
Differential Diagnosis of Solid Pancreatic Lesions Using Detective Flow Imaging Endoscopic Ultrasonography
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. EUS Examination
2.3. Image Evaluation
2.4. Study Design
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
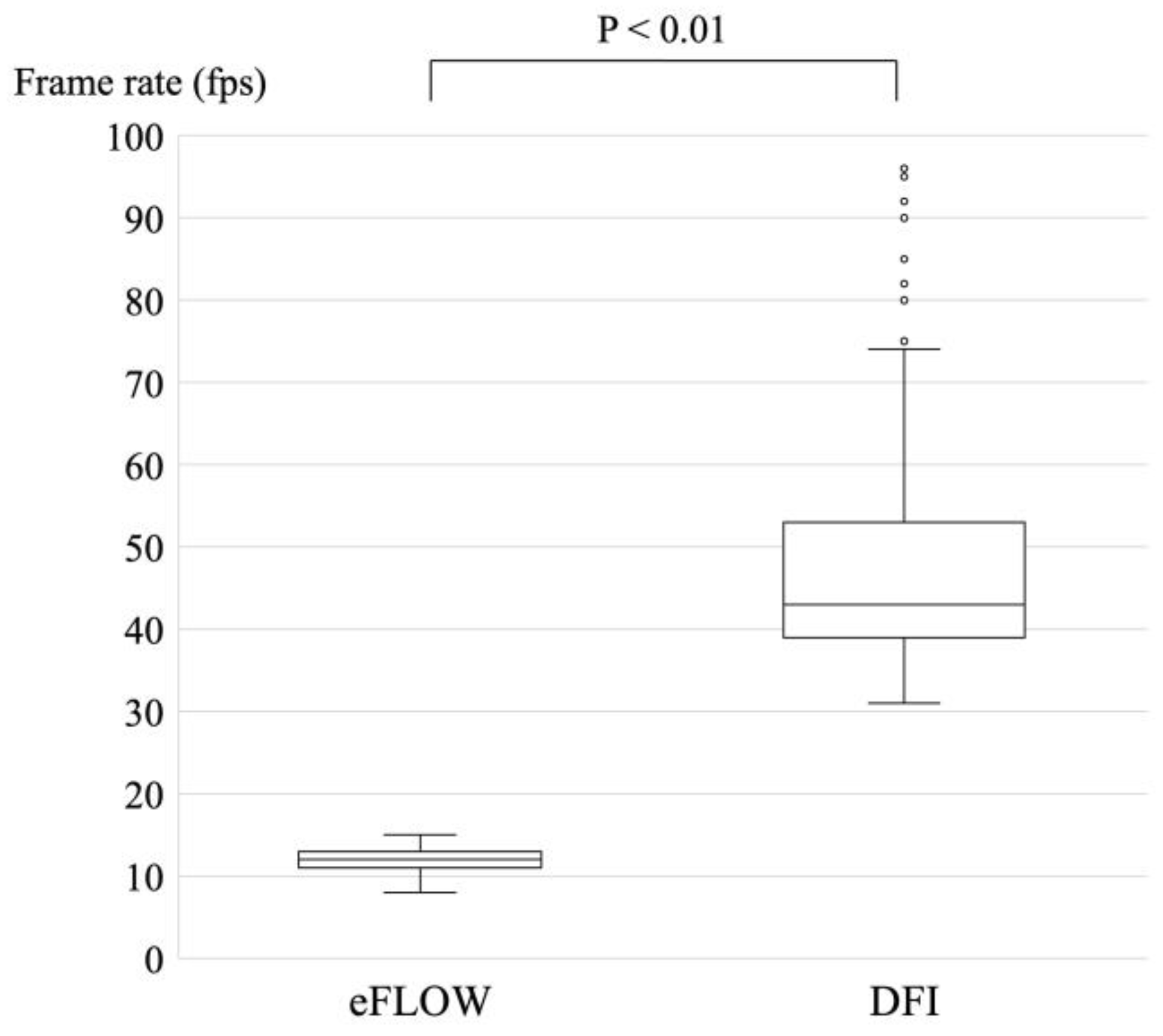
3.2. Frame Rates of eFLOW and DFI
3.3. Vessel Detection Rates of eFLOW and DFI
3.4. Findings of Pancreatic Cancer
3.5. Diagnostic Criteria for Pancreatic Cancer
3.6. Findings on Lesions Other Than Pancreatic Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martínez-Noguera, A.; D’Onofrio, M. Ultrasonography of the Pancreas. 1. Conventional Imaging. Abdom. Imaging 2007, 32, 136–149. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, M.; Gallotti, A.; Pozzi Mucelli, R. Imaging Techniques in Pancreatic Tumors. Expert Rev. Med. Devices 2010, 7, 257–273. [Google Scholar] [CrossRef] [PubMed]
- Zamboni, G.A.; Ambrosetti, M.C.; D’Onofrio, M.; Pozzi Mucelli, R. Ultrasonography of the Pancreas. Radiol. Clin. N. Am. 2012, 50, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Ciaravino, V.; D’Onofrio, M. Pancreatic Ultrasound: State of the Art. J. Ultrasound Med. 2019, 38, 1125–1137. [Google Scholar] [CrossRef]
- Tanaka, S.; Nakaizumi, A.; Ioka, T.; Oshikawa, O.; Uehara, H.; Nakao, M.; Yamamoto, K.; Ishikawa, O.; Ohigashi, H.; Kitamra, T. Main Pancreatic Duct Dilatation: A Sign of High Risk for Pancreatic Cancer. Jpn. J. Clin. Oncol. 2002, 32, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Hanada, K.; Amano, H.; Abe, T. Early Diagnosis of Pancreatic Cancer: Current Trends and Concerns. Ann. Gastroenterol. Surg. 2017, 1, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Fusaroli, P.; Kypraios, D.; Caletti, G.; Eloubeidi, M.A. Pancreatico-Biliary Endoscopic Ultrasound: A Systematic Review of the Levels of Evidence, Performance and Outcomes. World J. Gastroenterol. 2012, 18, 4243–4256. [Google Scholar] [CrossRef] [PubMed]
- Teshima, C.W.; Sandha, G.S. Endoscopic Ultrasound in the Diagnosis and Treatment of Pancreatic Disease. World J. Gastroenterol. 2014, 20, 9976–9989. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Shi, L.; Koch, J.; Löwe, A.; Dong, Y.; Cui, X.; Worni, M.; Jenssen, C. Early Detection of Pancreatic Tumors by Advanced EUS Imaging. Minerva Gastroenterol. 2022, 68, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Osher, E.; Scapa, E.; Klausner, J.; Greenman, Y.; Tordjman, K.; Melhem, A.; Nachmany, I.; Sofer, Y.; Geva, R.; Blachar, A.; et al. Pancreatic Incidentaloma: Differentiating nonfunctioning pancreatic neuroendocirne tumors from intrapancreatic accessory spleen. Endocr. Pract. 2016, 22, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Lv, K.; Xiao, M.; Tan, L.; Gui, Y.; Zhang, J.; Chen, X.; Jia, W.; Li, J. The Diagnostic Performance of Contrast-Enhanced Ultrasound versus Contrast-Enhanced Computed Tomography for Pancreatic Carcinoma: A Systematic Review and Meta-Analysis. Transl. Cancer Res. 2022, 11, 3645–3656. [Google Scholar] [CrossRef] [PubMed]
