
A Clinical-Genetic Score for Predicting Weight Loss after Bariatric Surgery: The OBEGEN Study

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Statement on Ethics
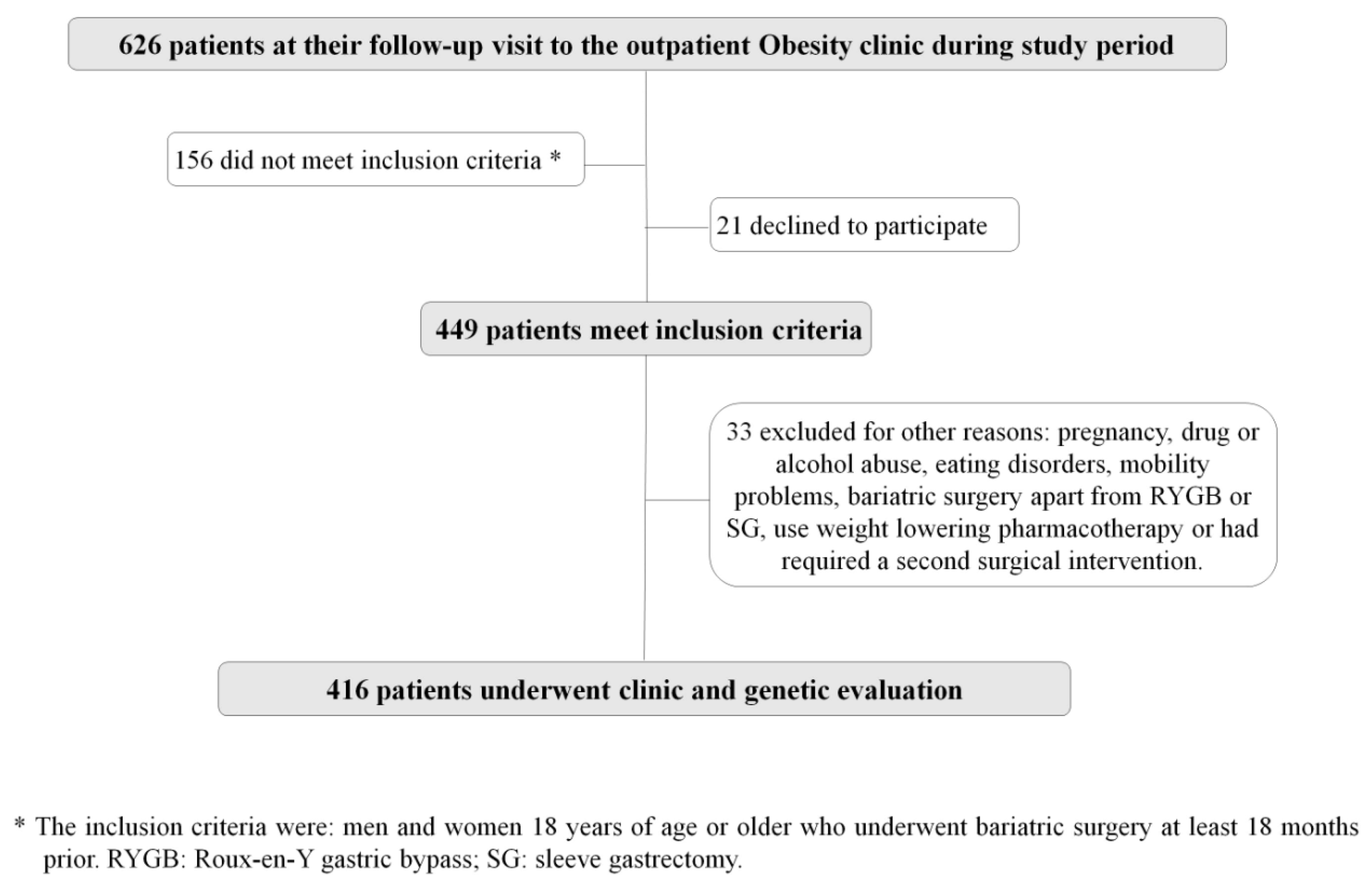
2.2. Study Design and Description of the Study Population
2.3. Outcome Weight Measures
2.4. Genotyping
2.5. Statistical Methods
3. Results
3.1. Baseline Characteristics of Patients
3.2. Construction of a Clinical Risk Score
3.3. Construction of a Genetic Risk Score
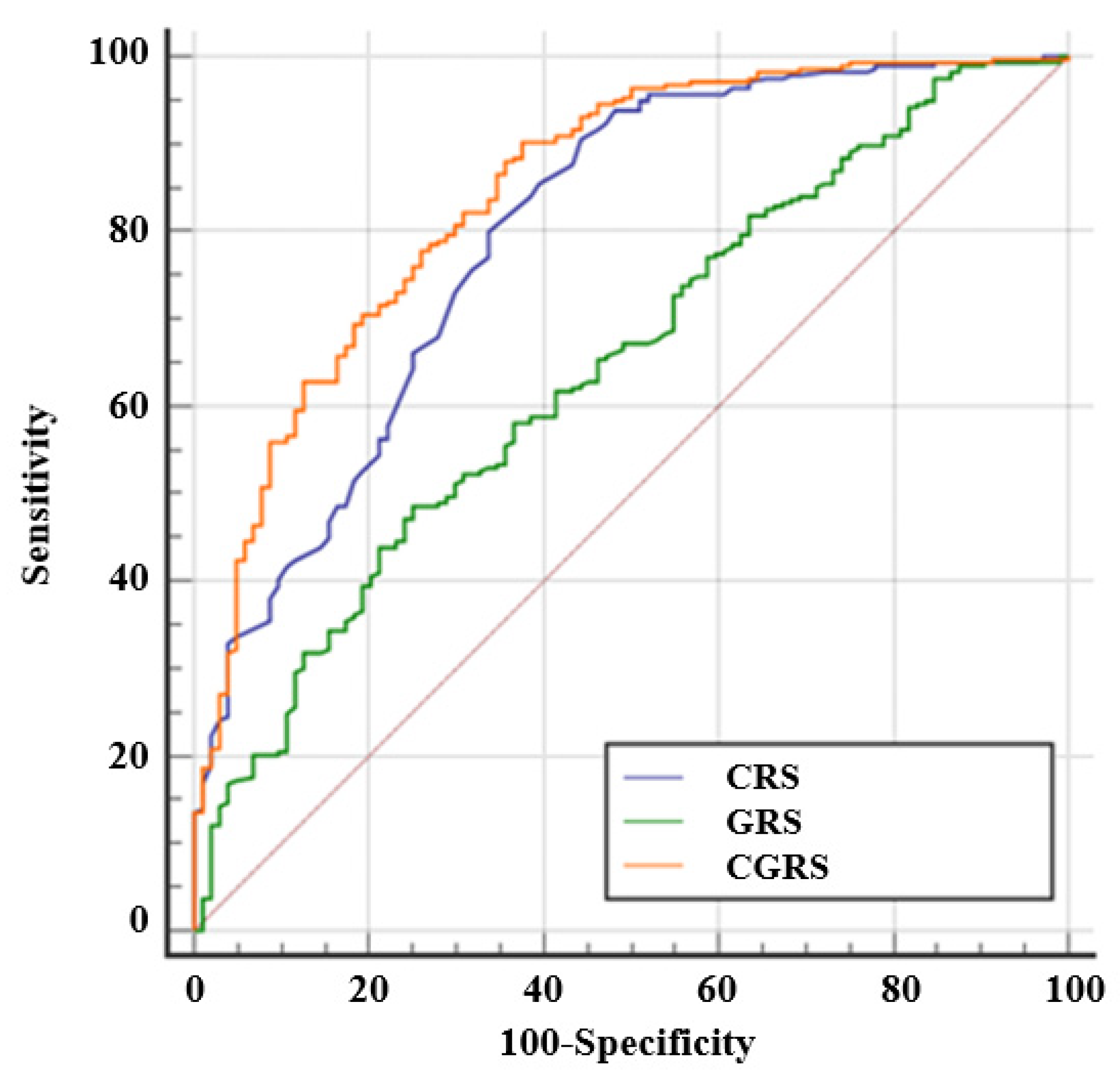
3.4. Construction of the OBEGEN Clinical-Genetic Risk Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Locke, A.; Kahali, B.; Berndt, S.I.; Justice, A.E.; Pers, T.; Day, F.; Powell, C.; Vedantam, S.; Buchkovich, M.L.; Yang, J.; et al. Genetic studies of body mass index yield new insights for obesity biology. Nat. Cell Biol. 2015, 518, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Null, N. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef] [Green Version]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Vitiello, A.; Higa, K.; Himpens, J.; Buchwald, H.; Scopinaro, N. IFSO Worldwide Survey 2016: Primary, Endoluminal, and Revisional Procedures. Obes. Surg. 2018, 28, 3783–3794. [Google Scholar] [CrossRef] [PubMed]
- Sarabu, N. Weight and Metabolic Outcomes 12 Years after Gastric Bypass. N. Engl. J. Med. 2018, 378, 93–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalewski, P.K.; Olszewski, R.; Walędziak, M.; Janik, M.; Kwiatkowski, A.; Gałązka-Świderek, N.; Cichoń, K.; Brągoszewski, J.; Paśnik, K. Long-Term Outcomes of Laparoscopic Sleeve Gastrectomy—A Single-Center, Retrospective Study. Obes. Surg. 2017, 28, 130–134. [Google Scholar] [CrossRef]
- Roth, A.E.; Thornley, C.J.; Blackstone, R.P. Outcomes in Bariatric and Metabolic Surgery: An Updated 5-Year Review. Curr. Obes. Rep. 2020, 9, 380–389. [Google Scholar] [CrossRef]
- Karlsson, J.; Taft, C.; Rydén, A.; Sjöström, L.; Sullivan, M. Ten-year trends in health-related quality of life after surgical and conventional treatment for severe obesity: The SOS intervention study. Int. J. Obes. 2007, 31, 1248–1261. [Google Scholar] [CrossRef] [Green Version]
