Cost-Efficient and Easy to Perform PCR-Based Assay to Identify Met Exon 14 Skipping in Formalin-Fixed Paraffin-Embedded (FFPE) Non-Small Cell Lung Cancer (NSCLC) Samples

 , , , and
, , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Ethics
2.3. Polymerase Chain Reaction (PCR)
2.4. Next-Generation Sequencing (NGS)
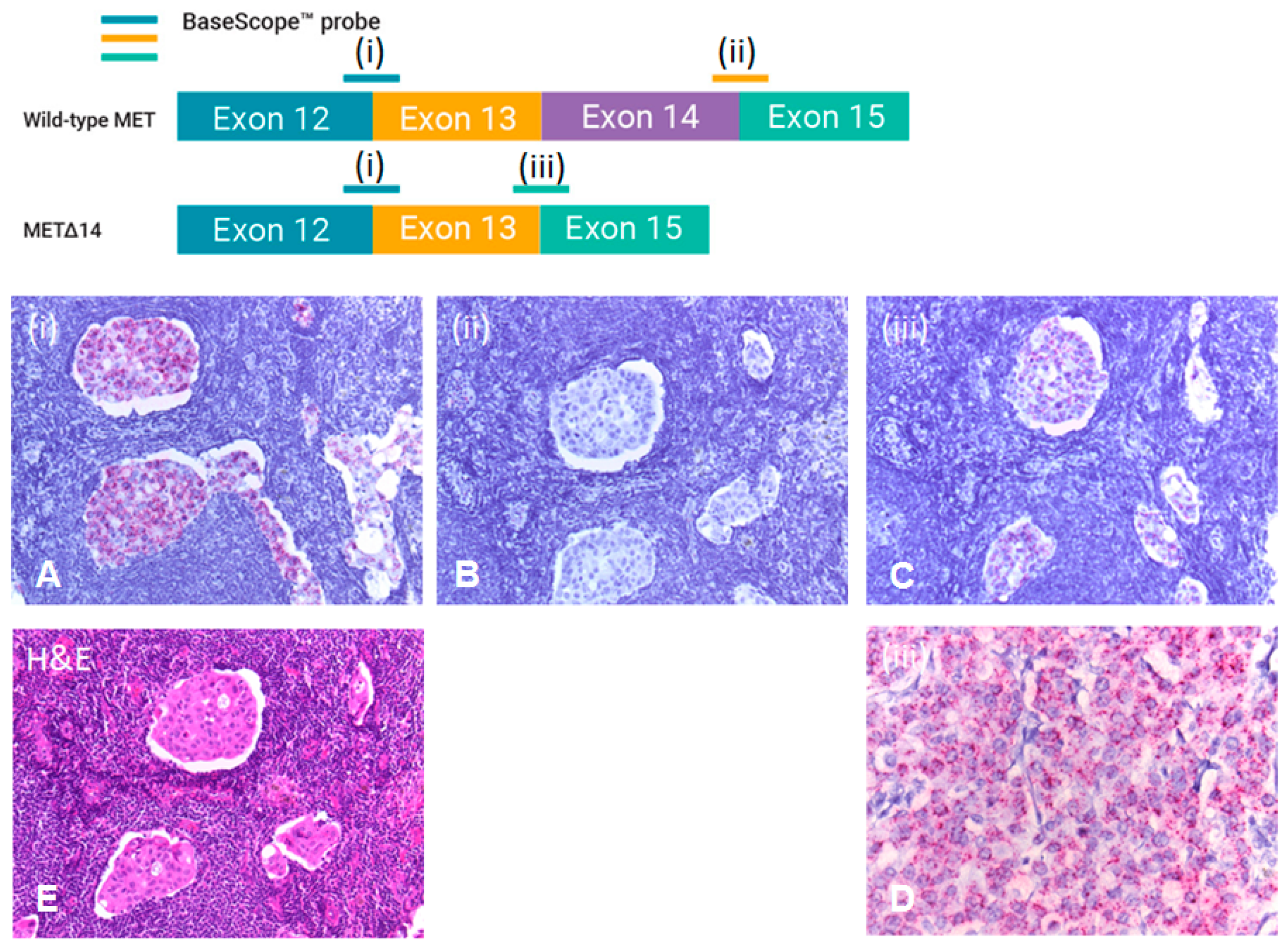
2.5. RNA In Situ Hybridisation (RISH)
3. Results
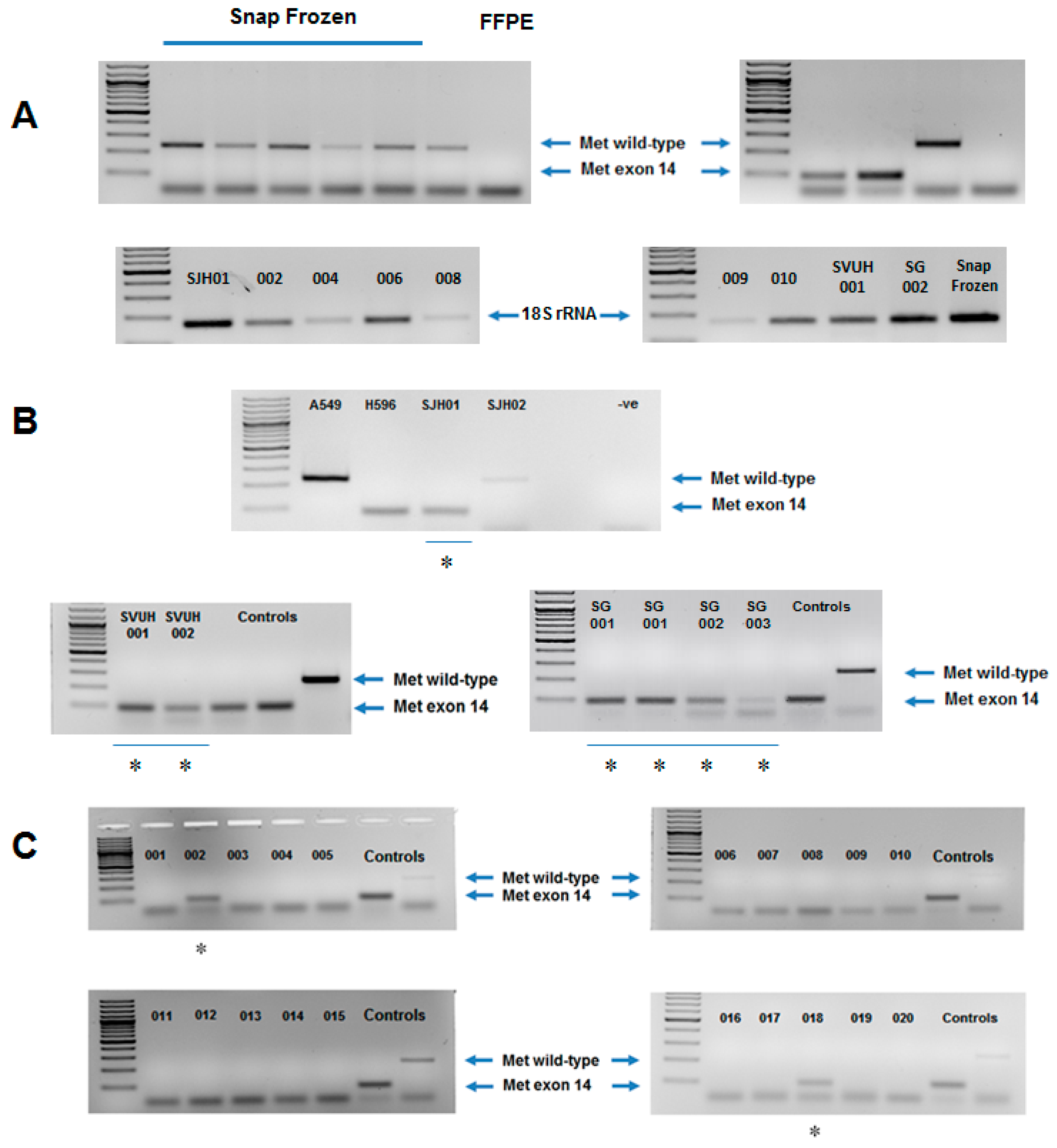
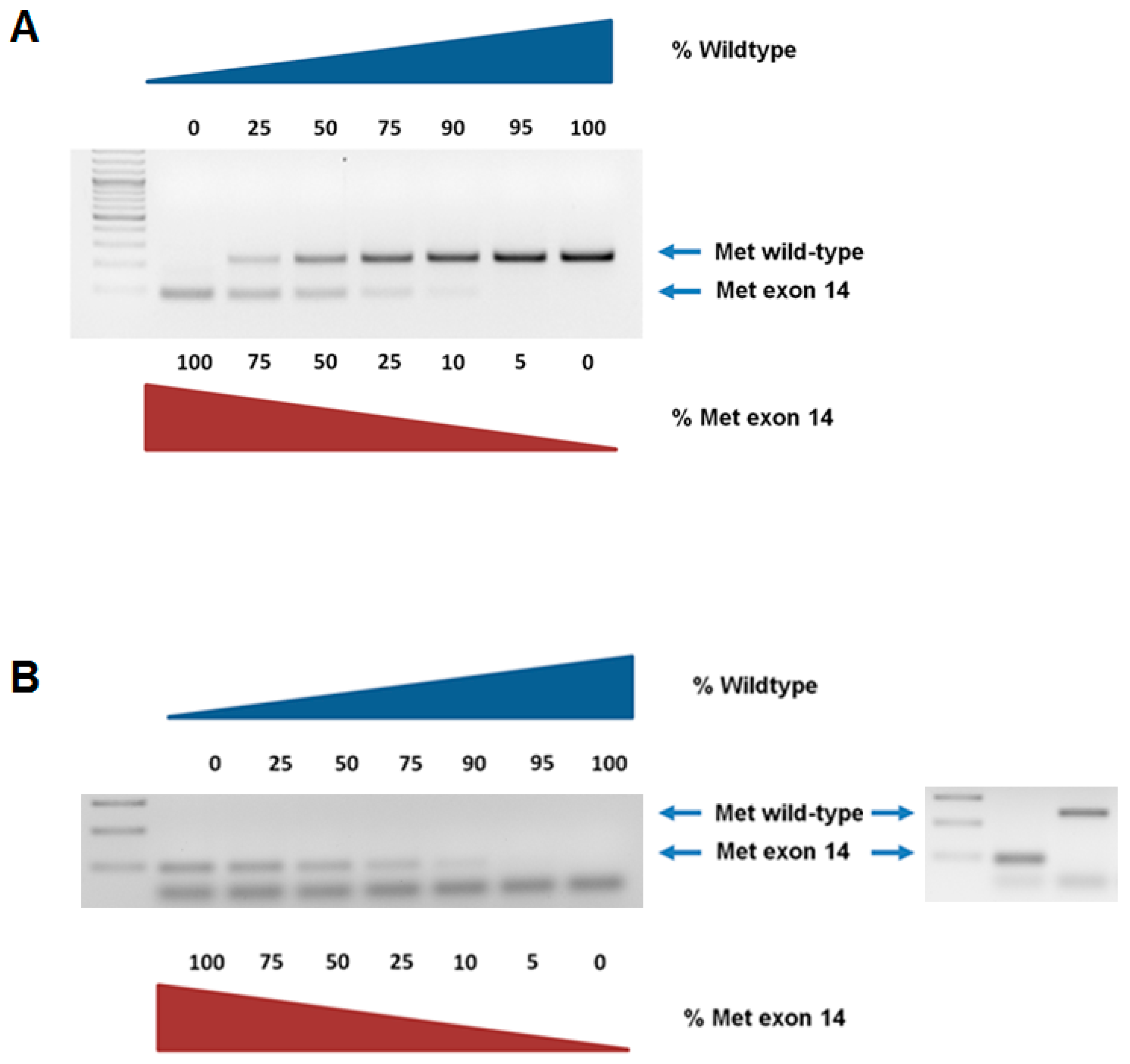
3.1. Reverse Transcription Polymerase Chain Reaction (RT-PCR)
3.2. Next-Generation Sequencing (NGS)
3.3. RNA In Situ Hybridisation (RISH)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Da Cunha Santos, G.; Shepherd, F.A.; Tsao, M.S. EGFR mutations and lung cancer. Annu. Rev. Pathol. 2011, 6, 49–69. [Google Scholar] [CrossRef] [PubMed]
- Organ, S.L.; Tsao, M.S. An overview of the c-MET signaling pathway. Ther. Adv. Med. Oncol. 2011, 3, S7–S19. [Google Scholar] [CrossRef] [PubMed]
- Frampton, G.M.; Ali, S.M.; Rosenzweig, M.; Chmielecki, J.; Lu, X.; Bauer, T.M.; Akimov, M.; Bufill, J.A.; Lee, C.; Jentz, D.; et al. Activation of MET via diverse exon 14 splicing alterations occurs in multiple tumor types and confers clinical sensitivity to MET inhibitors. Cancer Discov. 2015, 5, 850–859. [Google Scholar] [CrossRef] [PubMed]
- Reungwetwattana, T.; Liang, Y.; Zhu, V.; Ou, S.I. The race to target MET exon 14 skipping alterations in non-small cell lung cancer: The Why, the How, the Who, the Unknown, and the Inevitable. Lung Cancer 2017, 103, 27–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bubendorf, L.; Dafni, U.; Schobel, M.; Finn, S.P.; Tischler, V.; Sejda, A.; Marchetti, A.; Thunnissen, E.; Verbeken, E.K.; Warth, A.; et al. Prevalence and clinical association of MET gene overexpression and amplification in patients with NSCLC: Results from the European Thoracic Oncology Platform (ETOP) Lungscape project. Lung Cancer 2017, 111, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Ricciuti, B.; Marcomigni, L.; Metro, G.; Bellezza, G.; Caselli, E.; Baglivo, S.; Chiari, R. Identification of EML4-ALK Rearrangement and MET Exon 14 R988C Mutation in a Patient with High-Grade Neuroendocrine Lung Carcinoma Who Experienced a Lazarus Response to Crizotinib. J. Thorac. Oncol. 2018, 13, e220–e222. [Google Scholar] [CrossRef] [PubMed]
