rs622342 in SLC22A1, CYP2C9*2 and CYP2C9*3 and Glycemic Response in Individuals with Type 2 Diabetes Mellitus Receiving Metformin/Sulfonylurea Combination Therapy: 6-Month Follow-Up Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement and Patient Recruitment
2.2. Biochemical Measurements
2.3. DNA Sampling and Genotyping
2.4. Statistical Analysis
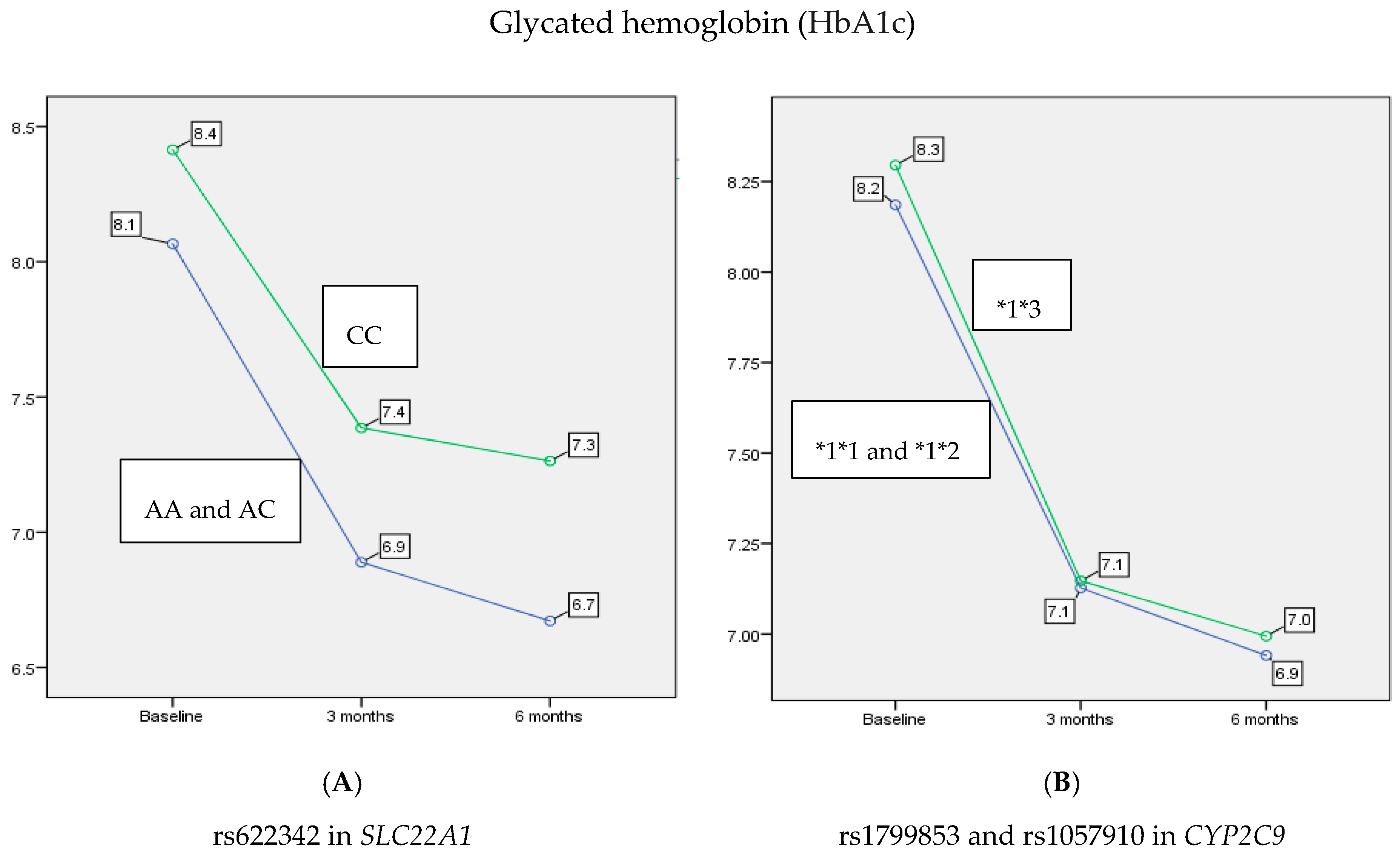
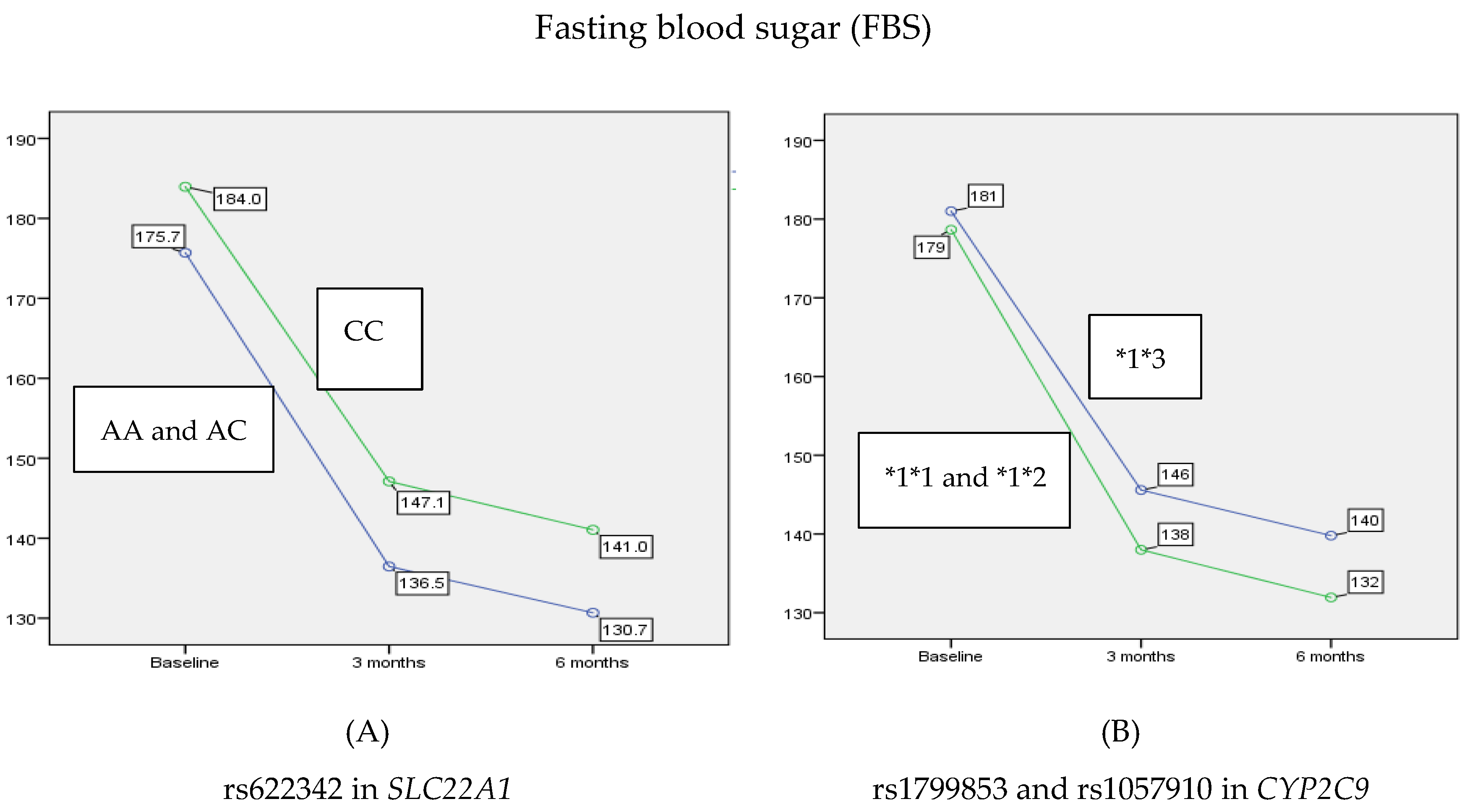
3. Results
4. Discussion
5. Conclusions and Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Harreiter, J.; Roden, M. Diabetes mellitus—Definition, Klassifikation, Diagnose, Screening und Prävention (Update 2019). Wien. Klin. Wochenschr. 2019, 131, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Javeed, N.; Matveyenko, A.V. Circadian Etiology of Type 2 Diabetes Mellitus. Physiology 2018, 33, 138–150. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, A.B.; Zhang, N.; van der Pluijm, W. Global Prevalence of Type 2 Diabetes over the Next Ten Years (2018–2028). Diabetes 2018, 67, 202. [Google Scholar] [CrossRef]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2017, 14, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.Y.; Lee, S.J.; Lee, S.; Kim, S.J.; Han, S.J.; Kim, H.J.; Kim, D.J.; Kim, Y.S.; Woo, J.T.; Ahn, K.J.; et al. Failure of monotherapy in clinical practice in patients with type 2 diabetes: The Korean National Diabetes Program. J. Diabetes Investig. 2018, 9, 1144–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, D.; Zhang, T.; Zheng, P.; Liang, Z.; Wang, S.; Xie, J.; Zhao, L.; Zhang, Y.; Situ, B. Comparison of Oral Antidiabetic Drugs as Add-On Treatments in Patients with Type 2 Diabetes Uncontrolled on Metformin: A Network Meta-Analysis. Diabetes Ther. 2018, 9, 1945–1958. [Google Scholar] [CrossRef] [PubMed]
