Four Virtual-Reality Simulators for Diagnostic Abdominal Ultrasound Training in Radiology

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nayahangan, L.J.; Nielsen, K.R.; Albrecht-Beste, E.; Bachmann Nielsen, M.; Paltved, C.; Lindorff-Larsen, K.G.; Nielsen, B.U.; Konge, L. Determining procedures for simulation-based training in radiology: A nationwide needs assessment. Eur. Radiol. 2018, 28, 2319. [Google Scholar] [CrossRef] [PubMed]
- Konge, L.; Albrecht-Beste, E.; Nielsen, M.B. Virtual-reality simulation-based training in ultrasound. Ultraschall. Med. 2014, 35, 95–97. [Google Scholar] [CrossRef] [PubMed]
- Konge, L.; Clementsen, P.F.; Ringsted, C.; Minddal, V.; Larsen, K.R.; Annema, J.T. Simulator training for endobronchial ultrasound: a randomised controlled trial. Eur. Respir. J. 2015, 46, 2352. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, M.L.; Ewertsen, C.; Konge, L.; Albrecht-Beste, E.; Nielsen, M.B. Simulation-Based Abdominal Ultrasound Training—A Systematic Review. Ultraschall. Med. 2016, 37, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Konge, L.; Ringsted, C.; Bjerrum, F.; Tolsgaard, M.G.; Bitsch, M.; Sørensen, J.L.; Schroeder, T.V. The Simulation Centre at Rigshospitalet, Copenhagen, Denmark. J. Surg. Educ. 2015, 72, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.L.; Copel, J.A. Point-of-care ultrasonography. N. Engl. J. Med. 2011, 364, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Motola, I.; Devine, L.A.; Chung, H.S.; Sullivan, J.E.; Issenberg, S.B. Simulation in healthcare education: A best evidence practical guide. AMEE Guide No. 82. Med. Teach. 2013, 35, 1511–1530. [Google Scholar] [CrossRef] [PubMed]
- Le, C.-K.; Lewis, J.; Steinmetz, P.; Dyachenko, A.; Oleskevich, S. The Use of Ultrasound Simulators to Strengthen Scanning Skills in Medical Students: A Randomized Controlled Trial. J. Ultrasound. Med. 2018. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Dyre, L.; Tabor, A.; Ringsted, C.; Tolsgaard, M.G. Imperfect practice makes perfect: Error management training improves transfer of learning. Med. Educ. 2017, 51, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Taksøe-Vester, C.; Dreisler, E.; Andreasen, L.A.; Dyre, L.; Ringsted, C.; Tabor, A.; Tolsgaard, M.G. Up or down? A randomized trial comparing image orientations during transvaginal ultrasound training. Acta Obstet. Gynecol. Scand. 2018, 97, 1455–1462. [Google Scholar]
- Jensen, J.K.; Dyre, L.; Jørgensen, M.E.; Andreasen, L.A.; Tolsgaard, M.G. Collecting Validity Evidence for Simulation-Based Assessment of Point-of-Care Ultrasound Skills. J. Ultrasound. Med. Off. 2017, 36, 2475–2483. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, M.L.; Nielsen, K.R.; Albrecht-Beste, E.; Konge, L.; Nielsen, M.B. Development of a reliable simulation-based test for diagnostic abdominal ultrasound with a pass/fail standard usable for mastery learning. Eur. Radiol. 2018, 28, 51–57. [Google Scholar] [CrossRef] [PubMed]
