
Artificial Intelligence and COVID-19 Using Chest CT Scan and Chest X-ray Images: Machine Learning and Deep Learning Approaches for Diagnosis and Treatment

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Search Criterion
2.2. Statistical Analysis
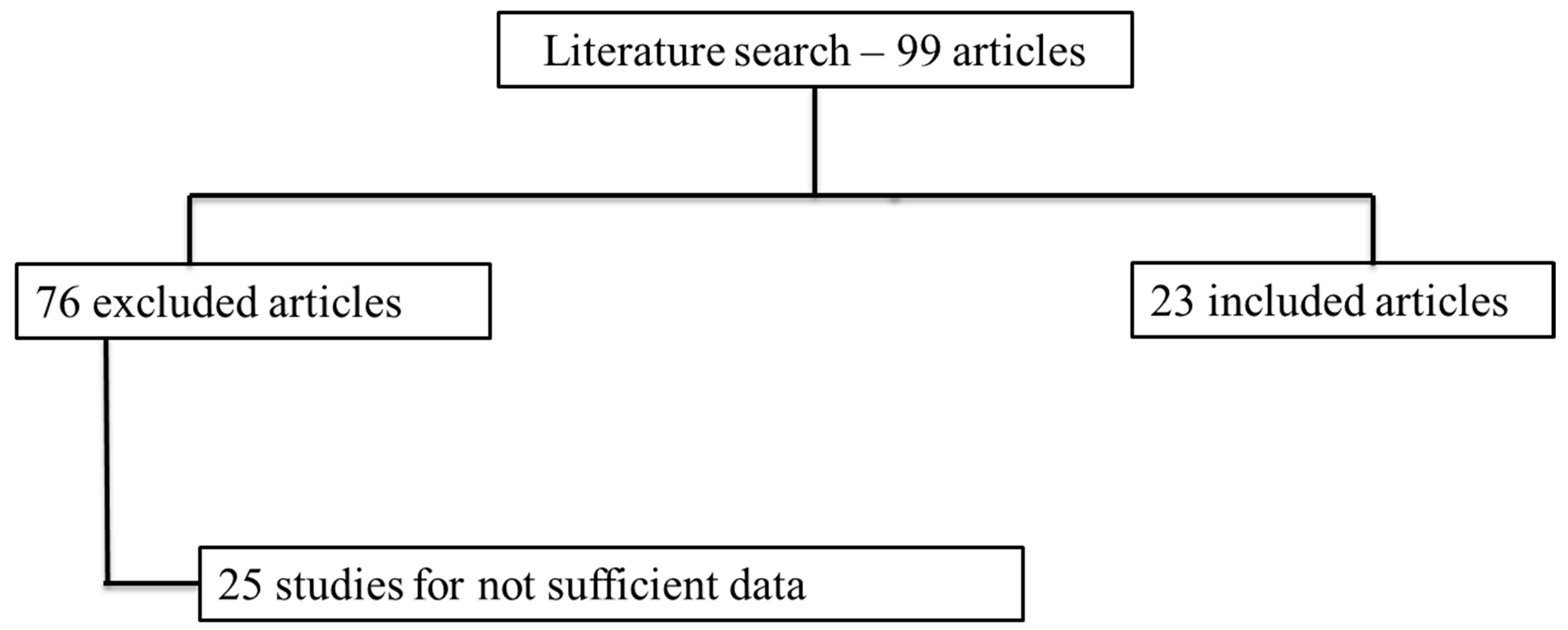
3. Results
4. Discussions
4.1. Application on Chest X-Ray Images
4.2. Application on Chest CT images
4.3. Critical Considerations and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Summary of Probable SARS Cases with onset of Illness from 1 November 2002 to 31 July 2003 (based on data as of 31 December 2003). Available online: https://www.who.int/home/search?indexCatalogue=genericsearchindex1 (accessed on 24 June 2021).
- WHO. Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Available online: https://www.who.int/health-topics/middle-east-respiratory-syndrome-coronavirus-mers#tab=tab_1 (accessed on 24 June 2021).
- WHO. Naming the Coronavirus Disease (COVID-2019) and the Virus That Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 24 June 2021).
- Giovanetti, M.; Angeletti, S.; Benvenuto, D.; Ciccozzi, M. A doubt of multiple introduction of SARS-CoV-2 in Italy: A preliminary overview. J. Med. Virol. 2020, 92, 1634–1636. [Google Scholar] [CrossRef]
- Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). COVID-19 Dashboard. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 5 August 2020).
