
Non-Vitamin K Antagonist Oral Anticoagulants and Risk of Myocardial Infarction in Patients with Atrial Fibrillation with or without Percutaneous Coronary Interventions: A Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
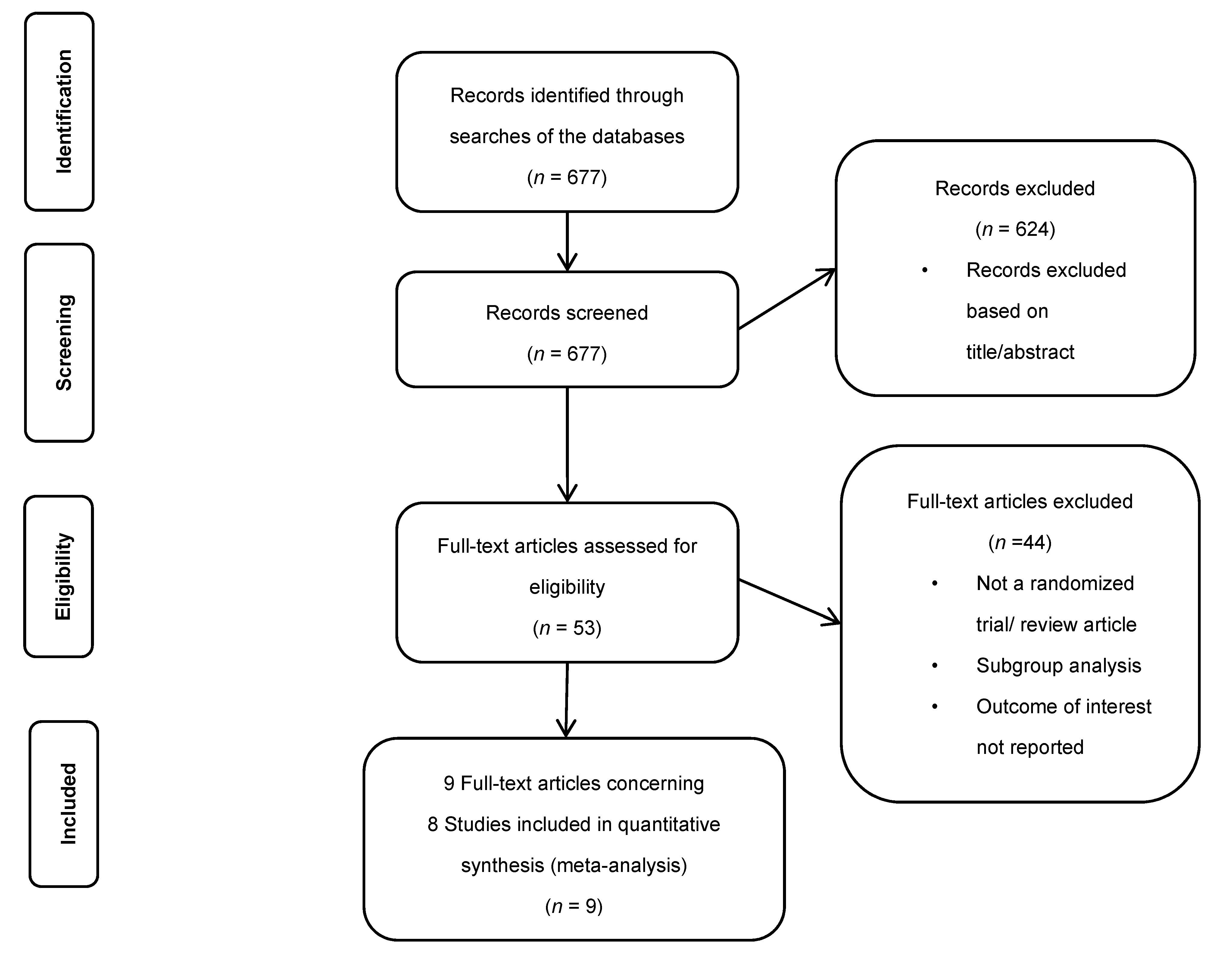
2.1. The Search Strategy and Selection Criteria
- (a)
- Only Phase III RCTs in patients with AF treated with oral anticoagulants (OAC) containing two arms, NOAC vs. warfarin, were analyzed.
- (b)
- Only RCTs with AF patients undergoing PCI for ACS or CCS and containing two arms, DAT (NOAC + P2Y12) vs. standard TAT, were analyzed.
- (c)
- All studies with included information on at least three following endpoints: death, stroke, and MI. We analyzed in detail the data contained in the publication and the accompanying Supplementary Materials. Two co-authors (SG and MM) performed the review and qualification for the analysis, and the third co-author (MKO) completed the final evaluation.
- (d)
- Clinical observational studies, data registers (a real-world registry-RWD), review papers, and comments were excluded.
