Impact of Implementing Antenatal Syphilis Point-of-Care Testing on Maternal Mortality in KwaZulu-Natal, South Africa: An Interrupted Time Series Analysis



Abstract
:1. Background
2. Methodology
2.1. Study Design, Population, and Location
2.2. Exposure
2.3. Data Extraction
2.4. Data analysis
2.5. Ethics Statement
3. Results
Summary of the Study Population and Sample Size
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNAIDS. The Gap Report. Available online: http://www.unaids.org/sites/default/files/media_asset/UNAIDS_Gap_report_en.pdf (accessed on 18 November 2019).
- Department of Health. National Strategic Plan on HIV, STIs and TB 2012–2016. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=3&ved=2ahUKEwiosYbwyZ3mAhXFGaYKHe2XBJEQFjACegQIBRAC&url=http%3A%2F%2Fwww.health.gov.za%2Findex.php%2Fshortcodes%2F2015-03-29-10-42-47%2F2015-04-30-08-18-10%2F2015-04-30-08-21-56%3Fdownload%3D579%3Ahiv-national-strategic-plan-on-hiv-stis-and-tb-2012-2016-summary&usg=AOvVaw2VI-h6VYlAzWt1sugeKjFt (accessed on 5 December 2019).
- Statistics South Africa. Mid-year Population Estimates. Available online: http://www.statssa.gov.za/publications/P0302/P03022019.pdf (accessed on 3 November 2019).
- Mashamba-Thompson, T.P.; Morgan, R.L.; Sartorius, B.; Dennis, B.; Drain, P.K.; Thabane, L. Effect of point-of-care diagnostics on maternal outcomes in human immunodeficiency virus–infected women: systematic review and meta-analysis. Point Care 2017, 16, 67. [Google Scholar] [CrossRef] [PubMed]
- Amnesty International. Struggle for Maternal Health Barriers to Antenatal Care in South Africa; 2014. Available online: https://cisp.cachefly.net/assets/articles/attachments/51965_amnesty_southafrica530062014en.pdf (accessed on 5 December 2019).
- Bronzan, R.N.; Mwesigwa-Kayongo, D.C.; Narkunas, D.; Schmid, G.P.; Neilsen, G.A.; Ballard, R.C.; Karuhije, P.; Ddamba, J.; Nombekela, E.; Hoyi, G. Onsite rapid antenatal syphilis screening with an immunochromatographic strip improves case detection and treatment in rural South African clinics. Sex. Transm. Dis. 2007, 34, S55–S60. [Google Scholar] [CrossRef] [PubMed]
- Pronyk, P.; Kim, J.; Makhubele, M.; Hargreaves, J.; Mohlala, R.; Hausler, H. Introduction of voluntary counselling and rapid testing for HIV in rural South Africa: From theory to practice. AIDS Care 2002, 14, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Dhatt, R.; Theobald, S.; Buzuzi, S.; Ros, B.; Vong, S.; Muraya, K.; Molyneux, S.; Hawkins, K.; González-Beiras, C.; Ronsin, K. The role of women’s leadership and gender equity in leadership and health system strengthening. Glob. HealthEpidemiol. Genom. 2017, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullick, S.; Beksinksa, M.; Msomi, S. Treatment for syphilis in antenatal care: Compliance with the three dose standard treatment regimen. Sex. Transm. Infect. 2005, 81, 220–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuupiel, D.; Tlou, B.; Bawontuo, V.; Mashamba-Thompson, T.P. Accessibility of pregnancy-related point-of-care diagnostic tests for maternal healthcare in rural primary healthcare facilities in Northern Ghana: A cross-sectional survey. Heliyon 2019, 5, e01236. [Google Scholar] [CrossRef] [Green Version]
- Kuupiel, D.; Adu, K.M.; Bawontuo, V.; Mashamba-Thompson, T.P. Geographical Accessibility to District Hospitals/Medical Laboratories for Comprehensive Antenatal Point-of-Care Diagnostic Services in the Upper East Region, Ghana. EClinicalMedicine 2019, 13, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Mabey, D.C.; Sollis, K.A.; Kelly, H.A.; Benzaken, A.S.; Bitarakwate, E.; Changalucha, J.; Chen, X.-S.; Yin, Y.-P.; Garcia, P.J.; Strasser, S. Point-of-care tests to strengthen health systems and save newborn lives: The case of syphilis. PLoS Med. 2012, 9, e1001233. [Google Scholar] [CrossRef] [Green Version]
