Active Matrix Metalloproteinase-8 Point-of-Care (PoC)/Chairside Mouthrinse Test vs. Bleeding on Probing in Diagnosing Subclinical Periodontitis in Adolescents

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
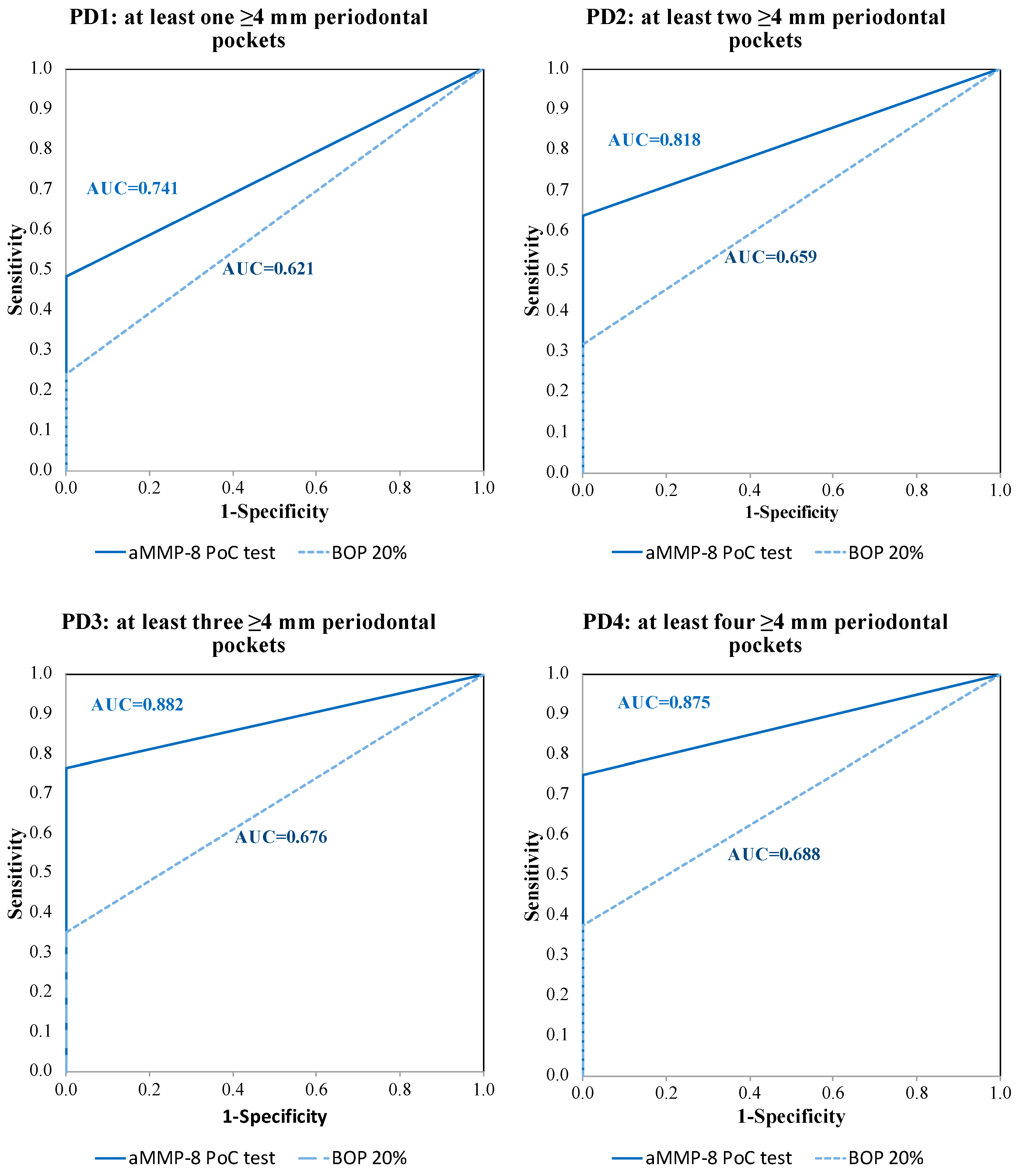
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sorsa, T.; Gürsoy, U.K.; Nwhator, S.; Hernandez, M.; Tervahartiala, T.; Leppilahti, J.; Gürsoy, M.; Könönen, E.; Emingil, G.; Pussinen, P.J.; et al. Analysis of Matrix Metalloproteinases, Especially MMP-8, in Gingival Crevicular Fluid, Mouthrinse and Saliva for Monitoring Periodontal Diseases. Periodontol. 2000 2016, 70, 142–163. [Google Scholar] [CrossRef]
- Heikkinen, A.M.; Räisänen, I.T.; Tervahartiala, T.; Sorsa, T. Cross-Sectional Analysis of Risk Factors for Subclinical Periodontitis; Active Matrix Metalloproteinase-8 as a Potential Indicator in Initial Periodontitis in Adolescents. J. Periodontol. 2018, in press. [Google Scholar] [CrossRef] [PubMed]
- Leppilahti, J.M.; Hernández-Rios, P.A.; Gamonal, J.A.; Tervahartiala, T.; Brignardello-Petersen, R.; Mäntylä, P.; Sorsa, T.; Hernández, M. Matrix Metalloproteinases and Myeloperoxidase in Gingival Crevicular Fluid Provide Site-Specific Diagnostic Value for Chronic Periodontitis. J. Clin. Periodontol. 2014, 41, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Leppilahti, J.M.; Kallio, M.A.; Tervahartiala, T.; Sorsa, T.; Mäntylä, P. Gingival Crevicular Fluid Matrix Metalloproteinase-8 Levels Predict Treatment Outcome among Smokers with Chronic Periodontitis. J. Periodontol. 2014, 85, 250–260. [Google Scholar] [CrossRef]
- Leppilahti, J.M.; Sorsa, T.; Kallio, M.A.; Tervahartiala, T.; Emingil, G.; Han, B.; Mäntylä, P. The Utility of Gingival Crevicular Fluid Matrix Metalloproteinase-8 Response Patterns in Prediction of Site-Level Clinical Treatment Outcome. J. Periodontol. 2015, 86, 777–787. [Google Scholar] [CrossRef]
- Lee, W.; Aitken, S.; Sodek, J.; McCulloch, C.A. Evidence of a Direct Relationship between Neutrophil Collagenase Activity and Periodontal Tissue Destruction In Vivo: Role of active enzyme in human periodontitis. J. Periodontal. Res. 1995, 30, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Romanelli, R.; Mancini, S.; Laschinger, C.; Overall, C.M.; Sodek, J.; McCulloch, C.A. Activation of Neutrophil Collagenase in Periodontitis. Infect. Immun. 1999, 67, 2319–2326. [Google Scholar]