2.2. Study Outcomes
2.3. Data Synthesis and Analysis
3. Results
3.1. Identified Studies Characteristics
3.2. Results of the Standard Meta-Analysis
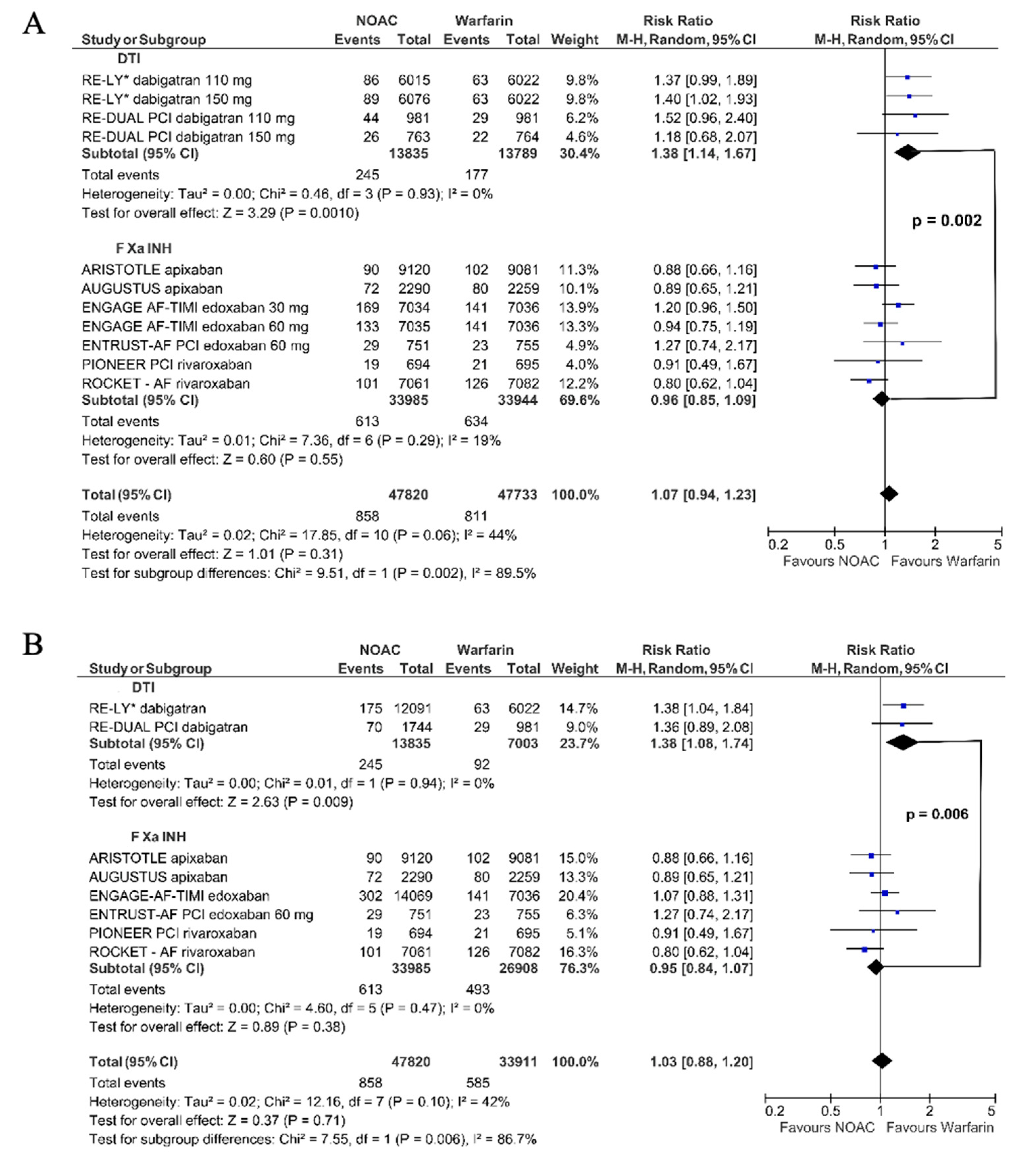
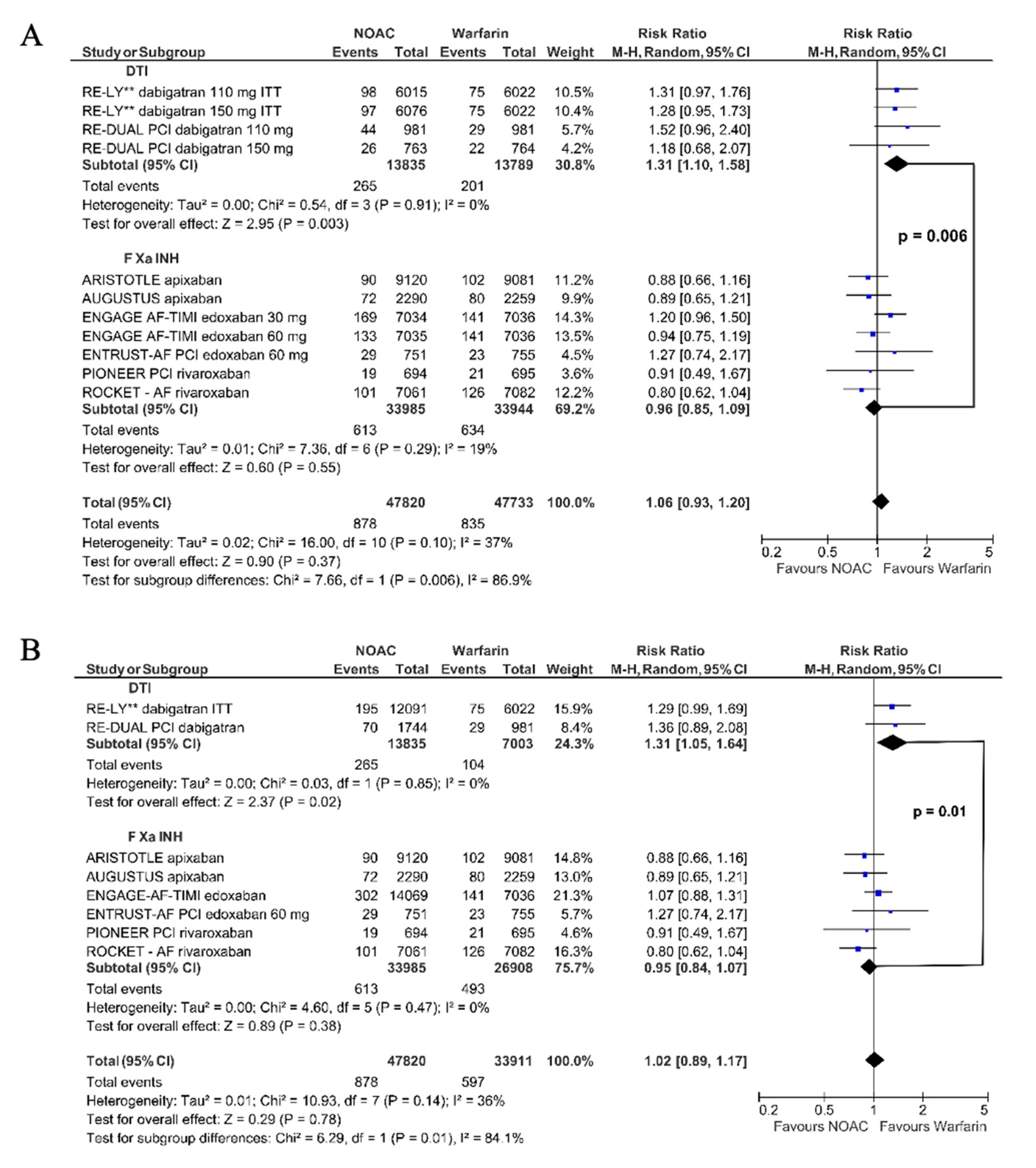
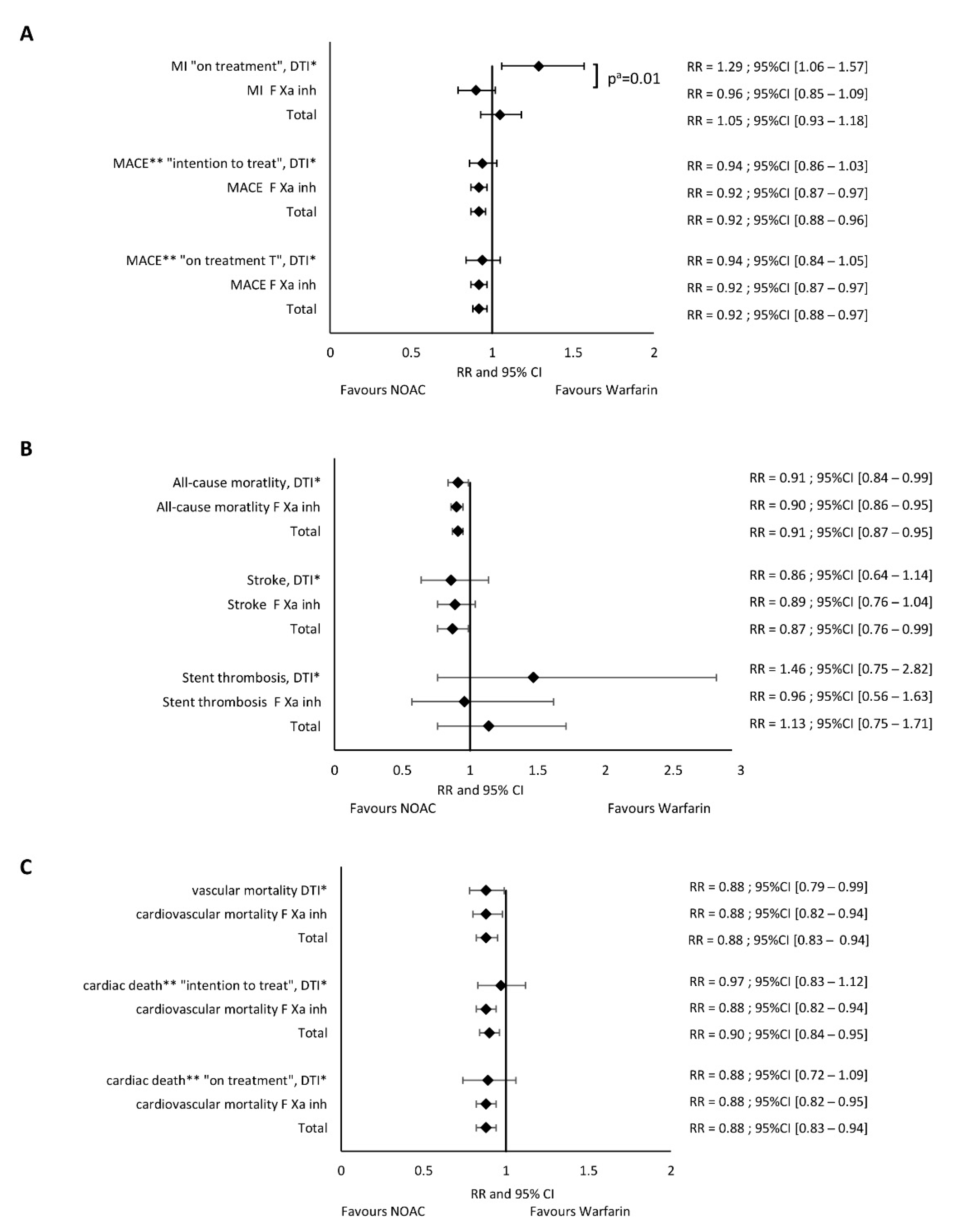
3.2.1. Myocardial Infarction
3.2.2. Major Adverse Cardiac Events
3.2.3. All-Cause Mortality
3.2.4. Stroke
3.2.5. Stent Thrombosis
3.2.6. Cardiovascular Death
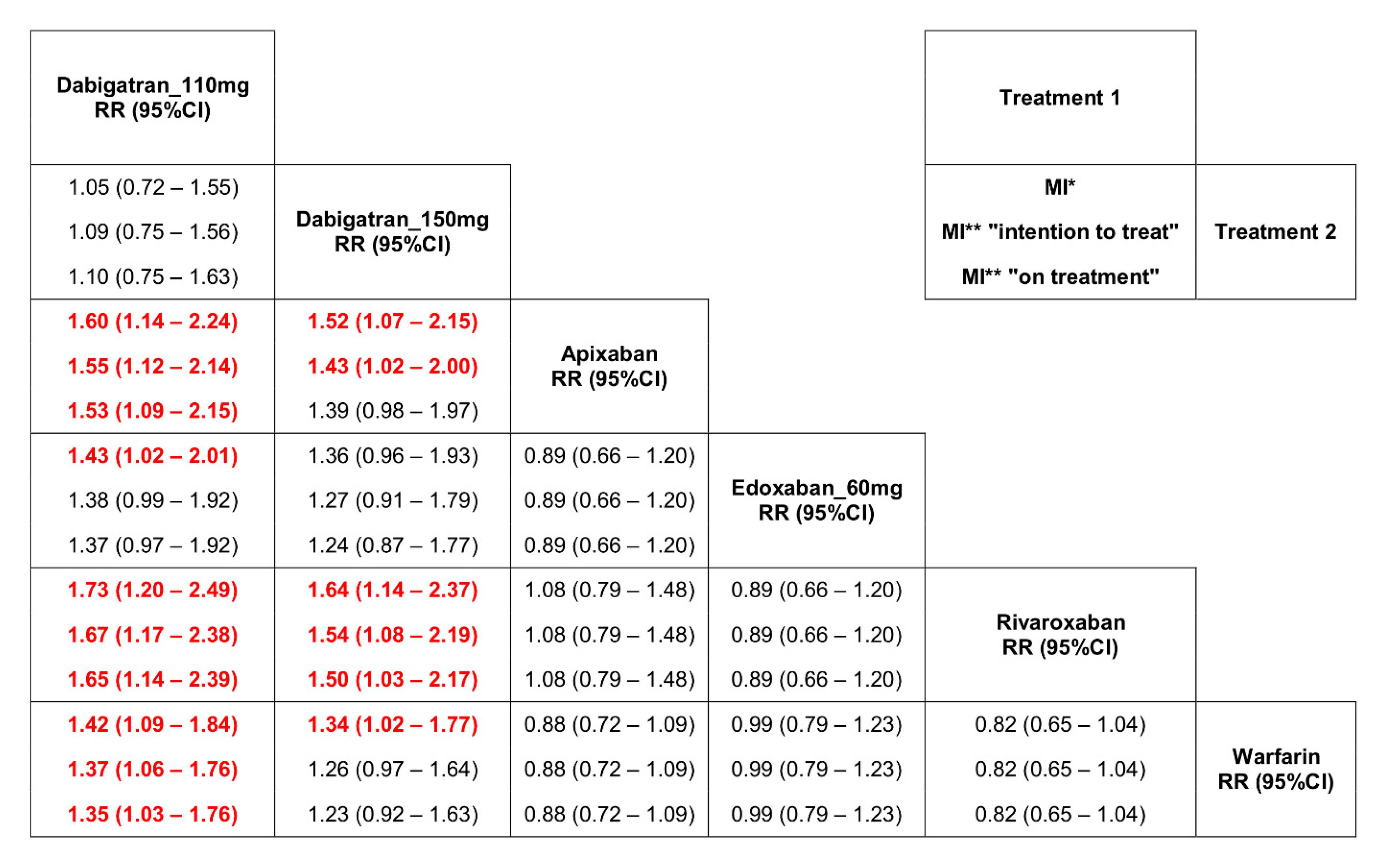
3.3. Results of the Network Meta-Analysis
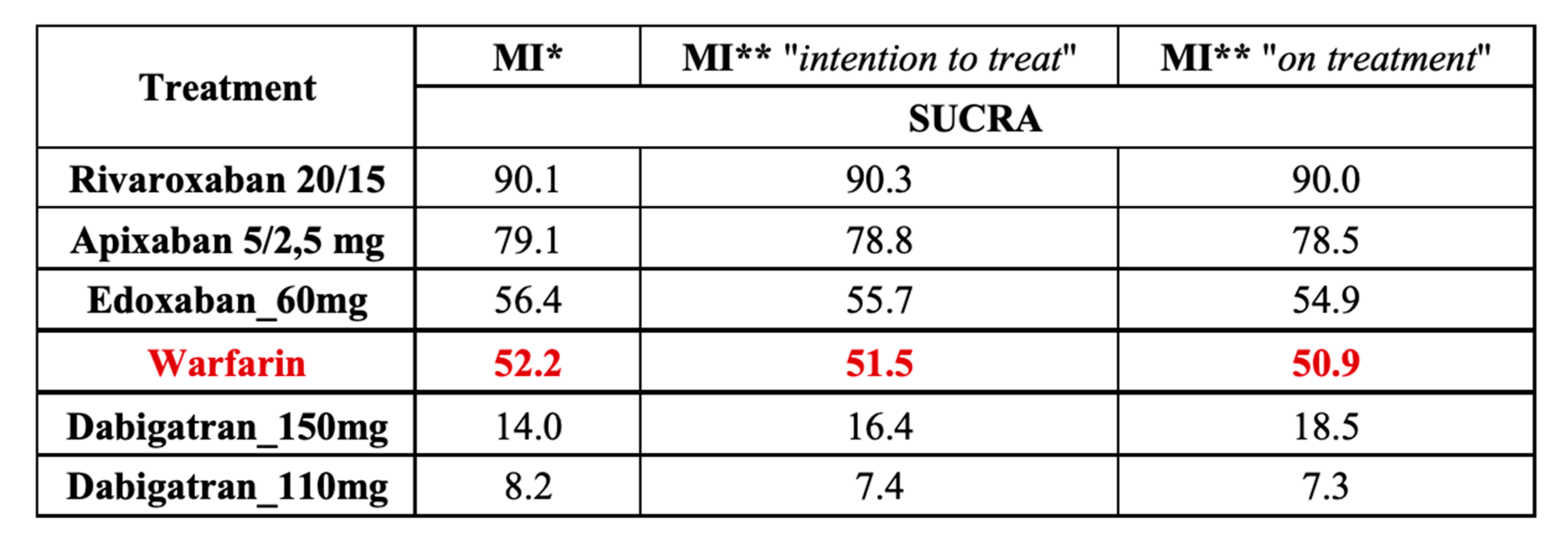
3.4. Results of the Analysis with SUCRA
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dewilde, W.J.; Oirbans, T.; Verheugt, F.W.; Kelder, J.C.; De Smet, B.J.; Herrman, J.P.; Adriaenssens, T.; Vrolix, M.; Heestermans, A.A.; Vis, M.M.; et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: An open-label, randomised, controlled trial. Lancet 2013, 381, 1107–1115. [Google Scholar] [CrossRef]
- Fiedler, K.A.; Maeng, M.; Mehilli, J.; Schulz-Schuepke, S.; Byrne, R.A.; Sibbing, D.; Hoppmann, P.; Schneider, S.; Fusaro, M.; Ott, I.; et al. Duration of Triple Therapy in Patients Oral Anticoagulation After Drug-Eluting Stent Implantation The ISAR-TRIPLE Trial. J. Am. Coll. Cardiol. 2015, 65, 1619–1629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.W.; Wildgoose, P.; Birmingham, M.; Ianus, J.; Burton, P.; Van Eickels, M.; et al. Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI. N. Engl. J. Med. 2016, 375, 2423–2434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.Y.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation. N. Engl. J. Med. 2017, 377, 1513–1524. [Google Scholar] [CrossRef]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef] [Green Version]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomised, open-label, phase 3b trial. Lancet 2019, 394, 1335–1343. [Google Scholar] [CrossRef]
- Golwala, H.B.; Cannon, C.P.; Steg, P.G.; Doros, G.; Qamar, A.; Ellis, S.G.; Oldgren, J.; Ten Berg, J.M.; Kimura, T.; Hohnloser, S.H.; et al. Safety and efficacy of dual vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of randomized clinical trials. Eur. Heart J. 2018, 39, 1726–1735. [Google Scholar] [CrossRef]
- Haller, P.M.; Sulzgruber, P.; Kaufmann, C.; Geelhoed, B.; Tamargo, J.; Wassmann, S.; Schnabel, R.B.; Westermann, D.; Huber, K.; Niessner, A.; et al. Bleeding and ischemic outcomes in patients treated with dual or triple antithrombotic therapy—Systematic review and meta-analysis. Eur. Heart J. Cardiovasc. Pharmacother. 2019, 5, 226–236. [Google Scholar] [CrossRef]
- Grajek, S.; Olasinska-Wisniewska, A.; Michalak, M.; Ritter, S.S. Triple versus double antithrombotic therapy in patients with atrial fibrillation and stent implantation: A meta-analysis of randomized trials. Kardiologia Polska 2019, 77, 837–845. [Google Scholar] [CrossRef] [Green Version]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, M.; Cannon, C.P.; Granger, C.B.; Verheugt, F.W.A.; Li, J.; Berg, J.M.; et al. Optimal Antithrombotic Regimens for Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention An Updated Network Meta-analysis. JAMA Cardiol. 2020, 5, 582–589. [Google Scholar] [CrossRef]