- Kubik, J.F.; Gill, R.S.; Laffin, M.; Karmali, S. The Impact of Bariatric Surgery on Psychological Health. J. Obes. 2013, 2013, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Still, C.D.; Wood, G.C.; Chu, X.; Erdman, R.; Manney, C.H.; Benotti, P.N.; Petrick, A.T.; Strodel, W.E.; Mirshahi, U.L.; Mirshahi, T.; et al. High Allelic Burden of Four Obesity SNPs Is Associated With Poorer Weight Loss Outcomes Following Gastric Bypass Surgery. Obesity 2011, 19, 1676–1683. [Google Scholar] [CrossRef]
- Livhits, M.; Mercado, C.; Yermilov, I.; Parikh, J.A.; Dutson, E.; Mehran, A.; Ko, C.Y.; Gibbons, M.M. Preoperative Predictors of Weight Loss Following Bariatric Surgery: Systematic Review. Obes. Surg. 2011, 22, 70–89. [Google Scholar] [CrossRef]
- Aliakbarian, H.; Bhutta, H.Y.; Heshmati, K.; Kunju, S.U.; Sheu, E.G.; Tavakkoli, A. Pre-operative Predictors of Weight Loss and Weight Regain Following Roux-en-Y Gastric Bypass Surgery: A Prospective Human Study. Obes. Surg. 2020, 30, 4852–4859. [Google Scholar] [CrossRef]
- Kitamura, R.; Chen, R.; Trickey, A.; Eisenberg, D. Positive and Negative Independent Predictive Factors of Weight Loss After Bariatric Surgery in a Veteran Population. Obes. Surg. 2020, 30, 2124–2130. [Google Scholar] [CrossRef]
- Moustafa, J.S.E.-S.; Froguel, P. From obesity genetics to the future of personalized obesity therapy. Nat. Rev. Endocrinol. 2013, 9, 402–413. [Google Scholar] [CrossRef]
- Pigeyre, M.; Yazdi, F.T.; Kaur, Y.; Meyre, D. Recent progress in genetics, epigenetics and metagenomics unveils the pathophysiology of human obesity. Clin. Sci. 2016, 130, 943–986. [Google Scholar] [CrossRef] [Green Version]
- Bray, M.S.; Loos, R.; McCaffery, J.; Ling, C.; Franks, P.; Weinstock, G.; Snyder, M.P.; Vassy, J.; Agurs-Collins, T.; The Conference Working Group. NIH working group report—Using genomic information to guide weight management: From universal to precision treatment. Obesity 2015, 24, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciudin, A.; Fidilio, E.; Ortiz, A.; Pich, S.; Salas, E.; Mesa, J.; Hernández, C.; Simó-Servat, O.; Lecube, A.; Simó, R. Genetic Testing to Predict Weight Loss and Diabetes Remission and Long-Term Sustainability after Bariatric Surgery: A Pilot Study. J. Clin. Med. 2019, 8, 964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Listed, N. 1983 metropolitan height and weight tables. Stat. Bull. Metrop. Life Found. 1983, 64, 3–9. [Google Scholar]