- Mancini, S.; Romanelli, R.; Laschinger, C.A.; Overall, C.M.; Sodek, J.; McCulloch, C.A. Assessment of a Novel Screening Test for Neutrophil Collagenase Activity in the Diagnosis of Periodontal Diseases. J. Periodontol. 1999, 70, 1292–1302. [Google Scholar] [CrossRef]
- Sorsa, T.; Hernández, M.; Leppilahti, J.; Munjal, S.; Netuschil, L.; Mäntylä, P. Detection of Gingival Crevicular Fluid MMP-8 Levels with Different Laboratory and Chair-Side Methods. Oral Dis. 2010, 16, 39–45. [Google Scholar] [CrossRef]
- Sorsa, T.; Mäntylä, P.; Tervahartiala, T.; Pussinen, P.J.; Gamonal, J.; Hernandez, M. MMP Activation in Diagnostics of Periodontitis and Systemic Inflammation. J. Clin. Periodontol. 2011, 38, 817–819. [Google Scholar] [CrossRef] [PubMed]
- Hernández, M.; Gamonal, J.; Tervahartiala, T.; Mäntylä, P.; Rivera, O.; Dezerega, A.; Dutzan, N.; Sorsa, T. Associations between Matrix Metalloproteinase-8 and -14 and Myeloperoxidase in Gingival Crevicular Fluid from Subjects with Progressive Chronic Periodontitis: A Longitudinal Study. J. Periodontol. 2010, 81, 1644–1652. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Heikkinen, A.M.; Leppilahti, J.; Tervahartiala, T.; Solomon Nwhator, S.; Rathnayake, N.; Mäntylä, P.; Gieselmann, D.-R.; Netuschil, L. Active Matrix Metalloproteinase-8, Contributor to Periodontitis and a Missing Link between Dentistry and Medicine. In Pathogenesis of Periodontal Diseases—Biological Concepts for Clinicians; Bostanci, N., Belibasakis, G., Eds.; Springer: Heidelberg, Germany, 2018; pp. 51–57. [Google Scholar]
- Sorsa, T.; Gieselmann, D.; Arweiler, N.B.; Hernández, M. A Quantitative Point-of-Care Test for Periodontal and Dental Peri-Implant Diseases. Nat. Rev. Dis. Prim. 2017, 3, 17069. [Google Scholar] [CrossRef]
- Nwhator, S.O.; Ayanbadejo, P.O.; Umeizudike, K.A.; Opeodu, O.I.; Agbelusi, G.A.; Olamijulo, J.A.; Arowojolu, M.O.; Sorsa, T.; Babajide, B.S.; Opedun, D.O. Clinical Correlates of a Lateral-Flow Immunoassay Oral Risk Indicator. J. Periodontol. 2014, 85, 188–194. [Google Scholar] [CrossRef]