- Kinross, P.; Suetens, C.; Dias, J.G.; Alexakis, L.; Wijermans, A.; Colzani, E.; Monnet, D.L. European Centre for Disease Prevention and Control (ECDC) Public Health Emergency Team Rapidly increasing cumulative incidence of coronavirus disease (COVID-19) in the European Union/European Economic Area and the United Kingdom, 1 January to 15 March 2020. Eurosurveillance 2020, 25, 2000285. [Google Scholar] [CrossRef]
- Kostoulas, P.; Eusebi, P.; Hartnack, S. Diagnostic Accuracy Estimates for COVID-19 Real-Time Polymerase Chain Reaction and Lateral Flow Immunoassay Tests with Bayesian Latent-Class Models. Am. J. Epidemiol. 2021, 190, 1689–1695. [Google Scholar] [CrossRef]
- Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Spijker, R.; Taylor-Phillips, S.; Adriano, A.; Beese, S.; Dretzke, J.; di Ruffano, L.F.; et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst. Rev. 2020, 2020, CD013652. [Google Scholar] [CrossRef]
- Beigmohammadi, M.T.; Bitarafan, S.; Abdollahi, A.; Amoozadeh, L.; Salahshour, F.; Abadi, M.M.A.; Soltani, D.; Motallebnejad, Z.A. The association between serum levels of micronutrients and the severity of disease in patients with COVID-19. Nutrition 2021, 91–92, 111400. [Google Scholar] [CrossRef] [PubMed]
- Stramare, R.; Carretta, G.; Capizzi, A.; Boemo, D.G.; Contessa, C.; Motta, R.; De Conti, G.; Causin, F.; Giraudo, C.; Donato, D. Radiological management of COVID-19: Structure your diagnostic path to guarantee a safe path. Radiol. Med. 2020, 125, 691–694. [Google Scholar] [CrossRef] [PubMed]
- Ierardi, A.M.; Wood, B.J.; Arrichiello, A.; Bottino, N.; Bracchi, L.; Forzenigo, L.; Andrisani, M.C.; Vespro, V.; Bonelli, C.; Amalou, A.; et al. Preparation of a radiology department in an Italian hospital dedicated to COVID-19 patients. Radiol. Med. 2020, 125, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Cappabianca, S.; Fusco, R.; de Lisio, A.; Paura, C.; Clemente, A.; Gagliardi, G.; Lombardi, G.; Giacobbe, G.; Russo, G.M.; Belfiore, M.P.; et al. Correction to: Clinical and laboratory data, radiological structured report findings and quantitative evaluation of lung involvement on baseline chest CT in COVID-19 patients to predict prognosis. Radiol. Med. 2021, 126, 643. [Google Scholar] [CrossRef]
- Carvalho, E.D.; Silva, R.R.; Araújo, F.H.; Rabelo, R.D.A.; Filho, A.O.D.C. An approach to the classification of COVID-19 based on CT scans using convolutional features and genetic algorithms. Comput. Biol. Med. 2021, 136, 104744. [Google Scholar] [CrossRef]
- Nakazono, T.; Yamaguchi, K.; Egashira, R.; Mizuguchi, M.; Irie, H. Anterior mediastinal lesions: CT and MRI features and differential diagnosis. JPN J. Radiol. 2021, 39, 101–117. [Google Scholar] [CrossRef]
- Koç, A.; Sezgin, S.; Kayıpmaz, S. Comparing different planimetric methods on volumetric estimations by using cone beam computed tomography. Radiol. Med. 2020, 125, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.-X.; Liu, C.; Liu, J.; Ding, Z.; Shi, F.; Guo, M.; Zhao, W.; Li, X.; Wei, Y.; Gao, Y.; et al. Cross-Site Severity Assessment of COVID-19 from CT Images via Domain Adaptation. IEEE Trans. Med Imaging 2021, 1. [Google Scholar] [CrossRef]
- Gaia, C.; Chiara, C.M.; Silvia, L.; Chiara, A.; Luisa, D.C.M.; Giulia, B.; Silvia, P.; Lucia, C.; Alessandra, T.; Annarita, S.; et al. Chest CT for early detection and management of coronavirus disease (COVID-19): A report of 314 patients admitted to Emergency Department with suspected pneumonia. Radiol. Med. 2020, 125, 931–942. [Google Scholar] [CrossRef] [PubMed]
- Giannitto, C.; Sposta, F.M.; Repici, A.; Vatteroni, G.; Casiraghi, E.; Casari, E.; Ferraroli, G.M.; Fugazza, A.; Sandri, M.T.; Chiti, A.; et al. Chest CT in patients with a moderate or high pretest probability of COVID-19 and negative swab. Radiol. Med. 2020, 125, 1260–1270. [Google Scholar] [CrossRef] [PubMed]
- Crimì, F.; Cabrelle, G.; Zanon, C.; Quaia, E. Chest computed tomography in COVID-19 infection. Clin. Transl. Imaging 2021, 8, 1–2. [Google Scholar] [CrossRef]
- Giovagnoni, A. Facing the COVID-19 emergency: We can and we do. Radiol. Med. 2020, 125, 337–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montesi, G.; Di Biase, S.; Chierchini, S.; Pavanato, G.; Virdis, G.E.; Contato, E.; Mandoliti, G. Radiotherapy during COVID-19 pandemic. How to create a No fly zone: A Northern Italy experience. Radiol. Med. 2020, 125, 600–603. [Google Scholar] [CrossRef]
- Agostini, A.; Floridi, C.; Borgheresi, A.; Badaloni, M.; Pirani, P.E.; Terilli, F.; Ottaviani, L.; Giovagnoni, A. Proposal of a low-dose, long-pitch, dual-source chest CT protocol on third-generation dual-source CT using a tin filter for spectral shaping at 100 kVp for CoronaVirus Disease 2019 (COVID-19) patients: A feasibility study. Radiol. Med. 2020, 125, 365–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borghesi, A.; Maroldi, R. COVID-19 outbreak in Italy: Experimental chest X-ray scoring system for quantifying and monitoring disease progression. Radiol. Med. 2020, 125, 509–513. [Google Scholar] [CrossRef]