- Grover, B.T.; Morell, M.C.; Kothari, S.N.; Borgert, A.J.; Kallies, K.J.; Baker, M.T. Defining Weight Loss After Bariatric Surgery: A Call for Standardization. Obes. Surg. 2019, 29, 3493–3499. [Google Scholar] [CrossRef]
- Mirshahi, U.L.; Still, C.D.; Masker, K.K.; Gerhard, G.S.; Carey, D.J.; Mirshahi, T. TheMC4R(I251L) Allele Is Associated with Better Metabolic Status and More Weight Loss after Gastric Bypass Surgery. J. Clin. Endocrinol. Metab. 2011, 96, E2088–E2096. [Google Scholar] [CrossRef] [Green Version]
- Moleres, A.; Rendo-Urteaga, T.; Zulet, M.A.; Marcos, A.; Campoy, C.; Garagorri, J.M.; Martínez, J.A.; Azcona-Sanjulián, M.C.; Marti, A. Obesity Susceptibility Loci on Body Mass Index and Weight Loss in Spanish Adolescents after a Lifestyle Intervention. J. Pediatr. 2012, 161, 466–470.e2. [Google Scholar] [CrossRef]
- Blakemore, A.I.F.; Froguel, P. Investigation of Mendelian forms of obesity holds out the prospect of personalized medicine. Ann. N. Y. Acad. Sci. 2010, 1214, 180–189. [Google Scholar] [CrossRef]
- Welter, D.; MacArthur, J.; Morales, J.; Burdett, A.; Hall, P.; Junkins, H.; Klemm, A.; Flicek, P.; Manolio, T.; Hindorff, L.; et al. The NHGRI GWAS Catalog, a curated resource of SNP-trait associations. Nucleic Acids Res. 2013, 42, D1001–D1006. [Google Scholar] [CrossRef]
- Parri, A.; Benaiges, D.; Schröder, H.; Izquierdo-Pulido, M.; Ramón, J.; Villatoro, M.; Roux, J.F.-L.; Goday, A. Preoperative Predictors of Weight Loss at 4 Years Following Bariatric Surgery. Nutr. Clin. Pr. 2015, 30, 420–424. [Google Scholar] [CrossRef]
- Gerken, A.L.H.; Rohr-Kräutle, K.-K.; Weiss, C.; Seyfried, S.; Reissfelder, C.; Vassilev, G.; Otto, M. Handgrip Strength and Phase Angle Predict Outcome After Bariatric Surgery. Obes. Surg. 2020, 31, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.S.; Christensen, B.J.; Schmidt, J.B.; Tækker, L.; Holm, L.; Lunn, S.; Ritz, C.; Albrechtsen, N.J.W.; Holst, J.J.; Schnurr, T.M.; et al. Predictors of weight loss after bariatric surgery—A cross-disciplinary approach combining physiological, social, and psychological measures. Int. J. Obes. 2020, 44, 2291–2302. [Google Scholar] [CrossRef] [PubMed]
- Cottam, S.; Cottam, D.; Cottam, A. Sleeve Gastrectomy Weight Loss and the Preoperative and Postoperative Predictors: A Systematic Review. Obes. Surg. 2019, 29, 1388–1396. [Google Scholar] [CrossRef]