- Das, K.; Kudo, M.; Kitano, M.; Sakamoto, H.; Komaki, T.; Takagi, T.; Yamao, K. Diagnostic Value of Endoscopic Ultrasound-Guided Directional EFLOW in Solid Pancreatic Lesions. J. Med. Ultrason. 2013, 40, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, G.; Fujita, N.; Noda, Y.; Ito, K.; Horaguchi, J.; Koshida, S.; Kanno, Y.; Ogawa, T.; Masu, K.; Michikawa, Y. Vascular Image in Autoimmune Pancreatitis by Contrast-Enhanced Color-Doppler Endoscopic Ultrasonography: Comparison with Pancreatic Cancer. Endosc. Ultrasound 2014, 3, S13. [Google Scholar] [CrossRef] [PubMed]
- Kitano, M.; Kudo, M.; Yamao, K.; Takagi, T.; Sakamoto, H.; Komaki, T.; Kamata, K.; Imai, H.; Chiba, Y.; Okada, M.; et al. Characterization of Small Solid Tumors in the Pancreas: The Value of Contrast-Enhanced Harmonic Endoscopic Ultrasonography. Am. J. Gastroenterol. 2012, 107, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Kwek, B.E.A.; Ang, T.L.; Seo, D.W.; Imazu, H. Contrast-Enhanced Harmonic Endoscopic Ultrasonography of Solid Pancreatic Lesions. Endosc. Ultrasound 2013, 2, 142–147. [Google Scholar] [PubMed]
- Kitano, M.; Kamata, K.; Imai, H.; Miyata, T.; Yasukawa, S.; Yanagisawa, A.; Kudo, M. Contrast-Enhanced Harmonic Endoscopic Ultrasonography for Pancreatobiliary Diseases. Dig. Endosc. 2015, 27 (Suppl. S1), 60–67. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Sahai, A.V.; D’Onofrio, M.; Will, U.; Arcidiacono, P.G.; Petrone, M.C.; Hocke, M.; Braden, B.; Burmester, E.; Möller, K.; et al. Differential Diagnosis of Small Solid Pancreatic Lesions. Gastrointest. Endosc. 2016, 84, 933–940. [Google Scholar] [CrossRef] [PubMed]
- Kitano, M.; Yamashita, Y. New Imaging Techniques for Endoscopic Ultrasonography: Contrast-Enhanced Endoscopic Ultrasonography. Gastrointest. Endosc. Clin. N. Am. 2017, 27, 569–583. [Google Scholar] [CrossRef] [PubMed]
- He, X.-K.; Ding, Y.; Sun, L.-M. Contrast-Enhanced Endoscopic Ultrasound for Differential Diagnosis of Pancreatic Cancer: An Updated Meta-Analysis. Oncotarget 2017, 8, 66392–66401. [Google Scholar] [CrossRef] [PubMed]
