Our study evaluated the specific needs of families who have preschool children diagnosed with cerebral palsy, and identified several factors influencing these needs. Although our study focused on families in Latvia, the results may be helpful to families, care-givers and public health officials in other locations.
As Latvia does not have a unified register of patients with cerebral palsy, the information about the number of such families living in Latvia was based on information provided by the State Medical Commission for the Assessment of Health Condition and Working Ability, revealing that there were 264 children registered in Latvia who had been given the status of disabled based on the ICD G80 code (cerebral palsy), and who were between two and seven years of age. The research engaged 234 families, which is 88.6% of all potential families. Among the families included in the research, 84 families, or 36%, lived in Riga, 89 families (38%) lived in other Latvian cities, and 61 families (26%) lived in a rural territory. Such a distribution of places of residence allows us to assume that comprehensive information has been obtained about the needs and factors affecting families living in Latvia and raising preschool children with cerebral palsy.
4.1. Results of Family Needs Survey
According to the results of the Family Needs Survey, the biggest share of needs was pointed out in the “Needs for Information” subscale. More than half of respondents gave affirmative answers to all statements in this section. There is a similar trend also in other studies, where the needs of families with children with functional disabilities are explored [
17,
18,
19,
20,
21,
22]. This might mean that the majority of families who are raising children with developmental disorders feel that they lack information, and service providers should think how to improve the provision of information to these families. Still, Palisano and colleagues, observing a similar trend in their study, made the assumption that the large number of “Needs for Information” is possibly related to the opinion of the surveyed parents that “there is never too much information”, rather than a true lack of information [
20]. Despite this assumption, health care providers should make sure that families receive professional answers to their questions. It is especially important now, when the internet is broadly used to obtain information but often provides confusing, unsubstantiated information about the child’s treatment and rehabilitation opportunities [
23].
In our study, a large number of respondents pointed out that they need information about services that are available for their child with cerebral palsy (88.9%) and services that they would need in the future (85%). The data published by other authors are slightly different. Just 54% of parents surveyed by Farmer, 63% of parents surveyed by Ellis and 59% of parents polled by Palisano mentioned that they need information about the presently available services, while 74%, 78% and 68% of parents, respectively, were interested in future services [
17,
20,
21]. Such differences show that families living in Latvia are less informed about services available for their children with developmental disorders, and service providers should make sure that the family is informed about issues important to it.
Families surveyed by us (more often than families surveyed by other researchers) said that they wish to obtain information about their child’s disorders, as well as about training and education opportunities for the child. Possibly, such increased interest can be explained via the peculiarities of the age of the children. Our research included preschool children, while other authors studied families with children of different ages, including school age. It is noted that the younger the child, the higher the parents’ interest in all kinds of information. Young parents are scared and unconfident, they have not yet gotten used to the new situation and supply of services, and they are looking for every opportunity to promote the child’s development [
20].
The next most important area, in which most of the families expressed a wish for additional support, was needs related to community services (treatment, rehabilitation, preschools, etc.) and financial support. Such a result is no surprise. It is well-known that cerebral palsy is an “expensive” disorder, and its costs may reach EUR 900,000 throughout a lifetime [
24]. The availability of services and financial challenges for families who are raising children with cerebral palsy are much higher than for other families with children of similar age [
25]. As is often a case, and was so in our research group, if one parent is not working any more or is working part-time, financial challenges are even higher.
It is alarming that 73% of respondents said that the family needs help to coordinate medical, social and education services. It should be noted that in countries with historically stable social support system, families less often point out the necessity related to the coordinated provision of medical, social and educational services [
7,
19,
20,
21].
It is an established fact that as the child with functioning disorders grows, the need for financial support also grows [
7]. Since in the families we surveyed the children were up to the age of seven, a comparatively small number of families said that they would need financial assistance for house modification. Still, more than half of the respondents needed financial support for special equipment or assistive devices. A similar need for financial support for the purchase of assistive devices was voiced by parents surveyed by Nitta in Japan and parents surveyed by Wang in China [
18,
26]. Meanwhile, in Farmer’s and Palisano’s surveys in the US, such needs were marked by just 19% and 34% of parents, respectively [
20,
21].
A large part of the surveyed families pointed out that they need not only financial, but also moral and psychological, support. As taking care of the sick child takes a large part of the day, and half of the children did not attend a preschool, it is not a surprise that the majority of the surveyed parents would like to have more time to themselves. Such type of needs is marked as important also in the reports published by other authors [
17,
18,
26].
Like in the research by Palisano and colleagues, just a small number of respondents noted needs that are related to family functioning [
20]. It is possible that families indeed do not need such assistance. Still, it cannot be excluded that parents are not aware of, or are not admitting, such needs. It is believed that parents who have a child with developmental orders or a chronic illness more often think about how to promote the child’s development and focus less on family needs, or do not consider them as needs, which might be a reason for elevated stress and families breaking apart [
27].