- McCaffery, J.M. Precision behavioral medicine: Implications of genetic and genomic discoveries for behavioral weight loss treatment. Am. Psychol. 2018, 73, 1045–1055. [Google Scholar] [CrossRef]
- Sarzynski, M.A.; Jacobson, P.; Rankinen, T.; Carlsson, B.; Sjöström, L.; Bouchard, C.; Carlsson, L.M.S. Associations of markers in 11 obesity candidate genes with maximal weight loss and weight regain in the SOS bariatric surgery cases. Int. J. Obes. 2010, 35, 676–683. [Google Scholar] [CrossRef] [Green Version]
- Velázquez-Fernández, D.; Mercado-Celis, G.; Flores-Morales, J.; Clavellina-Gaytán, D.; Vidrio, R.; Vidrio, E.; Mosti, M.; Sánchez-Aguilar, H.; Rodriguez, D.; León, P.; et al. Analysis of Gene Candidate SNP and Ancestral Origin Associated to Obesity and Postoperative Weight Loss in a Cohort of Obese Patients Undergoing RYGB. Obes. Surg. 2016, 27, 1481–1492. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, G.K.; Resende, C.M.; Durso, D.F.; Rodrigues, L.A.; Silva, J.L.P.; Reis, R.C.; Pereira, S.S.; Ferreira, D.C.; Franco, G.R.; Alvarez-Leite, J. A single FTO gene variant rs9939609 is associated with body weight evolution in a multiethnic extremely obese population that underwent bariatric surgery. Nutrition 2015, 31, 1344–1350. [Google Scholar] [CrossRef]
- Balasar, Ö.; Çakır, T.; Erkal, Ö.; Aslaner, A.; Cekic, B.; Uyar, M.; Bülbüller, N.; Oruç, M.T. The effect of rs9939609 FTO gene polymorphism on weight loss after laparoscopic sleeve gastrectomy. Surg. Endosc. 2015, 30, 121–125. [Google Scholar] [CrossRef]
- Kops, N.L.; Vivan, M.A.; Horvath, J.D.C.; de Castro, M.L.D.; Friedman, R. FABP2, LEPR223, LEP656, and FTO Polymorphisms: Effect on Weight Loss 2 Years After Bariatric Surgery. Obes. Surg. 2018, 28, 2705–2711. [Google Scholar] [CrossRef]
- Bandstein, M.; Voisin, S.; Nilsson, E.K.; Schultes, B.; Ernst, B.; Thurnheer, M.; Benedict, C.; Mwinyi, J.; Schiöth, H.B. A Genetic Risk Score is Associated with Weight Loss Following Roux-en Y Gastric Bypass Surgery. Obes. Surg. 2016, 26, 2183–2189. [Google Scholar] [CrossRef] [Green Version]
- Aasbrenn, M.; Schnurr, T.; Have, C.T.; Svendstrup, M.; Hansen, D.L.; Worm, D.; Balslev-Harder, M.; Hollensted, M.; Grarup, N.; Burgdorf, K.S.; et al. Genetic Determinants of Weight Loss after Bariatric Surgery. Obes. Surg. 2019, 29, 2554–2561. [Google Scholar] [CrossRef]