- Fichera, G.; Stramare, R.; De Conti, G.; Motta, R.; Giraudo, C. It’s not over until it’s over: The chameleonic behavior of COVID-19 over a six-day period. Radiol. Med. 2020, 125, 514–516. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Setola, S.; Galdiero, R.; Picone, C.; Izzo, F.; D’Aniello, R.; Miele, V.; Grassi, R.; Grassi, R.; et al. Lymphadenopathy after BNT162b2 Covid-19 Vaccine: Preliminary Ultrasound Findings. Biology 2021, 10, 214. [Google Scholar] [CrossRef] [PubMed]
- Belfiore, M.P.; Urraro, F.; Grassi, R.; Giacobbe, G.; Patelli, G.; Cappabianca, S.; Reginelli, A. Artificial intelligence to codify lung CT in Covid-19 patients. Radiol. Med. 2020, 125, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Neri, E.; Miele, V.; Coppola, F.; Grassi, R. Use of CT and artificial intelligence in suspected or COVID-19 positive patients: Statement of the Italian Society of Medical and Interventional Radiology. Radiol. Med. 2020, 125, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Carotti, M.; Salaffi, F.; Sarzi-Puttini, P.; Agostini, A.; Borgheresi, A.; Minorati, D.; Galli, M.; Marotto, D.; Giovagnoni, A. Chest CT features of coronavirus disease 2019 (COVID-19) pneumonia: Key points for radiologists. Radiol. Med. 2020, 125, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Shaw, B.; Daskareh, M.; Gholamrezanezhad, A. The lingering manifestations of COVID-19 during and after convalescence: Update on long-term pulmonary consequences of coronavirus disease 2019 (COVID-19). Radiol. Med. 2020, 126, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Di Serafino, M.; Notaro, M.; Rea, G.; Iacobellis, F.; Delli Paoli, V.; Acampora, C.; Ianniello, S.; Brunese, L.; Romano, L.; Vallone, G. The lung ultrasound: Facts or artifacts? In the era of COVID-19 outbreak. Radiol Med. 2020, 125, 738–753. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, D.; Albanesi, M.; Cavigli, E.; Moroni, C.; Bindi, A.; Luvarà, S.; Lucarini, S.; Busoni, S.; Mazzoni, L.N.; Miele, V. Chest X-ray in new Coronavirus Disease 2019 (COVID-19) infection: Findings and correlation with clinical outcome. Radiol. Med. 2020, 125, 730–737. [Google Scholar] [CrossRef]
- Pediconi, F.; Galati, F.; Bernardi, D.; Belli, P.; Brancato, B.; Calabrese, M.; Camera, L.; Carbonaro, L.A.; Caumo, F.; Clauser, P.; et al. Breast imaging and cancer diagnosis during the COVID-19 pandemic: Recommendations from the Italian College of Breast Radiologists by SIRM. Radiol. Med. 2020, 125, 926–930. [Google Scholar] [CrossRef]
- Borghesi, A.; Zigliani, A.; Masciullo, R.; Golemi, S.; Maculotti, P.; Farina, D.; Maroldi, R. Radiographic severity index in COVID-19 pneumonia: Relationship to age and sex in 783 Italian patients. Radiol. Med. 2020, 125, 461–464. [Google Scholar] [CrossRef]
- Gatti, M.; Calandri, M.; Barba, M.; Biondo, A.; Geninatti, C.; Gentile, S.; Greco, M.; Morrone, V.; Piatti, C.; Santonocito, A.; et al. Baseline chest X-ray in coronavirus disease 19 (COVID-19) patients: Association with clinical and laboratory data. Radiol. Med. 2020, 125, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Caruso, D.; Polici, M.; Zerunian, M.; Pucciarelli, F.; Polidori, T.; Guido, G.; Rucci, C.; Bracci, B.; Muscogiuri, E.; De Dominicis, C.; et al. Quantitative Chest CT analysis in discriminating COVID-19 from non-COVID-19 patients. Radiol. Med. 2020, 126, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Grassi, R.; Belfiore, M.P.; Montanelli, A.; Patelli, G.; Urraro, F.; Giacobbe, G.; Fusco, R.; Granata, V.; Petrillo, A.; Sacco, P.; et al. COVID-19 pneumonia: Computer-aided quantification of healthy lung parenchyma, emphysema, ground glass and consolidation on chest computed tomography (CT). Radiol. Med. 2020, 126, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Grassi, R.; Cappabianca, S.; Urraro, F.; Granata, V.; Giacobbe, G.; Magliocchetti, S.; Cozzi, D.; Fusco, R.; Galdiero, R.; Picone, C.; et al. Evolution of CT Findings and Lung Residue in Patients with COVID-19 Pneumonia: Quantitative Analysis of the Disease with a Computer Automatic Tool. J. Pers. Med. 2021, 11, 641. [Google Scholar] [CrossRef] [PubMed]
- Grassi, R.; Miele, V.; Giovagnoni, A. Artificial intelligence: A challenge for third millennium radiologist. Radiol. Med. 2019, 124, 241–242. [Google Scholar] [CrossRef] [Green Version]
- Neri, E.; Coppola, F.; Miele, V.; Bibbolino, C.; Grassi, R. Artificial intelligence: Who is responsible for the diagnosis? Radiol. Med. 2020, 125, 517–521. [Google Scholar] [CrossRef] [Green Version]
- Van Assen, M.; Muscogiuri, G.; Caruso, D.; Lee, S.J.; Laghi, A.; De Cecco, C.N. Artificial intelligence in cardiac radiology. Radiol. Med. 2020, 125, 1186–1199. [Google Scholar] [CrossRef]
