

Deep Convolutional Neural Networks Provide Motion Grading for High-Resolution Peripheral Quantitative Computed Tomography of the Scaphoid
 , , , , , , and
, , , , , , and 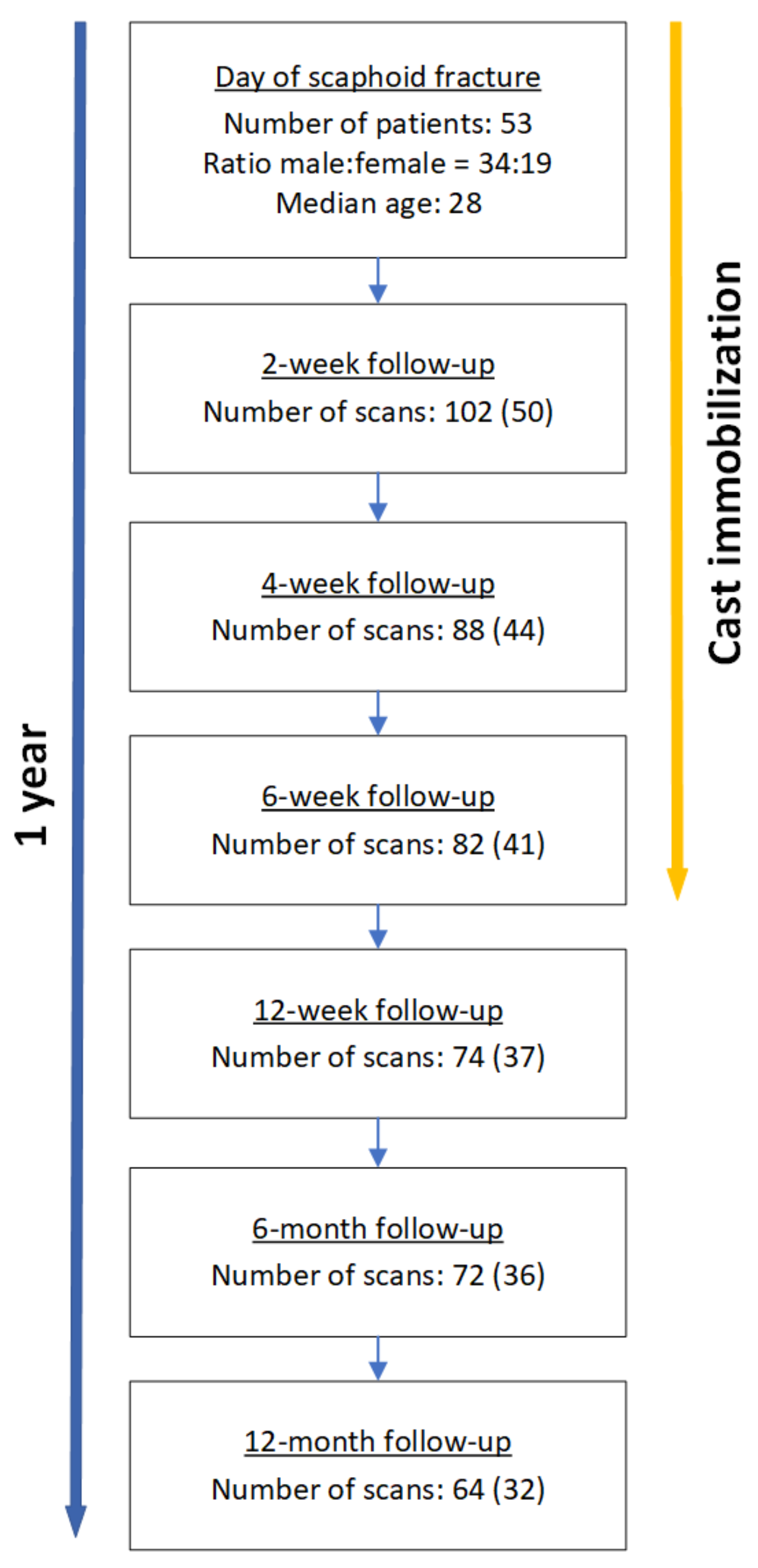{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Scan Acquisition
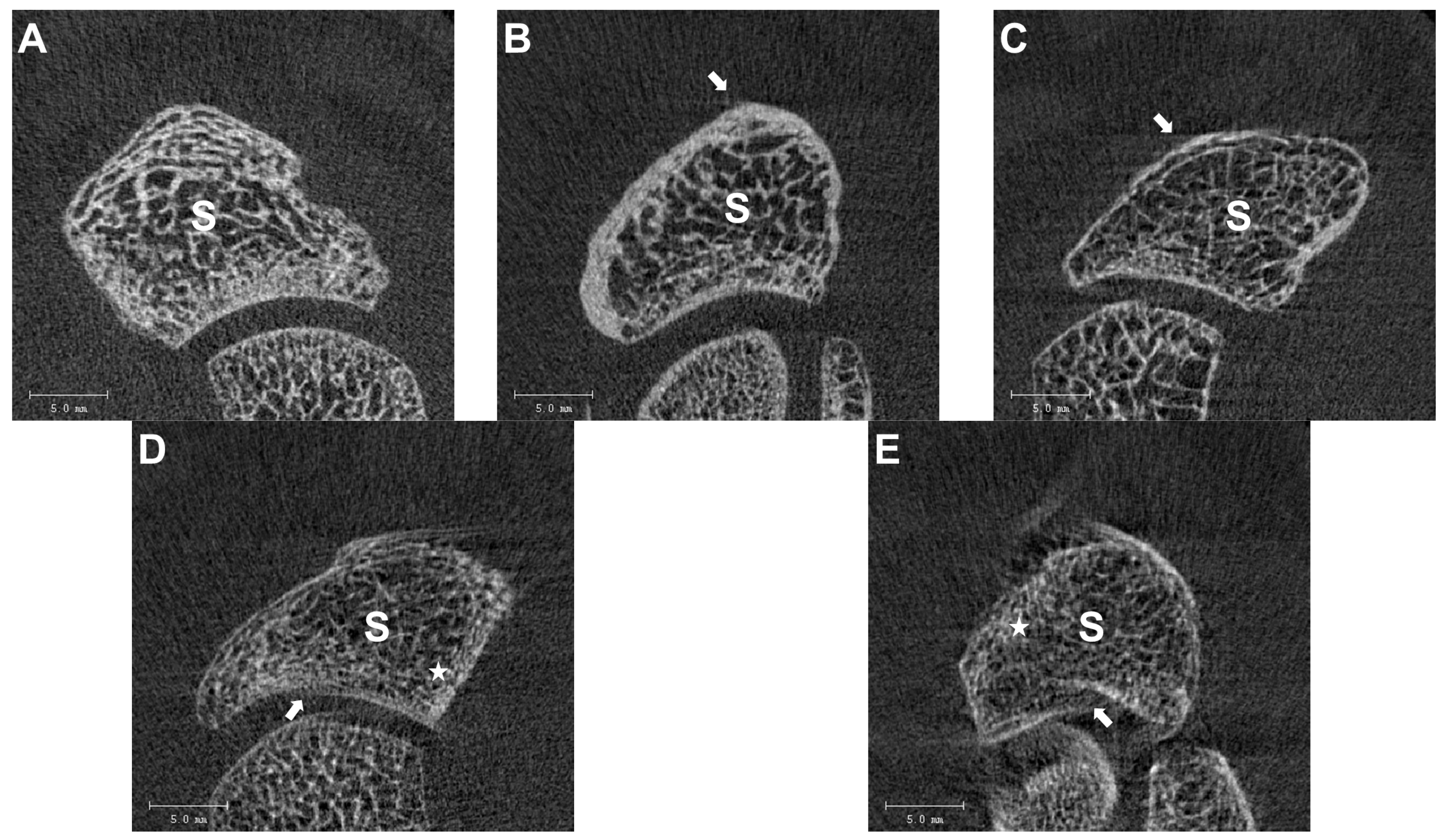
2.3. Image Quality Grading
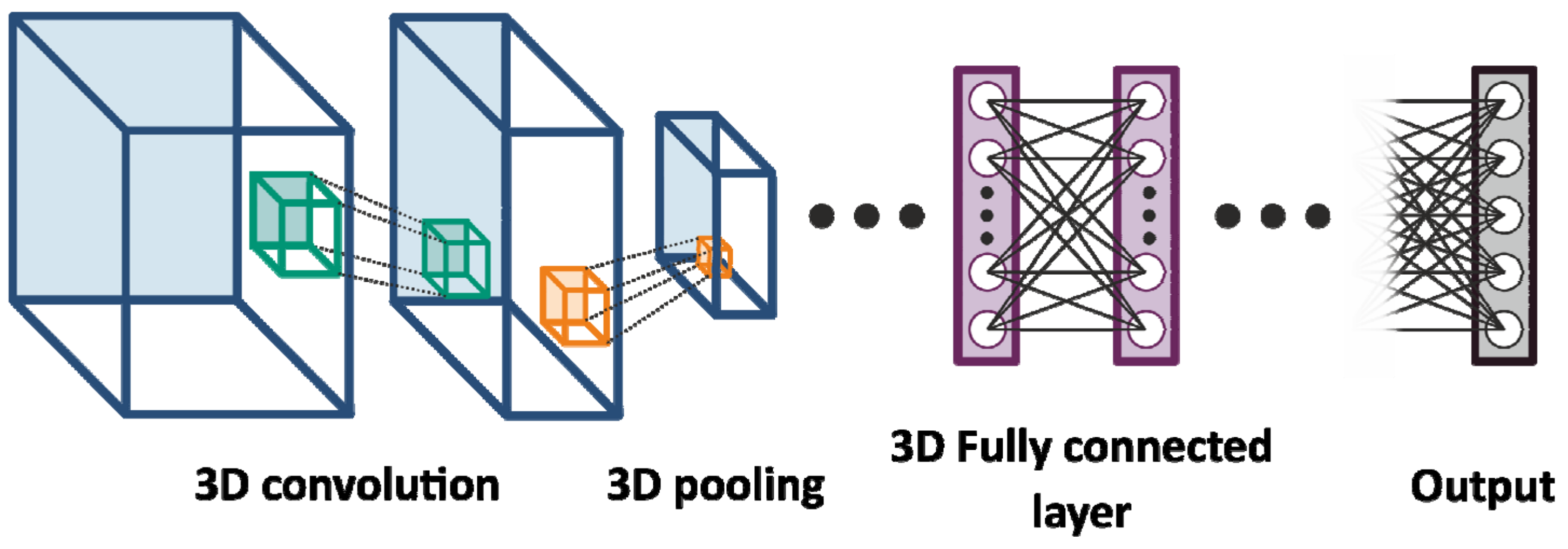
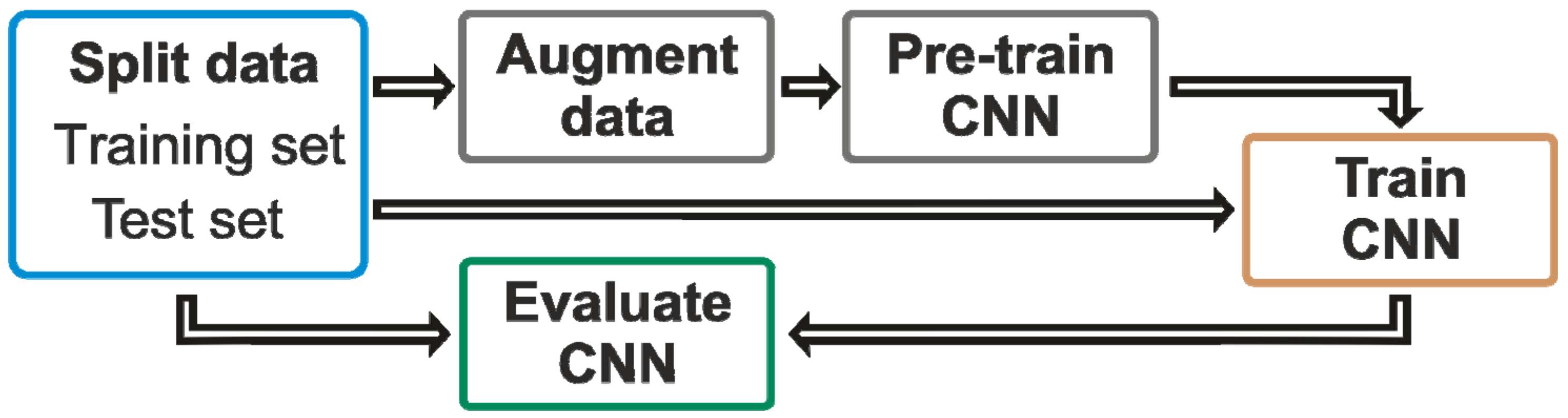
2.4. Machine-Learning Approach
3. Results
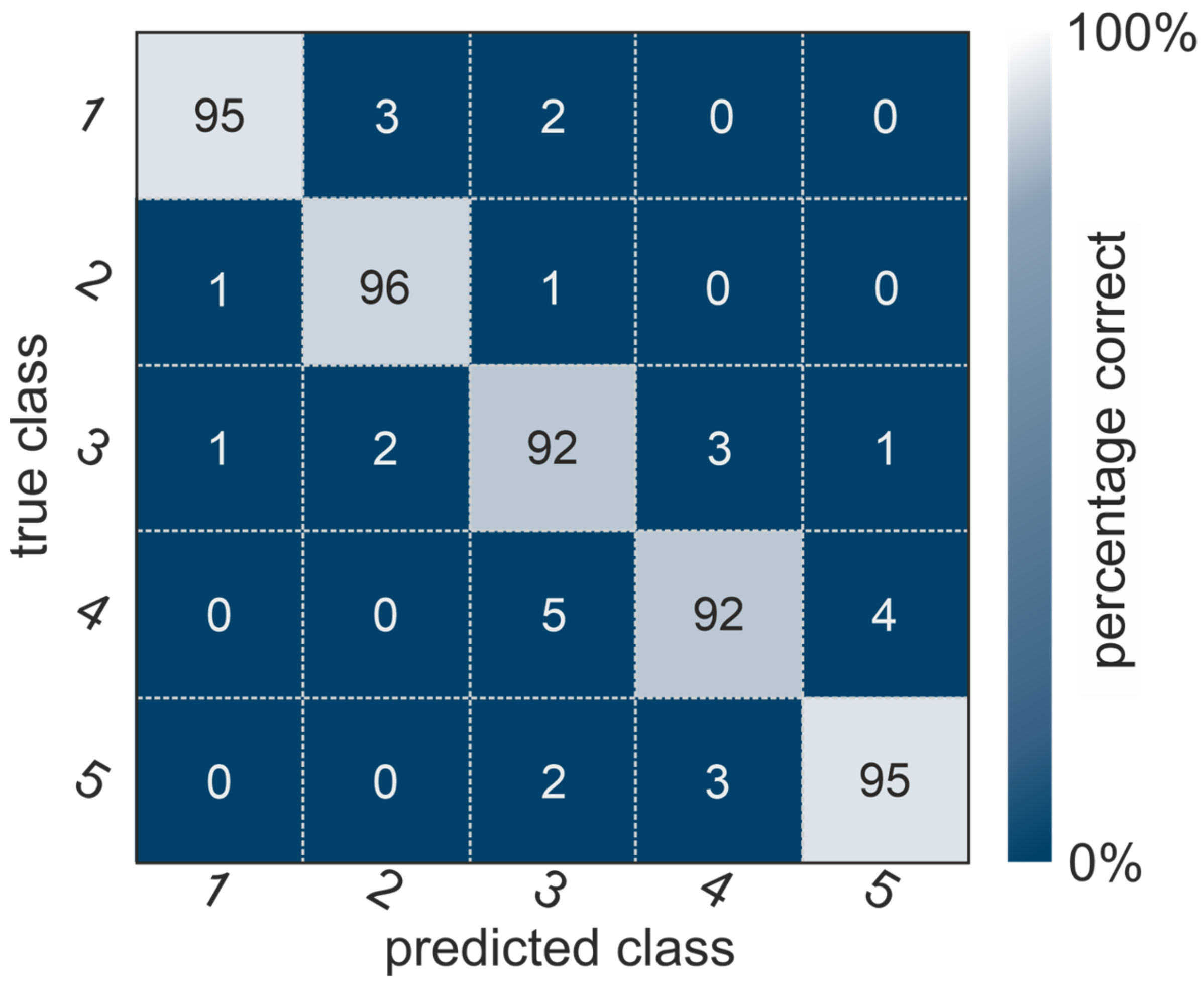
3.1. Confusion Matrix with High Accuracy
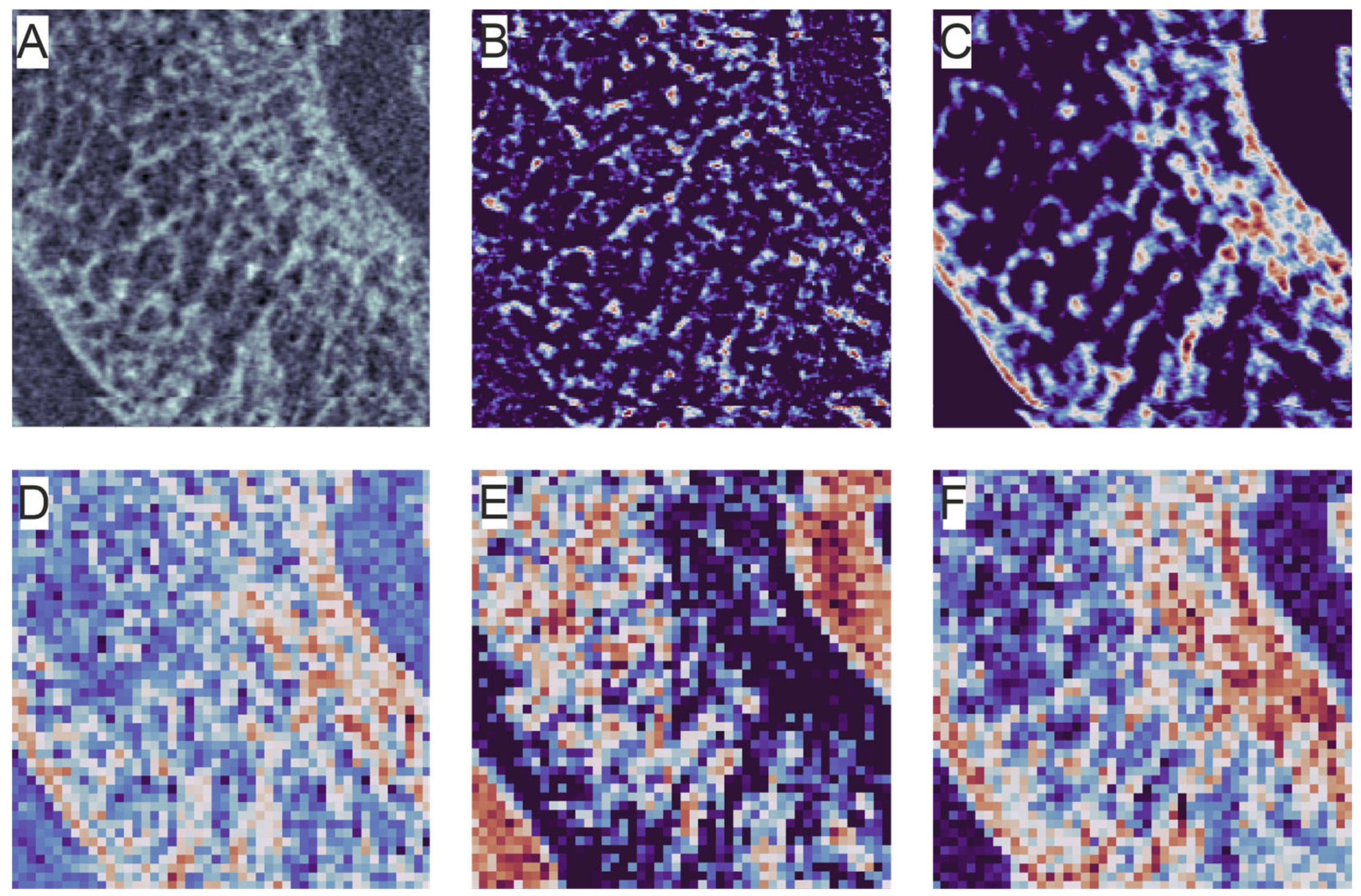
3.2. Suggested Focus of the Neural Network
3.3. Duration of the 3D-CNN Procedure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tada, K.; Ikeda, K.; Okamoto, S.; Hachinota, A.; Yamamoto, D.; Tsuchiya, H. Scaphoid Fracture—Overview and Conservative Treatment. Hand Surg. 2015, 20, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Jorgsholm, P.; Ossowski, D.; Thomsen, N.; Bjorkman, A. Epidemiology of scaphoid fractures and non-unions: A systematic review. Handchir. Mikrochir. Plast. Chir. 2020, 52, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Reigstad, O.; Grimsgaard, C.; Thorkildsen, R.; Reigstad, A.; Rokkum, M. Scaphoid non-unions, where do they come from? The epidemiology