- European Society of Radiology. The Minimum Training Recommendations for the Practice of Medical Ultrasound. Ultraschall. Med. 2006, 27, 79–105. [Google Scholar]
- Russel, L.; Østergaard, M.L.; Nielsen, M.B.; Konge, L.; Nielsen, K.R. Standardized assessment of competence in Focused Assessment with Sonography for Trauma. Acta Anaesthesiol. Scand. 2018. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, K.A. Acquisition and maintenance of medical expertice: A perspective from the expert-performance approach with delibrate practice. Acad. Med. J. 2015, 90, 1471–1486. [Google Scholar] [CrossRef] [PubMed]
- McGaghie, W.C. Mastery Learning: It Is Time for Medical Education to Join the 21st Century. Acad. Med. 2015, 90, 1438–1441. [Google Scholar] [CrossRef] [PubMed]
- Tolsgaard, M.G.; Ringsted, C.; Rosthøj, S.; Nørgaard, L.; Møller, L.; Freiesleben, N.L.C.; Dyre, L.; Tabor, A. The Effects of Simulation-based Transvaginal Ultrasound Training on Quality and Efficiency of Care: A Multicenter Single-blind Randomized Trial. Ann. Surg. 2017, 265, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, M.L.; Rue Nielsen, K.; Albrecht-Beste, E.; Kjær Ersbøll, A.; Konge, L.; Bachmann Nielsen, M. Simulator training improves ultrasound scanning performance on patients: A randomized controlled trial. Eur. Radiol. 2019. Epub ahead of print. [Google Scholar]


{kind=link}
| Demographics | Radiological Residents | Radiologists | All |
|---|---|---|---|
| Group size | 7 | 8 | 15 |
| Female | 3 | 2 | 5 |
| Male | 4 | 6 | 10 |
| Ultrasound experience in weeks (SD) | 13.9 (17.5) | 1093 (491.7) | - |
| Simulator | MedaPhor | Schallware | Simbionix (3D Systems) | CAE Healthcare |
|---|---|---|---|---|
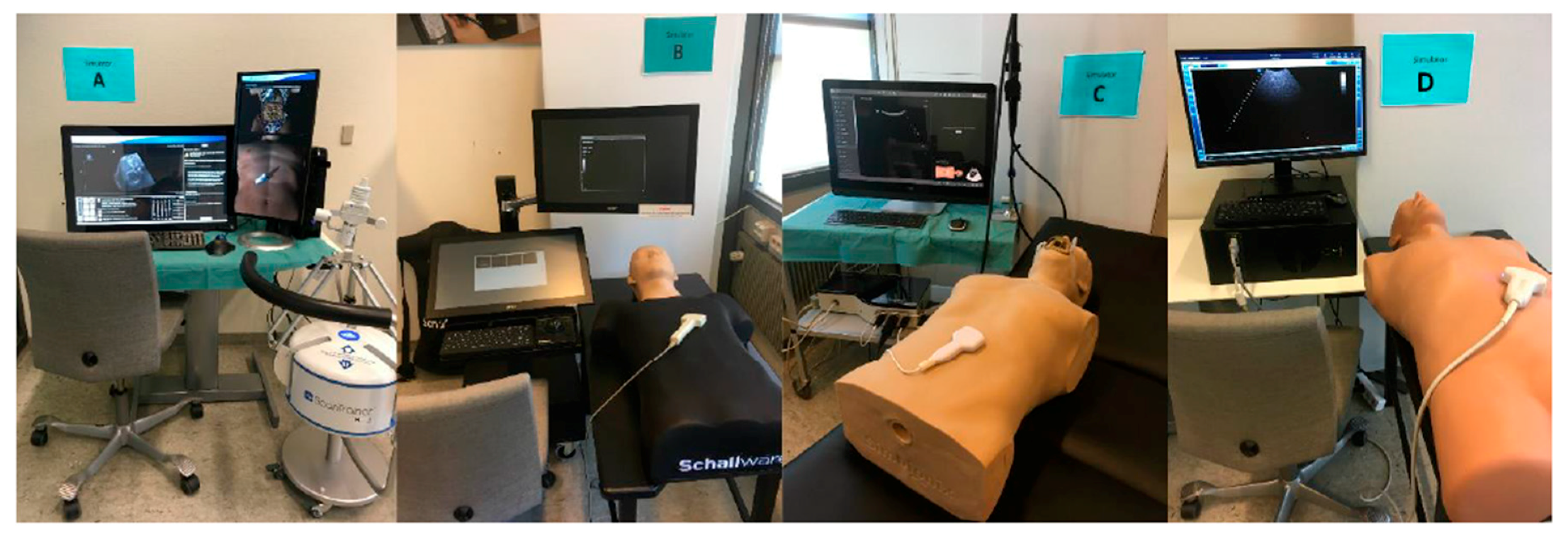
| Study mark | A | B | C | D |
| Version | ScanTrainer TVS & TAS, 2017x | Ultrasound Simulator Station-128 | U/S Mentor | CAE Vimedix |
| Primary based | Cardiff, UK Available worldwide | Berlin, Germany Available worldwide | Tel Aviv, Israel Available worldwide | Sarasota, Florida, US Available worldwide |
| Description | A hard drive, two screens, a floor-mounted haptic device, keyboard and mouse with rollerball. One screen displays image, buttons and help features, and the other screen displays the virtual patient and probe | A hard drive, two touch screens, keyboard with a rollerball, probes and a sensor table with a mannequin torso. One screen mimics ultrasound buttons and one shows the scan image | A hard drive, one touch screen with screen divisions, keyboard, probes and a sensor table with a mannequin torso. The split screen displays the scan image on one side, and buttons plus anatomical helping model on the other side | A hard drive, one split-screen, keyboard, mouse, probes and a sensor table with a mannequin torso. The screen displays the scan image, buttons and help features |