- Mosenzon, O.; Leibowitz, G. VERIFY the role of initial combination therapy in patients with type 2 diabetes. Lancet 2019, 394, 1483–1485. [Google Scholar] [CrossRef]
- Rangel, E.S.; E Inzucchi, S. Metformin: Clinical use in type 2 diabetes. Diabetology 2017, 60, 1586–1593. [Google Scholar] [CrossRef]
- Davies, M.J.; D’Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018, 41, 2669–2701. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.-I. Second-line Glucose-Lowering Therapy in Type 2 Diabetes Mellitus. Curr. Diabetes Rep. 2019, 19, 54. [Google Scholar] [CrossRef]
- Genere, N.; Montori, V.M. Review: Newer second-line drugs for diabetes are not more cost-effective than sulfonylureas. Ann. Intern. Med. 2018, 168. [Google Scholar] [CrossRef] [PubMed]
- Ordelheide, A.-M.; de Angelis, M.H.; Häring, H.-U.; Staiger, H. Pharmacogenetics of oral antidiabetic therapy. Pharmacogenomics 2018, 19, 577–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, X.; Giacomini, K.M. Transporters Involved in Metformin Pharmacokinetics and Treatment Response. J. Pharm. Sci. 2017, 106, 2245–2250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Takizawa, M.; Chen, E.; Schlessinger, A.; Segenthelar, J.; Choi, J.H.; Sali, A.; Kubo, M.; Nakamura, S.; Iwamoto, Y.; et al. Genetic polymorphisms in organic cation transporter 1 (OCT1) in Chinese and Japanese populations exhibit altered function. J. Pharmacol. Exp. Ther. 2010, 335, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Naja, K.; El Shamieh, S.; Fakhoury, R. rs622342A>C in SLC22A1 is associated with metformin pharmacokinetics and glycemic response. Drug Metab. Pharmacokinet. 2020, 35, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Chiba, K.; Shimizu, K.; Kato, M.; Miyazaki, T.; Nishibayashi, T.; Terada, K.; Sugiyama, Y. Estimation of Interindividual Variability of Pharmacokinetics of CYP2C9 Substrates in Humans. J. Pharm. Sci. 2017, 106, 2695–2703. [Google Scholar] [CrossRef] [Green Version]