and initial presentation of 270 scaphoid non-unions. Hand Surg. 2012, 17, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Yin, Z.G.; Zhang, J.B.; Kan, S.L.; Wang, X.G. Diagnostic accuracy of imaging modalities for suspected scaphoid fractures: Meta-analysis combined with latent class analysis. J. Bone Jt. Surg. Br. 2012, 94, 1077–1085. [Google Scholar] [CrossRef]
- Adey, L.; Souer, J.S.; Lozano-Calderon, S.; Palmer, W.; Lee, S.G.; Ring, D. Computed tomography of suspected scaphoid fractures. J. Hand Surg. Am. 2007, 32, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Bevers, M.S.A.M.; Daniels, A.M.; Wyers, C.E.; van Rietbergen, B.; Geusens, P.P.M.M.; Kaarsemaker, S.; Janzing, H.M.J.; Hannemann, P.F.W.; Poeze, M.; van den Bergh, J.P.W. The Feasibility of High-Resolution Peripheral Quantitative Computed Tomography (HR-pQCT) in Patients with Suspected Scaphoid Fractures. J. Clin. Densitom. 2020, 23, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Daniels, A.M.; Wyers, C.E.; Janzing, H.M.J.; Sassen, S.; Loeffen, D.; Kaarsemaker, S.; van Rietbergen, B.; Hannemann, P.F.W.; Poeze, M.; van den Bergh, J.P. The interobserver reliability of the diagnosis and classification of scaphoid fractures using high-resolution peripheral quantitative CT. Bone Jt. J. 2020, 102-B, 478–484. [Google Scholar] [CrossRef]
