Liquid lncRNA Biopsy for the Evaluation of Locally Advanced and Metastatic Squamous Cell Carcinomas of the Head and Neck

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Volunteers
2.2. Treatment
2.3. Blood Sampling Design
2.4. Sample Collection
2.5. RNA Isolation
2.6. cDNA Synthesis and qRT-PCR Reaction
3. Statistical Analysis
4. Results
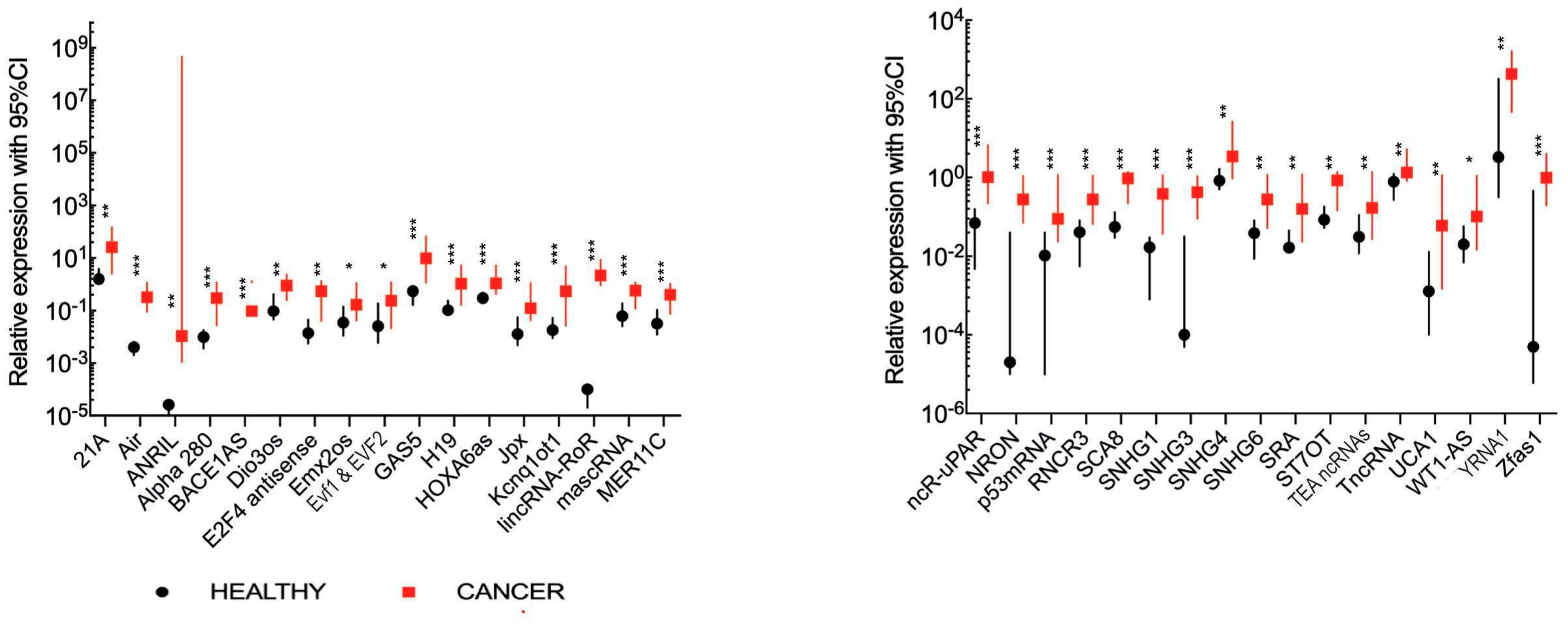
4.1. Comparison of lncRNA Expression Levels between Healthy Volunteers and All HNSCC Patients
4.2. Comparison of lncRNA Expression Levels between Healthy Volunteers and Recurrent and/or Metastatic HNSCC Patients
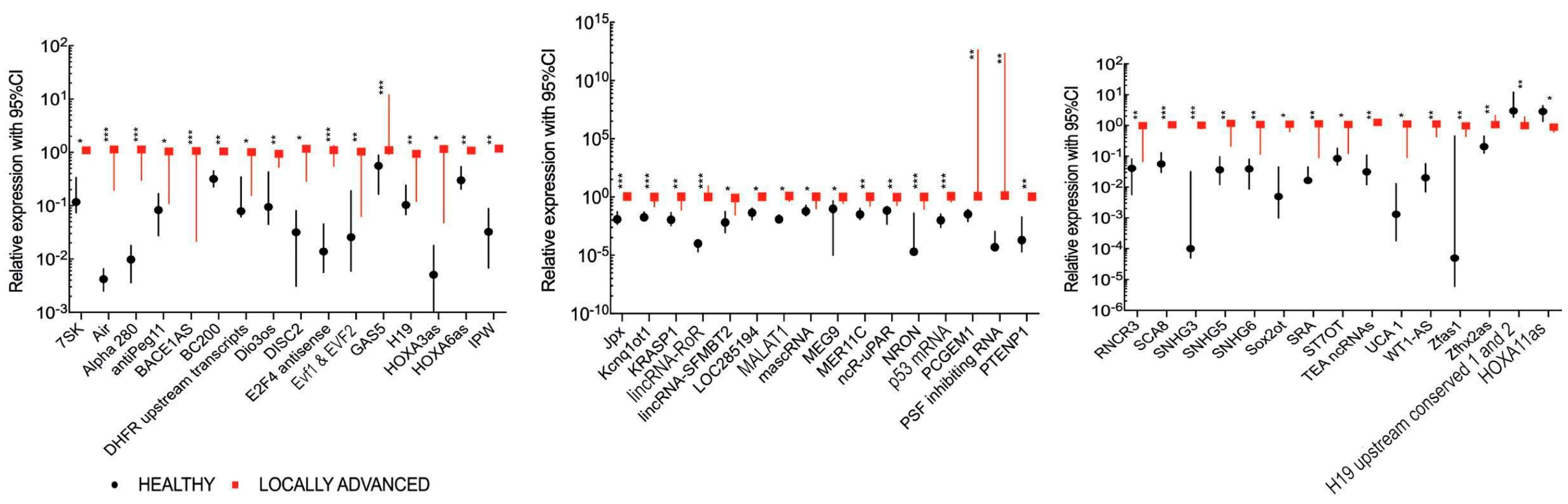
4.3. Comparison of lncRNA Expression Levels between Healthy Volunteers and Locally Advanced HNSCC Patients
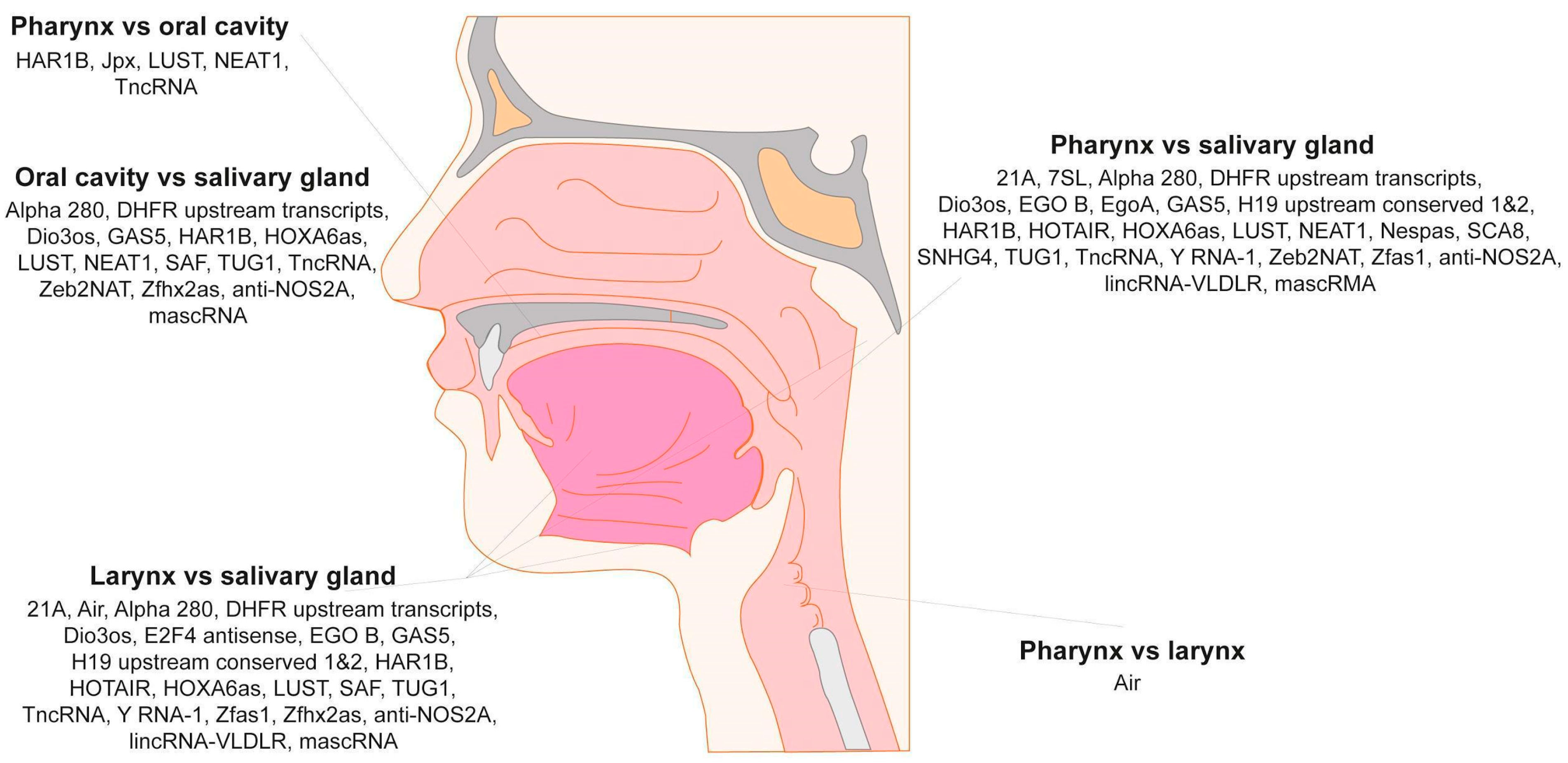
4.4. Plasma lncRNA Expression Differs Depending on Primary Tumor Localization
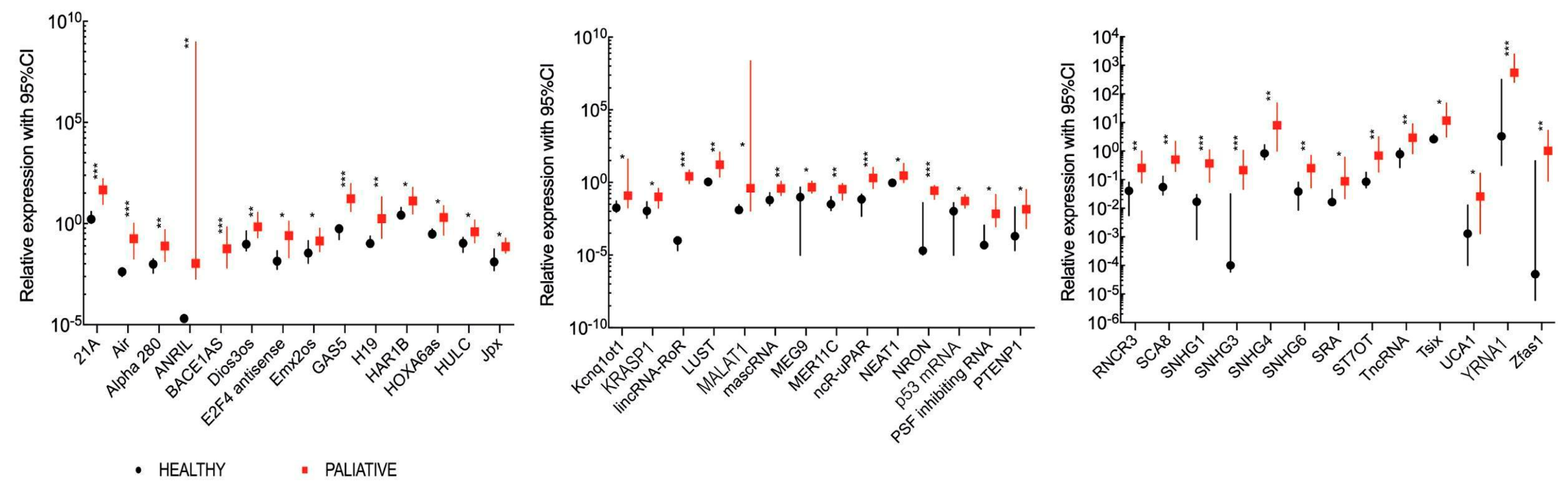
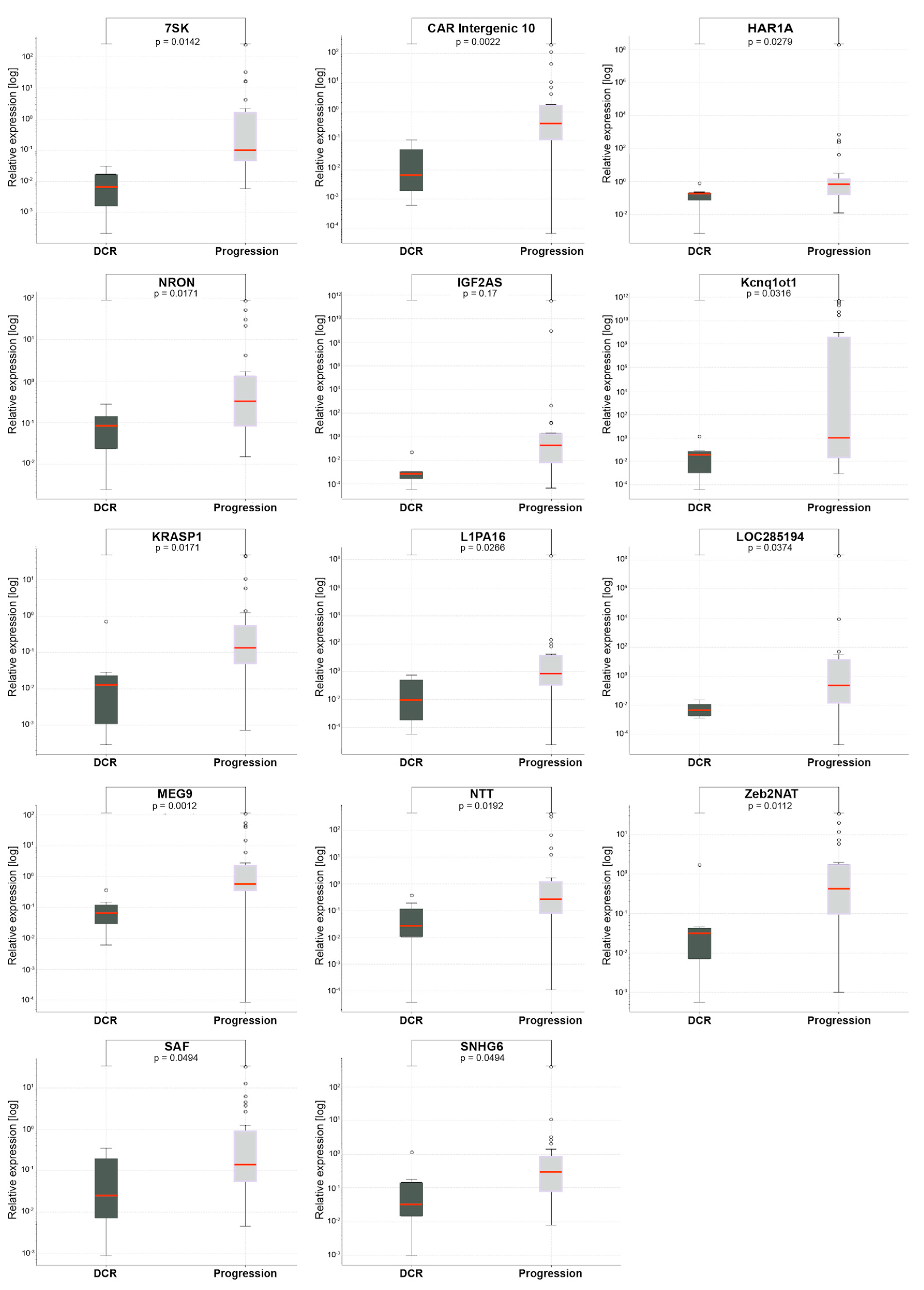
4.5. Comparison of lncRNA Expression Levels According to Treatment Response in HNSCC Patients Receiving Palliative Chemotherapy
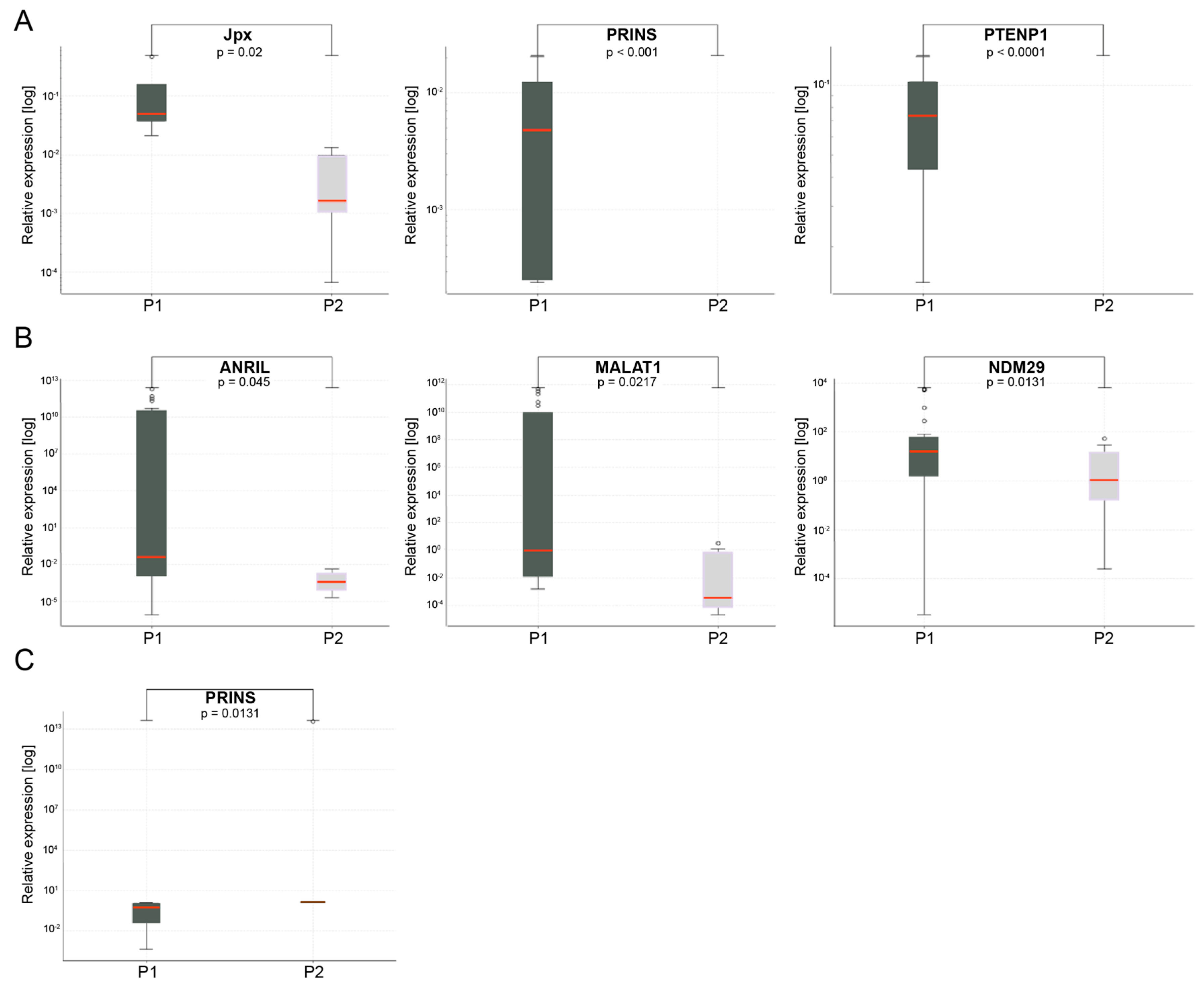
4.6. Changes in lncRNA Expression Levels during Induction Chemotherapy and Palliative Chemotherapy
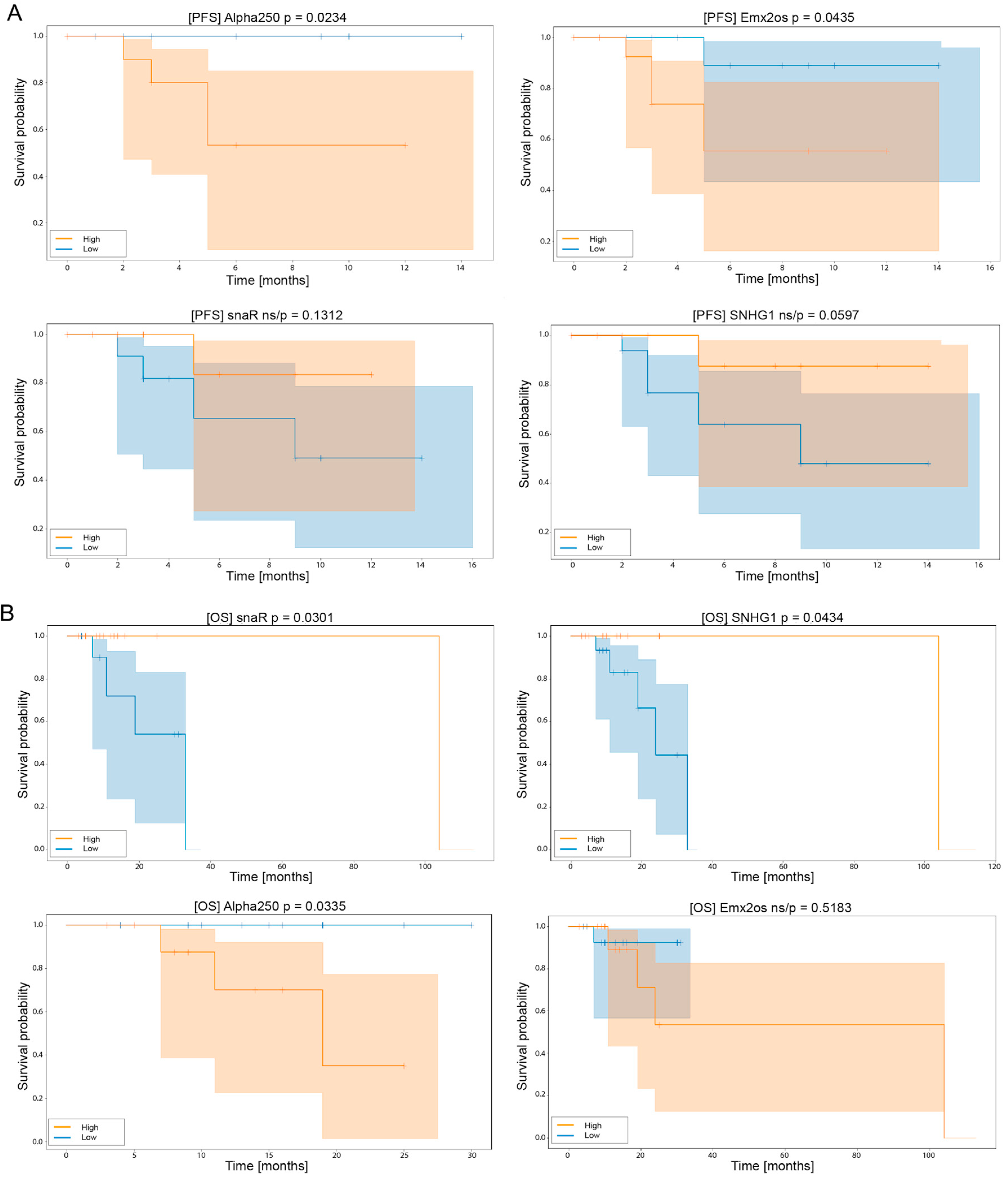
4.7. Assessment of lncRNA Expression in HNSCC Patients Receiving Palliative Chemotherapy Can Serve as a Prognostic Biomarker
4.8. lncRNA Expression Levels and Clinical and Laboratory Parameters of HNSCC Patients
5. Discussion
6. Conclusions, Limitation and Future Perspective
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of Data and Materials
Ethics Approval
References