- Kauffmann-Guerrero, D.; Kahnert, K.; Kumbrink, J.; Syunyaeva, Z.; Tufman, A.; Huber, R.M. Successful Treatment of a Patient With NSCLC Harboring an EGFR Mutation and a Concomitant Met Exon 14 Skipping Mutation Combining Afatinib and Crizotinib. Clin. Lung Cancer 2019, 20, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Kwon, D.; Koh, J.; Kim, S.; Go, H.; Kim, Y.A.; Keam, B.; Kim, T.M.; Kim, D.W.; Jeon, Y.K.; Chung, D.H. MET exon 14 skipping mutation in triple-negative pulmonary adenocarcinomas and pleomorphic carcinomas: An analysis of intratumoral MET status heterogeneity and clinicopathological characteristics. Lung Cancer 2017, 106, 131–137. [Google Scholar] [CrossRef]
- Kim, E.K.; Kim, K.A.; Lee, C.Y.; Kim, S.; Chang, S.; Cho, B.C.; Shim, H.S. Molecular Diagnostic Assays and Clinicopathologic Implications of MET Exon 14 Skipping Mutation in Non-small-cell Lung Cancer. Clin. Lung Cancer 2018, 20, e123–e132. [Google Scholar] [CrossRef]
- Pilotto, S.; Gkountakos, A.; Carbognin, L.; Scarpa, A.; Tortora, G.; Bria, E. MET exon 14 juxtamembrane splicing mutations: Clinical and therapeutical perspectives for cancer therapy. Ann. Transl. Med. 2017, 5, 2. [Google Scholar] [CrossRef]
- Mignard, X.; Ruppert, A.M.; Antoine, M.; Vasseur, J.; Girard, N.; Mazieres, J.; Moro-Sibilot, D.; Fallet, V.; Rabbe, N.; Thivolet-Bejui, F.; et al. c-MET Overexpression as a Poor Predictor of MET Amplifications or Exon 14 Mutations in Lung Sarcomatoid Carcinomas. J. Thorac. Oncol. 2018, 13, 1962–1967. [Google Scholar] [CrossRef] [PubMed]
- Vuong, H.G.; Ho, A.T.N.; Altibi, A.M.A.; Nakazawa, T.; Katoh, R.; Kondo, T. Clinicopathological implications of MET exon 14 mutations in non-small cell lung cancer—A systematic review and meta-analysis. Lung Cancer 2018, 123, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Saigi, M.; McLeer-Florin, A.; Pros, E.; Nadal, E.; Brambilla, E.; Sanchez-Cespedes, M. Genetic screening and molecular characterization of MET alterations in non-small cell lung cancer. Clin. Transl. Oncol. 