- Daniels, A.M.; Bevers, M.S.A.M.; Sassen, S.; Wyers, C.E.; van Rietbergen, B.; Geusens, P.P.M.M.; Kaarsemaker, S.; Hannemann, P.F.W.; Poeze, M.; van den Bergh, J.P.; et al. Improved Detection of Scaphoid Fractures with High-Resolution Peripheral Quantitative CT Compared with Conventional CT. J. Bone Jt. Surg. Am. 2020, 102, 2138–2145. [Google Scholar] [CrossRef]
- Bevers, M.S.A.M.; Daniels, A.M.; van Rietbergen, B.; Geusens, P.P.M.M.; van Kuijk, S.M.J.; Sassen, S.; Kaarsemaker, S.; Hannemann, P.F.W.; Poeze, M.; Janzing, H.M.J.; et al. Assessment of the healing of conservatively-treated scaphoid fractures using HR-pQCT. Bone 2021, 153, 116161. [Google Scholar] [CrossRef]
- Deutschmann, J.P.J.; Valentinitsch, A.; Pietschmann, P.; Varga, P.D.A.E.; Zysset, P.; Weber, G.; Resch, H.; Kainberger, F. Research network osteology vienna: Hochauflösende- und Mikro-CT in der Wiener Osteologie. J. Miner. 2010, 17, 104–109. [Google Scholar]
- Krug, R.; Burghardt, A.J.; Majumdar, S.; Link, T.M. High-Resolution Imaging Techniques for the Assessment of Osteoporosis. Radiol. Clin. N. Am. 2010, 48, 601–621. [Google Scholar] [CrossRef] [PubMed]
- Link, T.M. Osteoporosis Imaging State of the Art and Advanced Imaging. Radiology 2012, 263, 3–17. [Google Scholar] [CrossRef] [PubMed]