- Shield, K.D.; Ferlay, F.; Jemal, A.; Sankaranarayanan, R.; Chaturvedi, A.K.; Bray, F.; Soerjomataram, I. The global incidence of lip, oral cavity, and pharyngeal cancers by subsite in 2012. CA Cancer J. Clin. 2017, 67, 51–56. [Google Scholar] [CrossRef]
- Tsao, S.W.; Tsang, C.M.; Lo, K.W. Epstein-Barr virus infection and nasopharyngeal carcinoma. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2017, 372, 20160270. [Google Scholar] [CrossRef] [PubMed]
- The Cancer Genome Atlas Network. Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature 2015, 517, 576–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonella, L.; Giannoccaro, M.; Alfieri, S.; Canevari, S.; De Cecco, L. Gene Expression Signatures for Head and Neck Cancer Patient Stratification: Are Results Ready for Clinical Application? Curr. Treat. Options Oncol. 2017, 18, 32. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.; Young, R.J.; Rischin, D. Head and neck squamous cell carcinoma: Genomics and emerging biomarkers for immunomodulatory cancer treatments. Semin. Cancer Biol. 2018, 52, 228–240. [Google Scholar] [CrossRef]
- Sannigrahi, M.K.; Sharma, R.; Panda, N.K.; Khullar, M. Role of non-coding RNAs in head and neck squamous cell carcinoma: A narrative review. Oral Dis. 2018, 24, 1417–1427. [Google Scholar] [CrossRef] [PubMed]
- Guglas, K.; Bogaczyńska, M.; Kolenda, T.; Ryś, M.; Teresiak, A.; Bliźniak, R.; Łasińska, I.; Mackiewicz, J.; Lamperska, K. lncRNA in HNSCC: Challenges and potential. Contemp. Oncol. 2017, 21, 259–266. [Google Scholar] [CrossRef] [Green Version]
- Arantes, L.M.R.B.; De Carvalho, A.C.; Melendez, M.E.; Carvalho, A.L. Serum, plasma and saliva biomarkers for head and neck cancer. Expert Rev. Mol. Diagn. 2018, 18, 85–112. [Google Scholar] [CrossRef]
