Equilibrium CT Texture Analysis for the Evaluation of Hepatic Fibrosis: Preliminary Evaluation against Histopathology and Extracellular Volume Fraction

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Histological Analysis
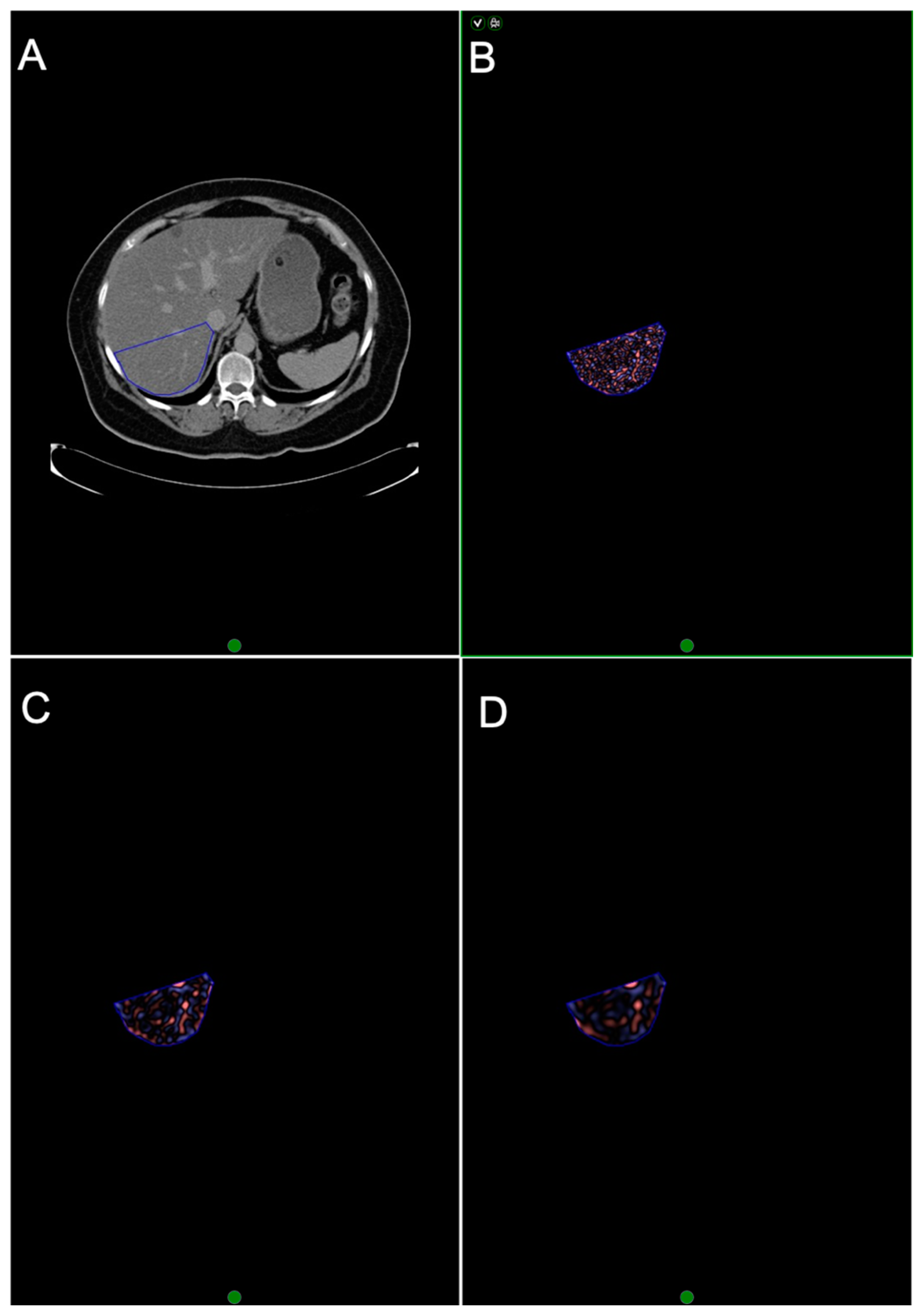
2.3. EQ-CT
2.4. CTTA
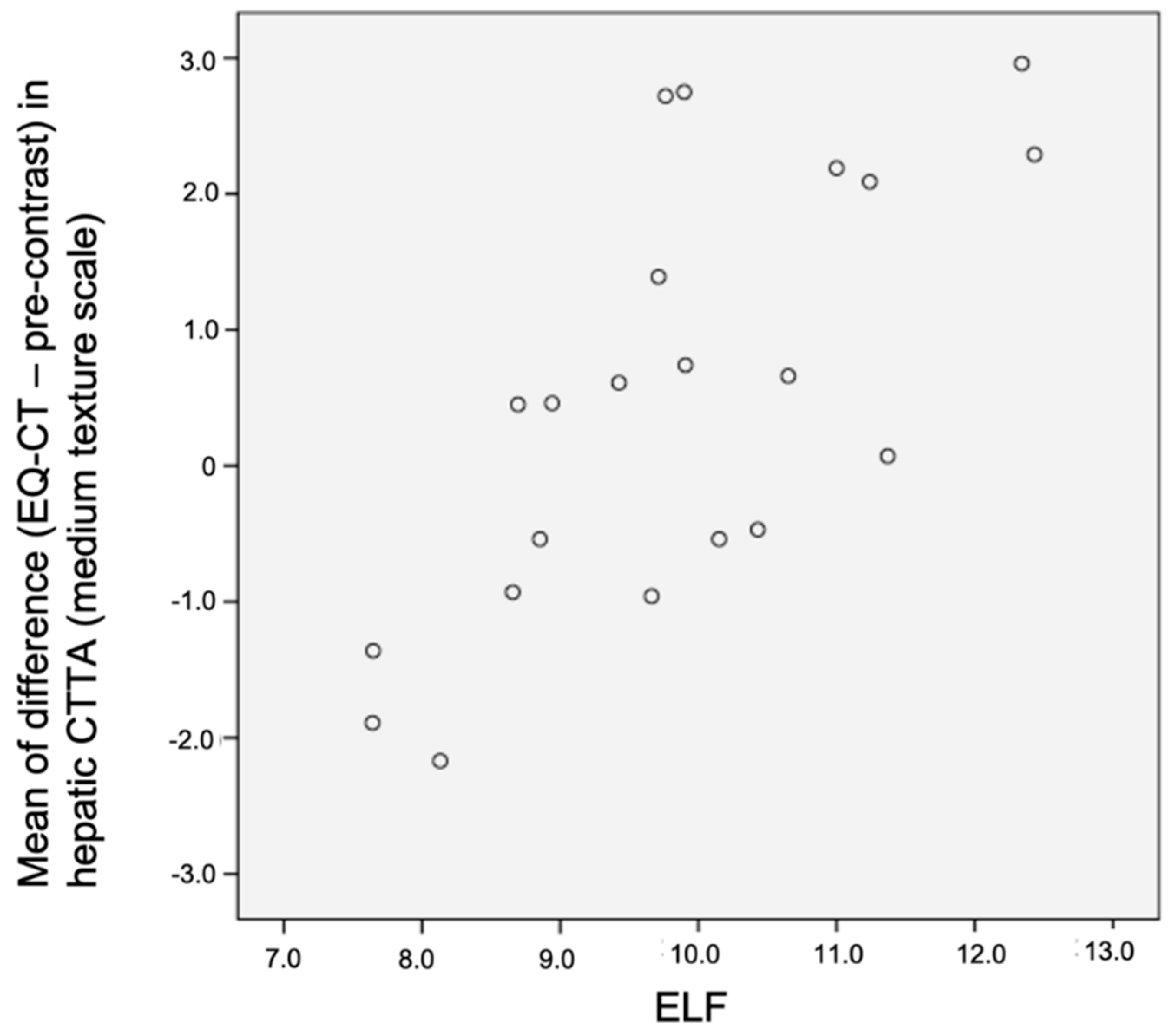
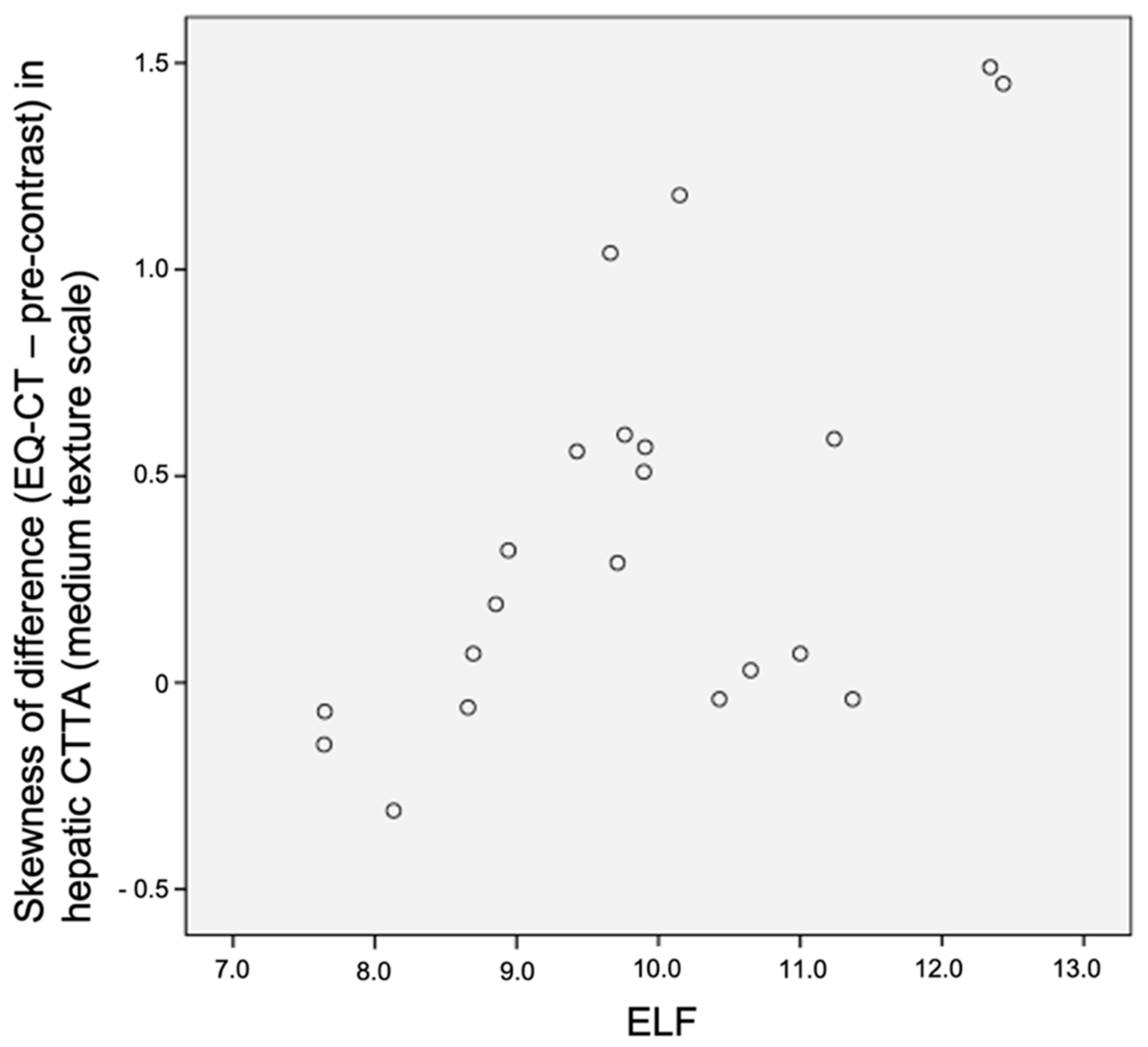
2.5. ELF Test Biomarker
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bosetti, C.; Levi, F.; Lucchini, F.; Zatonski, W.A.; Negri, E.; La Vecchia, C. Worldwide mortality from cirrhosis: An update to 2002. J. Hepatol. 2007, 46, 827–839. [Google Scholar] [CrossRef] [PubMed]
- Cowie, B.C.; Carville, K.S.; MacLachlan, J.H. Mortality due to viral hepatitis in the Global Burden of Disease Study 2010: New evidence of an urgent global public health priority demanding action. Antivir. Ther. 2013, 18, 953–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Axley, P.; Ahmed, Z.; Arora, S.; Haas, A.; Kuo, Y.-F.; Kamath, P.S. NASH is most rapidly growing etiology for acute-on-chronic liver failure related hospitalization and disease burden in the US. Liver Transplant. 2019, 25, 695–705. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, T.; Friedman, S.L. Mechanisms of hepatic stellate cell activation. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 397–411. [Google Scholar]
- Alpers, D.H.; Yamada, T. Textbook of Gastroenterology, 5th ed.; Wiley-Blackwell: Chichester, UK, 2009. [Google Scholar]
- Gilmore, I.T.; Burroughs, A.; Murray-Lyon, I.M.; Williams, R.; Jenkins, D.; Hopkins, A. Indications, methods, and outcomes of percutaneous liver biopsy in England and Wales: An audit by the British Society of Gastroenterology and the Royal College of Physicians of London. Gut 1995, 536, 437–441. [Google Scholar] [CrossRef] [Green Version]