- MacNeil, J.A.; Boyd, S.K. Improved reproducibility of high-resolution peripheral quantitative computed tomography for measurement of bone quality. Med. Eng. Phys. 2008, 30, 792–799. [Google Scholar] [CrossRef]
- Sode, M.; Burghardt, A.J.; Pialat, J.-B.; Link, T.M.; Majumdar, S. Quantitative characterization of subject motion in HR-pQCT images of the distal radius and tibia. Bone 2011, 48, 1291–1297. [Google Scholar] [CrossRef] [PubMed]
- Bonaretti, S.; Vilayphiou, N.; Chan, C.M.; Yu, A.; Nishiyama, K.; Liu, D.; Boutroy, S.; Ghasem-Zadeh, A.; Boyd, S.K.; Chapurlat, R.; et al. Operator variability in scan positioning is a major component of HR-pQCT precision error and is reduced by standardized training. Osteoporos. Int. 2017, 28, 245–257. [Google Scholar] [CrossRef]
- Zebaze, R.; Ghasem-Zadeh, A.; Mbala, A.; Seeman, E. A new method of segmentation of compact-appearing, transitional and trabecular compartments and quantification of cortical porosity from high resolution peripheral quantitative computed tomographic images. Bone 2013, 54, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Walle, M.; Eggemann, D.; Atkins, P.R.; Kendall, J.J.; Stock, K.; Müller, R.; Collins, C.J. Motion grading of high-resolution quantitative computed tomography supported by deep convolutional neural networks. Bone 2023, 166, 116607. [Google Scholar] [CrossRef]