- Omoto, S.; Kitano, M.; Fukasawa, M.; Ashida, R.; Kato, H.; Shiomi, H.; Sugimori, K.; Kanno, A.; Chiba, Y.; Takano, S.; et al. Tissue Harmonic versus Contrast-Enhanced Harmonic Endoscopic Ultrasonography for the Diagnosis of Pancreatic Tumors: Prospective Multicenter Study. Dig. Endosc. 2022, 34, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Miwa, H.; Numata, K.; Sugimori, K.; Kaneko, T.; Sakamaki, K.; Ueda, M.; Fukuda, H.; Tanaka, K.; Maeda, S. Differential Diagnosis of Solid Pancreatic Lesions Using Contrast-Enhanced Three-Dimensional Ultrasonography. Abdom. Imaging 2014, 39, 988–999. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.; Meng, Y.; Zhang, Y.; Zhao, W.; Wang, X.; Jin, M.; Guo, R. Superb Microvascular Imaging (SMI) Compared with Conventional Ultrasound for Evaluating Thyroid Nodules. BMC Med. Imaging 2017, 17, 65. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, Y.; Ishida, H.; Naganuma, H.; Komatsuda, T.; Miyazawa, H.; Miyauchi, T.; Takahashi, S.; Tozawa, T.; Enomoto, K. Superb Microvascular Imaging (SMI) Findings of Splenic Artery Pseudoaneurysm: A Report of Two Cases. J. Med. Ultrason. 2018, 45, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zhou, P.; Zhao, Y.; Tian, S.; Wu, X. Superb Microvascular Imaging Compared with Contrast-Enhanced Ultrasound for Assessing Laser Ablation Treatment of Benign Thyroid Nodules. BioMed Res. Int. 2018, 2018, 1025657. [Google Scholar] [CrossRef] [PubMed]
- Miwa, H.; Numata, K.; Sugimori, K.; Kaneko, T.; Maeda, S. Vascular Evaluation Using Transabdominal Ultrasound for Gallbladder Polyps. J. Med. Ultrason. 2021, 48, 159–173. [Google Scholar] [CrossRef] [PubMed]
- Bakdik, S.; Arslan, S.; Oncu, F.; Durmaz, M.S.; Altunkeser, A.; Eryilmaz, M.A.; Unlu, Y. Effectiveness of Superb Microvascular Imaging for the Differentiation of Intraductal Breast Lesions. Med. Ultrason. 2018, 20, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, A.G.; Mlekusch, I.; Wickenhauser, G.; Assadian, A.; Taher, F. Clinical Applications of B-Flow Ultrasound: A Scoping Review of the Literature. Diagnostics 2023, 13, 397. [Google Scholar] [CrossRef] [PubMed]
- Matsui, M.; Jikuzono, T.; Kure, S.; Ishibashi, O.; Akasu, H.; Sugitani, I. Usefulness of Ultrasonographic Detective Flow Imaging to Diagnose Parathyroid Tumors: Two Case Reports. J. Nippon Med. Sch. 2022, 90, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Yoshikawa, T.; Yamazaki, H.; Kawaji, Y.; Tamura, T.; Hatamaru, K.; Itonaga, M.; Ashida, R.; Ida, Y.; Maekita, T.; et al. A Novel Endoscopic Ultrasonography Imaging Technique for Depicting Microcirculation in Pancreatobiliary Lesions without the Need for Contrast-Enhancement: A Prospective Exploratory Study. Diagnostics 2021, 11, 2018. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Yoshikawa, T.; Kawaji, Y.; Tamura, T.; Hatamaru, K.; Itonaga, M.; Ida, Y.; Maekita, T.; Iguchi, M.; Murata, S.I.; et al. Novel Endoscopic Ultrasonography Imaging Technique for Visualizing Microcirculation without Contrast Enhancement in Subepithelial Lesions: Prospective Study. Dig. Endosc. 