

Improving Respiratory Infection Diagnosis with Deep Learning and Combinatorial Fusion: A Two-Stage Approach Using Chest X-ray Imaging

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
- In addressing the diagnostic challenges of respiratory infections, the application of artificial intelligence (AI) and deep learning is gaining prominence. Specifically, convolutional neural networks (CNNs) are employed to enhance the accuracy and efficiency of medical imaging diagnoses [8]. This study aims to leverage AI and deep learning to develop a more effective diagnostic tool for COVID-19 pneumonia, addressing the gaps and challenges in current diagnostic methodologies [9].
- The field of medical imaging has extensively adopted CNNs due to their utility in symptom identification and learning [10]. Furthermore, with the advent of deep CNNs and their successful application in various areas, the use of deep learning techniques with chest X-rays is becoming increasingly popular. This is bolstered by the availability of vast data sets to train deep-learning algorithms [11].
- Given the ongoing development of vaccines and treatments for COVID-19, deep learning-based techniques that assist radiologists in diagnosing this disease could potentially enable faster and more accurate assessments especially in remote areas [14].
2. Related Works
- Classified the diseases with five art of states pre-trained convolutional neural network using CXR images.
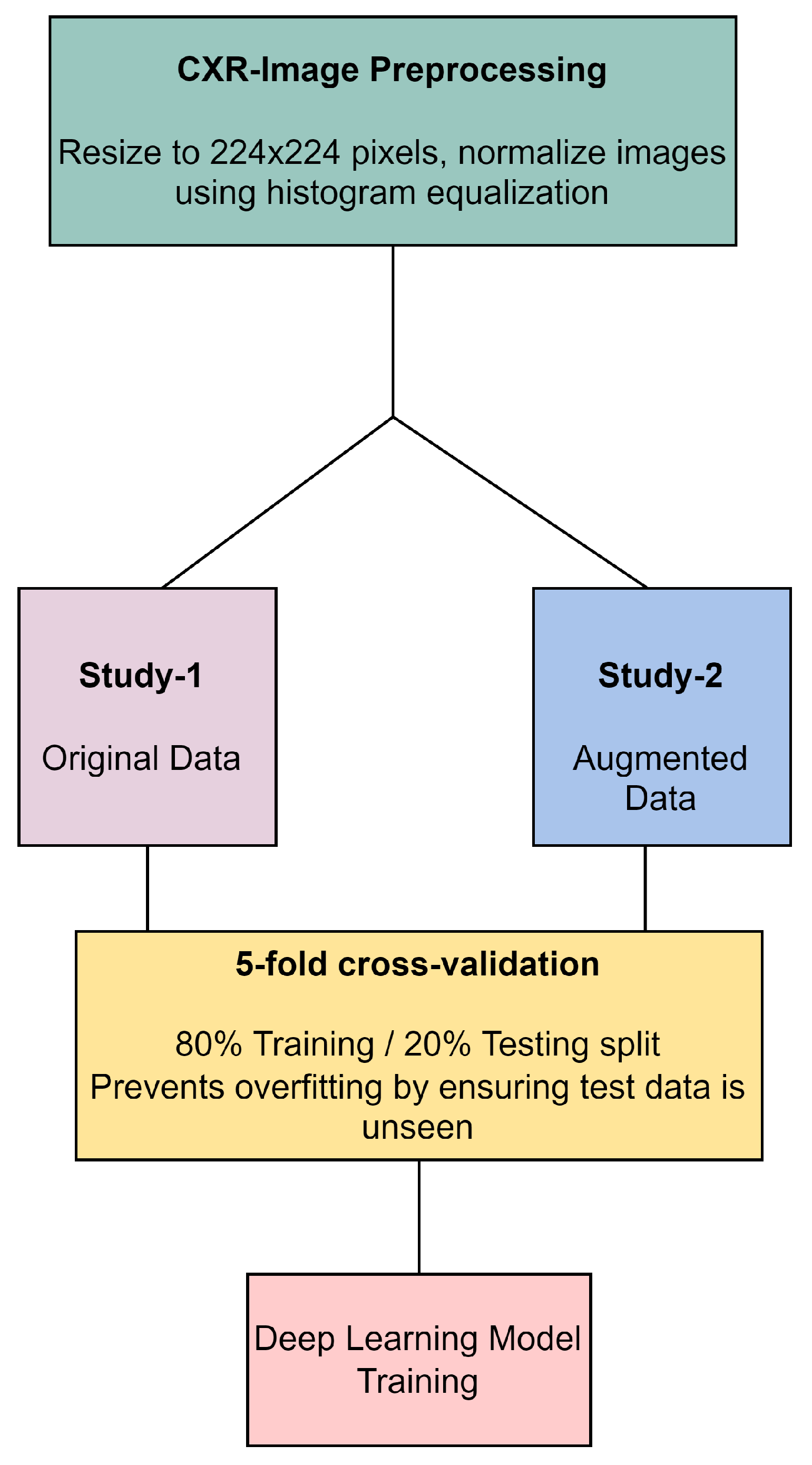
- To resolve data imbalance, the study employs a fivefold cross-validation approach, ensuring a balanced data representation and consistent model evaluation.