2018, 20, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Saffroy, R.; Fallet, V.; Girard, N.; Mazieres, J.; Sibilot, D.M.; Lantuejoul, S.; Rouquette, I.; Thivolet-Bejui, F.; Vieira, T.; Antoine, M.; et al. MET exon 14 mutations as targets in routine molecular analysis of primary sarcomatoid carcinoma of the lung. Oncotarget 2017, 8, 42428–42437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrock, A.B.; Li, S.D.; Frampton, G.M.; Suh, J.; Braun, E.; Mehra, R.; Buck, S.C.; Bufill, J.A.; Peled, N.; Karim, N.A.; et al. Pulmonary Sarcomatoid Carcinomas Commonly Harbor Either Potentially Targetable Genomic Alterations or High Tumor Mutational Burden as Observed by Comprehensive Genomic Profiling. J. Thorac. Oncol. 2017, 12, 932–942. [Google Scholar] [CrossRef]
- Schrock, A.B.; Frampton, G.M.; Suh, J.; Chalmers, Z.R.; Rosenzweig, M.; Erlich, R.L.; Halmos, B.; Goldman, J.; Forde, P.; Leuenberger, K.; et al. Characterization of 298 Patients with Lung Cancer Harboring MET Exon 14 Skipping Alterations. J. Thorac. Oncol. 2016, 11, 1493–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awad, M.M.; Oxnard, G.R.; Jackman, D.M.; Savukoski, D.O.; Hall, D.; Shivdasani, P.; Heng, J.C.; Dahlberg, S.E.; Janne, P.A.; Verma, S.; et al. MET Exon 14 Mutations in Non-Small-Cell Lung Cancer Are Associated with Advanced Age and Stage-Dependent MET Genomic Amplification and c-Met Overexpression. J. Clin. Oncol. 2016, 34, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Tong, J.H.; Yeung, S.F.; Chan, A.W.; Chung, L.Y.; Chau, S.L.; Lung, R.W.; Tong, C.Y.; Chow, C.; Tin, E.K.; Yu, Y.H.; et al. MET Amplification and Exon 14 Splice Site Mutation Define Unique Molecular Subgroups of Non-Small Cell Lung Carcinoma with Poor Prognosis. Clin. Cancer Res. 2016, 22, 3048–3056. [Google Scholar] [CrossRef]
