Invasive Ductal Carcinoma of the Breast With High Hormone Receptor Positivity and Human Epidermal Growth Factor Receptor 2 Negativity. JAMA Netw. Open 2021, 4, e211785. [Google Scholar] [CrossRef]
- Liu, W.C.; Liu, H.E.; Kao, Y.W.; Qin, L.; Lin, K.C.; Fang, C.Y.; Tsai, L.L.; Shia, B.C.; Wu, S.Y. Definitive radiotherapy or surgery for early oral squamous cell carcinoma in old and very old patients: A propensity-score-matched, nationwide, population-based cohort study. Radiother. Oncol. 2020, 151, 214–221. [Google Scholar] [CrossRef]
- The National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology. Available online: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp (accessed on 15 January 2021).
- Hammond, M.E.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American Society of Clinical Oncology/College Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J. Clin. Oncol. 2010, 28, 2784–2795. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Chen, J.H.; Yen, Y.C.; Yang, H.C.; Liu, S.H.; Yuan, S.P.; Wu, L.L.; Lee, F.P.; Lin, K.C.; Lai, M.T.; Wu, C.C.; et al. Curative-Intent Aggressive Treatment Improves Survival in Elderly Patients With Locally Advanced Head and Neck Squamous Cell Carcinoma and High Comorbidity Index. Medicine 2016, 95, e3268. [Google Scholar] [CrossRef]
- Lin, S.H.; Wang, L.; Myles, B.; Thall, P.F.; Hofstetter, W.L.; Swisher, S.G.; Ajani, J.A.; Cox, J.D.; Komaki, R.; Liao, Z. Propensity score-based comparison of long-term outcomes with 3-dimensional conformal radiotherapy vs intensity-modulated radiotherapy for esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 1078–1085. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group; Darby, S.; McGale, P.; Correa, C.; Taylor, C.; Arriagada, R.; Clarke, M.; Cutter, D.; Davies, C.; Ewertz, M.; et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet 2011, 378, 1707–1716. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.M.; Hsieh, M.C.; Qin, L.; Zhang, J.; Wu, S.Y. Metformin reduces radiation-induced cardiac toxicity risk in patients having breast cancer. Am. J. Cancer Res. 2019, 9, 1017–1026. [Google Scholar]
- Lee, C.H.; Zhang, J.F.; Yuan, K.S.; Wu, A.T.H.; Wu, S.Y. Risk of cardiotoxicity induced by adjuvant anthracycline-based chemotherapy and radiotherapy in young and old Asian women with breast cancer. Strahlenther. Onkol. 2019, 195, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Giordano, S.H.; Kuo, Y.F.; Freeman, J.L.; Buchholz, T.A.; Hortobagyi, G.N.; Goodwin, J.S. Risk of cardiac death after adjuvant radiotherapy for breast cancer. J. Natl. Cancer Inst. 2005, 97, 419–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darby, S.C.; McGale, P.; Taylor, C.W.; Peto, R. Long-term mortality from heart disease and lung cancer after radiotherapy for early breast cancer: Prospective cohort study of about 300,000 women in US SEER cancer registries. Lancet Oncol. 2005, 6, 557–565. [Google Scholar] [CrossRef]