- Orgel, L.E.; Crick, F.H.C. Selfish DNA: The ultimate parasite. Nature 1980, 284, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Niu, D.K.; Jiang, L. Can ENCODE tell us how much junk DNA we carry in our genome? Biochem. Biophys. Res. Commun. 2013, 430, 1340–1343. [Google Scholar] [CrossRef] [PubMed]
- Kiss, T. Biogenesis of small nuclear RNPs. J. Cell Sci. 2004, 117, 5949–5951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prensner, J.R.; Chinnaiyan, A.M. The emergence of lncRNAs in cancer biology. Cancer Discov. 2011, 1, 391–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, A.Q.; Nolasco, S.; Soares, H. Non-Coding RNAs: Multi-Tasking Molecules in the Cell. Int. J. Mol. Sci. 2013, 14, 16010–16039. [Google Scholar] [CrossRef] [PubMed]
- Chi, Y.; Wang, D.; Yu, W.; Yang, J. Long Non-Coding RNA in the Pathogenesis of Cancers. Cells 2019, 8, 1015. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, A.M.; Chang, H.Y. Long Noncoding RNAs in Cancer Pathways. Cancer Cell 2016, 29, 452–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, R.W.; Wang, Y.; Chen, L.L. Cellular functions of long noncoding RNAs. Nat. Cell Biol. 2019, 21, 542–551. [Google Scholar] [CrossRef]
- Derrien, T.; Johnson, R.; Bussotti, G.; Tanzer, A.; Djebali, S.; Tilgner, H.; Guernec, G.; Martín, D.; Merkel, A.; Knowles, D.G.; et al. The GENCODE v7 catalog of human long noncoding RNAs: Analysis of their gene structure, evolution, and expression. Genome Res. 2012, 22, 1775–1789. [Google Scholar] [CrossRef] [Green Version]
- Johnsson, P.; Lipovich, L.; Grandér, D.; Morris, K.V. Evolutionary conservation of long non-coding RNAs; sequence, structure, function. Biochim. Biophys. Acta 2014, 1840, 1063–1071. [Google Scholar] [CrossRef] [Green Version]