- Heikkinen, A.M.; Nwhator, S.O.; Rathnayake, N.; Mäntylä, P.; Vatanen, P.; Sorsa, T. Pilot Study on Oral Health Status as Assessed by an Active Matrix Metalloproteinase-8 Chairside Mouthrinse Test in Adolescents. J. Periodontol. 2016, 87, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Heikkinen, A.M.; Raivisto, T.; Kettunen, K.; Kovanen, L.; Haukka, J.; Pakbaznejad Esmaeili, E.; Elg, J.; Gieselmann, D.-R.; Rathnayake, N.; Ruokonen, H.; et al. Pilot Study on the Genetic Background of an Active Matrix Metalloproteinase-8 Test in Finnish Adolescents. J. Periodontol. 2017, 88, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, K.; Keller, T.; Noack, B.; Freitag, A.; Netuschil, L.; Hoffmann, T. Evaluation of a Novel Point-of-Care Test for Active Matrix Metalloproteinase-8: Agreement between Qualitative and Quantitative Measurements and Relation to Periodontal Inflammation. J. Periodontal. Res. 2017, 52, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.; Ebersole, J.L.; Kryscio, R.J.; Danaher, R.J.; Dawson, D., 3rd; Al-Sabbagh, M.; Miller, C.S. Rapid Assessment of Salivary MMP-8 and Periodontal Disease Using Lateral Flow Immunoassay. Oral Dis. 2016, 22, 681–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izadi Borujeni, S.; Mayer, M.; Eickholz, P. Activated Matrix Metalloproteinase-8 in Saliva as Diagnostic Test for Periodontal Disease? A Case-Control Study. Med. Microbiol. Immunol. 2015, 204, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Rios, P.; Hernández, M.; Garrido, M.; Tervahartiala, T.; Leppilahti, J.; Kuula, H.; Heikkinen, A.M.; Mäntylä, P.; Rathnayake, N.; Nwhator, S.; et al. Oral Fluid Matrix Metalloproteinase (MMP)-8 as a Diagnostic Tool in Chronic Periodontitis. Metalloproteinases Med. 2016, 3, 11–18. [Google Scholar] [CrossRef]
- Leppilahti, J.M.; Harjunmaa, U.; Järnstedt, J.; Mangani, C.; Hernández, M.; Tervahartiala, T.; Lopez, R.; Ashorn, U.; Ashorn, P.; Gieselmann, D.-R.; et al. Diagnosis of Newly Delivered Mothers for Periodontitis with a Novel Oral-Rinse aMMP-8 Point-of-Care Test in a Rural Malawian Population. Diagnostics 2018, 8, 67. [Google Scholar] [CrossRef]
- Räisänen, I.T.; Heikkinen, A.M.; Siren, E.; Tervahartiala, T.; Gieselmann, D.-R.; Van der Schoor, G.-J.; Van der Schoor, P.; Sorsa, T. Point-of-Care/Chairside aMMP-8 Analytics of Periodontal Diseases’ Activity and Episodic Progression. Diagnostics 2018, 8, 74. [Google Scholar] [CrossRef]