- Katsareli, E.A.; Amerikanou, C.; Rouskas, K.; Dimopoulos, A.; Diamantis, T.; Alexandrou, A.; Griniatsos, J.; Bourgeois, S.; Dermitzakis, E.; Ragoussis, J.; et al. A Genetic Risk Score for the Estimation of Weight Loss After Bariatric Surgery. Obes. Surg. 2020, 30, 1482–1490. [Google Scholar] [CrossRef]
- Peters, K.; Beilby, J.; Cadby, G.; Warrington, N.M.; Bruce, D.G.; Davis, W.A.; Davis, T.M.; Wiltshire, S.; Knuiman, M.; McQuillan, B.M.; et al. A comprehensive investigation of variants in genes encoding adiponectin (ADIPOQ) and its receptors (ADIPOR1/R2), and their association with serum adiponectin, type 2 diabetes, insulin resistance and the metabolic syndrome. BMC Med. Genet. 2013, 14, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyriakou, T.; Collins, L.J.; Spencer-Jones, N.J.; Malcolm, C.; Wang, X.; Snieder, H.; Swaminathan, R.; Burling, K.A.; Hart, D.J.; Spector, T.D.; et al. Adiponectin gene ADIPOQ SNP associations with serum adiponectin in two female populations and effects of SNPs on promoter activity. J. Hum. Genet. 2008, 53, 718–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gholami, M.; Sharifi, F.; Shahriari, S.; Khoshnevisan, K.; Larijani, B.; Amoli, M.M. Association of interleukin-6 polymorphisms with obesity: A systematic review and meta-analysis. Cytokine 2019, 123, 154769. [Google Scholar] [CrossRef]
- Razquin, C.; Martinez, J.A.; Martinez-Gonzalez, M.A.; Fernández-Crehuet, J.; Santos, J.M.; Marti, A. A Mediterranean diet rich in virgin olive oil may reverse the effects of the −174G/C IL6 gene variant on 3-year body weight change. Mol. Nutr. Food Res. 2010, 54, S75–S82. [Google Scholar] [CrossRef] [PubMed]
- Delahanty, L.M.; Pan, Q.; Jablonski, K.A.; Watson, K.E.; McCaffery, J.; Shuldiner, A.; Kahn, S.E.; Knowler, W.C.; Florez, J.C.; Franks, P.W.; et al. Genetic Predictors of Weight Loss and Weight Regain After Intensive Lifestyle Modification, Metformin Treatment, or Standard Care in the Diabetes Prevention Program. Diabetes Care 2011, 35, 363–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soenen, S.; Mariman, E.C.; Vogels, N.; Bouwman, F.G.; Hoed, M.D.; Brown, L.; Westerterp-Plantenga, M.S. Relationship between perilipin gene polymorphisms and body weight and body composition during weight loss and weight maintenance. Physiol. Behav. 2009, 96, 723–728. [Google Scholar] [CrossRef]