- Adak, T.; Samadi, A.; Ünal, A.Z.; Sabuncuoglu, S. A reappraisal on metformin. Regul. Toxicol. Pharmacol. 2018, 92, 324–332. [Google Scholar] [CrossRef]
- Song, J.; Yang, Y.; Mauvais-Jarvis, F.; Wang, Y.-P.; Niu, T. KCNJ11, ABCC8 and TCF7L2 polymorphisms and the response to sulfonylurea treatment in patients with type 2 diabetes: A bioinformatics assessment. BMC Med Genet. 2017, 18, 64. [Google Scholar] [CrossRef]
- Becker, M.; Visser, L.E.; van Schaik, R.H.N.; Hofman, A.; Uitterlinden, A.G.; Stricker, B.H. Genetic variation in the organic cation transporter 1 is associated with metformin response in patients with diabetes mellitus. Pharmacogenomics J. 2009, 9, 242–247. [Google Scholar] [CrossRef]
- Umamaheswaran, G.; Praveen, R.G.; Damodaran, S.E.; Das, A.K.; Adithan, C. Influence of SLC22A1 rs622342 genetic polymorphism on metformin response in South Indian type 2 diabetes mellitus patients. Clin. Exp. Med. 2014, 15, 511–517. [Google Scholar] [CrossRef]
- Reséndiz-Abarca, C.A.; Flores-Alfaro, E.; Suárez-Sánchez, F.; Cruz, M.; Valladares-Salgado, A.; Alarcón-Romero, L.D.C.; Vázquez-Moreno, M.A.; Wacher-Rodarte, N.A.; Gomez-Zamudio, J. Altered Glycemic Control Associated With Polymorphisms in the SLC22A1 (OCT1) Gene in a Mexican Population With Type 2 Diabetes Mellitus Treated With Metformin: A Cohort Study. J. Clin. Pharmacol. 2019, 59, 1384–1390. [Google Scholar] [CrossRef] [PubMed]
- Ebid, A.-H.I.M.; Ehab, M.; Ismail, A.; Soror, S.; Mahmoud, M. The influence of SLC22A1 rs622342 and ABCC8 rs757110 genetic variants on the efficacy of metformin and glimepiride combination therapy in Egyptian patients with type 2 diabetes. J. Drug Assess. 