- Regev, A.; Berho, M.; Jeffers, L.J.; Milikowski, C.; Molina, E.G.; Pyrsopoulos, N.T.; Feng, Z.Z.; Reddy, K.R.; Schiff, E.R. Sampling error and intraobserver variation in liver biopsy in patients with chronic HCV infection. Am. J. Gastroenterol. 2002, 97, 2614–2618. [Google Scholar] [CrossRef]
- Rosenberg, W.M.; Voelker, M.; Thiel, R.; Becka, M.; Burt, A.; Schuppan, D.; Hubscher, S.; Roskams, T.; Pinzani, M.; Arthur, M.J.; et al. Serum markers detect the presence of liver fibrosis: A cohort study. Gastroenterology 2004, 127, 1704–1713. [Google Scholar] [CrossRef] [Green Version]
- Bandula, S.; Punwani, S.; Rosenberg, W.M.; Jalan, R.; Hall, A.R.; Dhillon, A.; Moon, J.C.; Taylor, S.A. Equilibrium contrast-enhanced CT imaging to evaluate hepatic fibrosis: Initial validation by comparison with histopathologic sampling. Radiology 2015, 275, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Lubner, M.G.; Malecki, K.; Kloke, J.; Ganeshan, B.; Pickhardt, P.J. Texture analysis of the liver at MDCT for assessing hepatic fibrosis. Abdom. Radiol. 2017, 42, 2069–2078. [Google Scholar] [CrossRef]
- Daginawala, N.; Li, B.; Buch, K.; Yu, H.; Tischler, B.; Qureshi, M.M.; Soto, J.A.; Anderson, S. Using texture analyses of contrast enhanced CT to assess hepatic fibrosis. Eur. J. Radiol. 2016, 85, 511–517. [Google Scholar] [CrossRef]
- Zhang, X.; Gao, X.; Liu, B.J.; Ma, K.; Yan, W.; Liling, L.; Yuhong, H.; Fujita, H. Effective staging of fibrosis by the selected texture features of liver: Which one is better, CT or MR imaging? Comput. Med. Imaging Graph. 2015, 46 Pt 2, 227–236. [Google Scholar] [CrossRef]