- Hubbard, T.; Barker, D.; Birney, E.; Cameron, G.; Chen, Y.; Clark, L.; Cox, T.; Cuff, J.; Curwen, V.; Down, T.; et al. The Ensembl genome database project. Nucl. Acid Res. 2002, 30, 38–41. [Google Scholar] [CrossRef] [Green Version]
- Morris, K.V.; Mattick, J.S. The rise of regulatory RNA. Nat. Rev. Genet. 2014, 15, 423–437. [Google Scholar] [CrossRef] [Green Version]
- Iyer, M.K.; Niknafs, Y.S.; Malik, R. The landscape of long noncoding RNAs in the human transcriptome. Nat. Genet. 2015, 47, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Ji, Z.; Song, R.; Regev, A.; Struhl, K. Many lncRNAs, 5′UTRs and pseudogenes are translated and some are likely to Express functional proteins. eLife 2015, 4, e08890. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Yang, M.; Guo, H.; Yang, L.; Wu, J.; Li, R.; Liu, P.; Lian, Y.; Zheng, X.; Yan, J.; et al. Single-cell RNA-Seq profliling of human preimplantation embryos and embryonic stem cells. Nat. Struct. Mol. Biol. 2013, 20, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Pirogov, S.A.; Gvozdev, V.A.; Klenov, M.S. Long Noncoding RNAs and Stress Response in the Nucleolus. Cells 2019, 8, 668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guglas, K.; Kolenda, T.; Teresiak, A.; Kopczyńska, M.; Łasińska, I.; Mackiewicz, J.; Mackiewicz, A.; Lamperska, K. lncRNA Expression after Irradiation and Chemoexposure of HNSCC Cell Lines. Noncoding RNA 2018, 4, 33. [Google Scholar] [CrossRef] [Green Version]
- Puvvula, P.K. LncRNAs Regulatory Networks in Cellular Senescence. Int. J. Mol. Sci. 2019, 20, 2615. [Google Scholar] [CrossRef] [Green Version]
- Dahariya, S.; Paddibhatla, I.; Kumar, S.; Raghuwanshi, S.; Pallepati, A.; Gutti, R.K. Long non-coding RNA: Classification, biogenesis and functions in blood cells. Mol. Immunol. 2019, 112, 82–92. [Google Scholar] [CrossRef]