2021, 33, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Miwa, H.; Sugimori, K.; Maeda, S. Vessel Images of Gallbladder Polypoid Lesions on Detective Flow Imaging Endoscopic Ultrasonography. Dig. Endosc. 2023, 35, e61–e62. [Google Scholar] [CrossRef] [PubMed]
- Balaban, D.V.; Coman, L.; Marin, F.S.; Balaban, M.; Tabacelia, D.; Vasilescu, F.; Costache, R.S.; Jinga, M. Metastatic Renal Cell Carcinoma to Pancreas: Case Series and Review of the Literature. Diagnostics 2023, 13, 1368. [Google Scholar] [CrossRef] [PubMed]
- Ciaravino, V.; De Robertis, R.; Tinazzi Martini, P.; Cardobi, N.; Cingarlini, S.; Amodio, A.; Landoni, L.; Capelli, P.; D’Onofrio, M. Imaging Presentation of Pancreatic Neuroendocrine Neoplasms. Insights Imaging 2018, 9, 943–953. [Google Scholar] [CrossRef] [PubMed]
- Shankar, P.R.; Wasnik, A.P.; Al-Hawary, M.M.; Francis, I.R.; Kaza, R.K. Hypervascular Pancreatic “Lesions”: A Pattern-Based Approach to Differentiation. Abdom. Radiol. 2018, 43, 1013–1028. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.S.; Seo, D.-W.; So, H.; Ko, S.W.; Joo, H.D.; Oh, D.; Song, T.J.; Park, D.H.; Lee, S.S.; Lee, S.K.; et al. Clinical Utility of Directional EFLOW Compared with Contrast-Enhanced Harmonic Endoscopic Ultrasound for Assessing the Vascularity of Pancreatic and Peripancreatic Masses. Pancreatology 2022, 22, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Erkan, M.; Hausmann, S.; Michalski, C.W.; Schlitter, A.M.; Fingerle, A.A.; Dobritz, M.; Friess, H.; Kleeff, J. How Fibrosis Influences Imaging and Surgical Decisions in Pancreatic Cancer. Front. Physiol. 2012, 3, 389. [Google Scholar] [CrossRef] [PubMed]
- Erkan, M.; Hausmann, S.; Michalski, C.W.; Fingerle, A.A.; Dobritz, M.; Kleeff, J.; Friess, H. The Role of Stroma in Pancreatic Cancer: Diagnostic and Therapeutic Implications. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Fukui, H.; Onishi, H.; Nakamoto, A.; Tsuboyama, T.; Ota, T.; Yano, K.; Enchi, Y.; Yamada, D.; Takeda, Y.; Kobayashi, S.; et al. Pancreatic Fibrosis by Extracellular Volume Fraction Using Contrast-Enhanced Computed Tomography and Relationship with Pancreatic Cancer. Eur. J. Radiol. 2022, 156, 110522. [Google Scholar] [CrossRef] [PubMed]
- Nakai, Y.; Hamada, T.; Hakuta, R.; Ishigaki, K.; Saito, K.; Saito, T.; Takahara, N.; Mizuno, S.; Kogure, H.; Koike, K.; et al. Endoscopic Ultrasonography-guided Tissue Acquisition for Small Solid Pancreatic Lesions: Does the size matter? DEN Open 2021, 28, 352. [Google Scholar] [CrossRef] [PubMed]