- Enhanced the deep learning model testing accuracy using combinatorial fusion analysis.
3. Datasets and Model
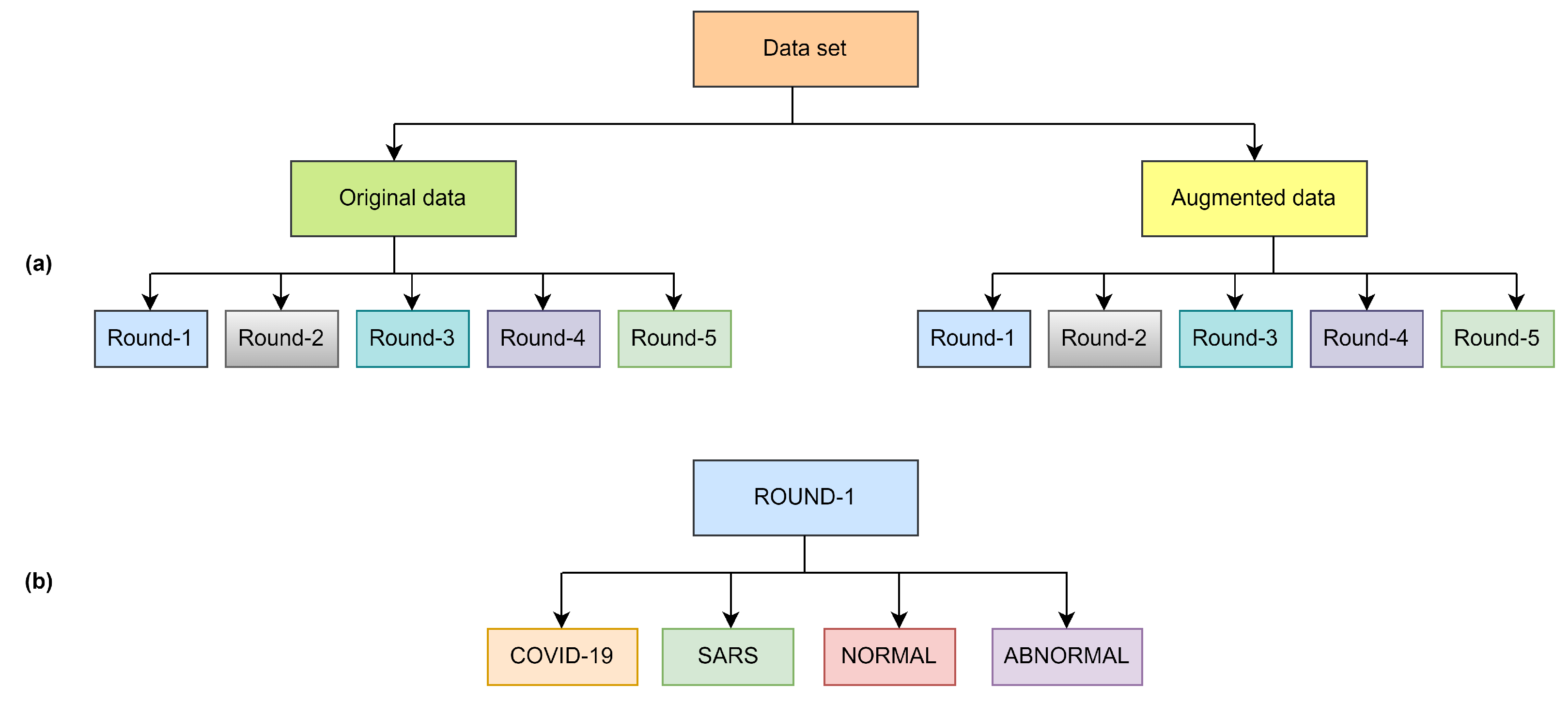
3.1. Datasets
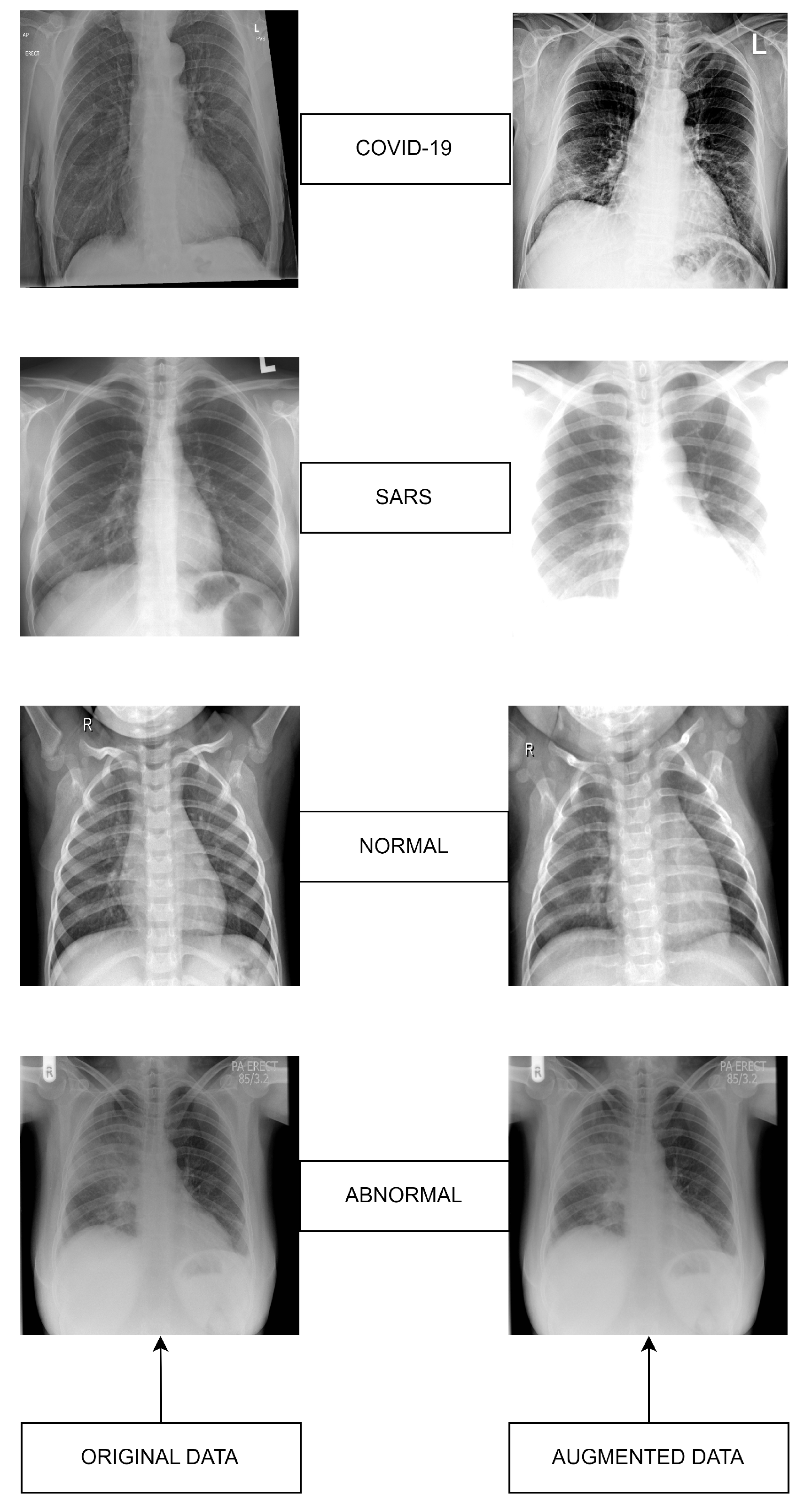
3.2. Original Dataset
3.3. Augmented Dataset
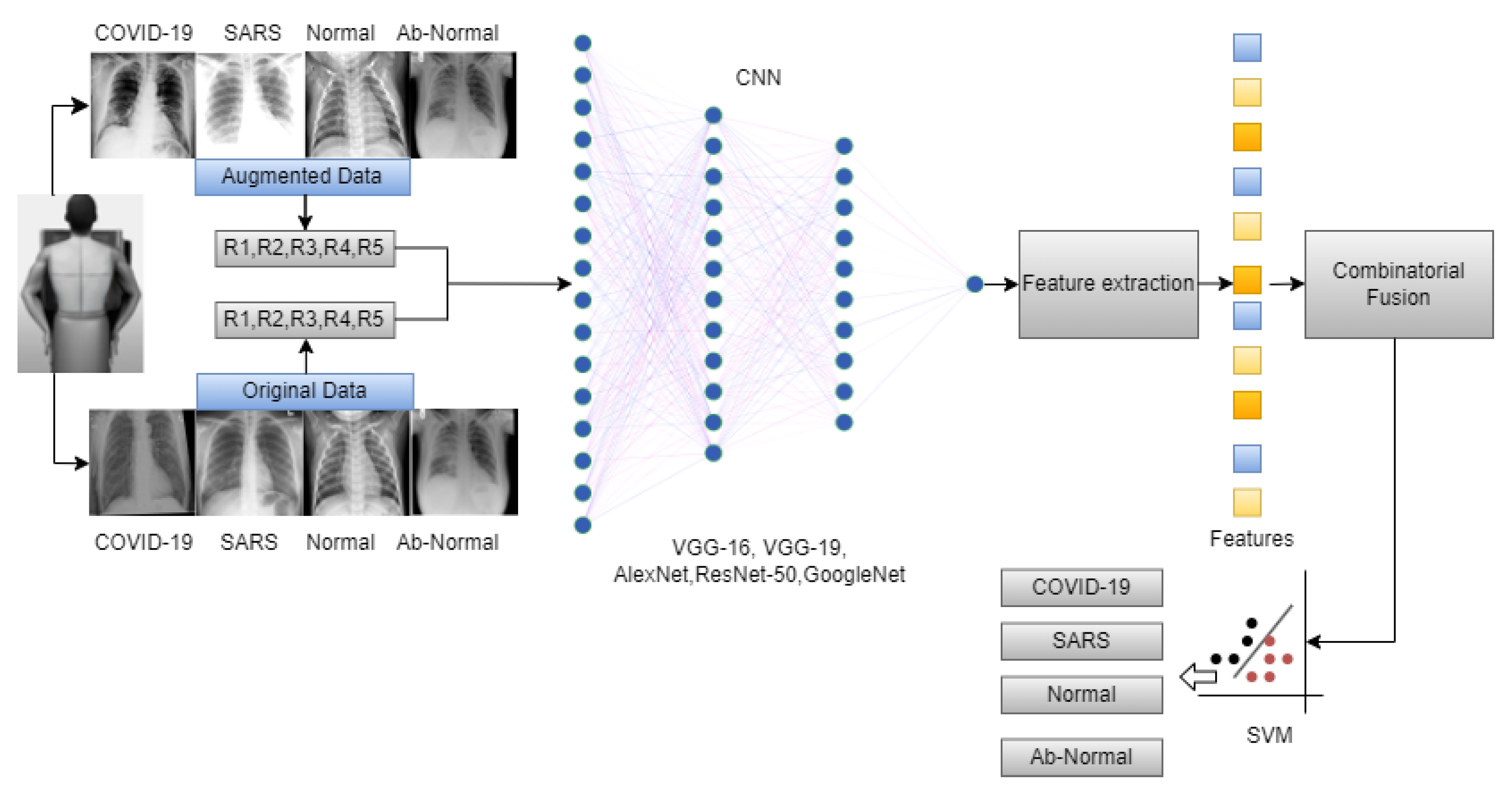
3.4. Deep Learning CNN Model Selection
3.5. VGG-16
3.6. VGG-19
3.7. AlexNet
3.8. ResNet-50
3.9. GoogleNet
4. Materials and Methods
Combinatorial Fusion
5. Performance and Evaluation Matrix
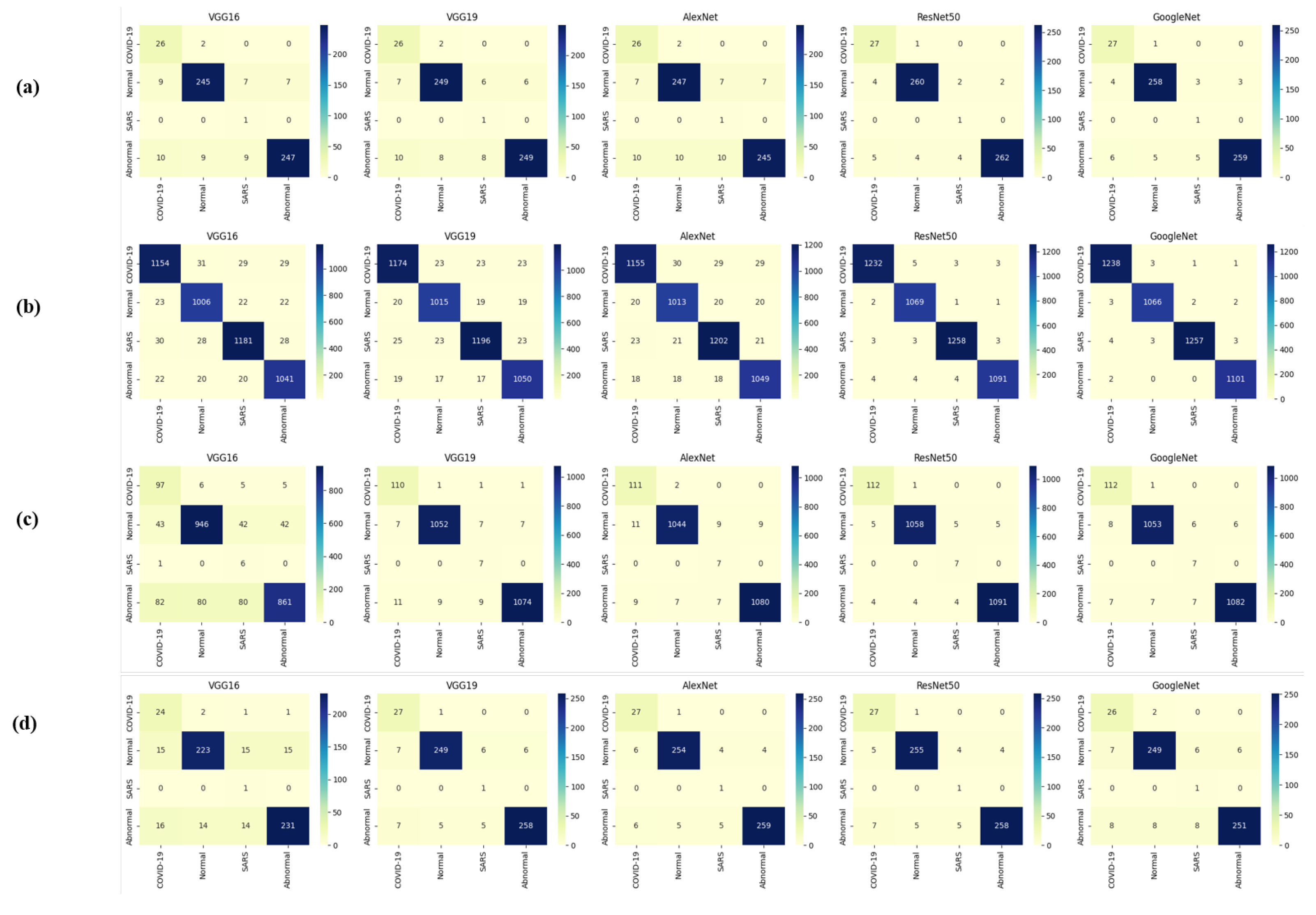
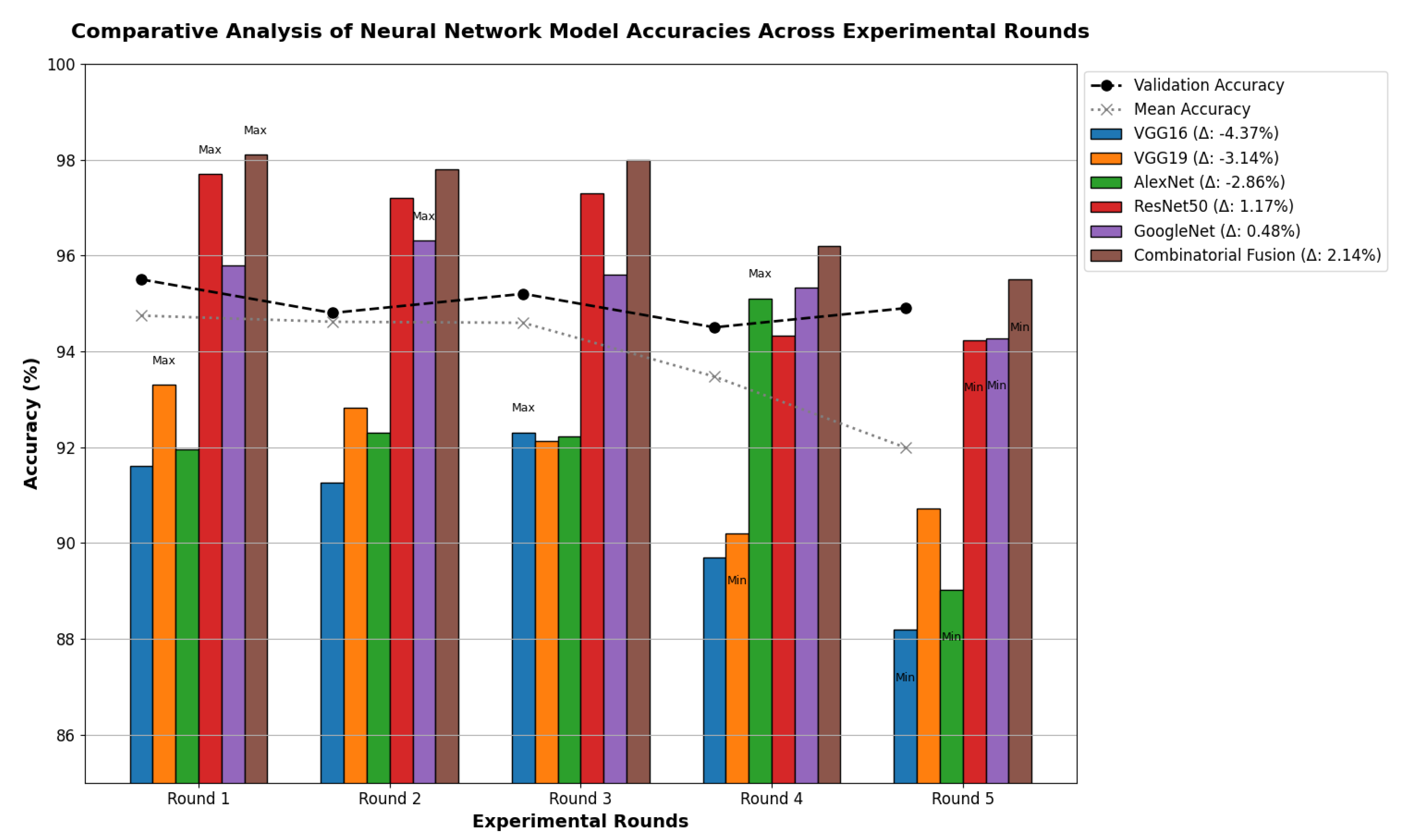
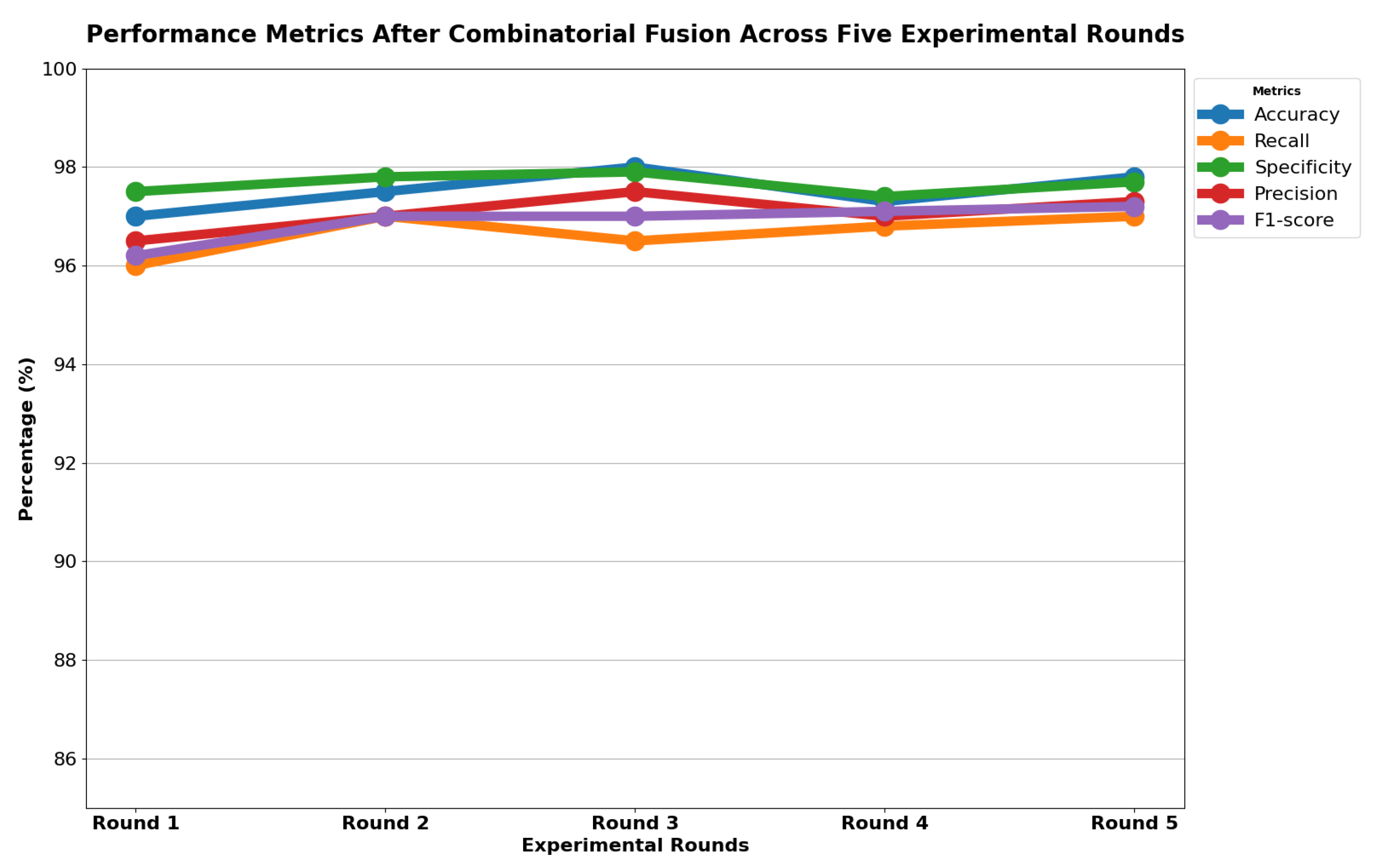
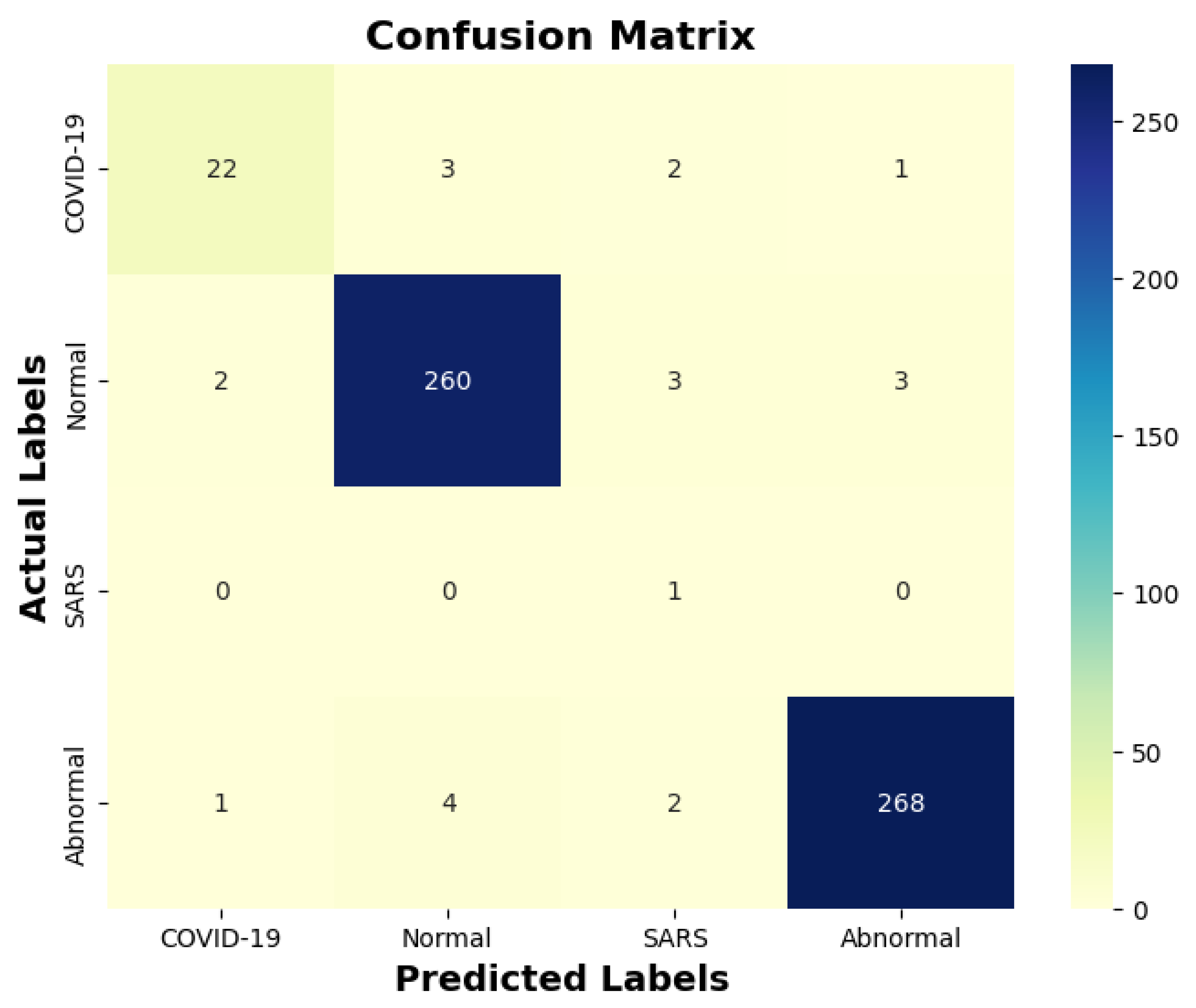
6. Results
6.1. Discussion
6.2. Comparison