- Alassiri, S.; Parnanen, P.; Rathnayake, N.; Johannsen, G.; Heikkinen, A.M.; Lazzara, R.; van der Schoor, P.; van der Schoor, J.G.; Tervahartiala, T.; Gieselmann, D.; et al. The Ability of Quantitative, Specific, and Sensitive Point-of-Care/Chair-Side Oral Fluid Immunotests for aMMP-8 to Detect Periodontal and Peri-Implant Diseases. Dis. Markers 2018, 1306396. [Google Scholar] [CrossRef]
- Lang, N.P.; Joss, A.; Orsanic, T.; Gusberti, F.A.; Siegrist, B.E. Bleeding on Probing. A Predictor for the Progression of Periodontal Disease? J. Clin. Periodontol. 1986, 13, 590–596. [Google Scholar] [CrossRef]
- Daly, C.G.; Mitchell, D.H.; Highfield, J.E.; Grossberg, D.E.; Stewart, D. Bacteremia Due to Periodontal Probing: A Clinical and Microbiological Investigation. J. Periodontol. 2001, 72, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Riggio, M.P.; Walker, K.F.; MacKenzie, D.; Shearer, B. Bacteraemia Following Periodontal Procedures. J. Periodontol. 2005, 32, 708–713. [Google Scholar] [CrossRef]
- Davies, J.; Davies, D. Origins and Evolution of Antibiotic Resistance. Microbiol. Mol. Biol. Rev. 2010, 74, 417–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association Declaration of Helsinki: Recommendations Guiding Medical Doctors in Biomedical Research Involving Human Subjects. Adopted by the 18th World Medical Assembly, Helsinki, Finland, 1964 and as Revised by the World Medical Assembly in Tokyo, Japan, 1975, in Venice, Italy, 1983, in Hong Kong, 1989, in Somerset West, Republic of South Africa, 1996, in Edinburgh, Scotland, 2000, in Washington, United States, 2002, in Tokyo, Japan, 2004, in Seoul, Korea, 2008. Available online: https://www.wma.net/wp-content/uploads/2018/07/DoH-Oct2008.pdf (accessed on 22 March 2019).
- Heikkinen, A.M.; Pakbaznejad Esmaeili, E.; Kovanen, L.; Ruokonen, H.; Kettunen, K.; Haukka, J.; Tervahartiala, T.; Sorsa, T. Periodontal Initial Radiological Findings of Genetically Predisposed Finnish Adolescents. J. Clin. Diagn. Res. 2017, 11, ZC25–ZC28. [Google Scholar] [CrossRef] [PubMed]
- Heikkinen, A.M.; Pajukanta, R.; Pitkäniemi, J.; Broms, U.; Sorsa, T.; Koskenvuo, M.; Meurman, J.H. The Effect of Smoking on Periodontal Health of 15- to 16-Year-Old Adolescents. J. Periodontol. 2008, 79, 2042–2047. [Google Scholar] [CrossRef]
- Heikkinen, A.M. Oral Health, Smoking and Adolescence. [Dissertation]. University of Helsinki, Finland, Faculty of Medicine, Institute of Dentistry, 2011. Available online: http://urn.fi/URN:ISBN:978-952-10-7250-5 (accessed on 22 March 2019).