- Eyileten, C.; Postula, M.; Jakubik, D.; Toma, A.; Mirowska-Guzel, D.; Patti, G.; Renda, G.; Siller-Matula, J.M. Non-Vitamin K Oral Anticoagulants (NOAC) Versus Vitamin K Antagonists (VKA) for Atrial Fibrillation with Elective or Urgent Percutaneous Coronary Intervention: A Meta-Analysis with a Particular Focus on Combination Type. J. Clin. Med. 2020, 9, 1120. [Google Scholar] [CrossRef] [Green Version]
- Gargiulo, G.; Goette, A.; Tijssen, J.; Eckardt, L.; Lewalter, T.; Vranckx, P.; Valgimigli, M. Safety and efficacy outcomes of double vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of non-vitamin K antagonist oral anticoagulant-based randomized clinical trials. Eur. Heart J. 2019, 40, 3757–3767. [Google Scholar] [PubMed] [Green Version]
- Andò, G.; Costa, F. Double or triple antithrombotic therapy after coronary stenting and atrial fibrillation: A systematic review and meta-analysis of randomized clinical trials. Int. J. Cardiol. 2020, 302, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Hear. J. 2020, 42, 373–498. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Berthelemy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Uchino, K.; Hernandez, A.V. Dabigatran Association with Higher Risk of Acute Coronary Events Meta-analysis of Noninferiority Randomized Controlled Trials. Dabigatran Association with Higher Risk of Acute Coronary Events Meta-analysis of Noninferiority Randomized Controlled Trials. Arch. Intern. Med. 2012, 172, 397–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, K.H. Coronary and mortality risk of novel oral antithrombotic agents: A meta-analysis of large randomised trials. BMJ Open 2012, 2, e001592. [Google Scholar] [CrossRef]
- Chatterjee, S.; Sharma, A.; Uchino, K.; Biondi-Zoccai, G.; Lichstein, E.; Murkherjee, D. Rivaroxaban and risk of myocardial infarction: Insights from a meta-analysis and trial sequential analysis of randomized clinical trials. Coron. Artery Dis. 2013, 24, 628–635. [Google Scholar] [CrossRef]
- Artang, R.; Rome, E.; Nielsen, J.D.; Vidaillet, H.J. Meta-Analysis of Randomized Controlled Trials on Risk of Myocardial Infarction from the Use of Oral Direct Thrombin Inhibitors. Am. J. Cardiol. 2013, 112, 1973–1979. [Google Scholar] [CrossRef] [Green Version]
- Loke, Y.K.; Pradhan, S.; Yeong, J.K.; Kwok, C.S. Comparative coronary risks of apixaban, rivaroxaban and dabigatran: A meta-analysis and adjusted indirect comparison. Br. J. Clin. Pharmacol. 2014, 78, 707–717. [Google Scholar] [CrossRef] [Green Version]