- De Schacht, C.; Lucas, C.; Sitoe, N.; Machekano, R.; Chongo, P.; Temmerman, M.; Tobaiwa, O.; Guay, L.; Kassaye, S.; Jani, I.V. Implementation of point-of-care diagnostics leads to variable uptake of syphilis, anemia and CD4+ T-Cell count testing in rural maternal and child health clinics. PLoS ONE 2015, 10, e0135744. [Google Scholar] [CrossRef] [Green Version]
- Mashamba-Thompson, T.; Sartorius, B.; Drain, P. Operational assessment of point-of-care diagnostics in rural primary healthcare clinics of KwaZulu-Natal, South Africa: A cross-sectional survey. BMC Health Serv. Res. 2018, 18, 380. [Google Scholar] [CrossRef] [Green Version]
- Lynn, W.; Lightman, S. Syphilis and HIV: A dangerous combination. Lancet Infect. Dis. 2004, 4, 456–466. [Google Scholar] [CrossRef]
- Berman, S.M. Maternal syphilis: Pathophysiology and treatment. Bull. World Health Organ. 2004, 82, 433–438. [Google Scholar] [PubMed]
- Blencowe, H.; Cousens, S.; Kamb, M.; Berman, S.; Lawn, J.E. Lives Saved Tool supplement detection and treatment of syphilis in pregnancy to reduce syphilis related stillbirths and neonatal mortality. BMC Public Health 2011, 11, S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawkes, S.; Matin, N.; Broutet, N.; Low, N. Effectiveness of interventions to improve screening for syphilis in pregnancy: A systematic review and meta-analysis. Lancet Infect. Dis. 2011, 11, 684–691. [Google Scholar] [CrossRef]
- Buchacz, K.; Patel, P.; Taylor, M.; Kerndt, P.R.; Byers, R.H.; Holmberg, S.D.; Klausner, J.D. Syphilis increases HIV viral load and decreases CD4 cell counts in HIV-infected patients with new syphilis infections. Aids 2004, 18, 2075–2079. [Google Scholar] [CrossRef] [PubMed]
- Yeganeh, N.; Watts, H.D.; Camarca, M.; Soares, G.; Joao, E.; Pilotto, J.H.; Gray, G.; Theron, G.; Santos, B.; Fonseca, R. Syphilis in HIV-infected Mothers and Infants: Results from the NICHD/HPTN 040 Study. Pediatric Infect. Dis. J. 2015, 34, e52–e57. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.; Pillay, T.; Moodley, J.M.; Connolly, C.A.; Durban Perinatal TB HIV-1 Study Group. Maternal mortality associated with tuberculosis–HIV-1 co-infection in Durban, South Africa. Aids 2001, 15, 1857–1863. [Google Scholar] [CrossRef]
- Mashamba-Thompson, T.; Drain, P.; Sartorius, B. Evaluating the accessibility and utility of HIV-related point-of-care diagnostics for maternal health in rural South Africa: A study protocol. BMJ Open 2016, 6, e011155. [Google Scholar] [CrossRef]
- Shadish, W.R.; Cook, T.D.; Campbell, D.T. Experimental and quasi-experimental designs for generalized causal inference. J. Am. Stat. Assoc. 2005, 100, 708. [Google Scholar]
- Taljaard, M.; McKenzie, J.E.; Ramsay, C.R.; Grimshaw, J.M. The use of segmented regression in analysing interrupted time series studies: An example in pre-hospital ambulance care. Implement. Sci. 2014, 9, 77. [Google Scholar] [CrossRef] [Green Version]
- Mate, K.S.; Bennett, B.; Mphatswe, W.; Barker, P.; Rollins, N. Challenges for routine health system data management in a large public programme to prevent mother-to-child HIV transmission in South Africa. PLoS ONE 2009, 4, e5483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mphatswe, W.; Mate, K.S.; Bennett, B.; Ngidi, H.; Reddy, J.; Barker, P.M.; Rollins, N. Improving public health information: A data quality intervention in KwaZulu-Natal, South Africa. Bull. World Health Organ. 2012, 90, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.; Soumerai, S.; Zhang, F.; Ross-Degnan, D. Segmented regression analysis of interrupted time series studies in medication use research. J. Clin. Pharm. Ther. 2002, 27, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Campbell, D.T.; Stanley, J.C. Experimental and Quasi-Experimental Designs for Research; Ravenio Books: 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/44787/9789241502986_eng.pdf (accessed on 5 December 2019).
