
Trop-2 Therapy in Metastatic Triple-Negative Breast Cancer in Italy: Clinical Opportunity and Regulatory Pitfalls


{kind=link}
Abstract
:1. Introduction
1.1. Sacituzumab Govitecan
1.2. Trop-2
1.3. Preclinical and Clinical Studies
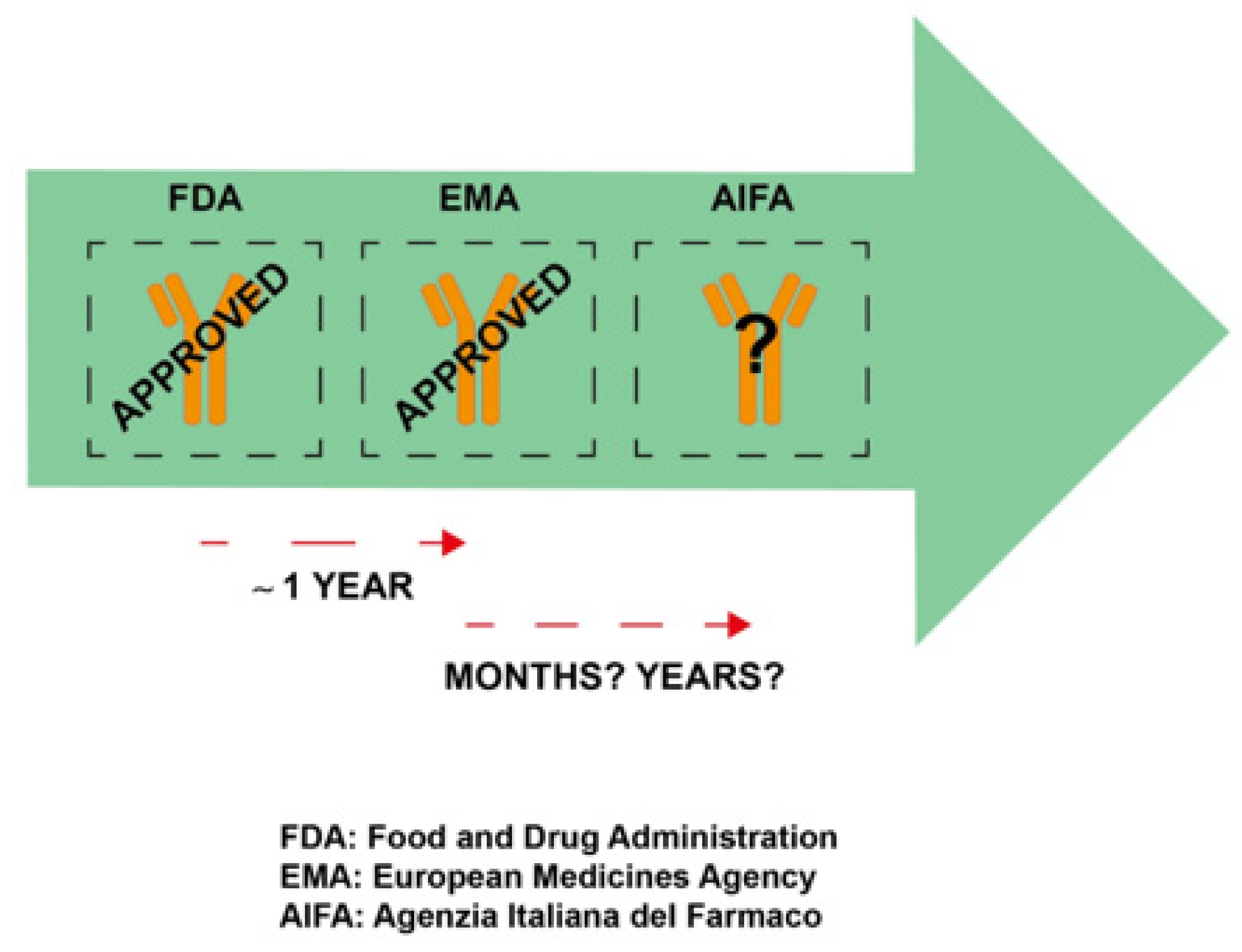
1.4. Regulatory Issue
2. Discussion
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| FDA | Food and Drug Administration |
| EMA | European Medicines Agency |
| AIFA | Agenzia Italiana del Farmaco |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- World Health Organization. Italy. 2020. Available online: https://gco.iarc.fr/today/data/factsheets/populations/380-italy-fact-sheets.pdf (accessed on 12 November 2021).
