
The Contribution of Pharmacogenetic Drug Interactions to 90-Day Hospital Readmissions: Preliminary Results from a Real-World Healthcare System

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
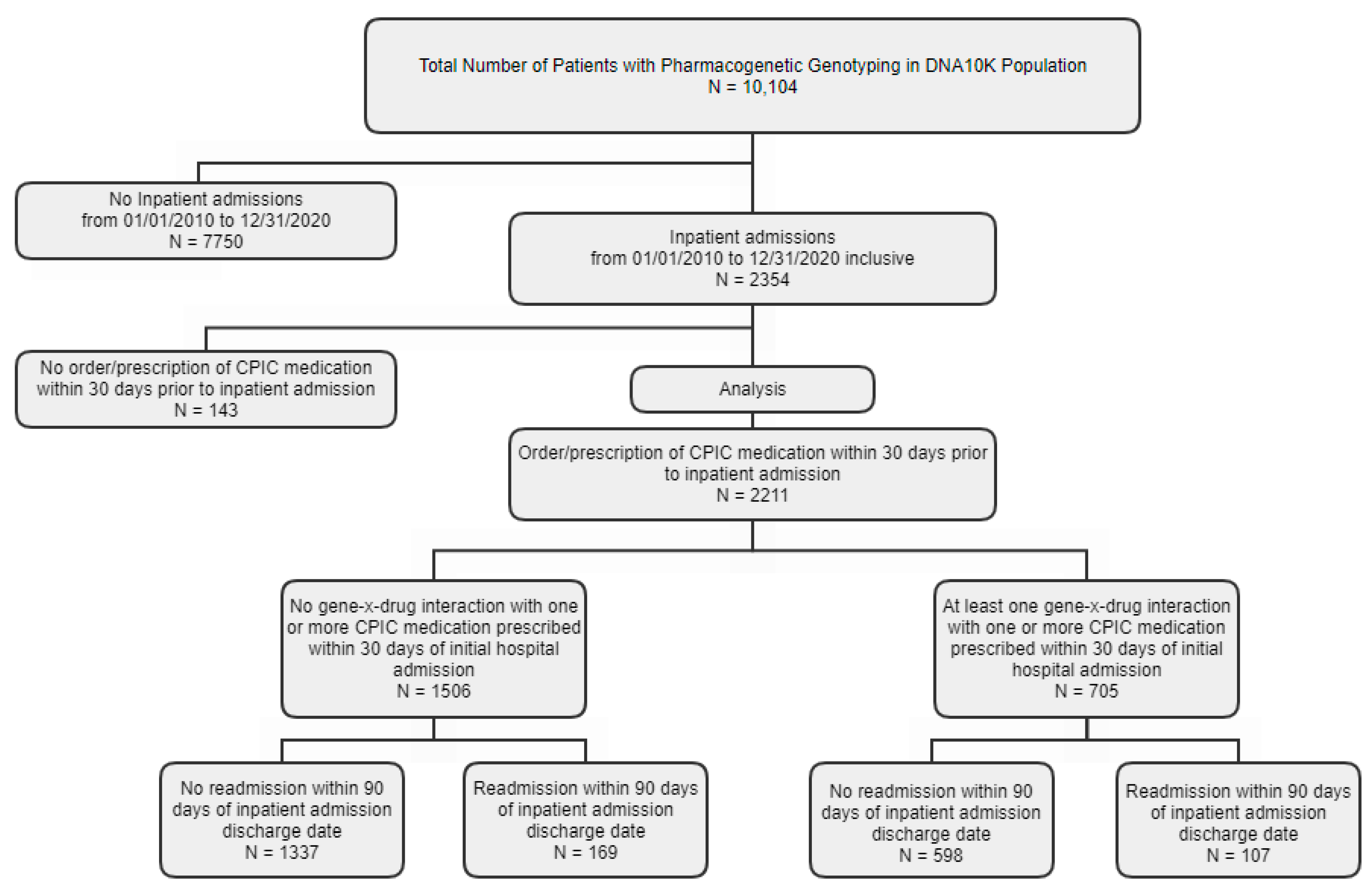
2.1. Patient Population
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zuckerman, R.B.; Sheingold, S.H.; Orav, E.J.; Ruhter, J.; Epstein, A.M. Readmissions, Observation, and the Hospital Readmissions Reduction Program. N. Engl. J. Med. 2016, 374, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Wadhera, R.K.; Yeh, R.W.; Joynt Maddox, K.E. The Hospital Readmissions Reduction Program—Time for a Reboot. N. Engl. J. Med. 2019, 380, 2289–2291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Morabet, N.; Uitvlugt, E.B.; van den Bemt, B.J.F.; van den Bemt, P.; Janssen, M.J.A.; Karapinar-Carkit, F. Prevalence and Preventability of Drug-Related Hospital Readmissions: A Systematic Review. J. Am. Geriatr. Soc. 2018, 66, 602–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caudle, K.E.; Klein, T.E.; Hoffman, J.M.; Muller, D.J.; Whirl-Carrillo, M.; Gong, L.; McDonagh, E.M.; Sangkuhl, K.; Thorn, C.F.; Schwab, M.; et al. Incorporation of pharmacogenomics into routine clinical practice: The Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline development process. Curr. Drug Metab. 2014, 15, 209–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, P.Y.; Ryu, E.; Pathak, J.; Jenkins, G.D.; Batzler, A.; Hathcock, M.A.; Black, J.L.; Olson, J.E.; Cerhan, J.R.; Bielinski, S.J. Increased risk of hospitalization for ultrarapid metabolizers of cytochrome P450 2D6. Pharmgenom. Pers. Med. 2017, 10, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, P.Y.; Ryu, E.; Bielinski, S.J.; Hathcock, M.; Jenkins, G.D.; Cerhan, J.R.; Olson, J.E. No Association between Pharmacogenomics Variants and Hospital and Emergency Department Utilization: A Mayo Clinic Biobank Retrospective Study. Pharmgenom. Pers. Med. 2021, 14, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Weitzel, K.W.; Alexander, M.; Bernhardt, B.A.; Calman, N.; Carey, D.J.; Cavallari, L.H.; Field, J.R.; Hauser, D.; Junkins, H.A.; Levin, P.A.; et al. The IGNITE network: A model for genomic medicine implementation and research. BMC Med. Genom. 