- Anscombe, F.J. On Estimating Binomial Response Relations. Biometrika 1956, 43, 461–464. [Google Scholar] [CrossRef]
- Haldane, J. The Estimation and Significance of the Logarithm of a Ratio of Frequencies. Ann. Hum. Genet. 1956, 20, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S162–S170. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.; Guder, U.; Kreuz, M.; Löffler, M.; Kiess, W.; Hirsch, C.; Ziebolz, D.; Haak, R. aMMP-8 in Correlation to Caries and Periodontal Condition in Adolescents—Results of the Epidemiologic LIFE Child Study. Clin. Oral Investig. 2018, 22, 449–460. [Google Scholar] [CrossRef] [PubMed]
- Apajalahti, S.; Sorsa, T.; Railavo, S.; Ingman, T. The In Vivo Levels of Matrix Metalloproteinase-1 and -8 in Gingival Crevicular Fluid During Initial Orthodontic Tooth Movement. J. Dent. Res. 2003, 82, 1018–1022. [Google Scholar] [CrossRef] [PubMed]
- Ingman, T.; Apajalahti, S.; Mäntylä, P.; Savolainen, P.; Sorsa, T. Matrix Metalloproteinase-1 and -8 in Gingival Crevicular Fluid During Orthodontic Tooth Movement: A Pilot Study During 1 Month of Follow-Up After Fixed Appliance Activation. Eur. J. Orthod. 2005, 27, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Hanemaaijer, R.; Sorsa, T.; Konttinen, Y.T.; Ding, Y.; Sutinen, M.; Visser, H.; van Hinsbergh, V.W.; Helaakoski, T.; Kainulainen, T.; Rönkä, H.; et al. Matrix Metalloproteinase-8 Is Expressed in Rheumatoid Synovial Fibroblasts and Endothelial Cells. Regulation by Tumor Necrosis Factor-Alpha and Doxycycline. J. Biol. Chem. 1997, 272, 31504–31509. [Google Scholar] [CrossRef] [PubMed]
- Gürsoy, U.K.; Könönen, E.; Tervahartiala, T.; Gürsoy, M.; Pitkänen, J.; Torvi, P.; Suominen, A.L.; Pussinen, P.; Sorsa, T. Molecular Forms and Fragments of Salivary MMP-8 in Relation to Periodontitis. J. Clin. Periodontol. 2018, 45, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Uitto, V.J.; Suomalainen, K.; Sorsa, T. Salivary Collagenase. Origin, Characteristics and Relationship to Periodontal Health. J. Periodontal. Res. 1990, 25, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Gangbar, S.; Overall, C.M.; McCulloch, C.A.; Sodek, J. Identification of Polymorphonuclear Leukocyte Collagenase and Gelatinase Activities in Mouthrinse Samples: Correlation with Periodontal Disease Activity in Adult and Juvenile Periodontitis. J. Periodontal. Res. 1990, 25, 257–267. [Google Scholar] [CrossRef]
- Nieminen, M.T.; Vesterinen, P.; Tervahartiala, T.; Kormi, I.; Sinisalo, J.; Pussinen, P.J.; Sorsa, T. Practical Implications of Novel Serum ELISA-Assay for Matrix Metalloproteinase-8 in Acute Cardiac Diagnostics. Acute Card. Care 2015, 17, 46–47. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.; Choi, Y. Point-of-Care Diagnosis of Periodontitis Using Saliva: Technically Feasible but Still a Challenge. Front. Cell. Infect. Microbiol. 2015, 5, 65. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, N.; Nayak, P.A.; Rana, S. Point of Care—A Novel Approach to Periodontal Diagnosis—A Review. J. Clin. Diagn. Res. 2017, 11, ZE01–ZE06. [Google Scholar] [CrossRef] [PubMed]