| Price | €20,000 to €90,000 | €20,000 to €65,000 | 50,0000 to 100,000 USD | Not disclosed |
| Abdominal cases | About 250 | About 250 | 8 diagnostic and 11 FAST | 10 cases |
| Custom cases | Yes, customers can upload their own scans from patients | Yes, with additional equipment | All cases can be customized for severity and/or presence of pathology | All cases can be customized for severity and/or presence of pathology |
| Source of scan | Real patient CT scans blended with computer data | Real patient ultrasound b-mode scans | Computer generated data | Computer generated data |
| Feedback options | ScanTutor will test user against set metrics. Metrics can be customized. Full diagnostic list for each case | Region of interest (RoI) with the option of turning RoIs into questions/answers. Full diagnostic list for each case | Case severity feature/multiple scenarios pr. case. Skill tasks. Full diagnostic list for each case | Performance assessments with kinematic metrics. Full diagnostic list for each case |
| Dynamic features | Computer animated doppler incl. CFM, PW & CW. Breathing patient | Doppler pre-recorded | Computer animated Doppler Breathing patient | Computer animated Doppler Breathing patient |
| Other modules available | OBGYN eFAST/FAST Emergency Medicine General Medicine Breast | Obstetrics/Gynecology Cardiology TEE Pediatric (new born manikin) Irritable Boule Disease Virtual model, adult Heart/lungs animated Virtual fetus model | Basic sonography skills Obstetrics/Gynecology Fetal Neurosonography + Echo Cardiology TEE/Echo eFAST/RUSH Emergency Medicine Lung | Obstetrics/Gynecology Cardiology TEE FAST/eFAST Emergency Medicine |
| Overall Ranking | MedaPhor | Schallware | Simbionix | ViMedix |
|---|---|---|---|---|
| Overall Educational value |  |  |  |  |
| Residents/Experienced |  |  |  |  |
| Resembles real scanning on image |  |  |  |  |
| Residents/Experienced.tif |  |  |  |  |
| Resembles real scanning on probe handling |  |  |  |  |
| Residents/Experienced |  |  |  |  |
| Resembles real scanning knobology |  |  |  |  |
| Residents/Experienced |  |  |  |  |
| intuitive Use |  |  |  |  |
| Residents/Experienced.tif |  |  |  |  |
| Case description. |  |  |  |  |
| Residents/Experienced |  |  |  |  |
| Usable hints |  |  |  |  |
| Residents/Experienced |  |  |  |  |
| Useful Feedback |  |  |  |  |
| Residents/Experienced |  |  |  |  |
| Overall feel |  |  |  |  |
| Residents/Experienced |  |  |  |  |
| Comparing Mean Score by Groups | Radiological Residents | Radiologists | P Value |
|---|---|---|---|
| Simulator A | |||
| Educational Value (SD) | 3.1 (1.2) | 2.9 (1.2) | >0.05 |
| Fidelity (SD) | 2.9 (0.9) | 3.3 (1.3) | >0.05 |