- Kharsany, A.B.; Frohlich, J.A.; Yende-Zuma, N.; Mahlase, G.; Samsunder, N.; Dellar, R.C.; Zuma-Mkhonza, M.; Karim, S.S.A.; Karim, Q.A. Trends in HIV prevalence in pregnant women in rural South Africa. Jaids J. Acquir. Immune Defic. Syndr. 2015, 70, 289–295. [Google Scholar] [CrossRef] [Green Version]
- Lagana, A.S.; Vitale, S.G.; Sapia, F.; Valenti, G.; Corrado, F.; Padula, F.; Rapisarda, A.M.C.; D’Anna, R. miRNA expression for early diagnosis of preeclampsia onset: Hope or hype? J. Matern.-Fetal Neonatal Med. 2018, 31, 817–821. [Google Scholar] [CrossRef]
- Laganà, A.S.; Giordano, D.; Loddo, S.; Zoccali, G.; Vitale, S.G.; Santamaria, A.; Buemi, M.; D’Anna, R. Decreased Endothelial Progenitor Cells (EPCs) and increased Natural Killer (NK) cells in peripheral blood as possible early markers of preeclampsia: A case-control analysis. Arch. Gynecol. Obstet. 2017, 295, 867–872. [Google Scholar] [CrossRef]
- Salman, H.; Shah, M.; Ali, A.; Aziz, A.; Vitale, S.G. Assessment of Relationship of Serum Neurokinin-B Level in the Pathophysiology of Pre-eclampsia: A Case–Control Study. Adv. Ther. 2018, 35, 1114–1121. [Google Scholar] [CrossRef]
- WHO; UNAiDS; Unicef. Global HIV/AIDS Response: Epidemic Update and Health Sector Progress Towards Universal Access: Progress Report 2011. Available online: https://scholar.google.com.hk/scholar?hl=zh-CN&as_sdt=0%2C5&q=34.%09WHo%2C+UNAiDS%2C+Unicef.+Global+HIV%2FAIDS+response%3A+Epidemic+update+and+health+sector+progress+towards+universal+access%3A+Progress+report+2011.&btnG=#d=gs_cit&u=%2Fscholar%3Fq%3Dinfo%3As_Alx9YRhYMJ%3Ascholar.google.com%2F%26output%3Dcite%26scirp%3D0%26hl%3Dzh-CN (accessed on 10 December 2019).