- Tornyos, A.; Kehl, D.; D’Ascenzo, F.; Komócsi, A. Risk of Myocardial Infarction in Patients with Long-Term Non-Vitamin K Antagonist Oral Anticoagulant Treatment. Prog. Cardiovasc. Dis. 2016, 58, 483–494. [Google Scholar] [CrossRef]
- Morimoto, T.; Crawford, B.; Wada, K.; Ueda, S. Comparative efficacy and safety of novel oral anticoagulants in patients with atrial fibrillation: A network meta-analysis with the adjustment for the possible bias from open label studies. J. Cardiol. 2015, 66, 466–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Pakekh, A.; Pogue, A.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. RE-LY Steering Committee and Investigators* Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, M.P.; Mahaffey, K.W.; Garg, J.; Pan, P.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban Versus Warfarin in Nonvalvular Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granger, C.B.; Alexander, J.H.; Mcmurray, J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, R.; Ruff, C.T.; Braunwald, E.; Murphy, A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hohnloser, S.H.; Oldgren, J.; Yang, S.; Wallentin, L.; Ezekowitz, M.; Reilly, P.; Eikelboom, J.; Brueckmann, M.; Yusuf, S.; Connolly, S.J. Myocardial Ischemic Events in Patients With Atrial Fibrillation Treated With Dabigatran or Warfarin in the RE-LY (Randomized Evaluation of Long-Term Anticoagulation Therapy) Trial. Circulation 2012, 125, 669–676. [Google Scholar] [CrossRef]
- Bucher, H.C.; Guyatt, G.H.; Griffith, L.E.; Walter, S.D. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 1997, 50, 683–691. [Google Scholar] [CrossRef]
- Song, F.; Loke, Y.K.; Walsh, T.; Glenny, A.-M.; Eastwood, A.J.; Altman, D.G. Methodological problems in the use of indirect comparisons for evaluating healthcare interventions: Survey of published systematic reviews. BMJ 2009, 338, b1147. [Google Scholar] [CrossRef] [Green Version]
- Lumley, T. Network meta-analysis for indirect treatment comparisons. Statist. Med. 2002, 21, 2313–2324. [Google Scholar] [CrossRef]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P.A. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Connolly, S.J.; Eikelboom, J.; Joyner, C.; Diener, H.-C.; Hart, R.; Golitsyn, S.; Flaker, G.; Avezum, A.; Hohnloser, S.H.; Diaz, R.; et al. Apixaban in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011, 364, 806–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Reilly, P.A.; Wallentin, L. Newly identified events in the RE-LY Trial. N. Engl. J. Med. 2010, 363, 1875–1886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruff, C.h.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- Larsen, T.B.; Rasmussen, L.H.; Skjøth, F.; Due, K.M.; Callréus, T.; Rosenzweig, M.; Lip, G.Y. Efficacy and Safety of Dabigatran Etexilate and Warfarin in “Real-World” Patients With Atrial Fibrillation. J. Am. Coll. Cardiol. 2013, 61, 2264–2273. [Google Scholar] [CrossRef] [Green Version]