- Patt, D.A.; Goodwin, J.S.; Kuo, Y.F.; Freeman, J.L.; Zhang, D.D.; Buchholz, T.A.; Hortobagyi, G.N.; Giordano, S.H. Cardiac morbidity of adjuvant radiotherapy for breast cancer. J. Clin. Oncol. 2005, 23, 7475–7482. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.W.; Bronnum, D.; Darby, S.C.; Gagliardi, G.; Hall, P.; Jensen, M.B.; McGale, P.; Nisbet, A.; Ewertz, M. Cardiac dose estimates from Danish and Swedish breast cancer radiotherapy during 1977–2001. Radiother. Oncol. 2011, 100, 176–183. [Google Scholar] [CrossRef] [Green Version]
- McGale, P.; Darby, S.C.; Hall, P.; Adolfsson, J.; Bengtsson, N.O.; Bennet, A.M.; Fornander, T.; Gigante, B.; Jensen, M.B.; Peto, R.; et al. Incidence of heart disease in 35,000 women treated with radiotherapy for breast cancer in Denmark and Sweden. Radiother. Oncol. 2011, 100, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Boekel, N.B.; Jacobse, J.N.; Schaapveld, M.; Hooning, M.J.; Gietema, J.A.; Duane, F.K.; Taylor, C.W.; Darby, S.C.; Hauptmann, M.; Seynaeve, C.M.; et al. Cardiovascular disease incidence after internal mammary chain irradiation and anthracycline-based chemotherapy for breast cancer. Br. J. Cancer 2018, 119, 408–418. [Google Scholar] [CrossRef] [Green Version]
- Early Breast Cancer Trialists’ Collaborative Group; Peto, R.; Davies, C.; Godwin, J.; Gray, R.; Pan, H.C.; Clarke, M.; Cutter, D.; Darby, S.; McGale, P.; et al. Comparisons between different polychemotherapy regimens for early breast cancer: Meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet 2012, 379, 432–444. [Google Scholar] [CrossRef] [Green Version]
- Blum, J.L.; Flynn, P.J.; Yothers, G.; Asmar, L.; Geyer, C.E., Jr.; Jacobs, S.A.; Robert, N.J.; Hopkins, J.O.; O’Shaughnessy, J.A.; Dang, C.T.; et al. Anthracyclines in Early Breast Cancer: The ABC Trials-USOR 06-090, NSABP B-46-I/USOR 07132, and NSABP B-49 (NRG Oncology). J. Clin. Oncol. 2017, 35, 2647–2655. [Google Scholar] [CrossRef] [PubMed]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Munoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef]
- Cardinale, D.; Colombo, A.; Bacchiani, G.; Tedeschi, I.; Meroni, C.A.; Veglia, F.; Civelli, M.; Lamantia, G.; Colombo, N.; Curigliano, G.; et al. Early detection of anthracycline cardiotoxicity and improvement with heart failure therapy. Circulation 2015, 131, 1981–1988. [Google Scholar] [CrossRef] [Green Version]
- Von Hoff, D.D.; Layard, M.W.; Basa, P.; Davis, H.L., Jr.; Von Hoff, A.L.; Rozencweig, M.; Muggia, F.M. Risk factors for doxorubicin-induced congestive heart failure. Ann. Intern. Med. 1979, 91, 710–717. [Google Scholar] [CrossRef]
- Swain, S.M.; Whaley, F.S.; Ewer, M.S. Congestive heart failure in patients treated with doxorubicin: A retrospective analysis of three trials. Cancer 2003, 97, 2869–2879. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.G.; McKenzie, W.B.; Alexander, J.; Sager, P.; D’Souza, A.; Manatunga, A.; Schwartz, P.E.; Berger, H.J.; Setaro, J.; Surkin, L.; et al. Congestive heart failure and left ventricular dysfunction complicating doxorubicin therapy. Seven-year experience using serial radionuclide angiocardiography. Am. J. Med. 1987, 82, 1109–1118. [Google Scholar] [CrossRef]