- Pialat, J.B.; Burghardt, A.J.; Sode, M.; Link, T.M.; Majumdar, S. Visual grading of motion induced image degradation in high resolution peripheral computed tomography: Impact of image quality on measures of bone density and micro-architecture. Bone 2012, 50, 111–118. [Google Scholar] [CrossRef]
- Benedikt, S.; Horling, L.; Stock, K.; Degenhart, G.; Pallua, J.; Schmidle, G.; Arora, R. The impact of motion induced artifacts in the evaluation of HR- pQCT scans of the scaphoid bone: An assessment of inter- and intraobserver variability and quantitative parameters. Quant. Imaging Med. Surg. 2023, 13, 1336–1349. [Google Scholar] [CrossRef]
- Engelke, K.; Stampa, B.; Timm, W.; Dardzinski, B.; de Papp, A.E.; Genant, H.K.; Fuerst, T. Short-term in vivo precision of BMD and parameters of trabecular architecture at the distal forearm and tibia. Osteoporos. Int. 2012, 23, 2151–2158. [Google Scholar] [CrossRef]
- Pauchard, Y.; Liphardt, A.-M.; Macdonald, H.M.; Hanley, D.A.; Boyd, S.K. Quality control for bone quality parameters affected by subject motion in high-resolution peripheral quantitative computed tomography. Bone 2012, 50, 1304–1310. [Google Scholar] [CrossRef] [PubMed]