- Liu, S.; Liu, X.; Li, J.; Zhou, H.; Carr, M.J.; Zhang, Z.; Shi, W. Long noncoding RNAs: Novel regulators of virus-host interactions. Rev. Med. Virol. 2019, 29, e2046. [Google Scholar] [CrossRef]
- Lin, Y.H.; Wu, M.H.; Yeh, C.T.; Lin, K.H. Long Non-Coding RNAs as Mediators of Tumor Microenvironment and Liver Cancer Cell Communication. Int. J. Mol. Sci. 2018, 19, 3742. [Google Scholar] [CrossRef] [Green Version]
- Kung, J.T.; Colognori, D.; Lee, J.T. Long noncoding RNAs: Past, present, and future. Genetics 2013, 193, 651–669. [Google Scholar] [CrossRef] [Green Version]
- Kolenda, T.; Guglas, T.; Ryś, M.; Bogaczyńska, M.; Teresiak, A.; Bliźniak, R.; Łasińska, I.; Mackiewicz, J.; Lamperska, K. Biological role of long non-coding RNA in head and neck cancers. Rep. Pract. Oncol. Radiother. 2017, 22, 378–388. [Google Scholar] [CrossRef]
- Kolenda, T.; Guglas, K.; Kopczyńska, M.; Teresiak, A.; Bliźniak, R.; Mackiewicz, A.; Lamperska, K.; Mackiewicz, J. Oncogenic Role of ZFAS1 lncRNA in Head and Neck Squamous Cell Carcinomas. Cells 2019, 8, 366. [Google Scholar] [CrossRef] [Green Version]
- Kolenda, T.; Kopczyńska, M.; Guglas, K.; Teresiak, A.; Bliźniak, R.; Łasińska, I.; Mackiewicz, J.; Lamperska, K. EGOT lncRNA in head and neck squamous cell carcinomas. Pol. J. Pathol. 2018, 69, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Wu, X.; Yin, J.; Li, M.; Shen, J.; Li, J.; Zhao, Y.; Zhao, Q.; Wu, J.; Wen, Q.; et al. Identification of Genetic Mutations in Cancer: Challenge and Opportunity in the New Era of Targeted Therapy. Front. Oncol. 2019, 9, 263. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network Website. Available online: https://www.nccn.org (accessed on 20 June 2020).