2016, 9, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavallari, L.H.; Lee, C.R.; Beitelshees, A.L.; Cooper-DeHoff, R.M.; Duarte, J.D.; Voora, D.; Kimmel, S.E.; McDonough, C.W.; Gong, Y.; Dave, C.V.; et al. Multisite Investigation of Outcomes with Implementation of CYP2C19 Genotype-Guided Antiplatelet Therapy after Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2018, 11, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, O.; Kuivaniemi, H.; Tromp, G.; Faucett, W.A.; Li, R.; Manolio, T.A.; Sanderson, S.C.; Kannry, J.; Zinberg, R.; Basford, M.A.; et al. The Electronic Medical Records and Genomics (eMERGE) Network: Past, present, and future. Genet. Med. 2013, 15, 761–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen-Torvik, L.J.; Stallings, S.C.; Gordon, A.S.; Almoguera, B.; Basford, M.A.; Bielinski, S.J.; Brautbar, A.; Brilliant, M.H.; Carrell, D.S.; Connolly, J.J.; et al. Design and anticipated outcomes of the eMERGE-PGx project: A multicenter pilot for preemptive pharmacogenomics in electronic health record systems. Clin. Pharmacol. Ther. 2014, 96, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Leary, E.; Brilliant, M.; Peissig, P.; Griesbach, S. Preliminary outcomes of preemptive warfarin pharmacogenetic testing at a large rural healthcare center. Am. J. Health Syst. Pharm. 2019, 76, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Brixner, D.; Biltaji, E.; Bress, A.; Unni, S.; Ye, X.; Mamiya, T.; Ashcraft, K.; Biskupiak, J. The effect of pharmacogenetic profiling with a clinical decision support tool on healthcare resource utilization and estimated costs in the elderly exposed to polypharmacy. J. Med. Econ. 2016, 19, 213–228. [Google Scholar] [CrossRef] [PubMed]
- Callegari, C.; Isella, C.; Caselli, I.; Poloni, N.; Ielmini, M. Pharmacogenetic Tests in Reducing Accesses to Emergency Services and Days of Hospitalization in Bipolar Disorder: A 2-Year Mirror Analysis. J. Pers. Med. 2019, 9, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, L.S.; Henderson, J.C.; Neradilek, M.B.; Moyer, N.A.; Ashcraft, K.C.; Thirumaran, R.K. Clinical impact of pharmacogenetic profiling with a clinical decision support tool in polypharmacy home health patients: A prospective pilot randomized controlled trial. PLoS ONE 2017, 12, e0170905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christian, C.; Borden, B.A.; Danahey, K.; Yeo, K.T.J.; van Wijk, X.M.; Ratain, M.J.; O’Donnell, P.H. Pharmacogenomic-Based Decision Support to Predict Adherence to Medications. Clin. Pharmacol. Ther. 2020, 108, 368–376. [Google Scholar] [CrossRef] [PubMed]