- Anders, C.K.; Zagar, T.M.; Carey, L.A. The management of early-stage and metastatic triple-negative breast cancer: A review. Hematol. Oncol. Clin. N. Am. 2013, 27, 737–749. [Google Scholar] [CrossRef] [Green Version]
- Zeichner, S.B.; Terawaki, H.; Gogineni, K. A review of systemic treatment in metastatic triple-negative breast cancer. Breast Cancer 2016, 10, 25–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, F.; Costa, A.; Senkus, E.; Aapro, M.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.; Biganzoli, L.; Cardo-so, M.J.; et al. 3rd ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 3). Breast 2017, 31, 244–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Breast Cancer; Version 8. Available online: https://www.nccn.org/login?ReturnURL=https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 12 November 2021).
- Sharkey, R.M.; McBride, W.J.; Cardillo, T.M.; Govindan, S.V.; Wang, Y.; Rossi, E.A.; Chang, C.-H.; Goldenberg, D.M. Enhanced delivery of SN-38 to human tumor xenografts with an anti-Trop-2-SN-38 antibody conjugate (sacituzumab govitecan). Clin. Cancer Res. 2015, 21, 5131–5138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawato, Y.; Aonuma, M.; Hirota, Y.; Kuga, H.; Sato, K. Intra-cellular roles of SN-38, a metabolite of the camptothecin derivative CPT-11, in the anti-tumor effect of CPT-11. Cancer Res. 1991, 51, 4187–4191. [Google Scholar] [PubMed]
- TRODELVY. Prescribing Information. 2020. Available online: https://trodelvy.com/prescribing-information (accessed on 12 November 2021).
- Ocean, A.J.; Starodub, A.N.; Bardia, A.; Vahdat, L.T.; Isakoff, S.J.; Guarino, M.; Messersmith, W.A.; Picozzi, V.J.; Mayer, I.A.; Wegener, W.A.; et al. Sacituzumab govitecan (IMMU-132), an anti-Trop-2-SN-38 antibody-drug conjugate for the treatment of diverse epithelial cancers: Safety and pharmacokinetics. Cancer 2017, 123, 3843–3854. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, D.M.; Stein, R.; Sharkey, R.M. The emergence of trophoblast cell-surface antigen 2 (Trop-2) as a novel cancer target. Oncotarget 2018, 9, 28989–29006. [Google Scholar] [CrossRef] [Green Version]
- Lipinski, M.; Parks, D.R.; Rouse, R.V.; Herzenberg, L.A. Human trophoblast cell-surface antigens defined by monoclonal antibodies. Proc. Natl. Acad. Sci. USA 1981, 78, 5147–5150. [Google Scholar] [CrossRef] [Green Version]
- Ripani, E.; Sacchetti, A.; Corda, D.; Alberti, S. Human trop-2 is a tumor-associated calcium signal transducer. Int. J. Cancer 1998, 76, 671–676. [Google Scholar] [CrossRef]
- Zaman, S.; Jadid, H.; Denson, A.C.; Gray, J.E. Targeting trop-2 in solid tumors: Future prospects. OncoTargets Ther. 2019, 12, 1781–1790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, E.; Trerotola, M.; Aloisi, A.L.; Tripaldi, R.; Vacca, G.; La Sorda, R.; Lattanzio, R.; Piantelli, M.; Alberti, S. The trop-2 signalling network in cancer growth. Oncogene 2013, 32, 1594–1600. [Google Scholar] [CrossRef]