2019, 8, 115–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, K.; Donnelly, L.; Burch, L.; Tavendale, R.; Doney, A.S.F.; Leese, G.; Hattersley, A.T.; McCarthy, M.I.; Morris, A.D.; Lang, C.C.; et al. Loss-of-Function CYP2C9 Variants Improve Therapeutic Response to Sulfonylureas in Type 2 Diabetes: A Go-DARTS Study. Clin. Pharmacol. Ther. 2009, 87, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Surendiran, A.; Pradhan, S.C.; Agrawal, A.; Subrahmanyam, D.K.S.; Rajan, S.; Anichavezhi, D.; Adithan, S. Influence of CYP2C9 gene polymorphisms on response to glibenclamide in type 2 diabetes mellitus patients. Eur. J. Clin. Pharmacol. 2011, 67, 797–801. [Google Scholar] [CrossRef] [PubMed]
- Castelán-Martínez, O.D.; Hoyo-Vadillo, C.; Bazán-Soto, T.B.; Cruz, M.; Tesoro-Cruz, E.; Valladares-Salgado, A. CYP2C9*3 gene variant contributes independently to glycaemic control in patients with type 2 diabetes treated with glibenclamide. J. Clin. Pharm. Ther. 2018, 43, 768–774. [Google Scholar] [CrossRef]
- Molina-Guarneros, J.A.; Cuautle-Rodríguez, P.; Rodríguez-Rivera, N.; de Andrés, F.; Castillo-Nájera, F.; Llerena, A. Frequency of CYP2C9 (*2, *3 and IVS8-109A>T) allelic variants, and their clinical implications, among Mexican patients with diabetes mellitus type 2 undergoing treatment with glibenclamide and metformin. Biomed. Rep. 2019, 10, 283–295. [Google Scholar] [CrossRef] [Green Version]
- Klen, J.; Dolžan, V.; Janez, A. CYP2C9, KCNJ11 and ABCC8 polymorphisms and the response to sulphonylurea treatment in type 2 diabetes patients. Eur. J. Clin. Pharmacol. 2014, 70, 421–428. [Google Scholar] [CrossRef]
- Chen, L.; Li, J.H.; Kaur, V.; Muhammad, A.; Fernandez, M.; Hudson, M.S.; Goldfine, A.B.; Florez, J.C. The presence of two reduced function variants in CYP2C9 influences the acute response to glipizide. Diabet. Med. 2019. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Study Participants (n = 88) |
|---|---|
| Age | 56.6 ± 5 |
| Gender n (%) | |
| Male | 54 (61.4) |
| Female | 34 (38.6) |