- David, S.P.; Dunnenberger, H.M.; Ali, R.; Matsil, A.; Lemke, A.A.; Singh, L.; Zimmer, A.; Hulick, P.J. Implementing Primary Care Mediated Population Genetic Screening within an Integrated Health System. J. Am. Board Fam. Med. 2021, 34, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.L.; Chung, W.K.; Fedotov, A.; Kiryluk, K.; Weng, C.; Connolly, J.J.; Harr, M.; Hakonarson, H.; Leppig, K.A.; Larson, E.B.; et al. Harmonizing Outcomes for Genomic Medicine: Comparison of eMERGE Outcomes to ClinGen Outcome/Intervention Pairs. Healthcare 2018, 6, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helseth, D.L., Jr.; Gulukota, K.; Miller, N.; Yang, M.; Werth, T.; Sabatini, L.M.; Bouma, M.; Dunnenberger, H.M.; Wake, D.T.; Hulick, P.J.; et al. Flype: Software for enabling personalized medicine. Am. J. Med. Genet. C Semin. Med. Genet. 2021, 187, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Hicks, J.K.; Dunnenberger, H.M.; Gumpper, K.F.; Haidar, C.E.; Hoffman, J.M. Integrating pharmacogenomics into electronic health records with clinical decision support. Am. J. Health Syst. Pharm. 2016, 73, 1967–1976. [Google Scholar] [CrossRef] [PubMed]
- Kalinin, A.A.; Higgins, G.A.; Reamaroon, N.; Soroushmehr, S.; Allyn-Feuer, A.; Dinov, I.D.; Najarian, K.; Athey, B.D. Deep learning in pharmacogenomics: From gene regulation to patient stratification. Pharmacogenomics 2018, 19, 629–650. [Google Scholar] [CrossRef]


{kind=link}
| Inpatient Admissions 2010–2020 a | |||||||
|---|---|---|---|---|---|---|---|
| Overall 10,104 (100) | No 7750 (76.7) | Yes 2354 (23.3) | 90-Day Hospital Readmission b | ||||
| N = 2354 | |||||||
| No 2073 (88.1) | Yes 281 (11.9) | ||||||
| Age, median (IQR) | 50 (39–60) | 50 (40–60) | 48 (38–63) | 47 (37–62) | 59 (44–67) | * | |
| BMI, median (IQR) | 26.7 (23.6–31.1) | 26.6 (23.5–30.8) | 27.5 (23.8–32.1) | * | 27.3 (32.7–31.9) | 28.4 (24.5–33.3) | * |
| Sex | * | * | |||||
| Female | 6684 (66.2) | 4870 (62.8) | 1,814 (77.1) | 1622 (78.2) | 192 (68.3) | ||
| Male | 3420 (33.8) | 2880 (37.2) | 540 (22.9) | 451 (21.8) | 89 (31.7) | ||
| Race | * | * | |||||
| White | 6845 (67.7) | 5117 (66) | 1728 (73.4) | 1510 (72.8) | 218 (77.6) | ||
| Black or African American | 304 (3) | 201 (2.6) | 103 (4.4) | 80 (3.9) | 23 (8.2) | ||
| Asian | 746 (7.4) | 586 (7.6) | 160 (6.8) | 151 (7.3) | 9 (3.2) | ||
| American Indian or Alaska Native | 23 (0.2) | 19 (0.2) | 4 (0.2) | 4 (0.2) | 0 (0) | ||
| Pacific Islander/Hawaiian Native | 3 (0) | 3 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Other | 2,084 (20.6) | 1737 (22.4) | 347 (14.7) | 318 (15.3) | 29 (10.3) | ||
| Declined/Unknown | 99 (1) | 87 (1.1) | 12 (0.5) | 10 (0.5) | 2 (0.7) | ||
| Ethnicity | * | ||||||
| Hispanic/Latino | 497 (4.9) | 374 (4.8) | 123 (5.2) | 112 (5.4) | 11 (3.9) | ||
| Non-Hispanic | 9480 (93.8) | 7259 (93.7) | 2221 (94.4) | 1952 (94.2) | 269 (95.7) | ||