- Graham, D.J.; Reichman, M.E.; Wernecke, M.; Zhang, R.; Southworth, M.R.; Levenson, M.; Sheu, T.-C.; Mott, K.; Goulding, M.R.; Houstoun, M.; et al. Cardiovascular, Bleeding, and Mortality Risks in Elderly Medicare Patients Treated With Dabigatran or Warfarin for Nonvalvular Atrial Fibrillation. Circulation 2015, 131, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Lauffenburger, J.C.; Farley, J.F.; Gehi, A.K.; Rhoney, D.H.; Brookhart, M.A.; Fang, G. Effectiveness and Safety of Dabigatran and Warfarin in Real-World US Patients With Non-Valvular Atrial Fibrillation: A Retrospective Cohort Study. J. Am. Hear. Assoc. 2015, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.h.J.; Gerds, T.A.; Carlson, N.; Bonde, A.N.; Gislason, G.H.; Lamberts, M.; Olesen, J.B.; Pallisgaard, J.L.; Hansen, M.L.; Torp-Pedersen, C.; et al. Risk of Myocardial Infarction in Anticoagulated Patients With Atrial Fibrillation. J. Am. Coll. Cardiol. 2018, 72, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Wei, A.H.; Gu, Z.C.; Zhang, C.; Ding, Y.F.; Liu, D.; Li, J.; Liu, X.Y.; Lin, H.W.; Pu, J. Increased risk of myocardial infarction with dabigatran etexilate: Fact or fiction? A critical meta-analysis of over 580,000 patients from integrating randomized controlled trials and real-world studies. Int. J. Cardiol. 2018, 267, 1–7. [Google Scholar] [CrossRef]
- Larsen, T.B.; Rasmussen, L.H.; Gorst-Rasmussen, A.; Skjøth, F.; Rosenzweig, M.; Lane, D.A.; Lip, G.Y. Myocardial Ischemic Events in ‘Real World’ Patients with Atrial Fibrillation Treated with Dabigatran or Warfarin. Am. J. Med. 2013, 127, 329–336.e4. [Google Scholar] [CrossRef] [PubMed]
- Eilkenboom, J.W.; Weitz, J.I. Dabigatran and risk of myocardial infarction. Nat. Rev. Cardiol. 2012, 9, 260–262. [Google Scholar]
- Sipahi, I.; Celik, S.; Akyol, A. Dabigatran’s “Real-World” data about risk of Myocardial infarction and gastrointestinal bleeding contradicts with randomized trials. J. Am. Coll. Cardiol. 2013, 62, 945–946. [Google Scholar] [CrossRef] [Green Version]
- Larsen, T.B.; Rasmussen, L.H.; Skjoth, F.; Margrete, K.; Callreus, T.; Rosenzweig, M.; Lip, G.Y. Reply: Dabigatran’s “Real World” data about risk of myocardial infarction and gastrointestinal bleeding contradics with randomized trials. J. Am. Coll. Cardiol. 2013, 62, 946–947. [Google Scholar] [CrossRef] [Green Version]
- Hohnloser, S.H.; Eikelboom, J.W. Direct oral anticoagulants and myocardial infarction. The dust is settling. J. Am. Coll. Cardiol. 2018, 72, 27–28. [Google Scholar] [CrossRef]
- Polzin, A.; Dannenberg, L.; Wolff, G.; Zeus, T.; Kelm, M.; Petzold, T. Increased risk of myocardial infarction with dabigatran etexilate: Fact or fiction? A critical meta-analysis from integrating randomized controlled trials and real world studies: Wine or spritzer? Letter to Editor. Int. J. Cardiol. 2018, 270, 82. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Larsen, T.B.; Skjøth, F.; Rasmussen, L.H. Indirect Comparisons of New Oral Anticoagulant Drugs for Efficacy and Safety When Used for Stroke Prevention in Atrial Fibrillation. Am. Coll. Cardiol. 2012, 60, 738–746. [Google Scholar] [CrossRef] [Green Version]