- Chen, T.; Ning, Z.; Xu, L.; Feng, X.; Han, S.; Roth, H.R.; Xiong, W.; Zhao, X.; Hu, Y.; Liu, H.; et al. Radiomics nomogram for predicting the malignant potential of gastrointestinal stromal tumours preoperatively. Eur. Radiol. 2019, 29, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.-T.; Shan, Q.-Y.; Chen, S.-L.; Li, B.; Feng, S.-T.; Xu, E.-J.; Li, X.; Long, J.-Y.; Xie, X.-Y.; Lu, M.-D.; et al. CT-based radiomics for preoperative prediction of early recurrent hepatocellular carcinoma: Technical reproducibility of acquisition and scanners. Radiol. Med. 2020, 125, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Chang, W.; Kim, J.H.; Ahn, C.; Lee, H.; Kim, H.Y.; Cho, J.; Lee, Y.J.; Kim, Y.H. Dose reduction potential of vendor-agnostic deep learning model in comparison with deep learning–based image reconstruction algorithm on CT: A phantom study. Eur. Radiol. 2021, 8, 1–9. [Google Scholar] [CrossRef]
- Ma, J.; He, N.; Yoon, J.H.; Ha, R.; Li, J.; Ma, W.; Meng, T.; Lu, L.; Schwartz, L.H.; Wu, Y.; et al. Distinguishing benign and malignant lesions on contrast-enhanced breast cone-beam CT with deep learning neural architecture search. Eur. J. Radiol. 2021, 142, 109878. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Ni, S.; Yang, C.; Sun, W.; Huang, D.; Su, H.; Shu, J.; Qin, N. Axillary lymph node metastasis prediction by contrast-enhanced computed tomography images for breast cancer patients based on deep learning. Comput. Biol. Med. 2021, 136, 104715. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, D.; Bicci, E.; Bindi, A.; Cavigli, E.; Danti, G.; Galluzzo, M.; Granata, V.; Pradella, S.; Trinci, M.; Miele, V. Role of Chest Imaging in Viral Lung Diseases. Int. J. Environ. Res. Public Health 2021, 18, 6434. [Google Scholar] [CrossRef] [PubMed]
- Kirienko, M.; Ninatti, G.; Cozzi, L.; Voulaz, E.; Gennaro, N.; Barajon, I.; Ricci, F.; Carlo-Stella, C.; Zucali, P.; Sollini, M.; et al. Computed tomography (CT)-derived radiomic features differentiate prevascular mediastinum masses as thymic neoplasms versus lymphomas. Radiol. Med. 2020, 125, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Nazari, M.; Shiri, I.; Hajianfar, G.; Oveisi, N.; Abdollahi, H.; Deevband, M.R.; Oveisi, M.; Zaidi, H. Noninvasive Fuhrman grading of clear cell renal cell carcinoma using computed tomography radiomic features and machine learning. Radiol. Med. 2020, 125, 754–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palumbo, P.; Cannizzaro, E.; Bruno, F.; Schicchi, N.; Fogante, M.; Agostini, A.; De Donato, M.C.; De Cataldo, C.; Giovagnoni, A.; Barile, A.; et al. Coronary artery disease (CAD) extension-derived risk stratification for asymptomatic diabetic patients: Usefulness of low-dose coronary computed tomography angiography (CCTA) in detecting high-risk profile patients. Radiol. Med. 2020, 125, 1249–1259. [Google Scholar] [CrossRef]
- Zhang, L.; Kang, L.; Li, G.; Zhang, X.; Ren, J.; Shi, Z.; Li, J.; Yu, S. Computed tomography-based radiomics model for discriminating the risk stratification of gastrointestinal stromal tumors. Radiol. Med. 2020, 125, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Abdollahi, H.; Mofid, B.; Shiri, I.; Razzaghdoust, A.; Saadipoor, A.; Mahdavi, A.; Galandooz, H.M.; Mahdavi, S.R. Machine learning-based radiomic models to predict intensity-modulated radiation therapy response, Gleason score and stage in prostate cancer. Radiol. Med. 2019, 124, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Grassi, R.; Fusco, R.; Belfiore, M.P.; Montanelli, A.; Patelli, G.; Urraro, F.; Petrillo, A.; Granata, V.; Sacco, P.; Mazzei, M.A.; et al. Coronavirus disease 2019 (COVID-19) in Italy: Features on chest computed tomography using a structured report system. Sci. Rep. 2020, 10, 17236. [Google Scholar] [CrossRef]
- Reginelli, A.; Grassi, R.; Feragalli, B.; Belfiore, M.; Montanelli, A.; Patelli, G.; La Porta, M.; Urraro, F.; Fusco, R.; Granata, V.; et al. Coronavirus Disease 2019 (COVID-19) in Italy: Double Reading of Chest CT Examination. Biology 2021, 10, 89. [Google Scholar] [CrossRef]
- Agbehadji, I.E.; Awuzie, B.O.; Ngowi, A.B.; Millham, R.C. Review of Big Data Analytics, Artificial Intelligence and Nature-Inspired Computing Models towards Accurate Detection of COVID-19 Pandemic Cases and Contact Tracing. Int. J. Environ. Res. Public Health 2020, 17, 5330. [Google Scholar] [CrossRef]
- Bullock, J.; Luccioni, A.; Pham, K.H.; Lam, C.S.N.; Luengo-Oroz, M. Mapping the landscape of Artificial Intelligence applications against COVID-19. J. Artif. Intell. Res. 2020, 69, 807–845. [Google Scholar] [CrossRef]
- Naudé, W. Artificial intelligence vs. covid-19: Limitations, constraints and pitfalls. AI Soc. 2020, 35, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wang, J.; Nicholas, S.; Maitland, E.; Fan, Q. Application of Big Data Technology for COVID-19 Prevention and Control in China: Lessons and Recommendations. J. Med. Internet Res. 2020, 22, e21980. [Google Scholar] [CrossRef] [PubMed]
- Alballa, N.; Al-Turaiki, I. Machine Learning Approaches in COVID-19 Diagnosis, Mortality, and Severity Risk Prediction: A Review. Inform. Med. Unlocked 2021, 24, 100564. [Google Scholar] [CrossRef]