| Declined/Unknown | 127 (1.3) | 117 (1.5) | 10 (0.4) | 9 (0.4) | 1 (0.4) | ||
| Current Patient Status | * | * | |||||
| Alive | 10,083 (99.8) | 7743 (99.9) | 2340 (99.4) | 2067 (99.7) | 273 (97.2) | ||
| Deceased | 21 (0.2) | 7 (0.1) | 14 (0.6) | 6 (0.3) | 8 (2.8) | ||
| Marital Status | * | * | |||||
| Unmarried | 2823 (27.9) | 2232 (28.8) | 591 (25.1) | 492 (23.7) | 99 (35.2) | ||
| Married | 7198 (71.2) | 5439 (70.2) | 1759 (74.7) | 1577 (76.1) | 182 (64.8) | ||
| Unknown | 83 (0.8) | 79 (1) | 4 (0.2) | 4 (0.2) | 0 (0) | ||
| Employee Status | * | * | |||||
| Unemployed | 2899 (28.7) | 2059 (26.6) | 840 (35.7) | 697 (33.6) | 143 (50.9) | ||
| Employed | 6897 (68.3) | 5443 (70.2) | 1454 (61.8) | 1323 (63.8) | 131 (46.6) | ||
| Unknown | 308 (3) | 248 (3.2) | 60 (2.5) | 53 (2.6) | 7 (2.5) | ||
| Smoking Status | |||||||
| No | 9751 (96.5) | 7467 (96.3) | 2284 (97) | 2015 (97.2) | 269 (95.7) | ||
| Yes | 353 (3.5) | 283 (3.7) | 70 (3) | 58 (2.8) | 12 (4.3) | ||
| COVID Status | |||||||
| Yes | 52 (0.5) | 39 (0.5) | 13 (0.6) | 12 (0.6) | 1 (0.4) | ||
| Comorbidities | |||||||
| Cancer | 101 (1) | 44 (0.6) | 57 (2.4) | * | 41 (2) | 16 (5.7) | * |
| COPD | 98 (1) | 44 (0.6) | 54 (2.3) | * | 40 (1.9) | 14 (5) | * |
| Diabetes | 671 (6.6) | 442 (5.7) | 229 (9.7) | * | 182 (8.8) | 47 (16.7) | * |
| History of Diabetes | 740 (7.3) | 479 (6.2) | 261 (11.1) | * | 207 (10) | 54 (19.2) | * |
| Myocardial Infarction | 50 (0.5) | 17 (0.2) | 33 (1.4) | * | 26 (1.3) | 7 (2.5) | |
| Heart Failure | 93 (0.9) | 37 (0.5) | 56 (2.4) | * | 36 (1.7) | 20 (7.1) | * |
| Hypertension | 2074 (20.5) | 1463 (18.9) | 611 (26) | * | 491 (23.7) | 120 (42.7) | * |
| PVD | 83 (0.8) | 35 (0.5) | 48 (2) | * | 35 (1.7) | 13 (4.6) | * |
| Asthma | 940 (9.3) | 655 (8.5) | 285 (12.1) | * | 237 (11.4) | 48 (17.1) | * |
| CVA | 239 (2.4) | 115 (1.5) | 124 (5.3) | * | 91 (4.4) | 33 (11.7) | * |
| CPIC medication order/admin within 30 days prior to admission date in electronic medical record between 12/01/2009 and 12/31/2020 inclusive (N = 2211) | 1935/2211 (87.5) | 276/2211 (12.5) | |||||
| Drug interactions with orders in med Orders/Admin within 30 days prior to inpatient admission | * | ||||||
| Absent | 1337 (69.1) | 169 (61.2) | |||||
| Present | 598 (30.9) | 107 (38.8) | |||||
| Univariate Regression | Multivariable Regression Using Stepwise Selection Method | |||
|---|---|---|---|---|
| uOR (95% CI) | p-Value | aOR (95% CI) | p-Value | |
| Drug Interactions with Orders in Medication Orders/Administration within 30 Days Prior to Inpatient Admission Inclusive | ||||