- Kupó, P.; Szakács, Z.; Solymár, M.; Habon, T.; Czopf, L.; Hategan, L.; Csányi, B.; Borbás, J.; Tringer, A.; Varga, G.; et al. Direct Anticoagulants and Risk of Myocardial Infarction, a Multiple Treatment Network Meta-Analysis. Angiology 2019, 71, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Dale, B.; Eikelboom, J.W.; Weitz, J.I.; Young, E.; Paikin, J.S.; Coppens, M.; Whitlock, R.P.; Connolly, S.J.; Ginsberg, J.S.; Hirsh, J. Dabigatran attenuates thrombin generation to a lesser extent than warfarin: Could this explain their differential effects on intracranial hemorrhage and myocardial infarction? J. Thromb. Thrombolysis 2013, 35, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furugohri, T.; Sugiyama, N.; Morishima, Y.; Shibano, T. Antithrombin-independent thrombin inhibitors, but not direct factor Xa inhibitors, enhance thrombin generation in plasma through inhibition of thrombin-thrombomodulin-protein C system. J. Thromb. Haemost. 2011, 106, 1076–1083. [Google Scholar]
- Achilles, A.; Mohring, A.; Dannenberg, L.; Grandoch, M.; Hohlfeld, T.; Fischer, J.W.; Levkau, B.; Kelm, M.; Zeus, T.; Polzin, A. Dabigatran enhances platelet reactivity and platelet thrombin receptor expression in patients with atrial fibrillation. J. Thromb. Haemost. 2017, 15, 473–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christersson, C.; Oldgren, J.; Wallentin, L.; Siegbahn, A. Treatment with an oral direct thrombin inhibitor decreases platelet activity but increases markers of inflammation in patients with myocardial infarction. J. Intern. Med. 2011, 270, 215–223. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | RE-LY | ROCKET AF | ENGAGE AF TIMI 48 | ARISTOTLE | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Treatment/dose | Dabigatran 110 mg (n = 6015) | Dabigatran 150 mg (n = 6076) | Warfarin (n = 6022) | Rivaroxaban 20 mg or 15 mg daily if CrCl 30–49 mL/min (n = 7131) | Warfarin (n = 7133) | High Dose Edoxaban (n = 7035) | Low Dose Edoxaban (n = 7034) | Warfarin (n = 7036) | Apixaban 5 mg twice daily or 2.5 mg twice daily (n = 9120) | Warfarin (n = 9081) |
| Age, y, mean (SD) or median | Mean (SD) 71.4 (8.6) | Mean (SD) 71.5 (8.8) | Mean (SD) 71.6 (8.6) | Median 73 | Median 73 | Median 72 | Median 72 | Median 72 | Median 70 | Median 70 |
| Female, n (%) | 2150 (35.7) | 2236 (36.8) | 2213 (36.7) | 2831 (39.7) | 2832 (39.7) | 2669 (37.9) | 2730 (38.8) | 2641 (37.5) | 3234 (35.5) | 3182 (35.0) |
| Renal function, n (%) or as indicated otherwise | NA | NA | NA | Median CrCl 67 mL/min | Median CrCl 67 mL/min | CrCl ≤ 50 mL/min 1379 (19.6) | CrCl ≤ 50 mL/min 1334 (19.0) | CrCl ≤ 50 mL/min 1361 (19.3) | CrCl ≤ 50 mL/min 1502 (16.5) | CrCl ≤ 50 mL/min 1515 (16.7) |