- Garaulet, M.; Vera, B.; Bonnet-Rubio, G.; Gómez-Abellán, P.; Lee, Y.-C.; Ordovás, J.M. Lunch eating predicts weight-loss effectiveness in carriers of the common allele at PERILIPIN1: The ONTIME (Obesity, Nutrigenetics, Timing, Mediterranean) study. Am. J. Clin. Nutr. 2016, 104, 1160–1166. [Google Scholar] [CrossRef] [Green Version]
- Tan, C.Y.; Virtue, S.; Bidault, G.; Dale, M.; Hagen, R.; Griffin, J.L.; Vidal-Puig, A. Brown Adipose Tissue Thermogenic Capacity Is Regulated by Elovl6. Cell Rep. 2015, 13, 2039–2047. [Google Scholar] [CrossRef] [Green Version]
- Akbarian, S.-A.; Salehi-Abargouei, A.; Pourmasoumi, M.; Kelishadi, R.; Nikpour, P.; Heidari-Beni, M. Association of Brain-derived neurotrophic factor gene polymorphisms with body mass index: A systematic review and meta-analysis. Adv. Med. Sci. 2018, 63, 43–56. [Google Scholar] [CrossRef]
- Fox, C.S.; Heard-Costa, N.; Cupples, L.A.; Dupuis, J.; Vasan, R.S.; Atwood, L.D. Genome-wide association to body mass index and waist circumference: The Framingham Heart Study 100K project. BMC Med. Genet. 2007, 8, S18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benzinou, M.; Chèvre, J.-C.; Ward, K.J.; Lecoeur, C.; Dina, C.; Lobbens, S.; Durand, E.; Delplanque, J.; Horber, F.F.; Heude, B.; et al. Endocannabinoid receptor 1 gene variations increase risk for obesity and modulate body mass index in European populations. Hum. Mol. Genet. 2008, 17, 1916–1921. [Google Scholar] [CrossRef] [Green Version]
- Yu, K.; Li, L.; Zhang, L.; Guo, L.; Wang, C. Association between MC4R rs17782313 genotype and obesity: A meta-analysis. Gene 2020, 733, 144372. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Gene | Name | Chromosome Allocation of Human Ortholog | SNP |
|---|---|---|---|
| ACE | angiotensin I converting enzyme | 17q23.3 | rs4343 |
| ADIPOQ | adiponectin, C1Q and collagen domain containing | 3q27.3. | rs16861209 rs2241766 |
| ADRB3 | adrenoceptor beta 3 | 8p11.23. | rs4994 rs9693898 |
| AGRP | Agouti related neuropeptide | 16q22.1 | rs11575892 * |
| AGTR1 | angiotensin II receptor type 1 | 3q24. | rs5186 |
| APOA2 | apolipoprotein A2 | 11q23.3. | rs5082 |
| APOA5 | apolipoprotein A5 | 11q23.3. | rs651821 |
| APOC3 | apolipoprotein C3 | 11q23.3. | CD010 |