- Crino, S.F.; Bellocchi, M.C.C.; Mitri, R.D.; Inzani, F.; Rimbas, M.; Lisotti, A.; Manfredi, G.; Teoh, A.Y.B.; Mangiavillano, B.; Sendino, O.; et al. Wet-suction versus slow-pull technique for endoscopic ultrasound-guided fine-needle biopsy: S multiceneter, randomized, crossover trial. Endoscopy 2023, 55, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Al-Salameh, A.; Cadiot, G.; Calender, A.; Goudet, P.; Chanson, P. Clinical Aspects of Multiple Endocrine Neoplasia Type 1. Nat. Rev. Endocrinol. 2021, 17, 207–224. [Google Scholar] [CrossRef] [PubMed]
- Zwolak, A.; Świrska, J.; Tywanek, E.; Dudzińska, M.; Tarach, J.S.; Matyjaszek-Matuszek, B. Pancreatic Neuroendocrine Tumours in Patients with von Hippel-Lindau Disease. Endokrynol. Pol. 2020, 71, 256–259. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 104 | |
|---|---|
| Age, median (range), years | 72.5 years (38–86) |
| Sex, male, n (%) | 54 (52%) |
| Disease, n (%) | |
| Pancreatic cancer | 83 (80%) |
| Mass-forming pancreatitis | 9 (8.7%) |
| Neuroendocrine neoplasm | 6 (5.8%) |
| Pancreatic metastasis from RCC | 3 (2.9%) |
| Intrapancreatic accessory spleen | 2 (1.9%) |
| Malignant lymphoma | 1 (1.0%) |
| Location of lesions, n (%) | |
| Pancreatic head | 50 (48%) |
| Pancreatic body/tail | 54 (52%) |
| Transgastric scan, n (%) | 56 (54%) |
| Diameter of lesions, median (range) | 21 mm (6–53) |
| Depth of lesions, median (range) | 27.5 mm (13–53) |
| Modality | Category | Findings | Pancreatic Cancer n = 83 | Other Lesions n = 21 | p Value |
|---|---|---|---|---|---|
| Characteristics | Age | >75 years | 31/83, 37% | 5/21, 24% | 0.244 |
| Sex | Male | 42/83, 51% | 13/21, 62% | 0.354 | |
| Location | Pancreatic head | 45/83, 54% | 5/21, 24% | 0.013 | |
| Transgastric scan | 41/83, 49% | 15/21, 71% | 0.070 | ||
| Diameter of lesions | >20 mm | 50/83, 60% | 8/21, 38% | 0.068 | |
| Depth | >25 mm | 52/83, 63% | 8/21, 38% | 0.042 | |
| B-mode | Echogenicity | Hypoechoic | 81/83, 98% | 21/21, 100% | 0.473 |
| Border | Indistinct | 24/83, 30% | 4/21, 19% | 0.362 | |
| Contour | Irregular | 73/83, 88% | 10/21, 48% | <0.01 | |
| Internal echo | Heterogeneous | 69/83, 83% | 11/21, 52% | <0.01 | |
| Diagnostic criteria for pancreatic cancer | Irregular or Heterogeneous | 78/83, 94% | 17/21, 81% | 0.058 | |
| eFLOW | Vessel detection | Present | 20/83, 24% | 8/21, 38% | 0.196 |
| Vessel distribution | Peri-tumoral | 17/20, 85% | 5/8, 63% | 0.200 | |
| Vessel shape | Spotty | 14/20, 70% | 4/8, 50% | 0.318 | |
| DFI | Vessel detection | Present | 79/83, 95% | 21/21, 100% | 0.305 |
| Vascularity | Hypovascular | 80/83, 96% | 11/21, 52% | <0.01 | |
| Vessel distribution | Peritumoral | 66/79, 84% | 8/21, 38% | <0.01 | |