| Usability (SD) | 3.1 (0.9) | 3.5 (1.3) | >0.05 |
| Overall Satisfaction (SD) | 2.9 (1.4) | 2.9 (1.6) | >0.05 |
| Simulator B | |||
| Educational Value (SD) | 4.0 (0.6) | 3.8 (0.8) | >0.05 |
| Fidelity (SD) | 3.8 (0.8) | 4.1 (0.5) | >0.05 |
| Usability (SD) | 4.1 (0.8) | 3.9 (0.9) | >0.05 |
| Overall Satisfaction (SD) | 3.8 (1.0) | 3.9 (0.7) | >0.05 |
| Simulator C | |||
| Educational Value (SD) | 3.4 (1.3) | 1.3 (1.0) | >0.05 |
| Fidelity (SD) | 3.2 (0.8) | 3.2 (0.9) | >0.05 |
| Usability (SD) | 3.8 (0.7) | 4.0 (0.7) | >0.05 |
| Overall Satisfaction (SD) | 3.8 (1.0) | 3.3 (0.9) | >0.05 |
| Simulator D | |||
| Educational Value (SD) | 3.2 (1.1) | 2.9 (1.0) | >0.05 |
| Fidelity (SD) | 2.6 (0.7) | 3.0 (1.1) | >0.05 |
| Usability (SD) | 3.5 (0.5) | 3.2 (1.5) | >0.05 |
| Overall Satisfaction (SD) | 3.2 (1.3) | 3.0 (1.2) | >0.05 |
| Comparing Means Collective Score, Individual Questionnaires | Simulator A MedaPhor | Simulator B Schallware | Simulator C Simbionix | Simulator D ViMedix |
|---|---|---|---|---|
| Educational Value | ||||
| Benefits for novices | 3.8 (1.2) | 4.7 (0.5) | 4.4 (0.7) | 4.2 (0.9) |
| Benefits for intermediates | 3.1 (1.5) | 4.3 (1.0) | 3.3 (1.6) | 2.9 (1.5) |
| Benefits for advanced | 2.1 (1.1) | 2.7 (1.2) | 2.2 (1.3) | 2.0 (1.1) |
| Fidelity | ||||
| Scans resemble real life images | 3.5 (1.2) | 4.8 (0.4) | 2.5 (1.2) | 2.5 (1.2) |
| Probe resemble real life use | 2.5 (1.5) | 3.7 (1.1) | 4.0 (1.2) | 3.9 (1.0) |
| Knobs resemble real life use | 3.1 (1.6) | 3.5 (1.3) | 3.2 (1.4) | 2.1 (1.2) |
| Usability | ||||
| Intuitive use | 3.7 (1.3) | 4.4 (0.9) | 4.5 (0.6) | 4.2 (1.3) |
| Useful instructions | 3.1 (1.2) | 3.9 (1.1) | 3.9 (0.9) | 3.1 (1.4) |
| Useful feedback | 3.1 (1.1) | 3.7 (1.0) | 3.3 (1.1) | 2.7 (1.2) |
| Overall Satisfaction | ||||
| Easy to use | 3.3 (1.5) | 4.3 (0.9) | 4.5 (0.6) | 4.1 (1.5) |
| Overall feel | 2.9 (1.6) | 3.7 (1.0) | 3.7 (1.2) | 3.0 (1.5) |
| Recommend it to department | 2.4 (1.4) | 3.6 (1.1) | 2.6 (1.5) | 2.3 (1.3) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Østergaard, M.L.; Konge, L.; Kahr, N.; Albrecht-Beste, E.; Nielsen, M.B.; Nielsen, K.R. Four Virtual-Reality Simulators for Diagnostic Abdominal Ultrasound Training in Radiology. Diagnostics 2019, 9, 50. https://doi.org/10.3390/diagnostics9020050
Østergaard ML, Konge L, Kahr N, Albrecht-Beste E, Nielsen MB, Nielsen KR. Four Virtual-Reality Simulators for Diagnostic Abdominal Ultrasound Training in Radiology. Diagnostics. 2019; 9(2):50. https://doi.org/10.3390/diagnostics9020050
Chicago/Turabian StyleØstergaard, Mia Louise, Lars Konge, Niklas Kahr, Elisabeth Albrecht-Beste, Michael Bachmann Nielsen, and Kristina Rue Nielsen. 2019. "Four Virtual-Reality Simulators for Diagnostic Abdominal Ultrasound Training in Radiology" Diagnostics 9, no. 2: 50. https://doi.org/10.3390/diagnostics9020050