- Raiano, N.; Raiano, C.; Mazio, F.; Rossi, I.; Bordino, U.; De Simone, G.; Fusco, R.; Granata, V.; Cerciello, V.; Setola, S.V.; et al. Home mobile radiography service in the COVID-19 era. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3338–3341. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Izzo, F.; Setola, S.V.; Coppola, M.; Grassi, R.; Reginelli, A.; Cappabianca, S.; Petrillo, A. Covid-19 infection in cancer patients: The management in a diagnostic unit. Radiol. Oncol. 2021, 55, 121–129. [Google Scholar] [CrossRef]
- Bandirali, M.; Sconfienza, L.M.; Serra, R.; Brembilla, R.; Albano, D.; Pregliasco, F.E.; Messina, C. Chest Radiograph Findings in Asymptomatic and Minimally Symptomatic Quarantined Patients in Codogno, Italy during COVID-19 Pandemic. Radiology 2020, 295, E7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, G.; Yang, Z.; Gong, L.; Jiang, S.; Wang, L.; Zhang, H. Classification of lung nodules based on CT images using squeeze-and-excitation network and aggregated residual transformations. Radiol. Med. 2020, 125, 374–383. [Google Scholar] [CrossRef]
- Wang, S.; Kang, B.; Ma, J.; Zeng, X.; Xiao, M.; Guo, J.; Cai, M.; Yang, J.; Li, Y.; Meng, X.; et al. A deep learning algorithm using CT images to screen for Corona virus disease (COVID-19). Eur. Radiol. 2021, 31, 6096–6104. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, G.; Zhao, S. COVSeg-NET: A deep convolution neural network for COVID -19 lung CT image segmentation. Int. J. Imaging Syst. Technol. 2021, 31, 1071–1086. [Google Scholar] [CrossRef]
- Wang, R.; Jiao, Z.; Yang, L.; Choi, J.W.; Xiong, Z.; Halsey, K.; Tran, T.M.L.; Pan, I.; Collins, S.A.; Feng, X.; et al. Artificial intelligence for prediction of COVID-19 progression using CT imaging and clinical data. Eur. Radiol. 2021, 7, 1–8. [Google Scholar] [CrossRef]
- Peng, Q.-Y.; Chinese Critical Care Ultrasound Study Group (CCUSG); Wang, X.-T.; Zhang, L.-N. Findings of lung ultrasonography of novel corona virus pneumonia during the 2019–2020 epidemic. Intensiv. Care Med. 2020, 46, 849–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Xia, L. Coronavirus Disease 2019 (COVID-19): Role of Chest CT in Diagnosis and Management. Am. J. Roentgenol. 2020, 214, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Lei, J.; Li, J.; Li, X.; Qi, X. CT Imaging of the 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology 2020, 295, 18. [Google Scholar] [CrossRef] [Green Version]
- Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 145–151. [Google Scholar]
- American College of Radiology. ACR Recommendations for the Use of Chest Radiography and Computed Tomography (CT) for Suspected COVID-19 Infection. Available online: https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recommendations-for-Chest-Radiography-and-CT-for-Suspected-COVID19-Infection (accessed on 24 June 2021).
- The Royal Australian and New Zealand College of Radiologist. COVID-19 Updates. Available online: https://www.ranzcr.com/our-work/coronavirus (accessed on 24 June 2021).
- The Royal College of Radiologists. RCR position on the role of CT in patients suspected with COVID-19 infection. Available online: https://www.rcr.ac.uk/search-v2?search=the%20role%20of%20CT%20in%20patients%20suspected%20with%20COVID-19%20infection%20 (accessed on 24 June 2021).
- Canadian Association of Radiologists. Canadian Society of Thoracic Radiology and Canadian Association of Radiologists’ Statement on COVID -19. Available online: https://car.ca/news/canadian-society-of-thoracic-radiology-and-canadian-association-of-radiologists-statement-on-covid-19/ (accessed on 24 June 2021).
- Mossa-Basha, M.; Meltzer, C.C.; Kim, D.C.; Tuite, M.J.; Kolli, K.P.; Tan, B.S. Radiology Department Preparedness for COVID-19: Radiology Scientific Expert Review Panel. Radiology 2020, 296, E106–E112. [Google Scholar] [CrossRef] [Green Version]
- Zu, Z.Y.; Di Jiang, M.; Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.M.; Zhang, L.J. Coronavirus Disease 2019 (COVID-19): A Perspective from China. Radiology 2020, 296, E15–E25. [Google Scholar] [CrossRef] [Green Version]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef]
- Fang, Y.; Zhang, H.; Xu, Y.; Xie, J.; Pang, P.; Ji, W. CT Manifestations of Two Cases of 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology 2020, 295, 208–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, L.; Yu, J.; Shi, H. Severe Acute Respiratory Disease in a Huanan Seafood Market Worker: Images of an Early Casualty. Radiol. Cardiothorac. Imaging 2020, 2, e200033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gozes, O.; Frid-Adar, M.; Greenspan, H.; Browning, P.D.; Zhang, H.; Ji, W.; Bernheim, A.; Siegel, E. Rapid AI Development Cycle for the Coronavirus (COVID-19) Pandemic: Initial Results for Automated Detection & Patient Monitoring using Deep Learning CT Image Analysis. arXiv 2020, arXiv:2003.05037. [Google Scholar]
- Rahmatizadeh, S.; Valizadeh-Haghi, S.; Dabbagh, A. The role of artificial intelligence in management of critical COVID-19 patients. J. Cell. Mol. Anes. 2020, 5, 16–22. [Google Scholar]
- Sethy, P.K.; Behera, S.K.; Ratha, P.K.; Biswas, P. Detection of coronavirus Disease (COVID-19) based on Deep Features and Support Vector Machine. Int. J. Math. Eng. Manag. Sci. 2020, 5, 643–651. [Google Scholar] [CrossRef]