- Newman, L.; Kamb, M.; Hawkes, S.; Gomez, G.; Say, L.; Seuc, A.; Broutet, N. Global estimates of syphilis in pregnancy and associated adverse outcomes: Analysis of multinational antenatal surveillance data. PLoS Med. 2013, 10, e1001396. [Google Scholar] [CrossRef]
- Moline, H.R.; Smith, J.F., Jr. The continuing threat of syphilis in pregnancy. Curr. Opin. Obstet. Gynecol. 2016, 28, 101–104. [Google Scholar] [CrossRef]
- Lebastchi, A.H.; Yuh, D.D. Nationwide survey of US integrated 6-year cardiothoracic surgical residents. J. Thorac. Cardiovasc. Surg. 2014, 148, 401–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drain, P.K.; Hyle, E.P.; Noubary, F.; Freedberg, K.A.; Wilson, D.; Bishai, W.R.; Rodriguez, W.; Bassett, I.V. Diagnostic point-of-care tests in resource-limited settings. Lancet Infect. Dis. 2014, 14, 239–249. [Google Scholar] [CrossRef] [Green Version]
- Mabey, D.; Peeling, R.W.; Ustianowski, A.; Perkins, M.D. Diagnostics for the developing world. Nat. Rev. Microbiol. 2004, 2, 231–240. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
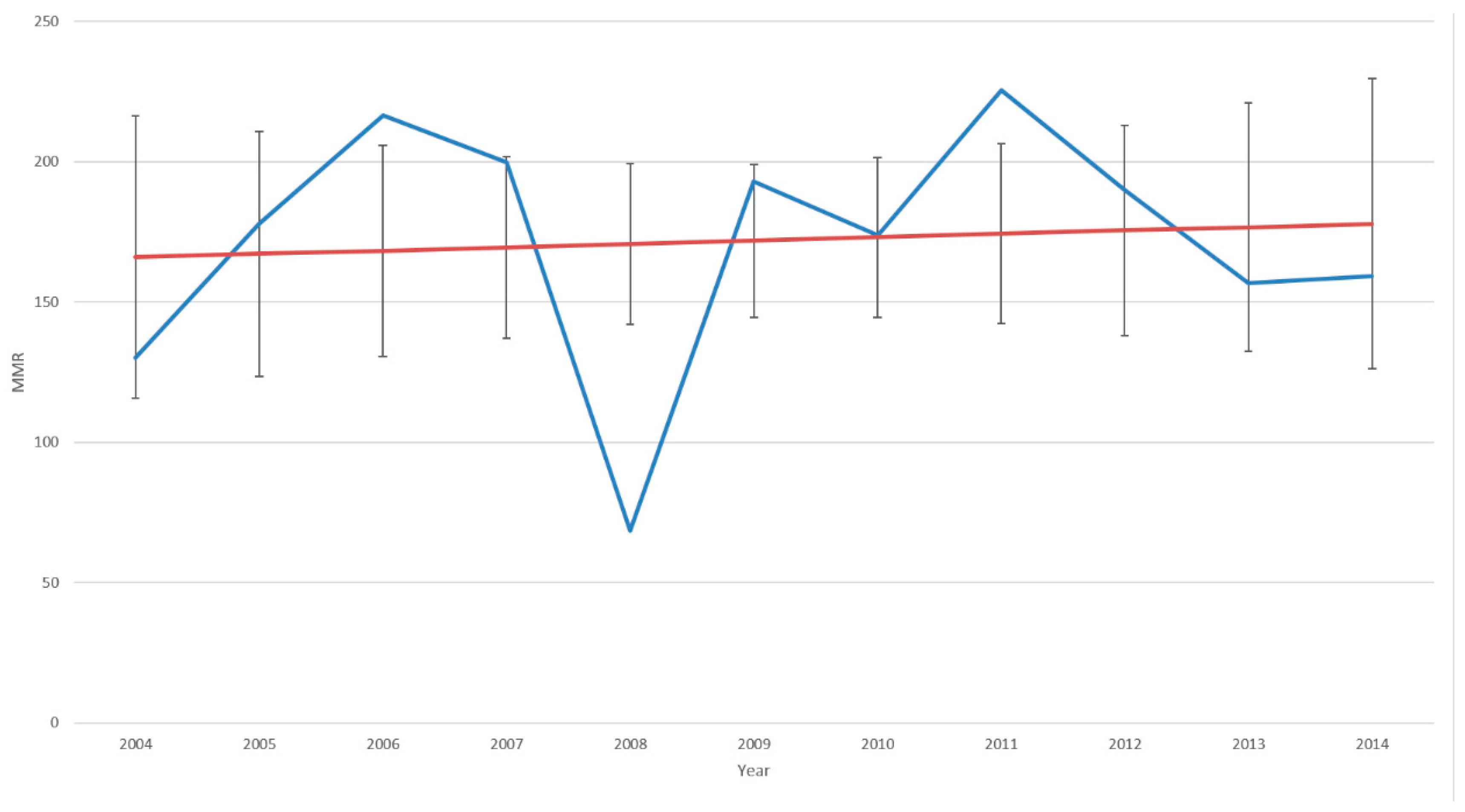
| Year | Number of Maternal Deaths in Facility | Number of Live Births in Facility | Maternal Mortality Ratio Per 100,000 Live Births |
|---|---|---|---|
| 2004 | 208 | 159712 | 130.23 |
| 2005 | 259 | 145617 | 177.86 |
| 2006 | 371 | 171230 | 216.67 |
| 2007 | 337 | 168580 | 199.91 |
| 2008 | 120 | 175227 | 68.48 |
| 2009 | 324 | 167847 | 193.03 |
| 2010 | 291 | 167544 | 173.69 |