- Naganawa, S.; Enooku, K.; Tateishi, R.; Akai, H.; Yasaka, K.; Shibahara, J.; Ushiku, T.; Abe, O.; Ohtomo, K.; Kiryu, S. Imaging prediction of nonalcoholic steatohepatitis using computed tomography texture analysis. Eur. Radiol. 2018, 28, 3050–3058. [Google Scholar] [PubMed]
- Cannella, R.; Borhani, A.A.; Tublin, M.; Behari, J.; Furlan, A. Diagnostic value of MR-based texture analysis for the assessment of hepatic fibrosis in patients with nonalcoholic fatty liver disease (NAFLD). Abdom. Radiol. 2019, 44, 1816–1824. [Google Scholar]
- Menghini, G. One-second biopsy of the liver--problems of its clinical application. N. Engl. J. Med. 1970, 283, 582–585. [Google Scholar] [CrossRef] [PubMed]
- Cholongitas, E.; Burroughs, A.K. Liver: Transjugular liver biopsy yields high-quality samples. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 491–492. [Google Scholar]
- Knodell, R.G.; Ishak, K.G.; Black, W.C.; Chen, T.S.; Craig, R.; Kaplowitz, N.; Kiernan, T.W.; Wollman, J. Formulation and application of a numerical scoring system for assessing histological activity in asymptomatic chronic active hepatitis. Hepatology 1981, 1, 431–435. [Google Scholar] [CrossRef]
- Calvaruso, V.; Burroughs, A.K.; Standish, R.; Manousou, P.; Grillo, F.; Leandro, G.; Maimone, S.; Pleguezuelo, M.; Xirouchakis, I.; Piero Guerrini, G.; et al. Computer-assisted image analysis of liver collagen: Relationship to Ishak scoring and hepatic venous pressure gradient. Hepatology 2009, 49, 1236–1244. [Google Scholar]
- Yeung, J.; Sivarajan, S.; Treibel, T.A.; Rosmini, S.; Fontana, M.; Gillmore, J.D.; Hawkins, P.N.; Punwani, S.; Moon, J.C.; Taylor, S.A.; et al. Measurement of liver and spleen interstitial volume in patients with systemic amyloid light-chain amyloidosis using equilibrium contrast CT. Abdom. Radiol. 2017, 42, 2646–2651. [Google Scholar]