6.3. Limitations and Future Recommendations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ulinici, M.; Covantev, S.; Wingfield-Digby, J.; Beloukas, A.; Mathioudakis, A.G.; Corlateanu, A. Screening, diagnostic and prognostic tests for COVID-19: A comprehensive review. Life 2021, 11, 561. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, A.; Sam, I.C.; Ong, Y.J.; Theo, C.H.; Pukhari, M.H.; Chan, Y.F. Comparative Evaluation of a Standard M10 Assay with Xpert Xpress for the Rapid Molecular Diagnosis of SARS-CoV-2, Influenza A/B Virus, and Respiratory Syncytial Virus. Diagnostics 2023, 13, 3507. [Google Scholar] [CrossRef]
- Lassmann, S.; Bauer, M.; Soong, R.; Schreglmann, J.; Tabiti, K.; Nährig, J.; Rüger, R.; Höfler, H.; Werner, M. Quantification of CK20 gene and protein expression in colorectal cancer by RT-PCR and immunohistochemistry reveals inter-and intratumour heterogeneity. J. Pathol. 2002, 198, 198–206. [Google Scholar] [CrossRef]
- Yin, Z.; Kang, Z.; Yang, D.; Ding, S.; Luo, H.; Xiao, E. A comparison of clinical and chest CT findings in patients with influenza A (H1N1) virus infection and coronavirus disease (COVID-19). Am. J. Roentgenol. 2020, 215, 1065–1071. [Google Scholar] [CrossRef]
- Jaegere, T.M.H.D.; Krdzalic, J.; Fasen, B.A.C.M.; Kwee, R.M.; COVID-19 CT Investigators South-East Netherlands (CISEN) Study Group. Radiological Society of North America