- Keefe, D.L. Trastuzumab-associated cardiotoxicity. Cancer 2002, 95, 1592–1600. [Google Scholar] [CrossRef]
- Perez, E.A.; Rodeheffer, R. Clinical cardiac tolerability of trastuzumab. J. Clin. Oncol. 2004, 22, 322–329. [Google Scholar] [CrossRef]
- Fiuza, M. Cardiotoxicity associated with trastuzumab treatment of HER2+ breast cancer. Adv. Ther. 2009, 26 (Suppl. 1), S9–S17. [Google Scholar] [CrossRef] [PubMed]
- Mehta, L.S.; Watson, K.E.; Barac, A.; Beckie, T.M.; Bittner, V.; Cruz-Flores, S.; Dent, S.; Kondapalli, L.; Ky, B.; Okwuosa, T.; et al. Cardiovascular Disease and Breast Cancer: Where These Entities Intersect: A Scientific Statement From the American Heart Association. Circulation 2018, 137, e30–e66. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L.; Weston, S.A.; Redfield, M.M.; Hellermann-Homan, J.P.; Killian, J.; Yawn, B.P.; Jacobsen, S.J. Trends in heart failure incidence and survival in a community-based population. JAMA 2004, 292, 344–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, L.; Jhund, P.S.; Petrie, M.C.; Claggett, B.L.; Barlera, S.; Cleland, J.G.F.; Dargie, H.J.; Granger, C.B.; Kjekshus, J.; Kober, L.; et al. Declining Risk of Sudden Death in Heart Failure. N. Engl. J. Med. 2017, 377, 41–51. [Google Scholar] [CrossRef]
- Yoo, S.; Lee, H.B.; Han, W.; Noh, D.Y.; Park, S.K.; Kim, W.H.; Kim, J.T. Total Intravenous Anesthesia versus Inhalation Anesthesia for Breast Cancer Surgery: A Retrospective Cohort Study. Anesthesiology 2019, 130, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.K.; Kim, H.H.; Jeon, Y.T. Retrospective analysis of 1-year mortality after gastric cancer surgery: Total intravenous anesthesia versus volatile anesthesia. Acta Anaesthesiol. Scand. 2019, 63, 1169–1177. [Google Scholar] [CrossRef]
- Lee, J.H.; Kang, S.H.; Kim, Y.; Kim, H.A.; Kim, B.S. Effects of propofol-based total intravenous anesthesia on recurrence and overall survival in patients after modified radical mastectomy: A retrospective study. Korean J. Anesth. 2016, 69, 126–132. [Google Scholar] [CrossRef]
- Enlund, M.; Berglund, A.; Ahlstrand, R.; Wallden, J.; Lundberg, J.; Warnberg, F.; Ekman, A.; Sjoblom Widfeldt, N.; Enlund, A.; Bergkvist, L. Survival after primary breast cancer surgery following propofol or sevoflurane general anesthesia-A retrospective, multicenter, database analysis of 6305 Swedish patients. Acta Anaesthesiol. Scand. 2020, 64, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Makito, K.; Matsui, H.; Fushimi, K.; Yasunaga, H. Volatile versus Total Intravenous Anesthesia for Cancer Prognosis in Patients Having Digestive Cancer Surgery. Anesthesiology 2020, 133, 764–773. [Google Scholar] [CrossRef]