- Malone, E.; Siu, L.L. Precision Medicine in Head and Neck Cancer: Myth or Reality? Clin. Med. Insights Oncol. 2018, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens, N.; Nakagawa, S.; Sun, X.; Hoshida, Y. Cancer biomarker discovery and validation. Transl. Cancer Res. 2015, 4, 256–269. [Google Scholar]
- Lianidou, E.; Pantel, K. Liquid biopsies. Genes Chromosomes Cancer 2019, 58, 219–232. [Google Scholar] [CrossRef]
- Sole, C.; Arnaiz, E.; Manterola, L.; Otaegui, D.; Lawrie, C.H. The circulating transcriptome as a source of cancer liquid biopsy biomarkers. Semin. Cancer Biol. 2019, 58, 100–108. [Google Scholar] [CrossRef]
- Eisenauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumors: Revised RECIST guideline (version 1.1). Eur. J. Cancer Suppl. 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Lippi, G. Systematic Assessment of the Hemolysis Index: Pros and Cons. Adv. Clin. Chem. 2015, 71, 157–170. [Google Scholar]
- Kolenda, T.; Ryś, M.; Guglas, K.; Teresiak, A.; Bliźniak, R.; Mackiewicz, J.; Lamperska, K. Quantification of long non-coding RNAs using qRT-PCR: Comparison of different cDNA synthesis methods and RNA stability. Arch. Med. Sci. 2019, 15. [Google Scholar] [CrossRef] [Green Version]
- Thomas, G.R.; Shnayder, Y. Chapter 40—genomic evaluation of head and neck cancer A2—ginsburg, geoffrey S. In Essentials of Genomic and Personalized Medicine; Willard, H.F., Ed.; Academic Press: Cambridge, MA, USA, 2010; pp. 511–521. [Google Scholar]
- Kolenda, T.; Guglas, K.; Baranowski, D.; Sobocińska, J.; Kopczyńska, M.; Teresiak, A.; Bliźniak, R.; Lamperska, K. cfRNAs as biomarkers in oncology—Still experimental or applied tool for personalized medicine already? Rep. Pract. Oncol. Radiother. 2020, 25, 783–792. [Google Scholar] [CrossRef]
- Yao, Y.; Chen, X.; Lu, S.; Zhou, C.; Xu, G.; Yan, Z.; Yang, J.; Yu, T.; Chen, W.; Qian, Y.; et al. Circulating Long Noncoding RNAs as Biomarkers for Predicting Head and Neck Squamous Cell Carcinoma. Cell. Physiol. Biochem. 2018, 50, 1429–1440. [Google Scholar] [CrossRef]
- Lu, C.W.; Zhou, D.D.; Xie, T.; Hao, J.L.; Pant, O.P.; Lu, C.B.; Liu, X.F. HOXA11 antisense long noncoding RNA (HOXA11-AS): A promising lncRNA in human cancers. Cancer Med. 2018, 7, 3792–3799. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.Y.; Huang, C.; Wang, W.; Li, H.B.; Sun, M.; Xie, M. HOXA11-AS: A novel regulator in human cancer proliferation and metastasis. Onco Targets Ther. 2018, 11, 4387–4393. [Google Scholar] [CrossRef] [Green Version]
- Thin, K.Z.; Tu, J.C.; Raveendran, S. Long non-coding SNHG1 in cancer. Clin. Chim. Acta 2019, 494, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.X.; Jiang, H.; Xiang, G.Z.; Zhang, W.R.; Weng, Y.H.; Qiu, F.D.; Wu, J.; Wang, H.G. Up-regulation of long non-coding RNA SNHG1 contributes to proliferation and metastasis in laryngeal squamous cell carcinoma. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 1333–1341. [Google Scholar]
- Gao, L.; Cao, H.; Cheng, X. A positive feedback regulation between long noncoding RNA SNHG1 and YAP1 modulates growth and metastasis in laryngeal squamous cell carcinoma. Am. J. Cancer Res. 2018, 8, 1712–1724. [Google Scholar]
- Wang, L.; Su, K.; Wu, H.; Li, J.; Song, D. LncRNA SNHG3 regulates laryngeal carcinoma proliferation and migration by modulating the miR-384/WEE1 axis. Life Sci. 2019, 232, 116597. [Google Scholar] [CrossRef]
- Tang, Y.; Wu, L.; Zhao, M.; Zhao, G.; Mao, S.; Wang, L.; Liu, S.; Wang, X. LncRNA SNHG4 promotes the proliferation, migration, invasiveness, and epithelial-mesenchymal transition of lung cancer cells by regulating miR-98-5p. Biochem. Cell Biol. 2019, 97, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Wang, Y.; Zhao, Y.; Gu, X. LncRNA SNHG5 promotes nasopharyngeal carcinoma progression by regulating miR-1179/HMGB3 axis. BMC Cancer 2020, 20, 178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Qiu, D.; Xie, X.; Shen, Y. Clinicopathological and prognostic value of SNHG6 in cancers: A systematic review and a meta-analysis. BMC Cancer 2020, 20, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Wang, J.; Ma, K. Knockdown of lncRNA SNHG6 Inhibites the Proliferation and Epithelial Mesenchymal Transition in Tongue Cancer Cells. Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi 2018, 34, 806–811. [Google Scholar] [PubMed]
- Guo, T.; Zambo, K.D.A.; Zamuner, F.T.; Ou, T.; Hopkins, C.; Kelley, D.Z.; Wulf, H.A.; Winkler, E.; Erbe, R.; Danilova, L.V.; et al. Chromatin structure regulates cancer-specific alternative splicing events in primary HPV-related oropharyngeal squamous cell carcinoma. Epigenetics 2020, 15, 959–971. [Google Scholar] [CrossRef]
- Martinez, B.V.; Dhahbi, J.M.; Lopez, Y.O.M.; Lamperska, K.; Golusinski, P.; Luczewski, L.; Kolenda, T.; Atamna, H.; Spindler, S.R.; Golusinski, W.; et al. Circulating small non-coding RNA signature in head and neck squamous cell carcinoma. Oncotarget 2015, 6, 19246–19263. [Google Scholar] [CrossRef]