| Vessel shape | Spotty | 68/79, 86% | 9/21, 43% | <0.01 | |
| Diagnostic criteria for pancreatic cancer | Hypovascular or Peritumoral or Spotty | 82/83, 99% | 12/21, 57% | <0.01 |
| Modality | Findings | Sensitivity | Specificity | PPV | NPV | Accuracy |
|---|---|---|---|---|---|---|
| B-mode | Irregular or Heterogeneous | 94% (78/83) | 19% (4/21) | 82% (78/95) | 44% (4/9) | 79% (82/104) |
| eFLOW | Absence of vessels | 76% (63/83) | 38% (8/21) | 83% (63/76) | 29% (8/28) | 68% (71/104) |
| DFI | Hypovascular or Peritumoral or Spotty | 99% (82/83) | 43% (9/21) | 87% (82/94) | 90% (9/10) | 88% (91/94) |
| Modality | Category | Findings | NEN n = 6 | MFP n = 9 | p Value |
|---|---|---|---|---|---|
| Characteristics | Age | >75 years | 1/6, 17% | 2/9, 22% | 0.792 |
| Sex | Male | 3/6, 50% | 7/2, 78% | 0.264 | |
| Location | Pancreatic head | 1/5, 17% | 3/9, 33% | 0.475 | |
| Transgastric scan | 4/6, 67% | 6/9, 67% | 1.000 | ||
| Diameter of lesions | >20 mm | 1/6, 17% | 5/9, 56% | 0.132 | |
| Depth | >25 mm | 1/6, 17% | 5/9, 56% | 0.132 | |
| B-mode | Echogenicity | Hypoechoic | 6/6, 100% | 9/9, 100% | - |
| Border | Indistinct | 0/6, 0% | 4/9, 44% | 0.057 | |
| Contour | Irregular | 2/6, 33% | 7/9, 78% | 0.085 | |
| Internal echo | Heterogeneous | 2/6, 33% | 7/9, 78% | 0.085 | |
| eFLOW | Vessel detection | Present | 2/6, 33% | 2/9, 22% | 0.634 |
| DFI | Vessel detection | Present | 6/6, 100% | 9/9, 100% | - |
| Vascularity | Hypovascular | 1/6, 17% | 9/9, 100% | < 0.01 | |
| Vessel distribution | Peritumoral | 1/6, 17% | 5/9, 56% | 0.132 | |
| Vessel shape | Spotty | 1/6, 17% | 6/9, 67% | 0.572 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miwa, H.; Sugimori, K.; Yonei, S.; Yoshimura, H.; Endo, K.; Oishi, R.; Funaoka, A.; Tsuchiya, H.; Kaneko, T.; Numata, K.; et al. Differential Diagnosis of Solid Pancreatic Lesions Using Detective Flow Imaging Endoscopic Ultrasonography. Diagnostics 2024, 14, 882. https://doi.org/10.3390/diagnostics14090882
Miwa H, Sugimori K, Yonei S, Yoshimura H, Endo K, Oishi R, Funaoka A, Tsuchiya H, Kaneko T, Numata K, et al. Differential Diagnosis of Solid Pancreatic Lesions Using Detective Flow Imaging Endoscopic Ultrasonography. Diagnostics. 2024; 14(9):882. https://doi.org/10.3390/diagnostics14090882
Chicago/Turabian StyleMiwa, Haruo, Kazuya Sugimori, Shoichiro Yonei, Hayato Yoshimura, Kazuki Endo, Ritsuko Oishi, Akihiro Funaoka, Hiromi Tsuchiya, Takashi Kaneko, Kazushi Numata, and et al. 2024. "Differential Diagnosis of Solid Pancreatic Lesions Using Detective Flow Imaging Endoscopic Ultrasonography" Diagnostics 14, no. 9: 882. https://doi.org/10.3390/diagnostics14090882