| BDNF | brain derived neurotrophic factor | 11p14.1. | rs6265 rs925946 |
| CCDC93 | coiled-coil domain containing 93 | 2q14.1 | rs10490628 * |
| CDKAL1 | CDK5 regulatory subunit associated protein 1 like 1 | 6p22.3. | rs7754840 |
| CDKN2B | cyclin dependent kinase inhibitor 2B | 9p21.3. | rs10811661 |
| CLOCK | clock circadian regulator | 4q12. | rs4580704 rs4864548 |
| CNR1 | cannabinoid receptor 1 | 6q15 | rs6454674 * |
| ELOVL6 | ELOVL fatty acid elongase 6 | 4q25. | rs682447 |
| ESR1 | estrogen receptor 1 | 6q25.1 | rs3778099 * |
| FTO | fat mass and obesity associated | 16q12.2. | rs9939609 |
| GHRL | ghrelin and obestatin prepropeptide | 3p25.3. | rs696217 |
| IGF2 | insulin like growth factor 2 | 11p15.5 | rs680 * |
| INSIG2 | insulin induced gene 2 | 2q14.1. | rs7566605 rs3771942 * |
| IL-1B | interleukin 1 beta | 2q14.1 | rs1143643 * |
| IL6 | interleukin 6 | 7p15.3. | rs1800795 |
| LEP | leptin | 7q32.1. | rs12535708 |
| LEPR | leptin receptor | 1p31.3. | rs1137100 |
| LPL | lipoprotein lipase | 8p.22. | rs328 |
| MC4R | melanocortin 4 receptor | 18q21.32. | rs12970134 rs52820871 rs17700633 rs2229616 rs17782313 |
| MTCH2 | mitochondrial carrier 2 | 11p11.2. | rs10838738 |
| NEGR1 | neuronal growth regulator 1 | 1p31.1 | rs2568958 * |
| PLIN1 | perilipin 1 | 15q26.1. | rs1052700 rs894160 |
| PPARA | peroxisome proliferator activated receptor alpha | 22q13.31. | rs1800206 |
| PPARG | peroxisome proliferator activated receptor gamma | 3p25.2. | rs1801282 |
| PCSK1 | proprotein convertase subtilisin/kexin type 1 | 5q15. | rs6235 |
| PON1 | paraoxonase 1 | 7q21.3. | CD014 |
| SIRT1 | sirtuin 1 | 10q21.3 | rs7069102 * |
| TCF7L2 | transcription factor 7 like 2 | 10q25.2. | rs7903146 |
| TMEM18 | transmembrane protein 18 | 2p25.3 | rs2867125 * |
| UCP1 | uncoupling protein 1 | 4q31.2 | rs45539933 * |
| UCP2 | uncoupling protein 2 | 11q13.4. | rs659366 |
| UCP3 | uncoupling protein 3 | 11q13.4. | rs1800849 |
| WFS1 | wolframin ER transmembrane glycoprotein | 4p16.1. | rs10010131 |
| Total | %EWL > 50% | %EWL ≤ 50% | p | |
|---|---|---|---|---|
| Patients, n (%) | 416 | 301 (72.3) | 115 (27.6) | <0.001 |
| Female, n (%) | 348 (83.6) | 260 (86.3) | 88 (76.5) | <0.001 |
| Age (yrs) | 48.3 ± 10.3 | 49.0 ± 10.4 | 51.5 ± 9.2 | 0.003 |
| SG, n (%) | 137 (32.9) | 105 (34.8) | 32 (27.8) | <0.001 |