- Kolenda, T.; Rutkowski, P.; Michalak, M.; Kozak, K.; Guglas, K.; Ryś, M.; Galus, Ł.; Woźniak, S.; Ługowska, I.; Gos, A.; et al. Plasma lncRNA expression profile as a prognostic tool in BRAF-mutant metastatic melanoma patients treated with BRAF inhibitor. Oncotarget 2019, 10, 3879–3893. [Google Scholar] [CrossRef] [Green Version]
- Guglas, K.; Kolenda, T.; Stasiak, M.; Kopczyńska, M.; Teresiak, A.; Ibbs, M.; Bliźniak, R.; Lamperska, K. YRNAs: New Insights and Potential Novel Approach in Head and Neck Squamous Cell Carcinoma. Cells 2020, 9, 1281. [Google Scholar] [CrossRef]
- Guglas, K.; Kołodziejczak, I.; Kolenda, T.; Kopczyńska, M.; Teresiak, A.; Sobocińska, J.; Bliźniak, R.; Lamperska, K. YRNAs and YRNA-Derived Fragments as New Players in Cancer Research and Their Potential Role in Diagnostics. Int. J. Mol. Sci. 2020, 21, 5682. [Google Scholar] [CrossRef]
- Drewell, R.A.; Arney, K.L.; Arima, T.; Barton, S.C.; Brenton, J.D.; Surani, M.A. Novel conserved elements upstream of the H19 gene are transcribed and act as mesodermal enhancers. Development 2002, 129, 1205–1213. [Google Scholar]
- Song, C.; Song, C.; Chen, K.; Zhang, X. Inhibition of long non-coding RNA IGF2AS protects apoptosis and neuronal loss in anesthetic-damaged mouse neural stem cell derived neurons. Biomed. Pharmacother. 2017, 85, 2018–2024. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, X.; Hu, R.; Hao, L. Retraction: Prognostic implication and functional role of long noncoding RNA IGF2AS in human non-small cell lung cancer. J. Cell. Biochem. 2019, 20, 12067. [Google Scholar]
- Cohen, N.; Fedewa, S.; Chen, A.Y. Epidemiology and demographics of the head and neck cancer population. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 381–395. [Google Scholar] [CrossRef] [PubMed]
- Fayda, M.; Isin, M.; Tambas, M. Do circulating long non-coding RNAs (lncRNAs) (LincRNA-p21, GAS 5, HOTAIR) predict the treatment response in patients with head and neck cancer treated with chemoradiotherapy? Tumour Biol. 2016, 37, 3969–3978. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Xin, Y.; Zhou, L. Cisplatin and paclitaxel target significant long noncoding RNAs in laryngeal squamous cell carcinoma. Med. Oncol. 2014, 31, 246. [Google Scholar] [CrossRef]
- Ren, S.; Li, G.; Liu, C. Next generation deep sequencing identified a novel lncRNA n375709 associated with paclitaxel resistance in nasopharyngeal carcinoma. Oncol. Rep. 2016, 36, 1861–1867. [Google Scholar] [CrossRef]
- Li, L.; Gu, M.; You, B. Long non-coding RNA ROR promotes proliferation, migration and chemoresistance of nasopharyngeal carcinoma. Cancer Sci. 2016, 107, 1215–1222. [Google Scholar] [CrossRef]
- Tasheva, E.S.; Roufa, D.S. Regulation of human RPS14 transcription by intronic antisense RNAs and ribosomal protein S14. Genes Dev. 1995, 9, 304–316. [Google Scholar] [CrossRef] [Green Version]
- Tang, Z.; Wei, G.; Zhang, L.; Xu, Z. Signature microRNAs and long noncoding RNAs in laryngeal cancer recurrence identified using a competing endogenous RNA network. Mol. Med. Rep. 2019, 19, 4806–4818. [Google Scholar] [CrossRef] [Green Version]
- Liang, K.; Yang, Y.; Zha, D.; Yue, B.; Qiu, J.; Zhang, C. Overexpression of lncRNA snaR is correlated with progression and predicts poor survival of laryngeal squamous cell carcinoma. J. Cell. Biochem. 2018. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group Stratification | PFS | OS | ||||
|---|---|---|---|---|---|---|---|
| p-Val | HR | 95% CI | p-Val | HR | 95% CI | ||
| Age | <61 vs. >61 | 0.82 | 0.80 | 0.16–4.2 | 0.30 | 0.41 | 0.06–2.61 |
| NLR | <5 vs. >5 | 0.54 | 0.60 | 0.12–3.06 | 0.90 | 0.51 | 0.19–6.25 |
| BMI | <18.49 vs. >25 | 0.89 | 1.10 | 0.22–5.75 | 0.46 | 2.15 | 0.28–16.8 |
| Primary tumor localization | Pharynx vs. oral cavity | 0.40 | 0.67 | 0.01–30.1 | 0.44 | 0.23 | 0.0–10.48 |
| Primary tumor localization | Pharynx vs. larynx | 0.40 | 0.67 | 0.01–30.1 | 0.44 | 0.23 | 0.0–10.48 |
| Primary tumor localization | Pharynx vs. salivary gland | 0.40 | 0.67 | 0.01–30.1 | 0.44 | 0.23 | 0.0–10.48 |
| Primary tumor localization | Oral cavity vs. salivary gland | 0.46 | 1.80 | 0.36–9.27 | 0.44 | 0.22 | 0.14–8.60 |
| Primary tumor localization | Larynx vs. salivary gland | 0.90 | 1.10 | 0.21–5.76 | 0.90 | 1.09 | 0.14–8.60 |
| lncRNA Alpha 250 | High vs. low expression | 0.039 | 0.10 | 0.01–0.89 | 0.042 | 0.20 | 0.01–0.88 |
| lncRNA Emx2os | High vs. low expression | 0.13 | 0.26 | 0.04–1.54 | - | - | - |
| lncRNA snaR | High vs. low expression | - | - | - | 0.20 | 3.0 | 0.45–20.50 |
| lncRNA SNHG1 | High vs. low expression | - | - | - | 0.10 | 6.9 | 0.66–74.12 |
| Parameter | Group Stratification | PFS | OS | ||||
|---|---|---|---|---|---|---|---|
| p-Val | HR | 95%CI | p-Val | HR | 95%CI | ||
| Age | <61 vs. >61 | 0.90 | 0.84 | 0.02–30.31 | 0.60 | 0.48 | 0.03–9.05 |
| NLR | <5 vs. >5 | 0.90 | 0.86 | 0.02–33.56 | 0.90 | 0.80 | 0.06–12.33 |
| BMI | <18.49 vs. >25 | 0.90 | 1.09 | 0.22–47.52 | 0.90 | 1.01 | 0.02–43.42 |
| Primary tumor localization | Pharynx vs. oral cavity | 0.90 | 0.91 | 0–285.89 | 0.80 | 0.23 | 0–135.53 |
| Primary tumor localization | Pharynx vs. larynx | 0.90 | 0.91 | 0–285.89 | 0.80 | 0.69 | 0–135.53 |