- Bandula, S.; White, S.K.; Flett, A.S.; Lawrence, D.; Pugliese, F.; Ashworth, M.T.; Punwani, S.; Taylor, S.A.; Moon, J.C. Measurement of myocardial extracellular volume fraction by using equilibrium contrast-enhanced CT: Validation against histologic findings. Radiology 2013, 269, 396–403. [Google Scholar]
- Miles, K.A.; Ganeshan, B.; Hayball, M.P. CT texture analysis using the filtration-histogram method: What do the measurements mean? Cancer Imaging 2013, 13, 400–406. [Google Scholar] [CrossRef] [Green Version]
- Mahmoud-Ghoneim, D.; Toussaint, G.; Constans, J.M.; de Certaines, J.D. Three dimensional texture analysis in MRI: A preliminary evaluation in gliomas. Magn. Reson. Imaging 2003, 21, 983–987. [Google Scholar] [PubMed]
- Park, H.J.; Kim, J.H.; Choi, S.Y.; Lee, E.S.; Park, S.J.; Byun, J.Y.; Choi, B.I. Prediction of Therapeutic Response of Hepatocellular Carcinoma to Transcatheter Arterial Chemoembolization Based on Pretherapeutic Dynamic CT and Textural Findings. Am. J. Roentgenol. 2017, 209, W211–W220. [Google Scholar]
- Chen, W.; Giger, M.L.; Li, H.; Bick, U.; Newstead, G.M. Volumetric texture analysis of breast lesions on contrast-enhanced magnetic resonance images. Magn. Reson. Med. 2007, 58, 562–571. [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Whole Liver | Liver Segment VII | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EQ-contrast minus pre-contrast | EQ-contrast minus pre-contrast | ||||||||||||||||
| Mean | Skewness | Mean | Skewness | ||||||||||||||
| SSF (mm) | 3 | 4 | 5 | 6 | 3 | 4 | 5 | 6 | 3 | 4 | 5 | 6 | 3 | 4 | 5 | 6 | |