| RYGB, n (%) | 280 (67.3) | 218 (72.4) | 62 (53.9) | <0.001 |
| Initial BMI (Kg/m2) | 44.3 ± 7.9 | 44.5 ± 9.6 | 44.2 ± 7.3 | 0.554 |
| Initial weight (Kg) | 113.0 ± 18.4 | 112.3 ± 20.3 | 113.4 ± 13.8 | 0.361 |
| Excess weight (Kg) | 49.3 ± 17.3 | 48.7 ± 19.2 | 51.3 ± 12.2 | 0.020 |
| Nadir BMI (Kg/m2) | 29.9 ± 5.8 | 28.5 ± 4.5 | 37.0 ± 6.8 | <0.001 |
| Type 2 diabetes, n (%) | 173 (41.5) | 128 (42.5) | 45 (39.1) | <0.001 |
| Hypertension (%) | 286 (68.7) | 204 (67.7) | 82 (71.3) | <0.001 |
| Dyslipidemia (%) | 306 (73.5) | 212 (70.4) | 94 (81.7) | 0.010 |
| Sleep apnea (%) | 116 (27.8) | 88 (29.2) | 28 (24.3) | <0.001 |
| Clinical Variables | Genetic Variants | All selected Variants | |||
|---|---|---|---|---|---|
| Coefficient | Coefficient † | Coefficient † | |||
| Age | −0.03458 | rs16861209 | −0.30388 | CRS | 1.13897 |
| Type of surgery | 0.69588 | rs17782313 | 0.32234 | GRS | 1.30048 |
| Type 2 Diabetes | 3.05077 | rs1800795 | −0.33407 | Constant | −1.34401 |
| Constant | −3.75577 | rs1801282 | 0.33407 | ||
| rs3771942 | −0.17997 | ||||
| rs6454674 | 0.24788 | ||||
| rs682447 | 0.41113 | ||||
| rs894160 | 0.28848 | ||||
| rs925946 | 0.28604 | ||||
| Constant | −0.30768 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciudin, A.; Fidilio, E.; Gutiérrez-Carrasquilla, L.; Caixàs, A.; Vilarrasa, N.; Pellitero, S.; Simó-Servat, A.; Vilallonga, R.; Ruiz, A.; de la Fuente, M.; et al. A Clinical-Genetic Score for Predicting Weight Loss after Bariatric Surgery: The OBEGEN Study. J. Pers. Med. 2021, 11, 1040. https://doi.org/10.3390/jpm11101040
Ciudin A, Fidilio E, Gutiérrez-Carrasquilla L, Caixàs A, Vilarrasa N, Pellitero S, Simó-Servat A, Vilallonga R, Ruiz A, de la Fuente M, et al. A Clinical-Genetic Score for Predicting Weight Loss after Bariatric Surgery: The OBEGEN Study. Journal of Personalized Medicine. 2021; 11(10):1040. https://doi.org/10.3390/jpm11101040
Chicago/Turabian StyleCiudin, Andreea, Enzamaría Fidilio, Liliana Gutiérrez-Carrasquilla, Assumpta Caixàs, Núria Vilarrasa, Silvia Pellitero, Andreu Simó-Servat, Ramon Vilallonga, Amador Ruiz, Maricruz de la Fuente, and et al. 2021. "A Clinical-Genetic Score for Predicting Weight Loss after Bariatric Surgery: The OBEGEN Study" Journal of Personalized Medicine 11, no. 10: 1040. https://doi.org/10.3390/jpm11101040