| CHA2DS2VASc, mean (SD) | 2.1 (1.1) | 2.2 (1.2) | 2.1 (1.1) | 3.48 (0.94) | 3.46 (0.95) | 2.8 (1.0) | 2.8 (1.0) | 2.8 (1.0) | 2.1 (1.1) | 2.1 (1.1) |
| HAS-BLED, mean (SD) or <3 vs. ≥3 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Hypertension, n (%) | 4738 (78.8) | 4795 (78.9) | 4750 (78.9) | 6436 (90.3) | 6474 (90.8) | 6591 (93.7) | 6575 (93.5) | 6588 (93.6) | 7962 (87.3) | 7954 (87.6) |
| Diabetes mellitus, n (%) | 1409 (23.4) | 1402 (23.1) | 1410 (23.4) | 2878 (40.4) | 2817 (39.5) | 2559 (36.4) | 2544 (36.2) | 2521 (35.8) | 2284 (25.0) | 2263 (24.9) |
| History of stroke or TIA, n (%) or systemic embolism | 1195 (19.9) | 1233 (20.3) | 1195 (19.8) | 3916 (54.9) | 3895 (54.6) | 1976 (28.1) | 2006 (28.5) | 1991 (28.3) | 1748 (19.2) | 1790 (19.7) |
| History of myocardial infarction, n (%) | 1008 (16.8) | 1029 (16.9) | 968 (16.1) | 1182 (16.6) | 1286 (18.0) | NA | NA | NA | 1319 (14.5) | 1266 (13.9) |
| History of CABG, n (%) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| History of PCI, n (%) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| ASA | 2404 (40.0) | 2352 (38.7) | 2442 (40.6) | 2586 (36.3) | 2619 (36.7) | 2070 (29.4) | 2018 (28.7) | 2092 (29.7) | 2859 (31.3) | 2773 (30.5) |
| Characteristics | PIONEER-AF PCI, 2016 | RE-DUAL PCI, 2017 | AUGUSTUS, 2019 | ENTRUST-AF PCI, 2019 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Therapy | DT (n = 709) Rivaroxaban (15 mg) + P2Y12 inhibitor (clopidogrel, 75 mg, or ticagrelor, 2 × 90 mg, or prasugrel, 10 mg) | TT (n = 706) VKA + ASA (75–100 mg) + P2Y12 inhibitor (clopidogrel, 75 mg, or ticagrelor, 2 × 90 mg, or prasugrel, 10 mg) | DT (n = 981) Dabigatran (2 × 110 mg) + P2Y12 inhibitor (clopidogrel, 75 mg, or ticagrelor, 2 × 90 mg) | DT (n = 763) Dabigatran (2 × 150 mg) + P2Y12 inhibitor (clopidogrel, 75 mg, or ticagrelor, 2 × 90 mg) | TT (n = 981) VKA + ASA (<100 mg) + P2Y12 inhibitor (clopidogrel, 75 mg, or ticagrelor, 2 × 90 mg) | TT (n = 764) Corresponding TT VKA | DT/TT (n = 2306) Apixaban (2 × 5 mg or 2 × 2.5 mg) + P2Y12 inhibitor + ASA, 81 mg/placebo | DT/TT (n = 2308) VKA + P2Y12 inhibitor + ASA, 81 mg/placebo | DT (n = 751) Edoxaban (60 mg/or 30 mg in specific indication) + P2Y12 inhibitor | TT (n = 755) VKA + P2Y12 inhibitor + ASA (100 mg, for 1–12 months) |
| Age, y, mean (SD) | 70.4 (9.1) | 69.9 (8.7) | 71.5 (8.9) | 68.6 (7.7) | 71.7 (8.9) | 68.8 (7.7) | 70.4 | 70.9 | 69 | 70 |
| Female sex, n (%) | 181 (25.5) | 188 (26.6) | 253 (25.8) | 171 (22.4) | 231 (23.5) | 170 (22.3) | 670 (29.1) | 667 (28.9) | 194 (26) | 192 (25) |
| Renal function, n (%) or as indicated otherwise | Mean (SD) CrCl, 78.3 (31.3) mL/min | Mean (SD) CrCl, 80.7 (30) mL/min | Mean (SD) CrCl, 76.3 (28.9) mL/min | Mean (SD) CrCl, 83.7 (31) mL/min | Mean (SD) CrCl, 75.4 (29.1) mL/min | Mean (SD) CrCl, 81.3 (29.6) mL/min | creat ≥ 1.5 mg/dL 173 (7.6) | creat ≥ 1.5 mg/dL 207 (9.2) | Mean 71.8 mL/min | Mean 71.7 mL/min |