- Liu, X.; Jia, Y.; Stoopler, M.B.; Shen, Y.; Cheng, H.; Chen, J.; Mansukhani, M.; Koul, S.; Halmos, B.; Borczuk, A.C. Next-Generation Sequencing of Pulmonary Sarcomatoid Carcinoma Reveals High Frequency of Actionable MET Gene Mutations. J. Clin. Oncol. 2016, 34, 794–802. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Burke, A.P.; Marx, A.; Nicholson, A.G. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart, 4th ed.; IARC Press: Lyon, France, 2015. [Google Scholar]
- Wynes, M.W.; Sholl, L.M.; Dietel, M.; Schuuring, E.; Tsao, M.S.; Yatabe, Y.; Tubbs, R.R.; Hirsch, F.R. An international interpretation study using the ALK IHC antibody D5F3 and a sensitive detection kit demonstrates high concordance between ALK IHC and ALK FISH and between evaluators. J. Thorac. Oncol. 2014, 9, 631–638. [Google Scholar] [CrossRef]
- Tsao, M.S.; Kerr, K.M.; Kockx, M.; Beasley, M.B.; Borczuk, A.C.; Botling, J.; Bubendorf, L.; Chirieac, L.; Chen, G.; Chou, T.Y.; et al. PD-L1 Immunohistochemistry Comparability Study in Real-Life Clinical Samples: Results of Blueprint Phase 2 Project. J. Thorac. Oncol. 2018, 13, 1302–1311. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.M.; Laeremans, A.; Wang, X.M.; Wu, X.; Zhang, B.; Doolittle, E.; Kim, J.; Li, N.; Pimentel, H.X.Y.; Park, E.; et al. Visualizing Genetic Variants, Short Targets, and Point Mutations in the Morphological Tissue Context with an RNA In Situ Hybridisation Assay. J. Vis. Exp. 2018, 138, 58097. [Google Scholar]
- Letovanec, I.; Finn, S.; Zygoura, P.; Smyth, P.; Soltermann, A.; Bubendorf, L.; Speel, E.J.; Marchetti, A.; Nonaka, D.; Monkhorst, K.; et al. Evaluation of NGS and RT-PCR Methods for ALK Rearrangement in European NSCLC Patients: Results from the European Thoracic Oncology Platform Lungscape Project. J. Thorac. Oncol. 2018, 13, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, N.A.; Hellmann, M.D.; Snyder, A.; Kvistborg, P.; Makarov, V.; Havel, J.J.; Lee, W.; Yuan, J.; Wong, P.; Ho, T.S.; et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 2015, 348, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Decoster, L.; Giron, P.; Mignon, S.; De Greve, J. The evolving first-line treatment of advanced non-small cell lung cancer harbouring epidermal growth factor receptor mutations. Transl. Lung Cancer Res. 2018, 7, S134–S137. [Google Scholar] [CrossRef] [Green Version]