chest CT classification system for reporting COVID-19 pneumonia: Interobserver variability and correlation with reverse-transcription polymerase chain reaction. Radiol. Cardiothorac. Imaging 2020, 2, e200213. [Google Scholar] [CrossRef] [PubMed]
- Pasa, F.; Golkov, V.; Pfeiffer, F.; Cremers, D.; Pfeiffer, D. Efficient deep network architectures for fast chest X-ray tuberculosis screening and visualization. Sci. Rep. 2019, 9, 6268. [Google Scholar] [CrossRef] [PubMed]
- Shah, F.M.; Joy, S.K.S.; Ahmed, F.; Hossain, T.; Humaira, M.; Ami, A.S.; Paul, S.; Jim, M.A.R.K.; Ahmed, S. A comprehensive survey of COVID-19 detection using medical images. SN Comput. Sci. 2021, 2, 434. [Google Scholar] [CrossRef]
- Shkolyar, E.; Jia, X.; Chang, T.C.; Trivedi, D.; Mach, K.E.; Meng, M.Q.H.; Xing, L.; Liao, J.C. Augmented bladder tumor detection using deep learning. Eur. Urol. 2019, 76, 714–718. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, M.; Based, M.A.; Haider, J.; Kowalski, M. COVID-19 detection from chest X-ray images using feature fusion and deep learning. Sensors 2021, 21, 1480. [Google Scholar]
- Kumar, A.; Vashishtha, G.; Gandhi, C.P.; Zhou, Y.; Glowacz, A.; Xiang, J. Novel convolutional neural network (NCNN) for the diagnosis of bearing defects in rotary machinery. IEEE Trans. Instrum. Meas. 2021, 70, 3510710. [Google Scholar] [CrossRef]