| No | Reference | 0.01 | Reference | 0.04 |
| Yes | 1.42 (1.09–1.84) | 1.32 (1.01–1.73) | ||
| Age (continuous, range 17–90) | 1.03 (1.02–1.04) | <0.0001 | 1.02 (1.01–1.03) | 0.0003 |
| Sex | ||||
| Female | Reference | - | - | |
| Male | 1.76 (1.34–2.33) | <0.0001 | - | - |
| Race | ||||
| Caucasian | Reference | Reference | ||
| Black or African American | 1.98 (1.20–3.25) | 0.005 | 1.84 (1.09–3.11) | 0.09 |
| Asian | 0.43 (0.21–0.85) | 0.01 | 0.57 (0.28–1.14) | 0.03 |
| Other * | 0.60 (0.40–0.91) | 0.06 | 0.75 (0.49–1.14) | 0.07 |
| Declined/Unknown | 1.46 (0.31–6.79) | 0.49 | 2.73 (0.58–12.99) | 0.18 |
| Ethnicity | ||||
| Non-Hispanic | Reference | - | - | |
| Hispanic/Latino | 0.72 (0.38–1.35) | 0.67 | - | - |
| Declined/Unknown | 0.86 (0.11–6.92) | 0.99 | - | - |
| Most recent BMI ≤ 30 | ||||
| Yes | Reference | - | - | |
| No | 1.30 (1.00–1.68) | 0.05 | - | - |
| Marital Status | ||||
| Unmarried | Reference | - | - | |
| Married | 0.57 (0.43–0.74) | 0.98 | - | - |
| Employee Status ** | ||||
| Employed | Reference | - | - | |
| Unemployed | 2.03 (1.57–2.62) | 0.02 | - | - |
| Unknown | 1.39 (0.61–3.12) | 0.95 | - | - |
| Smoking Status | ||||
| No | Reference | - | - | |
| Yes | 1.68 (0.88–3.19) | 0.11 | - | - |
| Number of comorbidities *** | ||||
| 0 | Reference | Reference | ||
| 1 | 2.02 (1.48–2.77) | 0.64 | 1.66 (1.19–2.30) | 0.91 |
| 2 | 2.53 (1.65–3.88) | 0.27 | 1.78 (1.13–2.82) | 0.71 |
| 3 or more | 4.06 (2.84–5.81) | <0.0001 | 2.69 (1.79–4.03) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
David, S.P.; Singh, L.; Pruitt, J.; Hensing, A.; Hulick, P.; Meltzer, D.O.; O’Donnell, P.H.; Dunnenberger, H.M. The Contribution of Pharmacogenetic Drug Interactions to 90-Day Hospital Readmissions: Preliminary Results from a Real-World Healthcare System. J. Pers. Med. 2021, 11, 1242. https://doi.org/10.3390/jpm11121242
David SP, Singh L, Pruitt J, Hensing A, Hulick P, Meltzer DO, O’Donnell PH, Dunnenberger HM. The Contribution of Pharmacogenetic Drug Interactions to 90-Day Hospital Readmissions: Preliminary Results from a Real-World Healthcare System. Journal of Personalized Medicine. 2021; 11(12):1242. https://doi.org/10.3390/jpm11121242
Chicago/Turabian StyleDavid, Sean P., Lavisha Singh, Jaclyn Pruitt, Andrew Hensing, Peter Hulick, David O. Meltzer, Peter H. O’Donnell, and Henry M. Dunnenberger. 2021. "The Contribution of Pharmacogenetic Drug Interactions to 90-Day Hospital Readmissions: Preliminary Results from a Real-World Healthcare System" Journal of Personalized Medicine 11, no. 12: 1242. https://doi.org/10.3390/jpm11121242