| ELF | rs | −0.03 | −0.088 | −0.103 | −0.094 | −0.352 | −0.253 | −0.032 | 0.235 | 0.435 | 0.642 | 0.694 | 0.609 | 0.571 | 0.530 | 0.443 | 0.282 |
| p-value | 0.898 | 0.703 | 0.658 | 0.687 | 0.118 | 0.268 | 0.889 | 0.305 | 0.049 | 0.002 | <0.001 | 0.003 | 0.007 | 0.013 | 0.044 | 0.216 | |
| Whole Liver | Liver Segment VII | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-contrast | EQ-contrast | Pre-contrast | EQ-contrast | |||||||||||
| SD | Entropy | MPP | SD | Entropy | MPP | SD | Entropy | MPP | SD | Entropy | MPP | |||
| SSF: 6 mm | CPA | rs | −0.663 | −0.597 | −0.554 | −0.524 | −0.502 | −0.584 | −0.555 | −0.472 | −0.368 | −0.404 | −0.601 | −0.378 |
| p-value | <0.001 | 0.001 | 0.002 | 0.015 | 0.02 | 0.005 | 0.002 | 0.01 | 0.049 | 0.07 | 0.004 | 0.091 | ||
| ECV | rs | −0.513 | −0.463 | −0.455 | −0.560 | −0.582 | −0.518 | −0.400 | −0.299 | −0.286 | −0.550 | −0.637 | −0.43 | |
| p-value | 0.004 | 0.011 | 0.013 | 0.008 | 0.006 | 0.016 | 0.032 | 0.115 | 0.132 | 0.010 | 0.002 | 0.052 | ||
| SSF: 5 mm | CPA | rs | −0.628 | −0.582 | −0.585 | −0.497 | −0.481 | −0.520 | −0.463 | −0.452 | −0.386 | −0.364 | −0.574 | −0.516 |
| p-value | <0.001 | 0.001 | 0.001 | 0.022 | 0.027 | 0.016 | 0.012 | 0.014 | 0.038 | 0.104 | 0.006 | 0.017 | ||
| ECV | rs | −0.483 | −0.393 | −0.448 | −0.571 | −0.557 | −0.588 | −0.368 | −0.318 | −0.332 | −0.591 | −0.628 | −0.414 | |
| p-value | 0.008 | 0.035 | 0.015 | 0.007 | 0.009 | 0.005 | 0.05 | 0.093 | 0.078 | 0.005 | 0.002 | 0.062 | ||
| SSF: 4 mm | CPA | rs | −0.516 | −0.479 | −0.486 | −0.396 | −0.386 | −0.409 | −0.555 | −0.472 | −0.368 | −0.404 | −0.601 | −0.378 |
| p-value | 0.004 | 0.009 | 0.008 | 0.076 | 0.084 | 0.066 | 0.002 | 0.01 | 0.049 | 0.07 | 0.004 | 0.091 | ||