- Stepan, L.P.; Trueblood, E.S.; Hale, K.; Babcook, J.; Borges, L.; Sutherland, C.L. Expression of Trop2 cell surface glycoprotein in normal and tumor tissues: Potential implications as a cancer therapeutic target. J. Histochem. Cytochem. 2011, 59, 701–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shvartsur, A.; Bonavida, B. Trop2 and its overexpression in cancers: Regulation and clinical/therapeutic implications. Genes Cancer 2015, 6, 84–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, P.; Chen, M.B.; Zhou, L.N.; Tang, M.; Liu, C.Y.; Lu, P.H. Impact of TROP2 expression on prognosis in solid tumors: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 33658. [Google Scholar] [CrossRef] [Green Version]
- Wolber, P.; Nachtsheim, L.; Hoffmann, F.; Klussmann, J.P.; Meyer, M.; von Eggeling, F.; Guntinas-Lichius, O.; Quaas, A.; Arolt, C. Trophoblast cell surface antigen 2 (Trop-2) protein is highly expressed in salivary gland carcinomas and represents a potential therapeutic target. Head Neck Pathol. 2021, 4, 22. [Google Scholar] [CrossRef]
- Seok, J.Y.; Astvatsaturyan, K.; Peralta-Venturina, M.; Lai, J.; Fan, X. TROP-2, 5hmC, and IDH1 expression in anaplastic thyroid carcinoma. Int. J. Surg. Pathol. 2021, 29, 368–377. [Google Scholar] [CrossRef]
- Lopez, S.; Perrone, E.; Bellone, S.; Bonazzoli, E.; Zeybek, B.; Han, C.; Tymon-Rosario, J.G.; Menderes, G.; Bianchi, A. Preclinical activity of sacituzumab govitecan (IMMU-132) in uterine and ovarian carcinosarcomas. Oncotarget 2020, 11, 560–570. [Google Scholar] [CrossRef] [Green Version]
- Raji, R.; Guzzo, F.; Carrara, L.; Varughese, J.; Cocco, E.; Bellone, S.; Betti, M.; Todeschini, P.; Gasparrini, S.; Ratner, E.; et al. Uterine and ovarian carcinosarcomas overexpressing Trop-2 are sensitive to hRS7, a humanized anti-Trop-2 antibody. J. Exp. Clin. Cancer Res. 2011, 30, 106. [Google Scholar] [CrossRef] [Green Version]
- Hsu, E.C.; Rice, M.A.; Bermudez, A.; Marques, F.J.; Aslan, M.; Liu, S.; Ghoochani, A.; Zhang, C.A.; Chen, Y.-S.; Zlitni, A.; et al. Trop2 is a driver of metastatic prostate cancer with neuroendocrine phenotype via PARP1. Proc. Natl. Acad. Sci. USA 2020, 117, 2032–2042. [Google Scholar] [CrossRef] [Green Version]
- Vranic, S.; Palazzo, J.; Sanati, S.; Florento, E.; Contreras, E.; Xiu, J.; Swensen, J.; Gatalica, Z. Potential novel therapy targets in neuroendocrine carcinomas of the breast. Clin. Breast Cancer 2019, 19, 131–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardillo, T.M.; Sharkey, R.M.; Rossi, D.L.; Arrojo, R.; Mostafa, A.A.; Goldenberg, D.M. Synthetic lethality exploitation by an anti-Trop-2-SN-38 antibody-drug conjugate, IMMU-132, plus PARP inhibitors in BRCA1/2-wild-type triple-negative breast cancer. Clin. Cancer Res. 2017, 23, 405–3415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syed, Y.Y. Sacituzumab Govitecan: First Approval. Drugs 2020, 80, 1019–1025. [Google Scholar] [CrossRef]
- Goldenberg, D.M.; Cardillo, T.M.; Govindan, S.V.; Rossi, E.A.; Sharkey, R.M. Trop-2 is a novel target for solid cancer therapy with sacituzumab govitecan (IMMU-132), an antibody-drug conjugate (ADC). Oncotarget 2015, 6, 22496–22512. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Kuai, X.; Zhou, X.; Jia, L.; Wang, J.; Yang, X.; Tian, Z.; Wang, X.; Lv, Q.; Wang, B.; et al. Trop2 is a potential biomarker for the promotion of EMT in human breast cancer. Oncol. Rep. 2018, 40, 759–766. [Google Scholar] [CrossRef] [Green Version]