- Sim, E.H.; Yang, I.A.; Wood-Baker, R.; Bowman, R.V.; Fong, K.M. Gefitinib for advanced non-small cell lung cancer. Cochrane Database Syst. Rev. 2018, 1, CD006847. [Google Scholar] [CrossRef]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef]
- Paik, P.K.; Drilon, A.; Fan, P.D.; Yu, H.; Rekhtman, N.; Ginsberg, M.S.; Borsu, L.; Schultz, N.; Berger, M.F.; Rudin, C.M.; et al. Response to MET inhibitors in patients with stage IV lung adenocarcinomas harboring MET mutations causing exon 14 skipping. Cancer Discov. 2015, 5, 842–849. [Google Scholar] [CrossRef] [Green Version]
- Jorge, S.E.; Schulman, S.; Freed, J.A.; VanderLaan, P.A.; Rangachari, D.; Kobayashi, S.S.; Huberman, M.S.; Costa, D.B. Responses to the multitargeted MET/ALK/ROS1 inhibitor crizotinib and co-occurring mutations in lung adenocarcinomas with MET amplification or MET exon 14 skipping mutation. Lung Cancer 2015, 90, 369–374. [Google Scholar] [CrossRef] [Green Version]
- Waqar, S.N.; Morgensztern, D.; Sehn, J. MET Mutation Associated with Responsiveness to Crizotinib. J. Thorac. Oncol. 2015, 10, e29–e31. [Google Scholar] [CrossRef] [Green Version]
- Mendenhall, M.A.; Goldman, J.W. MET-Mutated NSCLC with Major Response to Crizotinib. J. Thorac. Oncol. 2015, 10, e33–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabari, J.K.; Leonardi, G.C.; Shu, C.A.; Umeton, R.; Montecalvo, J.; Ni, A.; Chen, R.; Dienstag, J.; Mrad, C.; Bergagnini, I.; et al. PD-L1 expression, tumor mutational burden, and response to immunotherapy in patients with MET exon 14 altered lung cancers. Ann. Oncol. 2018, 29, 2085–2091. [Google Scholar] [CrossRef] [PubMed]
- Scagliotti, G.; von Pawel, J.; Novello, S.; Ramlau, R.; Favaretto, A.; Barlesi, F.; Akerley, W.; Orlov, S.; Santoro, A.; Spigel, D.; et al. Phase III Multinational, Randomized, Double-Blind, Placebo-Controlled Study of Tivantinib (ARQ 197) Plus Erlotinib Versus Erlotinib Alone in Previously Treated Patients with Locally Advanced or Metastatic Nonsquamous Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2015, 33, 2667–2674. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, H.; Azuma, K.; Yamamoto, N.; Takahashi, T.; Nishio, M.; Katakami, N.; Ahn, M.J.; Hirashima, T.; Maemondo, M.; Kim, S.W.; et al. A randomized, double-blind, placebo-controlled, phase III trial of erlotinib with or without a c-Met inhibitor tivantinib (ARQ 197) in Asian patients with previously treated stage IIIB/IV nonsquamous nonsmall-cell lung cancer harboring wild-type epidermal growth factor receptor (ATTENTION study). Ann. Oncol. 2015, 26, 2066–2072. [Google Scholar] [PubMed] [Green Version]
- Spigel, D.R.; Edelman, M.J.; O’Byrne, K.; Paz-Ares, L.; Mocci, S.; Phan, S.; Shames, D.S.; Smith, D.; Yu, W.; Paton, V.E.; et al. Results from the Phase III Randomized Trial of Onartuzumab Plus Erlotinib Versus Erlotinib in Previously Treated Stage IIIB or IV Non-Small-Cell Lung Cancer: METLung. J. Clin. Oncol. 2017, 35, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Heist, R.S.; Shim, H.S.; Gingipally, S.; Mino-Kenudson, M.; Le, L.; Gainor, J.F.; Zheng, Z.; Aryee, M.; Xia, J.; Jia, P.; et al. MET Exon 14 Skipping in Non-Small Cell Lung Cancer. Oncologist 2016, 21, 481–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, G.D.; Lee, S.E.; Oh, D.Y.; Yu, D.B.; Jeong, H.M.; Kim, J.; Hong, S.; Jung, H.S.; Oh, E.; Song, J.Y.; et al. MET Exon 14 Skipping Mutations in Lung Adenocarcinoma: Clinicopathologic Implications and Prognostic Values. J. Thorac. Oncol. 2017, 12, 1233–1246. [Google Scholar] [CrossRef]
- Qiu, T.; Li, W.; Zhang, T.; Xing, P.; Huang, W.; Wang, B.; Chu, L.; Guo, L.; Liu, X.; Li, Y.; et al. Distinct MET Protein Localization Associated with MET Exon 14 Mutation Types in Patients with Non-small-cell Lung Cancer. Clin. Lung Cancer 2018, 19, e391–e398. [Google Scholar] [CrossRef]
- Wallace, A.J. New challenges for BRCA testing: A view from the diagnostic laboratory. Eur. J. Hum. Genet. 2016, 24 (Suppl. 1), S10–S18. [Google Scholar] [CrossRef]
- Buermans, H.P.; den Dunnen, J.T. Next generation sequencing technology: Advances and applications. Biochim. Biophys. Acta 2014, 1842, 1932–1941. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Specimens | Specimen Type | Modalities Used to Confirm Presence of METex14 Skipping | METex14 Skipping Present |