- He, W.; You, M.; Wan, W.; Xu, F.; Li, F.; Li, A. Point-of-Care Periodontitis Testing: Biomarkers, Current Technologies, and Perspectives. Trends Biotechnol. 2018, 36, 1127–1144. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Periodontal Status | Measures of the Effectiveness of a Diagnostic Test | |||||||
|---|---|---|---|---|---|---|---|---|
| Test | PD1 | Healthy | OR | Se | Sp | Acc | FN | FP |
| aMMP-8 PoC+ | 14 | 0 | 34.6 | 48.3% | 100.0% | 68.1% | 45.5% | 0.0% |
| aMMP-8 PoC− | 15 | 18 | ||||||
| BOP+ | 7 | 0 | 12.3 | 24.1% | 100.0% | 53.2% | 55.0% | 0.0% |
| BOP− | 22 | 18 | ||||||
| Test | PD2 | Healthy | OR | Se | Sp | Acc | FN | FP |
| aMMP-8 PoC+ | 14 | 0 | 63.1 | 63.6% | 100.0% | 80.0% | 30.8% | 0.0% |
| aMMP-8 PoC− | 8 | 18 | ||||||
| BOP+ | 7 | 0 | 17.9 | 31.8% | 100.0% | 62.5% | 45.5% | 0.0% |
| BOP− | 15 | 18 | ||||||
| Test | PD3 | Healthy | OR | Se | Sp | Acc | FN | FP |
| aMMP-8 PoC+ | 13 | 0 | 111.0 | 76.5% | 100.0% | 88.6% | 18.2% | 0.0% |
| aMMP-8 PoC− | 4 | 18 | ||||||
| BOP+ | 6 | 0 | 20.9 | 35.3% | 100.0% | 68.6% | 37.9% | 0.0% |
| BOP− | 11 | 18 | ||||||
| Test | PD4 | Healthy | OR | Se | Sp | Acc | FN | FP |
| aMMP-8 PoC+ | 12 | 0 | 102.8 | 75.0% | 100.0% | 88.2% | 18.2% | 0.0% |
| aMMP-8 PoC− | 4 | 18 | ||||||
| BOP+ | 6 | 0 | 22.9 | 37.5% | 100.0% | 70.6% | 35.7% | 0.0% |
| BOP− | 10 | 18 | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Räisänen, I.T.; Sorsa, T.; van der Schoor, G.-J.; Tervahartiala, T.; van der Schoor, P.; Gieselmann, D.-R.; Heikkinen, A.M. Active Matrix Metalloproteinase-8 Point-of-Care (PoC)/Chairside Mouthrinse Test vs. Bleeding on Probing in Diagnosing Subclinical Periodontitis in Adolescents. Diagnostics 2019, 9, 34. https://doi.org/10.3390/diagnostics9010034
Räisänen IT, Sorsa T, van der Schoor G-J, Tervahartiala T, van der Schoor P, Gieselmann D-R, Heikkinen AM. Active Matrix Metalloproteinase-8 Point-of-Care (PoC)/Chairside Mouthrinse Test vs. Bleeding on Probing in Diagnosing Subclinical Periodontitis in Adolescents. Diagnostics. 2019; 9(1):34. https://doi.org/10.3390/diagnostics9010034
Chicago/Turabian StyleRäisänen, Ismo T., Timo Sorsa, Gerrit-Jan van der Schoor, Taina Tervahartiala, Peter van der Schoor, Dirk-Rolf Gieselmann, and Anna Maria Heikkinen. 2019. "Active Matrix Metalloproteinase-8 Point-of-Care (PoC)/Chairside Mouthrinse Test vs. Bleeding on Probing in Diagnosing Subclinical Periodontitis in Adolescents" Diagnostics 9, no. 1: 34. https://doi.org/10.3390/diagnostics9010034