4.2. Analysis of Factors Explaining Family Needs
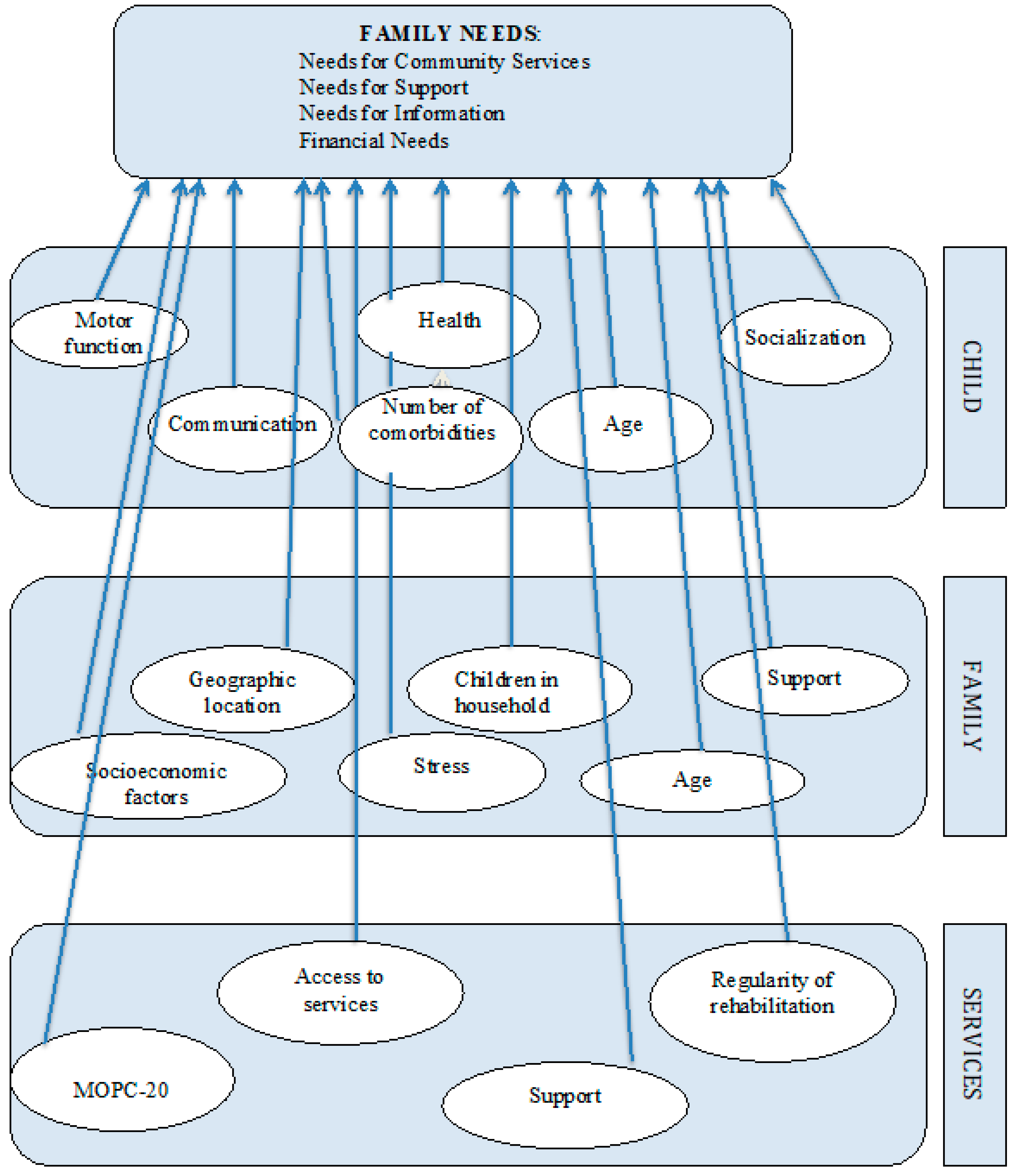
As hypothesised, the needs of families raising preschool children with cerebral palsy living in Latvia are affected by factors characterising families, children with cerebral palsy and rehabilitation service providers, and the unique impact of these factors depends on the type of family needs.
The literature sources name the child’s functioning limitations and health condition as significant factors influencing family needs—the more distinct the functioning limitations and complicated the health disorders, the higher are the family needs [
8,
18,
20,
21,
28,
29]. In our research, the level of the child’s mobility limitations was a significant factor influencing the financial needs of families—families whose children were able to walk without any assistive devices marked lower needs for financial support compared to families whose children did not have such a possibility. The obtained data match with information published by other authors [
8,
20]. Meanwhile, in contrast to results found by Almasri and colleagues, the influence of the child’s mobility limitation levels on family needs for services and support was not discovered in our research [
8].