- Gu, Q.Z.; Nijiati, A.; Gao, X.; Tao, K.L.; Li, C.D.; Fan, X.P.; Tian, Z. Trop2 promotes cell proliferation and migration in osteosarcoma through PI3K/AKT signaling. Mol. Med. Rep. 2018, 18, 1782–1788. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Tolaney, S.M.; Punie, K.; Loirat, D.; Oliveira, M.; Kalinsky, K.; Zelnak, A.; Aftimos, P.; Dalenc, F.; Sardesai, S. Biomarker analyses in the phase III ASCENT study of sacituzumab govitecan versus chemotherapy in patients with metastatic triple-negative breast cancer. Ann. Oncol. 2021, 32, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Hurvitz, S.A.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Sardesai, S.D.; Kalinsky, K.; Zelnak, A.B. ASCENT Clinical Trial Investigators. Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. N. Engl. J. Med. 2021, 384, 1529–1541. [Google Scholar] [CrossRef]
- Bartsch, R. SABCS 2020: Update on triple-negative and metastatic HER2-positive breast cancer. Memo 2021, 29, 1–5. [Google Scholar] [CrossRef]
- Brenner, A.J.; Pandey, R.; Chiou, J.; Floyd, J.; Surapreneni, P.; Kaklamani, V.; Lathrop, K.; Crownover, R.; Tiziani, S. Delivery and activity of SN-38 by sacituzumab govitecan in breast cancer brain metastases. In Proceedings of the San Antonio Breast Cancer Virtual Symposium, San Antonio, TX, USA, 8–11 December 2020. [Google Scholar] [CrossRef]
- Kalinsky, K.; Diamond, J.R.; Vahdat, L.T.; Tolaney, S.M.; Juric, D.; O’Shaughnessy, J.; Moroose, R.L.; Mayer, I.A.; Abramson, V.G.; Goldenberg, D.M.; et al. Sacituzumab govitecan in previously treated hormone receptor-positive/HER2-negative metastatic breast cancer: Final results from a phase I/II, single-arm, basket trial. Ann. Oncol. 2020, 31, 1709–1718. [Google Scholar] [CrossRef]
- Available online: https://www.intexo.it/wp-content/uploads/2021/05/02_Febbraio_2021_time_to_care_patient_report.pdf (accessed on 12 November 2021).
- Available online: https://www.issalute.it/index.php/la-salute-dalla-a-alla-z-menu/f/farmaci-come-si-sviluppa-un-nuovo-farmaco (accessed on 12 November 2021).
- Bardia, A.; Mayer, I.A.; Diamond, J.R.; Moroose, R.L.; Isakoff, S.J.; Starodub, A.N.; Shah, N.C.; O’Shaughnessy, J.; Kalinsky, K.; Guarino, M.; et al. Efficacy and Safety of Anti-Trop2 Antibody Drug Conjugate Sacituzumab Govitecan (IMMU-132) in Heavily Pretreated Patients with Metastatic Triple-Negative Breast Cancer. J. Clin. Oncol. 2017, 35, 2141–2148. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bravaccini, S.; Maltoni, R. Trop-2 Therapy in Metastatic Triple-Negative Breast Cancer in Italy: Clinical Opportunity and Regulatory Pitfalls. J. Pers. Med. 2021, 11, 1211. https://doi.org/10.3390/jpm11111211
Bravaccini S, Maltoni R. Trop-2 Therapy in Metastatic Triple-Negative Breast Cancer in Italy: Clinical Opportunity and Regulatory Pitfalls. Journal of Personalized Medicine. 2021; 11(11):1211. https://doi.org/10.3390/jpm11111211
Chicago/Turabian StyleBravaccini, Sara, and Roberta Maltoni. 2021. "Trop-2 Therapy in Metastatic Triple-Negative Breast Cancer in Italy: Clinical Opportunity and Regulatory Pitfalls" Journal of Personalized Medicine 11, no. 11: 1211. https://doi.org/10.3390/jpm11111211