- Groenning, B.A.; Nilsson, J.C.; Sondergaard, L.; Pedersen, F.; Trawinski, J.; Baumann, M.; Larsson, H.B.; Hildebrandt, P.R. Detection of left ventricular enlargement and impaired systolic function with plasma N-terminal pro brain natriuretic peptide concentrations. Am. Hear. J. 2002, 143, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.L.; Lee, C.H.; Chen, P.S.; Li, Y.H.; Lin, S.J.; Yang, Y.H. Validation of acute myocardial infarction cases in the national health insurance research database in taiwan. J. Epidemiol. 2014, 24, 500–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, C.L.; Kao, Y.H.; Lin, S.J.; Lee, C.H.; Lai, M.L. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol. Drug Saf. 2011, 20, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.C.; Lai, M.S.; Syu, C.Y.; Chang, S.C.; Tseng, F.Y. Accuracy of diabetes diagnosis in health insurance claims data in Taiwan. J. Formos. Med. Assoc. 2005, 104, 157–163. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Propensity Score–Weighted Population | ||||||
|---|---|---|---|---|---|---|
| Adjuvant WBRT N = 223 | Non-Adjuvant WBRT N = 71 | |||||
| Variable | n | (%) | n | (%) | Standardized Difference | |
| Age | Mean (SD) | 62.3 | (11.4) | 63.5 | (11.6) | 0.0311 |
| Median (IQR, Q1–Q3) | 63 | (54–70) | 63 | (54–71) | ||
| 20–65 | 167 | (73.6) | 52 | (73.2) | 0.0224 | |
| >65 | 60 | (26.4) | 19 | (26.8) | ||
| Diagnosis year | 2008–2012 | 89 | (39.2) | 28 | (39.4) | 0.0000 |
| 2013–2017 | 138 | (60.8) | 43 | (60.6) | ||
| CCI score | 0 | 73 | (32.7) | 22 | (31.0) | 0.0231 |
| ≥1 | 150 | (67.3) | 49 | (69.0) | ||
| Differentiation | I | 44 | (19.7) | 16 | (22.5) | - |
| II | 112 | (50.2) | 34 | (47.9) | 0.0566 | |
| III | 67 | (30.0) | 21 | (29.6) | 0.0452 | |
| AJCC clinical stage | I | 112 | (50.2) | 33 | (46.5) | 0.0831 |
| II–III | 111 | (49.8) | 38 | (53.5) | ||
| AJCC pathologic stage | I | 109 | (48.9) | 34 | (47.9) | - |
| II | 97 | (43.5) | 32 | (45.1) | 0.0242 | |
| III | 18 | (8.1) | 6 | (8.5) | 0.0170 | |
| pT | pT1 | 137 | (61.4) | 41 | (57.7) | 0.0737 |
| pT2–4 | 86 | (38.6) | 30 | (42.3) | ||
| pN | pN0 | 164 | (73.5) | 49 | (69.0) | 0.0705 |
| pN1–3 | 59 | (26.5) | 22 | (31.0) | ||
| Hypertension | 161 | (72.2) | 50 | (70.4) | 0.0584 | |
| Hyperlipidemia | 98 | (43.9) | 34 | (47.9) | 0.0871 | |
| CKD | 67 | (30.0) | 32 | (45.1) | 0.0171 | |
| Coronary arterial diseases | 88 | (39.5) | 27 | (38.0) | 0.0352 | |
| One-vessel stenosis | 60 | (26.9) | 18 | (25.4) | ||
| Two-vessel stenosis | 28 | (12.6) | 9 | (12.7) | ||
| Valvular disease | 17 | (7.6) | 6 | (8.5) | 0.0276 | |
| Aortic stenosis/regurgitation | 10 | (4.5) | 3 | (4.2) | ||
| Mitral stenosis/regurgitation | 7 | (3.1) | 3 | (4.2) | ||
| Atrial fibrillation | 60 | 26.9 | 19 | 26.8 | 0.0592 | |
| Cardiomyopathy | 71 | (31.8) | 23 | (32.4) | 0.0381 | |
| Ventricular arrhythmias | 6 | (2.7) | 2 | (2.8) | 0.0114 | |
| Diabetes mellitus | 76 | (34.1) | 27 | (38.0) | 0.0779 | |
| Statins | 58 | (26.0) | 20 | (28.2) | 0.0923 | |
| Antithrombotic therapy | 78 | (35.0) | 28 | (39.4) | 0.0610 | |
| Diuretic | 89 | (39.9) | 29 | (40.8) | 0.0276 | |
| Beta blockers | 133 | (59.6) | 46 | (64.8) | 0.0110 | |
