From Targeting Somatic Mutations to Finding Inherited Cancer Predispositions: The Other Side of the Coin


Abstract
:1. Introduction
2. Subjects and Methods
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| NGS | next-generation sequencing |
| ACMG | American College of Medical Genetics |
| SFMPP | Société française de médecine prédictive et personnalisée |
References
- Berger, M.F.; Mardis, E.R. The emerging clinical relevance of genomics in cancer medicine. Nat. Rev. Clin. Oncol. 2018, 15, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Mandelker, D.; Zhang, L. The emerging significance of secondary germline testing in cancer genomics. J. Pathol. 2018, 244, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Dumbrava, E.E.I.; Brusco, L.; Daniels, M.S.; Wathoo, C.; Shaw, K.R.; Lu, K.H.; Zheng, X.; Strong, L.C.; Litton, J.K.; Arun, B.; et al. Prevalence of incidental germline pathogenic (PV) and likely pathogenic (LPV) variants in hereditary cancer-related genes identified in matched tumor/normal sequencing of advanced solid tumors. J. Clin. Oncol. 2017, 35, 1524. [Google Scholar] [CrossRef]
- Abida, W.; Armenia, J.; Gopalan, A.; Brennan, R.; Walsh, M.; Barron, D.; Danila, D.; Rathkopf, D.; Morris, M.; Slovin, S.; et al. Prospective Genomic Profiling of Prostate Cancer Across Disease States Reveals Germline and Somatic Alterations That May Affect Clinical Decision Making. JCO Precis. Oncol. 2017, 1, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Pujol, P.; Perre, P.V.; Faivre, L.; Sanlaville, D.; Corsini, C.; Baertschi, B.; Anahory, M.; Vaur, D.; Olschwang, S.; Soufir, N.; et al. Guidelines for reporting secondary findings of genome sequencing in cancer genes: The SFMPP recommendations. Eur. J. Hum. Genet. 2018, 26, 1732–1742. [Google Scholar] [CrossRef] [PubMed]
- Media Tools Address from Anddi Rares. Available online: http://anddi-rares.org/bibliotheque-anddi-rares/films-anddi-rares/les-donnees-secondaires-issues-du-sequencage-haut-debit-du-genome.html (accessed on 17 October 2017).
- Green, R.C.; Berg, J.S.; Grody, W.W.; Kalia, S.S.; Korf, B.R.; Martin, C.L.; McGuire, A.L.; Nussbaum, R.L.; O’Daniel, J.M.; Ormond, K.E.; et al. American College of Medical Genetics and Genomics. ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing. Genet. Med. 2013, 15, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Colombo, N.; Huang, G.; Scambia, G.; Chalas, E.; Pignata, S.; Fiorica, J.; Le, L.V.; Ghamande, S.; González-Santiago, S.; Bover, I.; et al. Evaluation of a Streamlined Oncologist-Led BRCA Mutation Testing and Counseling Model for Patients with Ovarian Cancer. J. Clin. Oncol. 2018, 36, 1300–1307. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network: Genetic/Familial High-Risk Assessment: Breast and Ovarian. Version 1. 2018. Available online: https://www.nccn.org/ Google Scholar (accessed on 17 October 2017).
- Vergote, I.; Banerjee, S.; Gerdes, A.M.; van Asperen, C.; Marth, C.; Vaz, F.; Ray-Coquard, I.; Stoppa-Lyonnet, D.; Gonzalez-Martini, A.; Sehouli, J.; et al. Current perspectives on recommendations for BRCA genetic testing in ovarian cancer patients. Eur. J. Cancer 2016, 69, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Pennington, K.P.; Walsh, T.; Harrell, M.I.; Lee, M.K.; Pennil, C.C.; Rendi, M.H.; Thornton, A.; Norquist, B.M.; Casadei, S.; Nord, A.S.; et al. Germline and somatic mutations in homologous recombination genes predict platinum response and survival in ovarian, fallopian tube, and peritoneal carcinomas. Clin. Cancer Res. 2014, 20, 764–775. [Google Scholar] [CrossRef] [PubMed]
- The European Medicines Agency. p. 2014. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/lynparza (accessed on 15 July 2017).
- Enyedi, M.Z.; Jaksa, G.; Pintér, L.; Sükösd, F.; Gyuris, Z.; Hajdu, A.; Határvölgyi, E.; Priskin, K.; Haracska, L. Simultaneous detection of BRCA mutations and large genomic rearrangements in germline DNA and FFPE tumor samples. Oncotarget 2016, 7, 61845–61859. [Google Scholar] [CrossRef] [PubMed]
- Mafficini, A.; Simbolo, M.; Parisi, A.; Rusev, B.; Luchini, C.; Cataldo, I.; Piazzola, E.; Sperandio, N.; Turri, G.; Franchi, M.; et al. BRCA somatic and germline mutation detection in paraffin embedded ovarian cancers by next-generation sequencing. Oncotarget 2016, 7, 1076–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pujol, P.; Lyonnet, D.S.; Frebourg, T.; Blin, J.; Picot, M.C.; Lasset, C.; Dugast, C.; Berthet, P.; de Paillerets, B.B.; Sobol, H.; et al. Lack of referral for genetic counseling and testing in BRCA1/2 and Lynch syndromes: A nationwide study based on 240,134 consultations and 134,652 genetic tests. Breast Cancer Res. Treat. 2013, 141, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Menko, F.H.; Ter Stege, J.A.; van der Kolk, L.E.; Jeanson, K.N.; Schats, W.; Moha, D.A.; Bleiker, E.M.A. The uptake of presymptomatic genetic testing in hereditary breast-ovarian cancer and Lynch syndrome: A systematic review of the literature and implications for clinical practice. Fam. Cancer 2019, 18, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Slade, I.; Riddell, D.; Turnbull, C.; Hanson, H.; Rahman, N.; MCG programme. Development of cancer genetic services in the UK: A national consultation. Genome Med. 2015, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- INCa. Oncogénétique en 2016-Consultations, Laboratoires et Suivi. Collection Appui à la décision/Soins. December 2017. Available online: https://www.e-cancer.fr/Expertises-et-publications/Catalogue-des-publications/Oncogenetique-en-2016-Consultations-laboratoires-et-suivi (accessed on 15 July 2017).