| Type of index event, n (%) | NSTEMI, 130 (18.5) STEMI, 86 (12.3) UA, 145 (20.7) | NSTEMI, 123 (17.8) STEMI, 74 (10.7) UA, 164 (23.7) | ACS, 509 (51.9) CCS, 433 (44.1) Staged PCI, 156 (15.9) Other 43 (4.4) | ACS, 391 (51.2) CCS, 320 (41.9) Staged PCI, 138 (18.1) Other, 65 (8.5) | ACS, 475 (48.4) CCS, 429 (43.7) Staged PCI, 168 (17.1) Other, 62 (6.3) | ACS, 369 (48.3) CCS, 339 (44.4) Staged PCI, 134 (17.5) other 50 (6.5) | ACS and PCI, 873 (38) ACS -medical therapy, 547 (23.8) Elective PCI, 877 (38.2) | ACS and PCI, 841 (36.6) ACS -medical therapy, 550 (23.9) Elective PCI, 907 (39.5) | ACS 388 (52), CCS 363 (48) | ACS 389 (52), CCS 366 (48) |
| CHA2DS2VASc, mean (SD) | 3.7 (1.7) | 3.8 (1.6) | 3.7 (1.6) | 3.3 (1.5) | 3.8 (1.5) | 3.5 (1.5) | 3.9 (1.6) | 4.0 (1.6) | 4 | 4 |
| HAS-BLED, mean (SD) | NA | NA | 2.7 (0.7) | 2.6 (0.7) | 2.8 (0.8) | 2.7 (0.8) | 2.9 (1.0) | 2.9 (0.9) | 3 | 3 |
| Hypertension, n (%) | NA | NA | NA | NA | NA | NA | 2042 (88.6) | 2031 (88) | 674 (90) | 687 (91) |
| Diabetes mellitus, n (%) | NA | NA | 362 (36.9) | 260 (34.1) | 371 (37.9) | 303 (39.7) | 842 (36.5) | 836 (36.2) | 259 (34) | 258 (34) |
| Stroke or TIA, n (%) | NA | NA | 74 (7.5) | 52 (6.8) | 100 (10.2) | 77 (10.1) | 326 (14.2) | 307 (13.4) | 97 (13) | 92 (12) |
| History of myocardial infarction, n (%) | 20% | 22% | 237 (24.2) | 194 (25.4) | 268 (27.3) | 211 (27.6) | NA | NA | 188 (25) | 177 (23) |
| History of CABG, n (%) | NA | NA | 97 (9.9) | 79 (10.4) | 111 (11.3) | 87 (11.4) | NA | NA | 46 (6) | 49 (6) |
| History of PCI, n (%) | NA | NA | 326 (33.2) | 239 (31.3) | 347 (35.4) | 272 (35.6) | NA | NA | 199 (26) | 195 (26) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grajek, S.; Kałużna-Oleksy, M.; Siller-Matula, J.M.; Grajek, M.; Michalak, M. Non-Vitamin K Antagonist Oral Anticoagulants and Risk of Myocardial Infarction in Patients with Atrial Fibrillation with or without Percutaneous Coronary Interventions: A Meta-Analysis. J. Pers. Med. 2021, 11, 1013. https://doi.org/10.3390/jpm11101013
Grajek S, Kałużna-Oleksy M, Siller-Matula JM, Grajek M, Michalak M. Non-Vitamin K Antagonist Oral Anticoagulants and Risk of Myocardial Infarction in Patients with Atrial Fibrillation with or without Percutaneous Coronary Interventions: A Meta-Analysis. Journal of Personalized Medicine. 2021; 11(10):1013. https://doi.org/10.3390/jpm11101013
Chicago/Turabian StyleGrajek, Stefan, Marta Kałużna-Oleksy, Jolanta M. Siller-Matula, Maksymilian Grajek, and Michał Michalak. 2021. "Non-Vitamin K Antagonist Oral Anticoagulants and Risk of Myocardial Infarction in Patients with Atrial Fibrillation with or without Percutaneous Coronary Interventions: A Meta-Analysis" Journal of Personalized Medicine 11, no. 10: 1013. https://doi.org/10.3390/jpm11101013