- Kassani, S.H.; Kassasni, P.H.; Wesolowski, M.J.; Schneider, K.A.; Deters, R. Automatic detection of coronavirus disease (COVID-19) in X-ray and CT images: A machine learning-based approach. arXiv 2020, arXiv:2004.10641. [Google Scholar]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Bai, J.; Lu, Y.; Fang, Z.; Song, Q.; et al. Using Artificial Intelligence to Detect COVID-19 and Community-acquired Pneumonia Based on Pulmonary CT: Evaluation of the Diagnostic Accuracy. Radiology 2020, 296, E65–E71. [Google Scholar] [CrossRef]
- Ginneken, B.; Armato, S.J., III; Hoop, B.; van de Vorst, S.A.; Duindam, T.; Murphy, N.; Schilham, A.; Retico, A.; Fantacci, M.E.; Fujita, H.; et al. Comparing and combining algorithms for computer-aided detection of pulmonary nodules in computed tomography scans: The ANODE09 study. Med. Image Anal. 2010, 14, 707–722. [Google Scholar] [CrossRef] [Green Version]
- Bellotti, R.; De Carlo, F.; Gargano, G.; Tangaro, S.; Cascio, D.; Catanzariti, E.; Cerello, P.; Cheran, S.C.; Delogu, P.; De Mitri, I.; et al. A CAD system for nodule detection in low-dose lung CTs based on region growing and a new active contour model. Med. Phys. 2007, 34, 4901–4910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, L.; Campbell, G.; Jones, W.D.; Campagne, F.; Wen, Z.; Walker, S.J.; Su, Z.; Chu, T.M.; Goodsaid, F.M.; Pusztai, L.; et al. The MicroArray Quality Control (MAQC)-II study of common practices for the development and validation of microarray-based predictive models. Nat. Biotechnol. 2010, 28, 827–838. [Google Scholar] [PubMed]
- Jiao, Z.; Choi, J.W.; Halsey, K.; Tran, T.M.L.; Hsieh, B.; Wang, D.; Eweje, F.; Wang, R.; Chang, K.; Wu, J.; et al. Prognostication of patients with COVID-19 using artificial intelligence based on chest X-rays and clinical data: A retrospective study. Lancet Digit. Health 2021, 3, e286–e294. [Google Scholar] [CrossRef]
- Al-Waisy, A.S.; Al-Fahdawi, S.; Mohammed, M.A.; Abdulkareem, K.H.; Mostafa, S.A.; Maashi, M.S.; Arif, M.; Garcia-Zapirain, B. COVID-CheXNet: Hybrid deep learning framework for identifying COVID-19 virus in chest X-rays images. Soft Comput. 2020, 11, 1–16. [Google Scholar] [CrossRef]
- Cohen, J.P.; Morrison, P.; Dao, L. COVID-19 Image Data Collection. 2020. Available online: https://github.com/ieee8023/covid-chestxray-dataset (accessed on 24 June 2021).
- Cornacchia, S.; Errico, R.; La Tegola, L.; Maldera, A.; Simeone, G.; Fusco, V.; Niccoli-Asabella, A.; Rubini, G.; Guglielmi, G. The new lens dose limit: Implication for occupational radiation protection. Radiol. Med. 2019, 124, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Italian Society of Medical and Interventional Radiology (SIRM). 2020. Available online: https://www.sirm.org/en/italian-society-of-medical-and-interventional-radiology/ (accessed on 11 May 2020).
- Radiological Society of North America (RSNA). 2020. Available online: https://www.kaggle.com/c/rsna-pneumonia-detection-challenge/data (accessed on 11 May 2020).
- Kaggle’s Chest X-ray Images (Pneumonia) Dataset. 2020. Available online: https://www.kaggle.com/paultimothymooney/chest-xray-pneumonia (accessed on 11 May 2020).
- Ozcan, T. A new composite approach for COVID-19 detection in X-ray images using deep features. Appl. Soft Comput. 2021, 111, 107669. [Google Scholar] [CrossRef]
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Acharya, U.R. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput. Biol. Med. 2020, 121, 103792. [Google Scholar] [CrossRef] [PubMed]
- Du, R.; Tsougenis, E.D.; Ho, J.W.K.; Chan, J.K.Y.; Chiu, K.W.H.; Fang, B.X.H.; Ng, M.Y.; Leung, S.-T.; Lo, C.S.Y.; Wong, H.-Y.F.; et al. Machine learning application for the prediction of SARS-CoV-2 infection using blood tests and chest radiograph. Sci. Rep. 2021, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Dey, S.; Bhattacharya, R.; Malakar, S.; Mirjalili, S.; Sarkar, R. Choquet fuzzy integral-based classifier ensemble technique for COVID-19 detection. Comput. Biol. Med. 2021, 135, 104585. [Google Scholar] [CrossRef] [PubMed]
- Alruwaili, M.; Shehab, A.; El-Ghany, S.A. COVID-19 Diagnosis Using an Enhanced Inception-ResNetV2 Deep Learning Model in CXR Images. J. Health Eng. 2021, 2021, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.U.; Bukhari, S.S.; Syed, A.; Shah, S.S. The Diagnostic Evaluation of Convolutional Neural Network (CNN) for the Assessment of Chest X-ray of Patients Infected with COVID-19; medRxiv: Long Island, NY, USA, 2020. [Google Scholar]
- Khan, A.I.; Shah, J.L.; Bhat, M.M. CoroNet: A deep neural network for detection and diagnosis of COVID-19 from chest x-ray images. Comput. Methods Programs Biomed. 2020, 196, 105581. [Google Scholar] [CrossRef] [PubMed]
- Hemdan, E.E.-D.; Shouman, M.A.; Karar, M.E. COVIDx-Net: A Framework of Deep Learning Classifiers to Diagnose COVID-19 in X-ray Images. 2020. Available online: http://arxiv.org/abs/2003.11055 (accessed on 24 June 2021).