An unexpected result was the influence of the child’s communication limitations on family needs for community services—families with children who had more distinct communication problems most often noted that they need assistance in the finding and provision of medical, rehabilitation or education services. Obviously, rehabilitation and education services for children with motor disorders in Latvia are more available and better developed than services for children who, in addition, have distinctive communication limitations that often are combined with cognitive disorders; thus, the need for specific education and rehabilitation programmes increases.
The child’s communication limitations also affected the families’ needs for information—more distinct communication disorders in the child increased the number of family needs in this type of needs. It has been established that cognitive and behavioural disorders in children are factors that increase the family needs [
8,
19], while children with distinctive communication problems often have cognitive limitations and limited socialisation [
30,
31]. Considering the child’s age, the cognitive level of the children included in the research was not evaluated. Still, an assumption could be made that children with distinctive communication problems had more distinct cognitive limitations that possibly determined the higher family needs for services and information.
The data analysis in our research discovered that as the number of comorbidities associated with brain damage grows, the total family needs increase, as do needs for support and financial needs, and this factor had a significant effect on family needs in the above-mentioned types of needs.
The support provided by the closest family members was a very significant factor, affecting family needs—as the child’s primary caretaker received support and assistance from other family members, the number of family needs declined. Further, other researchers confirmed that families that have good and supportive mutual relations are more successful in solving issues that are related with the care and treatment of the sick child, and these families less often need “external” support [
20,
32]. This is valuable information for service providers. Service providers should be aware that in cases when the service is received by a family that lacks this internal support, there is possibly a greater need for services, information, and social and financial support.
Such factors as the education level and perceived stress level of the child’s primary caretaker had a similar impact on family needs. A high perceived stress level and elementary education were significant factors increasing family needs for support and community services. Lower education levels of parents so far have not been related with needs for additional support [
8,
19], while a correlation between elevated stress levels and the increased necessity for support has also been revealed in other studies [
21,
32,
33,
34]. It is interesting that the perceived stress level of the child’s primary caretaker had a higher unique impact on the family needs for services than the caretaker’s employment or the family’s income level. Employment and the family’s financial situation often are identified as factors that influence the family’s needs for community services [
19,
20,
21], while we did not find information about the impact of the caretaker’s stress level on this type of needs. Possibly, it is harder for persons with higher stress levels to organise their everyday activities and set priorities, and this has a negative effect on the quality of the person’s life, creating challenges for the optimum planning and organisation of the tasks [
32,
33].
If there is a child with health and functioning disorders in a family, then the availability of different health and social services becomes important. Farmer and Almasri in their studies discovered that families who live in cities where health, social care and educational institutions are more easily accessible in general mark lower needs than families living in more distant regions [
8,
21]. Our research also revealed a similar trend—families living in Riga noted lower needs for community services than families living in other cities or rural territories. Still, the influence of this factor on this area of needs was not confirmed. In our research, neither the place of residence nor the number of children in the family had a significant impact on family needs.
Among the most significant factors reducing family needs are higher socio-economic status and higher income [
7,
8,
21,
35]. This information is also confirmed in our research. Medium and, even more so, low family income levels increased the total number of family needs, and the number of family needs for community services, information and financial support. The only type of needs reviewed in the study that was not affected by the income level was family needs for support—equal needs for formal and informal support were voiced by those respondents whose family income level was assessed as high and those who assessed their income level as medium or even low.
Surprisingly, but in contrast with information published by Almasri and colleagues [
8], neither the availability of rehabilitation services at the place of residence nor the regularity of receiving rehabilitation services were factors that affected the family needs of our respondents. Support received from professionals, however, turned out to be a significant factor reducing needs. Higher support from professionals was a significant factor reducing total family needs and needs for information and support. Further, there was a positive reducing effect on family needs if the family noted that the received services complied with the principles of family-centred care. In particular, the role of the principle “Enabling and Partnership” should be underscored. By providing services based on cooperation and partnership principles, i.e., engaging the family in decision making as an equal partner, it is possible to significantly reduce the overall family needs and needs for support, services and additional financing. This is significant information for service providers, which proves the importance of the way the family is engaged in the treatment and rehabilitation processes, and of the skills of service providers in communicating with the client and cooperating. Our results match with the reports by Palisano and Almasri on the positive impact of family-centred care on reducing family needs in families who are raising children with cerebral palsy [
8,
20].
4.3. Summary of Factors Explaining Family Needs
In our research, 6 factors characterising children with cerebral palsy, 10 factors characterising families and 9 factors characterising rehabilitation services were reviewed as possible factors influencing family needs, but only one of the analysed factors—the family’s internal support—was identified as a significant factor influencing family needs in all areas of needs. As the child’s primary caretaker received support from other family members, other needs were considerably reduced.