- Rantalainen, T.; Chivers, P.; Beck, B.R.; Robertson, S.; Hart, N.H.; Nimphius, S.; Weeks, B.K.; McIntyre, F.; Hands, B.; Siafarikas, A. Please Don’t Move-Evaluating Motion Artifact From Peripheral Quantitative Computed Tomography Scans Using Textural Features. J. Clin. Densitom. 2018, 21, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Blew, R.M.; Lee, V.R.; Farr, J.N.; Schiferl, D.J.; Going, S.B. Standardizing Evaluation of pQCT Image Quality in the Presence of Subject Movement: Qualitative Versus Quantitative Assessment. Calcif. Tissue Int. 2014, 94, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Pauchard, Y.; Ayres, F.J.; Boyd, S.K. Automated quantification of three-dimensional subject motion to monitor image quality in high-resolution peripheral quantitative computed tomography. Phys. Med. Biol. 2011, 56, 6523–6543. [Google Scholar] [CrossRef] [PubMed]
- Anwar, S.M.; Majid, M.; Qayyum, A.; Awais, M.; Alnowami, M.; Khan, M.K. Medical Image Analysis using Convolutional Neural Networks: A Review. J. Med. Syst. 2018, 42, 226. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.B.; Kim, H.J.; Chun, J.M.; Lee, C.S.; Kim, S.Y.; Kim, P.T.; Jeon, I.H. Osseous microarchitecture of the scaphoid: Cadaveric study of regional variations and clinical implications. Clin. Anat. 2012, 25, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Mata-Mbemba, D.; Rohringer, T.; Ibrahim, A.; Adams-Webberc, T.; Moineddin, R.; Doria, A.S.; Vali, R. HR-pQCT imaging in children, adolescents and young adults: Systematic review and subgroup meta-analysis of normative data. PLoS ONE 2019, 14, e0225663. [Google Scholar] [CrossRef] [PubMed]
- Kawalilak, C.E.; Johnston, J.D.; Olszynski, W.P.; Kontulainen, S.A. Characterizing microarchitectural changes at the distal radius and tibia in postmenopausal women using HR-pQCT. Osteoporos. Int. 2014, 25, 2057–2066. [Google Scholar] [CrossRef]
- Whittier, D.E.; Manske, S.L.; Boyd, S.K.; Schneider, P.S. The Correction of Systematic Error due to Plaster and Fiberglass Casts on HR-pQCT Bone Parameters Measured In Vivo at the Distal Radius. J. Clin. Densitom. 2019, 22, 401–408. [Google Scholar] [CrossRef]
- Zhang, Q.; Hann, E.; Werys, K.; Wu, C.; Popescu, I.; Lukaschuk, E.; Barutcu, A.; Ferreira, V.M.; Piechnik, S.K. Deep learning with attention supervision for automated motion artefact detection in quality control of cardiac T1-mapping. Artif. Intell. Med. 2020, 110, 101955. [Google Scholar] [CrossRef]
- Lorch, B.; Vaillant, G.; Baumgartner, C.; Bai, W.; Rueckert, D.; Maier, A. Automated Detection of Motion Artefacts in MR Imaging Using Decision Forests. J. Med. Eng. 2017, 2017, 4501647. [Google Scholar] [CrossRef]