| Primary tumor localization | Pharynx vs. salivary gland | 0.90 | 0.91 | 0–285.89 | 0.80 | 0.60 | 0–135.53 |
| Primary tumor localization | Oral cavity vs. salivary gland | 0.80 | 1.48 | 0.04–55.74 | 0.90 | 0.80 | 0.04–19.84 |
| Primary tumor localization | Larynx vs. salivary gland | 0.90 | 0.93 | 0.2–37.21 | 0.70 | 1.73 | 0.07–41.21 |
| lncRNA Alpha 250 | High vs. low expression | 0.039 | 0.20 | 0.01–0.87 | 0.043 | 0.30 | 0.02–0.89 |
| lncRNA Emx2os | High vs. low expression | 0.80 | 0.67 | 0.02–24.62 | - | - | - |
| lncRNA snaR | High vs. low expression | - | - | - | 0.40 | 3.07 | 0.17–55.67 |
| lncRNA SNHG1 | high vs. low expression | - | - | - | 0.50 | 2.77 | 0.14–54.37 |
| Parameter | Alpha 250 | Emx2os | snaR | SNHG1 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median | Lower Quartile | Upper Quartile | p-Val | Median | Lower Quartile | Upper Quartile | p-Val | Median | Lower Quartile | Upper Quartile | p-Val | Median | Lower Quartile | Upper Quartile | p-Val | |
| Age | ||||||||||||||||
| >61 | 0.0035 | 0.0014 | 0.0826 | 0.6525 | 0.2418 | 0.0257 | 0.5946 | 0.6525 | 12.1099 | 7.024 | 26.7425 | 0.0183 | 0.5092 | 0.1419 | 1.3947 | 0.3046 |
| <61 | 0.0679 | 0.007 | 1.2219 | 0.0804 | 0.0462 | 0.3803 | 2.514 | 0.7354 | 5.9042 | 0.2833 | 0.037 | 1.1563 | ||||
| Sex | ||||||||||||||||
| Female | 73.826 | 0.0932 | 155.012 | 0.7974 | 0.1554 | 0.0352 | 40.359 | 0.9071 | 12.261 | 0.4948 | 930.9114 | 0.6916 | 0.348 | 0.0224 | 43.1257 | 0.7616 |
| Male | 0.0095 | 0.0026 | 0.1151 | 0.1181 | 0.0458 | 0.5864 | 4.7372 | 1.2829 | 17.1813 | 0.4133 | 0.1042 | 1.1313 | ||||
| Nicotinism | ||||||||||||||||
| Yes | 0.0446 | 0.0072 | 0.6322 | 0.2826 | 0.484 | 0.0473 | 1.1299 | 0.7293 | 10.3091 | 1.8426 | 31.6433 | 0.4775 | 0.6552 | 0.3728 | 1.16 | 0.1216 |
| No | 0.0065 | 0.0024 | 0.2138 | 0.1031 | 0.0311 | 0.2635 | 2.7132 | 0.3886 | 10.6872 | 0.1672 | 0.0715 | 0.6246 | ||||
| Alcoholism | ||||||||||||||||
| Yes | 0.1486 | 0.0089 | 0.9224 | 0.8107 | 0.2418 | 0.0518 | 2.3202 | 0.6718 | 5.5867 | 1.8152 | 25.3311 | 0.6451 | 0.3728 | 0.0641 | 1.1551 | 0.5932 |
| No | 0.0035 | 0.002 | 0.0396 | 0.1106 | 0.0348 | 0.5187 | 5.5404 | 0.6406 | 12.1099 | 0.4601 | 0.0881 | 1.5281 | ||||
| BMI | ||||||||||||||||
| N | 0.024 | 0.0029 | 0.1724 | 0.5619 | 0.2132 | 0.0907 | 0.4404 | 0.9255 | 3.934 | 2.0813 | 12.261 | 0.779 | 0.4756 | 0.139 | 1.4659 | 0.779 |
| PN | 0.0099 | 0.0024 | 0.532 | 0.0595 | 0.0284 | 0.8953 | 7.0999 | 0.844 | 22.5037 | 0.3253 | 0.0739 | 1.0851 | ||||
| NLR 1 | ||||||||||||||||
| >5 | 0.1254 | 0.0055 | 0.4669 | 0.2862 | 0.2418 | 0.0518 | 0.3917 | 0.2701 | 4.4906 | 0.6604 | 13.9262 | 0.8708 | 0.3524 | 0.045 | 0.9596 | 0.7863 |
| <5 | 0.0067 | 0.001 | 0.0772 | 0.1022 | 0.0247 | 0.5926 | 5.5404 | 1.5491 | 29.7874 | 0.4298 | 0.1075 | 2.0887 | ||||
| PLR 1 | ||||||||||||||||
| >215 | 0.0399 | 0.0032 | 0.2521 | 0.4602 | 0.2635 | 0.0555 | 0.7589 | 0.1886 | 2.4156 | 0.8338 | 11.3605 | 0.3775 | 0.2184 | 0.0565 | 0.7585 | 0.3219 |
| <215 | 0.0098 | 0.0018 | 0.2011 | 0.0804 | 0.0298 | 0.5809 | 9.1135 | 2.514 | 35.8773 | 0.5257 | 0.148 | 2.425 | ||||
| Stage | ||||||||||||||||
| IVA | 0.0026 | 0.0005 | 0.0035 | 0.215 | 0.1031 | 0.0257 | 0.5864 | 0.7916 | 0.976 | 0.2823 | 9.1135 | 0.1378 | 0.0823 | 0.0213 | 0.4832 | 0.0401 |
| IVC | 0.0679 | 0.0093 | 0.3368 | 0.1629 | 0.0458 | 0.5763 | 6.268 | 2.1179 | 23.6976 | 0.4601 | 0.1672 | 1.1551 | ||||
| Localization | ||||||||||||||||
| Pharynx | 0.2011 | 0.1021 | 0.4869 | 0.245 | 0.2465 | 0.076 | 0.557 | 0.6652 | 3.934 | 2.3602 | 17.083 | 0.4077 | 0.3994 | 0.2391 | 0.7773 | 0.5987 |
| Larynx | 0.0293 | 0.0037 | 0.2107 | 0.0518 | 0.0341 | 0.2938 | 3.8109 | 1.1966 | 9.4315 | 0.2778 | 0.0773 | 0.8421 | ||||
| Salivary gland | 0.0001 | 0.0001 | 0.0026 | 0.3061 | 0.0177 | 11.5981 | 69.1904 | 23.6976 | 81.0084 | 2.1747 | 0.4275 | 33.5545 | ||||
| Oral cavity | 0.025 | 0.0082 | 0.2494 | 0.1908 | 0.0704 | 0.59 | 2.7132 | 1.3064 | 10.5361 | 0.2972 | 0.0739 | 0.7585 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Łasińska, I.; Kolenda, T.; Guglas, K.; Kopczyńska, M.; Sobocińska, J.; Teresiak, A.; Strzelecki, N.O.; Lamperska, K.; Mackiewicz, A.; Mackiewicz, J. Liquid lncRNA Biopsy for the Evaluation of Locally Advanced and Metastatic Squamous Cell Carcinomas of the Head and Neck. J. Pers. Med. 2020, 10, 131. https://doi.org/10.3390/jpm10030131
Łasińska I, Kolenda T, Guglas K, Kopczyńska M, Sobocińska J, Teresiak A, Strzelecki NO, Lamperska K, Mackiewicz A, Mackiewicz J. Liquid lncRNA Biopsy for the Evaluation of Locally Advanced and Metastatic Squamous Cell Carcinomas of the Head and Neck. Journal of Personalized Medicine. 2020; 10(3):131. https://doi.org/10.3390/jpm10030131
Chicago/Turabian StyleŁasińska, Izabela, Tomasz Kolenda, Kacper Guglas, Magda Kopczyńska, Joanna Sobocińska, Anna Teresiak, Norbert Oksza Strzelecki, Katarzyna Lamperska, Andrzej Mackiewicz, and Jacek Mackiewicz. 2020. "Liquid lncRNA Biopsy for the Evaluation of Locally Advanced and Metastatic Squamous Cell Carcinomas of the Head and Neck" Journal of Personalized Medicine 10, no. 3: 131. https://doi.org/10.3390/jpm10030131