| Renin-angiotensin system inhibitor | 166 | (74.4) | 51 | (71.8) | 0.0853 | |
| Chemotherapy with anthracycline | 103 | (46.2) | 34 | (47.9) | 0.0072 | |
| Hormone receptor positive | 109 | (48.9) | 35 | (49.3) | 0.0089 | |
| Trastuzumab use | 21 | (9.3) | 7 | (9.9) | 0.0131 | |
| Nodal surgery | ALND | 139 | (61.2) | 40 | (56.3) | 0.0618 |
| SLNB | 84 | (38.8) | 31 | (43.7) | ||
| Hospital level | Academic center | 110 | (49.3) | 35 | (49.3) | 0.0000 |
| Non-academic center | 113 | (50.7) | 36 | (50.7) | ||
| Income | <NTD 18,000 | 65 | (29.1) | 20 | (28.2) | - |
| NTD 18,000–24,000 | 74 | (33.2) | 23 | (32.4) | 0.0231 | |
| NTD 24,000–36,000 | 40 | (17.9) | 12 | (16.9) | 0.0143 | |
| >NTD 36,000 | 44 | (19.7) | 16 | (22.5) | 0.0712 | |
| All-Cause Death | Local Recurrence | Distant Metastasis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| aHR * | (95% CI) | p Value | aHR * | (95% CI) | p Value | aHR * | (95% CI) | p Value | ||
| Adjuvant WBRT | No | Ref | 0.0424 | Ref | 0.0017 | Ref | 0.0004 | |||
| Yes | 0.60 | (0.44–0.94) | 0.33 | (0.24–0.71) | 0.37 | (0.22–0.63) | ||||
| Age | 20–65 | Ref | 0.0001 | Ref | 0.5641 | Ref | 0.5028 | |||
| >65 | 1.31 | (1.12–3.01) | 1.09 | (0.71–1.74) | 1.49 | (0.72–1.79) | ||||
| Diagnosis year | 2009–2012 | Ref | 0.4796. | Ref | 0.2554 | Ref | 0.7472 | |||
| 2013–2017 | 0.83 | (0.76–1.38) | 0.75 | (0.53–1.11) | 0.91 | (0.63–1.58) | ||||
| CCI score | 0 | Ref | 0.0385 | Ref | 0.5028 | Ref | 0.7631 | |||
| ≥1 | 1.15 | (1.09–1.66) | 1.03 | (0.70–1.68) | 1.02 | (0.57–1.55) | ||||
| Hypertension | Yes | 1.15 | (0.70–1.88) | 0.5482 | 0.93 | (0.61–1.43) | 0.8204 | 0.95 | (0.69–1.33) | 0.8861 |
| Hyperlipidemia | Yes | 1.06 | (0.66–2.01) | 0.6431 | 0.94 | (0.61–1.61) | 0.8421 | 0.92 | (0.65–1.61) | 0.8141 |
| CKD | Yes | 1.17 | (0.88–1.76) | 0.5157 | 0.88 | (0.70–1.81) | 0.7315 | 0.82 | (0.59–1.39) | 0.6929 |
| Coronary arterial diseases | No | Ref | 0.3868 | Ref | 0.5628 | Ref | 0.5806 | |||
| One-vessel stenosis | 1.26 | (0.77–1.98) | 0.81 | (0.52–1.19) | 0.88 | (0.71–1.44) | ||||
| Two-vessel stenosis | 1.36 | (0.80–2.33) | 0.77 | (0.50–1.23) | 0.87 | (0.78–1.57) | ||||
| Valvular disease | No | Ref | 0.3598 | Ref | 0.6724. | Ref | 0.6682 | |||
| Aortic stenosis/regurgitation | 1.16 | (0.76–2.18) | 0.98 | (0.61–1.41) | 0.96 | (0.54–1.77) | 0.7963 | |||
| Mitral stenosis/regurgitation | 1.17 | (0.74–2.10) | 0.94 | (0.59–1.33) | 0.95 | (0.50–1.91) | 0.8190 | |||
| Atrial fibrillation | Yes | 1.08 | (0.76–1.40) | 0.3200 | 0.79 | (0.49–1.80) | 0.4219 | 0.90 | (0.67–2.50) | 0.5893 |
| Cardiomyopathy | Yes | 1.13 | (0.88–1.65) | 0.1312 | 0.77 | (0.45–1.82) | 0.3404 | 0.92 | (0.63–2.57) | 0.5322 |
| Ventricular arrhythmias | Yes | 1.08 | (0.88–1.46) | 0.1786 | 0.89 | (0.53–2.67) | 0.2762 | 0.76 | (0.41–1.39) | 0.3174 |
| Diabetes | Yes | 1.06 | (0.84–1.14) | 0.3127 | 0.91 | (0.67–1.20) | 0.4714 | 0.68 | (0.52–1.28) | 0.8784 |
| Statins | Yes | 0.91 | (0.70–1.65) | 0.4387 | 0.94 | (0.55–1.76) | 0.5494 | 0.90 | (0.54–1.91) | 0.5499 |