- Ouchicha, C.; Ammor, O.; Meknassi, M. CVDNet: A novel deep learning architecture for detection of coronavirus (Covid-19) from chest x-ray images. Chaos Solitons Fractals 2020, 140, 110245. [Google Scholar] [CrossRef]
- Ko, H.; Chung, H.; Kang, W.S.; Kim, K.W.; Shin, Y.; Kang, S.J.; Lee, J.H.; Kim, Y.J.; Kim, N.Y.; Jung, H.; et al. COVID-19 Pneumonia Diagnosis Using a Simple 2D Deep Learning Framework With a Single Chest CT Image: Model Development and Validation. J. Med. Internet Res. 2020, 22, e19569. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.; Kay, F.; Tan, J.; Yan, Y.; Ng, Y.S.; Iyengar, P.; Peshock, R.; Jiang, S. Deep Learning–Based COVID-19 Pneumonia Classification Using Chest CT Images: Model Generalizability. Front. Artif. Intell. 2021, 4, 694875. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Zheng, S.; Li, L.; Zhang, X.; Zhang, X.; Huang, Z.; Chen, J.; Wang, R.; Zhao, H.; Zha, Y.; et al. Deep learning Enables Accurate Diagnosis of Novel Coronavirus (COVID-19) with CT images. IEEE/ACM Trans. Comput. Biol. Bioinform. 2021, 3, PP. [Google Scholar] [CrossRef]
- Xu, X.; Jiang, X.; Ma, C.; Du, P.; Li, X.; Lv, S.; Yu, L.; Ni, Q.; Chen, Y.; Su, J.; et al. A Deep Learning System to Screen Novel Coronavirus Disease 2019 Pneumonia. Engineering 2020, 6, 1122–1129. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Methodology | Imaging Modality | Dataset | Limits | Classification Problem | Classification Model | Accuracy [%] | Specificity [%] | Precision [%] | Area Under ROC Curve |
|---|---|---|---|---|---|---|---|---|---|---|
| Sethy et al. | deep learning | CXR | Firt dataset: 25 number of COVID-19+ and 25 number of COVID-19- X-ray images. Second dataset: 133 X-ray images of COVID-19+, including MERS, SARS, and ARDS and 133 chest X-ray images as COVID-19- | Number of patients. Moreover, the limitation of this methodology is that if the patient is in a critical situation and unable to attend for CXR scanning. The model is limited to classify the input chest X-ray image into only two classes either normal or COVID-19 | COVID-19 detection | resnet50 plus Support Vector Machine | 95.38 | |||
| Jiao et al. | deep learning | CXR | 1834 patients were identified and assigned to the model training (n = 1285), validation (n = 183), or testing (n = 366) sets. The number of patients that were identified for external testing of the model were 475. | The artificial intelligence model showed decreased performance on the external testing set relative to the internal testing set, indicating that generalization might not be possible. This finding could have been due to several factors, including heterogeneous data and image acquisition between the different hospital systems. The model is limited to classifying the input chest X-ray image into only two classes either normal or COVID-19 | predict the binary outcome of COVID-19 disease severity (critical or non-critical) | EfficientNet deep neural network and clinical data | 0.85 on internal testing and 0.80 on external testing | |||
| Al-Waisy et al. | deep learning | CXR | 200 X-ray images with confirmed COVID-19 infection come by Cohen’s GitHub database [58]; 200 COVID-19 CXR gathered from three different repository: Radiopaedia dataset [59], Italian Society of Medical and Interventional Radiology (SIRM) [60], and Radiological Society of North America (RSNA) [61]; 400 normal CXR by Kaggle’s CXR dataset [62] | Cases used in this study come from different databases. The model is limited to classifying the input chest X-ray image into only two classes, either normal or COVID-19 | COVID-19 detection | COVID-CheXNet system made by combining the results generated from two different deep learning models | 99.99 | 100 | 100 | |
| Ozcan et al. | deep learning | CXR | 127 X-ray images diagnosed with COVID-19, 500 no-findings and 500 pneumonia class | No external testing of the model and the patient number is low for multi class classification | COVID-19 versus no findings classification/multi-class classification COVID-19 versus no findings versus pneumonia | single layer-based (SLB) and a feature fusion based (FFB) composite systems using deep features | 99.52/87.64 | 98.03/99.7 | ||
| Ozturk et al. | deep learning | CXR | 127 X-ray images diagnosed with COVID-19, 500 no-findings and 500 pneumonia class | No external testing of the model and the patient number is low for multi class classification | COVID-19 versus no findings classification/multi-class classification COVID-19 versus no findings versus pneumonia | DarkNet model implementing 17 convolutional layers and introducing different filtering on each layer | 98.08/87.02 | 98.03/89.96 | ||
| Du et al. | machine learning | CXR | 447 cases with COVID-19; 405 with other viral PNA, 1515 with bacterial PNA, 1862 with Clinical PNA, 256 with other infections and 663 with other diseases | The model has a moderate specificity | COVID-19 detection | 68.4 | ||||
| Dey et al. | classifier ensemble technique | CXR | A total of 506 viral lung infection cases including 468 cases with COVID-19;46 bacterial lung infection and 26 fungal lung infection by https://github.com/ieee8023/covid-chestxray-dataset.; 1583 normal CXR and 4273 COVID-19+ CXR by https://www.kaggle.com/paultimothymooney/chest-xray-pneumonia/version/2. | No external testing of the model and patient number. | classification of Normal, COVID-19, and Pneumonia cases | Choquet fuzzy integral using two dense layers and one softmax layer | 99.02 | 99 | ||
| Alruwaili et al. | deep learning | CXR | 2905 CXR images, which are distributed into 219 COVID-19 images, 1345 viral pneumonia images, and 1341 for normal category | No external testing of the model and patient number. | COVID-19 vs. normal vs. viral pneumonia classification | Inception-ResNetV2 deep learning model | 99.83 | 98.11 | ||
| Bukhari et al. | deep learning | CXR | 93 CXR which have no radiological abnormality; 96 CXR with the radiological features of pneumonia different from COVID-19 infection; 89 digital images of chest X-rays of patients diagnosed with COVID-19 infection | The model takes a roughly higher training and testing run time compared to other models due to the complex structure of the inside modules. | healthy normal, bacterial pneumonia, viral pneumonia, and COVID-19 classification | resnet50 | 98.18 | 98.14 | ||