| 2011 | 378 | 167637 | 225.49 |
| 2012 | 312 | 164322 | 189.87 |
| 2013 | 256 | 163411 | 156.66 |
| 2014 | 254 | 159484 | 159.26 |
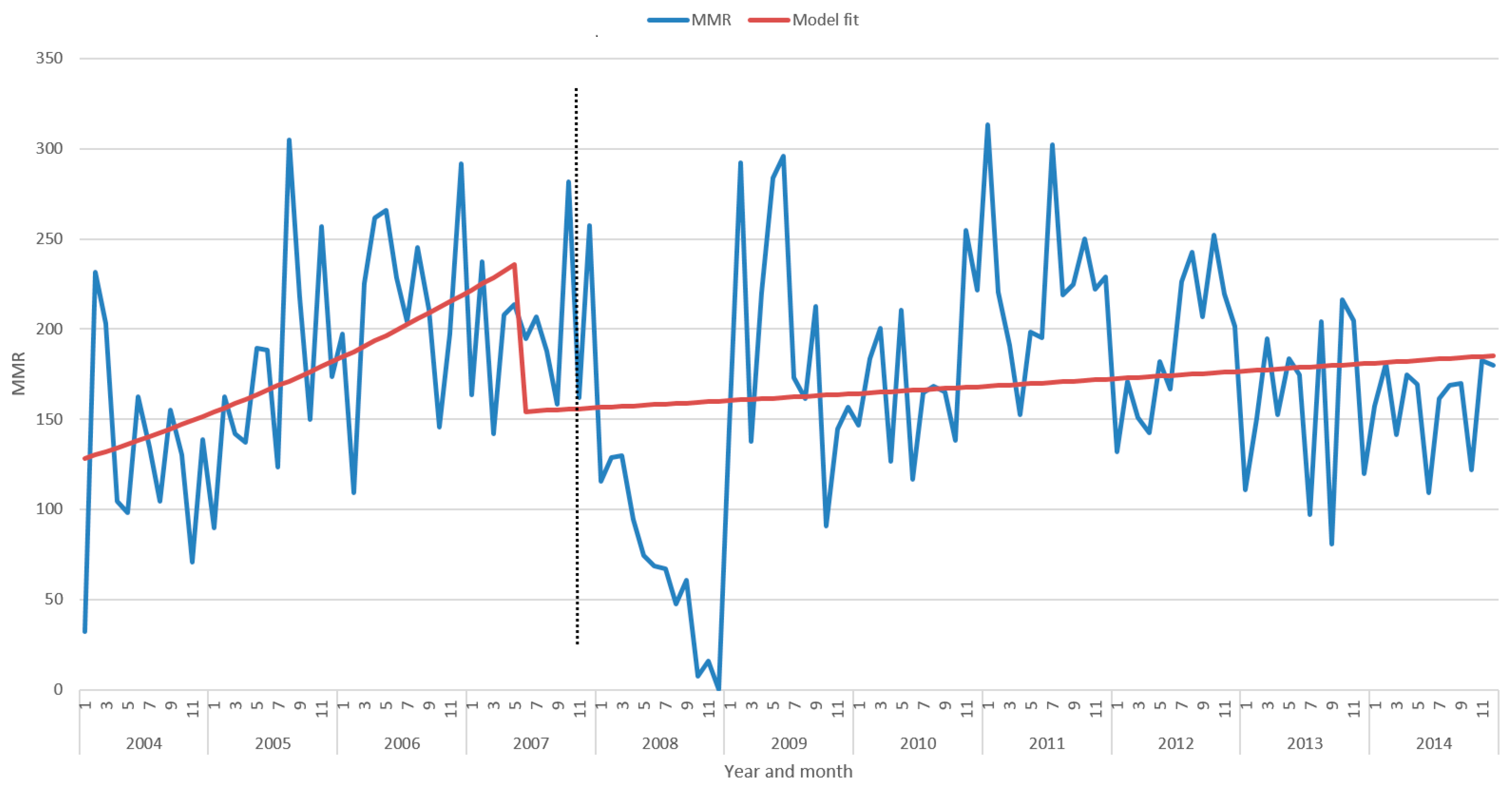
| Full Segmented Regression Model | RR | 95% CI | p Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| A0—Intercept i (2007, introduction of POC testing) | 0.001 | 0.001 | 0.001 | --- |
| A1—Baseline trend (before introduction of syphilis POC testing) | 1.015 | 1.01 | 1.021 | <0.001 |
| A2—Level change after introduction of syphilis POC testing | 0.653 | 0.567 | 0.752 | <0.001 |
| A3—Trend change introduction of syphilis POC testing | 0.987 | 0.981 | 0.992 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mashamba-Thompson, T.P.; Drain, P.K.; Kuupiel, D.; Sartorius, B. Impact of Implementing Antenatal Syphilis Point-of-Care Testing on Maternal Mortality in KwaZulu-Natal, South Africa: An Interrupted Time Series Analysis. Diagnostics 2019, 9, 218. https://doi.org/10.3390/diagnostics9040218
Mashamba-Thompson TP, Drain PK, Kuupiel D, Sartorius B. Impact of Implementing Antenatal Syphilis Point-of-Care Testing on Maternal Mortality in KwaZulu-Natal, South Africa: An Interrupted Time Series Analysis. Diagnostics. 2019; 9(4):218. https://doi.org/10.3390/diagnostics9040218
Chicago/Turabian StyleMashamba-Thompson, Tivani P., Paul K. Drain, Desmond Kuupiel, and Benn Sartorius. 2019. "Impact of Implementing Antenatal Syphilis Point-of-Care Testing on Maternal Mortality in KwaZulu-Natal, South Africa: An Interrupted Time Series Analysis" Diagnostics 9, no. 4: 218. https://doi.org/10.3390/diagnostics9040218