| Antithrombotic therapy | Yes | 1.03 | (0.77–1.51) | 0.2609 | 0.97 | (0.60–2.11) | 0.4980 | 0.88 | (0.51–1.90) | 0.4251 |
| Diuretic | Yes | 1.01 | (0.60–2.60) | 0.4427 | 0.95 | (0.58–2.29) | 0.5068 | 0.89 | (0.53–2.42) | 0.5778 |
| Beta blockers | Yes | 0.88 | (0.68–1.43) | 0.2080 | 0.90 | (0.50–2.99) | 0.4050 | 0.86 | (0.44–1.84) | 0.3160 |
| Renin-angiotensin system inhibitor | Yes | 0.86 | (0.54–1.97) | 0.5810 | 0.96 | (0.86–2.36) | 0.4169 | 0.87 | (0.57–1.81) | 0.5308 |
| pT | pT1 | Ref | 0.0217 | Ref | 0.0316 | Ref | 0.0245 | |||
| pT2–4 | 1.28 | (1.05–2.28) | 1.69 | (1.03–2.73) | 1.41 | (1.18–3.17) | ||||
| pN | pN0 | Ref | 0.0017 | Ref | 0.0072 | Ref | 0.0153 | |||
| pN1–3 | 2.31 | (1.30–4.24) | 1.72 | (1.35–4.30) | 1.66 | (1.24–2.69) | ||||
| Differentiation | I | Ref | 0.0003 | Ref | 0.0001 | Ref | 0.0001 | |||
| II | 1.44 | (1.10–2.00) | 1.86 | (1.43–2.18) | 1.82 | (1.39–2.79) | ||||
| III | 1.71 | (1.24–2.13) | 1.91 | (1.44–2.56) | 1.96 | (1.51–2.67) | ||||
| Chemotherapy with anthracycline | Yes | 0.97 | (0.35–1.54) | 0.2653 | 0.80 | (0.39–1.81) | 0.2876 | 0.82 | (0.60–1.77) | 0.4876 |
| Hormone receptor positive | Yes | 0.70 | (0.50–0.89) | 0.0085 | 0.68 | (0.51–0.88) | 0.0028 | 0.61 | (0.38–0.74) | 0.0016 |
| Trastuzumab use | Yes | 1.05 | (0.48–2.50) | 0.8893 | 1.60 | (0.71–3.70) | 0.8974 | 1.08 | (0.70–1.88) | 0.6432 |
| Nodal surgery | ALND | Ref | 0.8742 | Ref | 0.3682 | Ref | 0.3531 | |||
| SLNB | 1.12 | (0.93–1.24) | 1.25 | (0.81–2.25) | 1.37 | (0.71–2.78) | ||||
| Hospital level | Medical centers | Ref | 0.1667 | Ref | 0.4539 | Ref | 0.7830 | |||
| Non-medical centers | 1.09 | (0.80–1.25) | 0.91 | (0.60–2.55) | 0.95 | (0.70–1.50) | ||||
| Income | <NTD 18,000 | Ref | 0.4267 | Ref | 0.8541 | Ref | 0.7652 | |||
| NTD 18,000–24,000 | 1.31 | (0.60–2.94) | 1.21 | (0.68–2.16) | 1.14 | (0.65–1.98) | ||||
| NTD 24,000–36,000 | 1.51 | (0.85–2.67) | 1.38 | (0.71–2.47) | 1.51 | (0.76–2.19) | ||||
| >NTD 36,000 | 1.66 | (0.90–3.00) | 1.71 | (0.92–2.98) | 2.11 | (0.81–3.22) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Sum, S.-Y.; Hsu, J.-G.; Chiang, M.-F.; Lee, T.-S.; Wu, S.-Y. Adjuvant Whole Breast Radiotherapy Improve Survival in Women with Heart Failure with Reduced Ejection Fraction Receiving Breast-Conserving Surgery. J. Pers. Med. 2021, 11, 1358. https://doi.org/10.3390/jpm11121358
Zhang J, Sum S-Y, Hsu J-G, Chiang M-F, Lee T-S, Wu S-Y. Adjuvant Whole Breast Radiotherapy Improve Survival in Women with Heart Failure with Reduced Ejection Fraction Receiving Breast-Conserving Surgery. Journal of Personalized Medicine. 2021; 11(12):1358. https://doi.org/10.3390/jpm11121358
Chicago/Turabian StyleZhang, Jiaqiang, Shao-Yin Sum, Jeng-Guan Hsu, Ming-Feng Chiang, Tian-Shyug Lee, and Szu-Yuan Wu. 2021. "Adjuvant Whole Breast Radiotherapy Improve Survival in Women with Heart Failure with Reduced Ejection Fraction Receiving Breast-Conserving Surgery" Journal of Personalized Medicine 11, no. 12: 1358. https://doi.org/10.3390/jpm11121358