| Khan et al. | deep learning | CXR | 1203 normal, 660 bacterial Pneumonia and 931 viral Pneumonia cases | Small prepared dataset which indicates that given more data, the proposed model can achieve better results with minimum pre-processing of data | viral pneumonia, COVID-19, bacterial pneumonia, and normal classification/normal, COVID-19, and pneumonia classification | CoroNet: pretrained Xception convolution network | 89.6/95.0 | |||
| Hemdan et al. | deep learning | CXR | 25 normal cases and 25 positive COVID-19 images | The model is limited to classifying the input chest X-ray image into only two classes, either normal or COVID-19. Another limit is the number of patients | COVID-19 detection | InceptionV3, MobileNetV2, VGG19, DenseNet201, Inception-ResNetV2, ResNetV2, and Xception model | 90 | 83 | ||
| Sethy and Behera | deep learning and machine learning | CXR | 25 normal cases and 25 positive COVID-19 images | The model is limited to classifying the input chest X-ray image into only two classes, either normal or COVID-19 | detecting COVID-19 (ignoring SARS, MERS and ARDS) | deep learning for feature extraction and support vector machine (SVM) for classification | 95.38 | |||
| Ouchicha et al. | deep learning | CXR | 219 COVID-19, 1341 normal and 1345 viral pneumonia | The model has been trained on a small dataset of few images of various COVID-19, viral pneumonia and normal cases from publically available database | classification of Normal, COVID-19, and Pneumonia cases | local and global features of CXR using two parallel layers with reaching various kernel sizes | 97.2 | |||
| Gozes et al. | deep learning | CT | 106 COVID-19 chest CT scans and 99 normal ones | Patient number is low | COVID-19 versus no COVID-19 | robust 2D and 3D deep learning models | 0.948 | |||
| Wang et al. [63] | deep learning | CT | 740 for COVID-19 negative and 325 for COVID-19 positive | Sample size was relatively small | COVID-19 versus no COVID-19 | GoogleNet Inception v3 convolution neural network | 89.5 | 88 | ||
| Li et al. | deep learning | CT | 1292 with COVID-19, 1735 for community-acquired pneumonia, and 1325 for non-pneumonia abnormalities | The model is limited to classifying the input chest X-ray image into only two classes, either normal or COVID-19 | COVID-19 versus no COVID-19 | resnet50 | 90 | 0.96 | ||
| Ko et al. | deep learning | CT | 1194 chest CT COVID-19 images and 1357 chest CT images with non–COVID-19 pneumonia | The model is limited to classifying the input chest X-ray image into only two classes, either normal or COVID-19 | Classification of COVID-19 patients | FCONet developed by transfer learning using one of four state-of-the-art pretrained deep learning models (VGG16, ResNet-50, Inception-v3, or Xception) | 99.87 | 100 | ||
| Nguyen et al. | deep learning | CT | 101 with COVID-19, 118 with common Pneumonia and 118 for non-pneumonia abnormalities | Patient number is low for three classes classification | normal, COVID-19, and pneumonia classification | convolutional neural network | 87 | 0.83 | ||
| 1544 with COVID-19, 1556 with common Pneumonia and 118 for non-pneumonia abnormalities | 97 | 0.99 | ||||||||
| 281 with COVID-19 and 1068 for non-pneumonia abnormalities | 86 | 0.87 | ||||||||
| Zhang et al. [64] | CT | CT | There were 406 clearer COVID-19-positive lung CT images. The marked areas in the mask images are 0-“ground glass opacity,” 1-“consolidations,” 2-“lungs other,” 3-“background. | The complexity of the model and the number of patients | segment ground glass opaque lesions in COVID-19 lung CT images | COVSeg-NET model is based on the fully convolutional neural network model structure, which mainly includes convolutional layer, nonlinear unit activation function, maximum pooling layer, batch normalization layer, merge layer, flattening layer, sigmoid layer, and so forth | 100 | |||
| Song et al. | deep learning | CT | A total of 88 patients diagnosed with the COVID-19, 101 patients infected with bacteria pneumonia, and 86 healthy persons | Patient number is low for a three classes classification | normal verus COVID-19 classification/discriminating COVID-19 patients from others | resnet50 | 96/86 | 0.99/0.95 | ||
| Wang et al. [65] | machine learning | CT | A total of 1051 patients with RT-PCR confirmed COVID-19 and chest CT was included in this study | Patient selection bias, retrospective and multi-institutional nature of the study. | for prediction of COVID-19 progression using CT imaging and clinical data | 78 | 80 | |||
| Xu et al. | deep learning | CT | A total of 618 CT samples were collected: 219 samples from 110 patients with COVID-19 and 224 samples from 224 patients with influenza-A viral pneumonia (IAVP) | Patient selection bias, patient number is low | early screening model to distinguish COVID-19 from IAVP and healthy cases through pulmonary CT images | 3D deep learning network that consists of four basic stages, which are pre-processing, candidate region segmentation, classification | 86.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fusco, R.; Grassi, R.; Granata, V.; Setola, S.V.; Grassi, F.; Cozzi, D.; Pecori, B.; Izzo, F.; Petrillo, A. Artificial Intelligence and COVID-19 Using Chest CT Scan and Chest X-ray Images: Machine Learning and Deep Learning Approaches for Diagnosis and Treatment. J. Pers. Med. 2021, 11, 993. https://doi.org/10.3390/jpm11100993
Fusco R, Grassi R, Granata V, Setola SV, Grassi F, Cozzi D, Pecori B, Izzo F, Petrillo A. Artificial Intelligence and COVID-19 Using Chest CT Scan and Chest X-ray Images: Machine Learning and Deep Learning Approaches for Diagnosis and Treatment. Journal of Personalized Medicine. 2021; 11(10):993. https://doi.org/10.3390/jpm11100993
Chicago/Turabian StyleFusco, Roberta, Roberta Grassi, Vincenza Granata, Sergio Venanzio Setola, Francesca Grassi, Diletta Cozzi, Biagio Pecori, Francesco Izzo, and Antonella Petrillo. 2021. "Artificial Intelligence and COVID-19 Using Chest CT Scan and Chest X-ray Images: Machine Learning and Deep Learning Approaches for Diagnosis and Treatment" Journal of Personalized Medicine 11, no. 10: 993. https://doi.org/10.3390/jpm11100993