| BMI (Kg/m2) | 25.13 ± 1.35 |
| MAF | |
| rs622342 in SLC22A1 | 0.41 |
| Genotypes | |
| AA n (%) | 33 (37.5) |
| AC n (%) | 38 (43.2) |
| CC n (%) | 17 (19.3) |
| rs1799853/rs1057910 in CYP2C9 | 0.31 |
| Genotypes | |
| *1*1 n (%) | 51 (58.0) |
| *1*2 n (%) | 20 (22.7) |
| *1*3 n (%) | 17 (19.3) |
| Variables | Baseline | After 3 Months | After 6 Months | p |
|---|---|---|---|---|
| HbA1c (mmol/mol) | 8.1 ± 0.4 | 7.03 ± 0.44 | 6.84 ± 0.4 | <0.001 |
| FBS (mg/dL) | 177.6 ± 12.7 | 140.2 ± 15.6 | 134.7 ± 15.4 | <0.001 |
| Total cholesterol (mg/dL) | 215.3 ± 16.6 | 208.9 ± 14.7 | 203.7 ± 15.4 | <0.001 |
| LDL-C (mg/dL) | 135.3 ± 18.3 | 128.6 ± 16.3 | 120.1 ± 17.5 | <0.001 |
| HDL-C (mg/dL) | 42.7 ± 5.3 | 45.7 ± 4.9 | 47.7 ± 5.18 | <0.001 |
| Triglycerides (mg/dL) | 175.4 ± 15.5 | 165.1 ± 14.2 | 161.7 ± 13.83 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naja, K.; Salami, A.; El Shamieh, S.; Fakhoury, R. rs622342 in SLC22A1, CYP2C9*2 and CYP2C9*3 and Glycemic Response in Individuals with Type 2 Diabetes Mellitus Receiving Metformin/Sulfonylurea Combination Therapy: 6-Month Follow-Up Study. J. Pers. Med. 2020, 10, 53. https://doi.org/10.3390/jpm10020053
Naja K, Salami A, El Shamieh S, Fakhoury R. rs622342 in SLC22A1, CYP2C9*2 and CYP2C9*3 and Glycemic Response in Individuals with Type 2 Diabetes Mellitus Receiving Metformin/Sulfonylurea Combination Therapy: 6-Month Follow-Up Study. Journal of Personalized Medicine. 2020; 10(2):53. https://doi.org/10.3390/jpm10020053
Chicago/Turabian StyleNaja, Khaled, Ali Salami, Said El Shamieh, and Rajaa Fakhoury. 2020. "rs622342 in SLC22A1, CYP2C9*2 and CYP2C9*3 and Glycemic Response in Individuals with Type 2 Diabetes Mellitus Receiving Metformin/Sulfonylurea Combination Therapy: 6-Month Follow-Up Study" Journal of Personalized Medicine 10, no. 2: 53. https://doi.org/10.3390/jpm10020053