| ECV | rs | −0.388 | −0.322 | −0.351 | −0.543 | −0.492 | −0.555 | −0.4 | −0.299 | −0.286 | −0.550 | −0.637 | −0.43 | |
| p-value | 0.038 | 0.088 | 0.062 | 0.011 | 0.023 | 0.009 | 0.032 | 0.115 | 0.132 | 0.01 | 0.002 | 0.052 | ||
| SSF: 3 mm | CPA | rs | −0.377 | −0.342 | −0.314 | −0.383 | −0.37 | −0.399 | −0.379 | −0.351 | −0.332 | −0.402 | −0.422 | −0.427 |
| p-value | 0.044 | 0.07 | 0.097 | 0.087 | 0.099 | 0.073 | 0.043 | 0.062 | 0.079 | 0.071 | 0.057 | 0.054 | ||
| ECV | rs | −0.283 | −0.237 | −0.214 | −0.449 | −0.381 | −0.487 | −0.347 | −0.305 | −0.294 | −0.617 | −0.523 | −0.591 | |
| p-value | 0.137 | 0.217 | 0.264 | 0.041 | 0.088 | 0.025 | 0.065 | 0.107 | 0.122 | 0.003 | 0.015 | 0.005 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeung, J.; Ganeshan, B.; Endozo, R.; Hall, A.; Wan, S.; Groves, A.; Taylor, S.A.; Bandula, S. Equilibrium CT Texture Analysis for the Evaluation of Hepatic Fibrosis: Preliminary Evaluation against Histopathology and Extracellular Volume Fraction. J. Pers. Med. 2020, 10, 46. https://doi.org/10.3390/jpm10020046
Yeung J, Ganeshan B, Endozo R, Hall A, Wan S, Groves A, Taylor SA, Bandula S. Equilibrium CT Texture Analysis for the Evaluation of Hepatic Fibrosis: Preliminary Evaluation against Histopathology and Extracellular Volume Fraction. Journal of Personalized Medicine. 2020; 10(2):46. https://doi.org/10.3390/jpm10020046
Chicago/Turabian StyleYeung, Jason, Balaji Ganeshan, Raymond Endozo, Andrew Hall, Simon Wan, Ashley Groves, Stuart A. Taylor, and Steve Bandula. 2020. "Equilibrium CT Texture Analysis for the Evaluation of Hepatic Fibrosis: Preliminary Evaluation against Histopathology and Extracellular Volume Fraction" Journal of Personalized Medicine 10, no. 2: 46. https://doi.org/10.3390/jpm10020046