|---|---|---|---|
| Cohort 1 | |||
| Patient 1 (SJH01) | Lung resection—Adenocarcinoma | PCR, RISH, NGS | Y |
| Patient 2 (SVUH001) | Lung resection—Adenocarcinoma | PCR, RISH, NGS | Y |
| Patient 3 (SVUH002) | Lung resection—Sarcomatoid carcinoma | PCR, RISH, NGS | Y |
| Patient 4 (SG01) | Lymph Node—Large cell lung carcinoma | PCR, RISH, NGS | Y |
| Patient 5 (SG02) | Lung resection—Adenocarcinoma | PCR, RISH, NGS | Y |
| Patient 6 (SG03) | Lung resection—Undifferentiated-pleomorphic cancer of the lung | PCR, RISH, NGS | Y |
| Cohort 2 | |||
| 001 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 002 | Lung resection—Sarcomatoid carcinoma | PCR, RISH, NGS | Y |
| 003 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 004 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 005 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 006 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 007 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 008 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 009 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 010 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 011 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 012 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 013 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 014 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 015 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 016 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 017 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 018 | Lung resection—Sarcomatoid carcinoma | PCR, RISH, NGS | Y |
| 019 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| 020 | Lung resection—Sarcomatoid carcinoma | PCR | N |
| Standard | % METex14 | METex14 GBlock (10 ng/µL) (µL) | MetWT GBlock (10 ng/µL) (µL) | Total DNA (ng) |
|---|---|---|---|---|
| 1 | 100 | 5 | 0 | 50 |
| 2 | 75 | 3.75 | 1.25 | 50 |
| 3 | 50 | 2.5 | 2.5 | 50 |
| 4 | 25 | 1.25 | 3.75 | 50 |
| 5 | 10 | 0.5 | 4.5 | 50 |
| 6 | 5 | 0.25 | 4.75 | 50 |
| 7 | 0 | 0 | 0 | 50 |
| Immunohistochemistry | PCR | RNA In Situ Hybridisation | Next-Generation Sequencing | |