- Faisal, A.; Khalil, A.; Chai Lai, K.W. X-ray carpal bone segmentation and area measurement. Multimed. Tools Appl. 2022, 81, 37321–37332. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benedikt, S.; Zelger, P.; Horling, L.; Stock, K.; Pallua, J.; Schirmer, M.; Degenhart, G.; Ruzicka, A.; Arora, R. Deep Convolutional Neural Networks Provide Motion Grading for High-Resolution Peripheral Quantitative Computed Tomography of the Scaphoid. Diagnostics 2024, 14, 568. https://doi.org/10.3390/diagnostics14050568
Benedikt S, Zelger P, Horling L, Stock K, Pallua J, Schirmer M, Degenhart G, Ruzicka A, Arora R. Deep Convolutional Neural Networks Provide Motion Grading for High-Resolution Peripheral Quantitative Computed Tomography of the Scaphoid. Diagnostics. 2024; 14(5):568. https://doi.org/10.3390/diagnostics14050568
Chicago/Turabian StyleBenedikt, Stefan, Philipp Zelger, Lukas Horling, Kerstin Stock, Johannes Pallua, Michael Schirmer, Gerald Degenhart, Alexander Ruzicka, and Rohit Arora. 2024. "Deep Convolutional Neural Networks Provide Motion Grading for High-Resolution Peripheral Quantitative Computed Tomography of the Scaphoid" Diagnostics 14, no. 5: 568. https://doi.org/10.3390/diagnostics14050568