Like in the reports of other authors [
8,
19,
20], our research also revealed that factors reducing family needs included such socio-economic factors as the family’s income level, which was a significant factor affecting family needs in four types of needs, and the employment of the child’s primary caretaker, which had an impact on three types of family needs. The impact of factors related to the child’s health condition was less important—a larger number of comorbidities was a factor increasing family needs in three areas of needs, but its unique impact was low. Mobility and communication limitations were factors increasing family needs only in two areas of needs—distinctive communication limitation for the child increased family needs for community services and information, while severe mobility limitations increased financial needs and overall family needs.
The perceived stress level of the child’s primary caretaker turned out to be a significant factor affecting family needs in three areas of needs—higher perceived stress level increased the overall family needs and needs for community services and support.
The above-mentioned factors are unique, individual and in most cases cannot be directly influenced. Service providers who work with families raising a preschool child with cerebral palsy should consider the impact of the above-mentioned factors on family needs, and should pay additional attention to families with potentially higher risks of needs.
Analysis of the research results also revealed the significant impact of those factors that directly depend on service providers. Thus, the provision of rehabilitation services based on the family-centred care principle “Enabling and Partnership” was a significant factor reducing family needs in four areas of needs—overall family needs, needs for support, services and financial support. Meanwhile, a family receiving more support from professionals who work with the child or the family was a significant factor reducing family needs in three areas of needs.
In conclusion, the most important factors affecting the needs of families living in Latvia are related with the socio-economic situation and support of peers—family members or professionals who work with the family. Limitations in the child’s functioning and health disorders were factors influencing family needs to a lower extent.
4.4. Methodological Analysis and Limitations of the Research
In order to achieve the objective of the research, an analytical cross-sectional design was selected for the study. Thus, information about families living in Latvia and raising preschool children diagnosed with cerebral palsy, as well as family needs and factors affecting them, was obtained during a certain period of time. In order to claim that the information obtained during the study can be generalised in relation to another time period, data should be obtained repeatedly, but this was not planned. Thus, information obtained about the needs of families living in Latvia and factors affecting them should be assessed and interpreted with caution, not excluding possible changes in time.
Family needs were identified using a standardised questionnaire, the Family Needs Survey, which, during the period of obtaining the data, was the most recognised and broadly used questionnaire for identifying family needs. The questionnaire was developed to learn about the needs of those families who are raising preschool children with development disorders. Still, the questionnaire was developed several dozens of years ago and, even though its modified version was used to obtain the data, it is still possible that not all the needs of families living in Latvia and raising children with cerebral palsy were identified. The advantage of using a standardised questionnaire is simplicity in obtaining data, and the opportunity to analyse these data by using quantitative data analysis methods. Still, such a way of obtaining data does not allow one to study the problem thoroughly; therefore, it is recommended to conduct a more thorough study of the obtained data, using qualitative methods for data extraction and analysis.
The possible factors influencing family needs were identified, based on a comprehensive study of literature sources and factors that may affect family needs in cases when families take care of children with cerebral palsy. The needs of families raising children with developmental disorders have been studied broadly, but, during the preparation phase, we did not manage to find sources that have studied family needs in the nearest geopolitical region, with similar historical and socio-economic backgrounds. Thus, it is possible that we did not manage to identify the type of needs or possible factors influencing these needs that are unique for our region. As a limitation to the study, we should also name the fact that the overall number of comorbidities of the child was viewed as a factor affecting family needs, without assessing the possible impact of each comorbidity separately.
This is proven in the multiple linear regression analysis—the final models explained 23–61% of the changes in family needs. Thus, there could be other unpredicted and unidentified factors that might affect the needs of the families living in Latvia. Another limitation of the study is the fact that information characterising the child’s health condition was obtained from the caretaker, and we did not assess the possible unique impact of particular elements characterising the health conditions, such as behavioural problems, on family needs.
A more targeted approach would be to use the qualitative research design, which would allow us to understand the research problem more thoroughly and present a new hypothesis.
The factors affecting family needs were determined using the multiple linear regression analysis method. Such an analysis method was selected because it allows one to study the dependence of the features on a number of independent features, and the data obtained in the study met the requirements for conducting a multiple linear regression analysis. However, this type of analysis has its drawbacks. Even though we managed to study factors that might affect family needs and test their impact on the stability of the regression models, still, some inaccuracies during the data obtaining and analysis process cannot be excluded. It is also established that not all independent variables have a direct impact on the dependent feature [
20]; therefore, for a deeper understanding of the research problem and construct, further studies should focus on the indirect impact of the identified (and possible new) factors.



{kind=link}