- George, A.; Riddell, D.; Seal, S.; Talukdar, S.; Mahamdallie, S.; Ruark, E.; Cloke, V.; Slade, I.; Kemp, Z.; Gore, M.; et al. Implementing rapid, robust, cost-effective, patient-centred, routine genetic testing in ovarian cancer patients. Sci. Rep. 2016, 6, 29506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, K.S. Genetic Testing: What Problem Are We Trying to Solve? J. Clin. Oncol. 2017, 35, 3789–3791. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
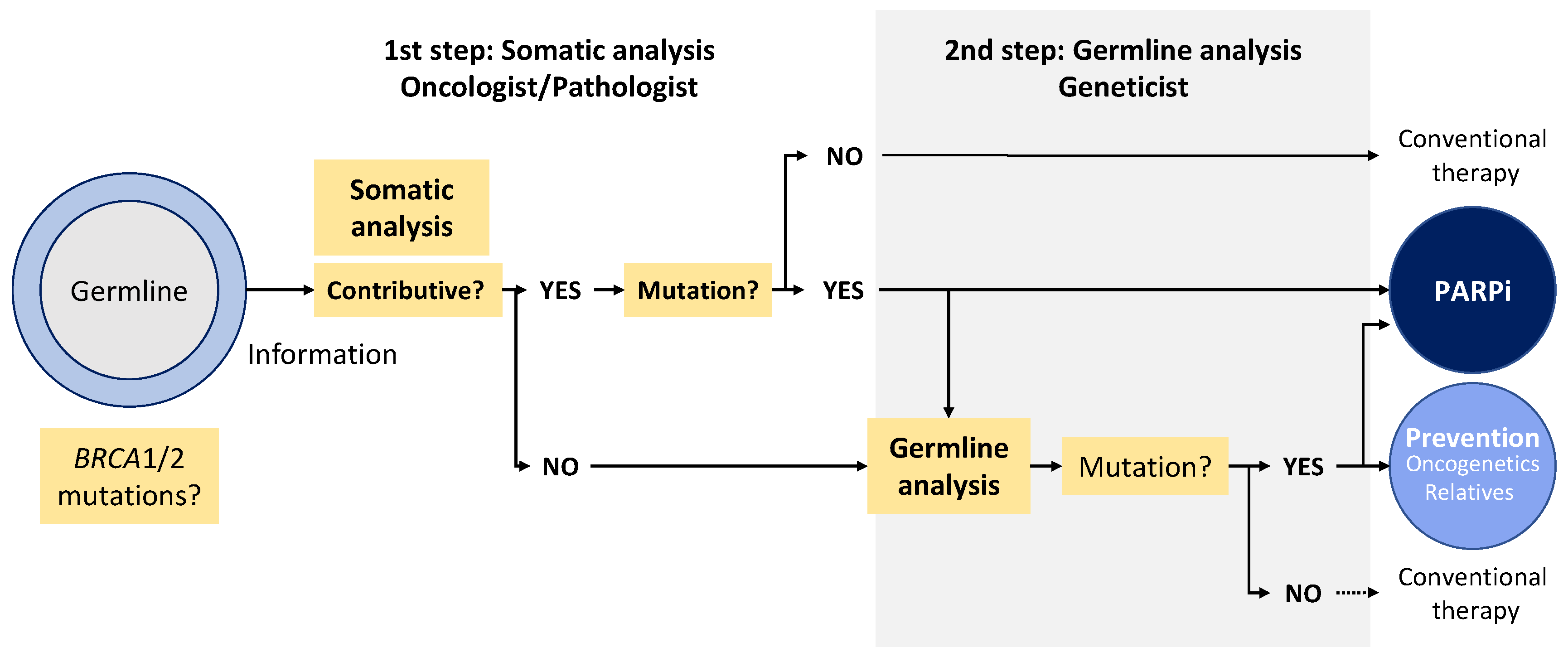
| Arguments in Favor of Starting with Somatic Analysis |
|---|
| Need to detect exclusive somatic mutation (5–7% ovarian cancer, breast?) |
| Possibility to detect large genomic rearrangement by somatic next-generation sequencing |
| Emergency of the results for therapeutic purpose |
| Cost (2 analyses systematically performed if starting by germline) |
| Oncologist more aware of BRCA issues and in first line |
| Most patients negative for BRCA mutation will not need genetic counselling |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pujol, P.; De La Motte Rouge, T.; Penault-Llorca, F. From Targeting Somatic Mutations to Finding Inherited Cancer Predispositions: The Other Side of the Coin. Diagnostics 2019, 9, 83. https://doi.org/10.3390/diagnostics9030083
Pujol P, De La Motte Rouge T, Penault-Llorca F. From Targeting Somatic Mutations to Finding Inherited Cancer Predispositions: The Other Side of the Coin. Diagnostics. 2019; 9(3):83. https://doi.org/10.3390/diagnostics9030083
Chicago/Turabian StylePujol, Pascal, Thibault De La Motte Rouge, and Frédérique Penault-Llorca. 2019. "From Targeting Somatic Mutations to Finding Inherited Cancer Predispositions: The Other Side of the Coin" Diagnostics 9, no. 3: 83. https://doi.org/10.3390/diagnostics9030083