|---|---|---|---|---|
| Benefits | -Cheap and cost-effective -Rapid result -Easily performed by a standard pathology laboratory -Direct visualisation of tissue | -Rapid result -Reliable, accurate method of detection | -Direct visualisation of tissue -Reliable, accurate method of detection | -High throughput -Reliable, accurate method of detection -Ability to multiplex -Automated analysis |
| Disadvantages | -Not specific for MET exon 14 skipping splice variant -Heterogeneity of staining has been reported -Interobserver variability | -No direct visualisation of tissue -Easily performed by a standard pathology laboratory | -Expensive reagents -More time consuming if process not automated -Requires multiple sections | -High start-up costs -Dedicated data analysis and storage required -No direct visualisation of tissue -Reduced sensitivity for large insertions or deletions >20 base pairs (bp) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Brien, O.; Wright, M.C.; O’Brien, C.; Geoghegan, O.; Leonard, N.; Nicholson, S.; Cuffe, S.; Fabre, A.; Jochum, W.; Joerger, M.; et al. Cost-Efficient and Easy to Perform PCR-Based Assay to Identify Met Exon 14 Skipping in Formalin-Fixed Paraffin-Embedded (FFPE) Non-Small Cell Lung Cancer (NSCLC) Samples. Diagnostics 2019, 9, 13. https://doi.org/10.3390/diagnostics9010013
O’Brien O, Wright MC, O’Brien C, Geoghegan O, Leonard N, Nicholson S, Cuffe S, Fabre A, Jochum W, Joerger M, et al. Cost-Efficient and Easy to Perform PCR-Based Assay to Identify Met Exon 14 Skipping in Formalin-Fixed Paraffin-Embedded (FFPE) Non-Small Cell Lung Cancer (NSCLC) Samples. Diagnostics. 2019; 9(1):13. https://doi.org/10.3390/diagnostics9010013
Chicago/Turabian StyleO’Brien, Odharnaith, Mark C. Wright, Cathal O’Brien, Orla Geoghegan, Niamh Leonard, Siobhan Nicholson, Sinéad Cuffe, Aurelie Fabre, Wolfram Jochum, Markus Joerger, and et al. 2019. "Cost-Efficient and Easy to Perform PCR-Based Assay to Identify Met Exon 14 Skipping in Formalin-Fixed Paraffin-Embedded (FFPE) Non-Small Cell Lung Cancer (NSCLC) Samples" Diagnostics 9, no. 1: 13. https://doi.org/10.3390/diagnostics9010013