- Sevi, M.; Aydin, İ. COVID-19 Detection Using Deep Learning Methods. In Proceedings of the 2020 International Conference on Data Analytics for Business and Industry: Way Towards a Sustainable Economy (ICDABI), Sakheer, Bahrain, 26–27 October 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Mahmud, T.; Rahman, M.A.; Fattah, S.A. CovXNet: A multi-dilation convolutional neural network for automatic COVID-19 and other pneumonia detection from chest X-ray images with transferable multi-receptive feature optimization. Comput. Biol. Med. 2020, 122, 103869. [Google Scholar] [CrossRef]
- Gupta, A.; Gupta, S.; Katarya, R. InstaCovNet-19: A deep learning classification model for the detection of COVID-19 patients using Chest X-ray. Appl. Soft Comput. 2021, 99, 106859. [Google Scholar] [CrossRef]
- Fusco, R.; Grassi, R.; Granata, V.; Setola, S.V.; Grassi, F.; Cozzi, D.; Pecori, B.; Izzo, F.; Petrillo, A. Artificial intelligence and COVID-19 using chest CT scan and chest X-ray images: Machine learning and deep learning approaches for diagnosis and treatment. J. Pers. Med. 2021, 11, 993. [Google Scholar] [CrossRef]
- Jebril, N. World Health Organization Declared a Pandemic Public Health Menace: A Systematic Review of the Coronavirus Disease 2019 “COVID-19”. Available online: https://ssrn.com/abstract=3566298 (accessed on 1 April 2020).
- Ranjan, A.; Kumar, C.; Gupta, R.K.; Misra, R. Transfer Learning Based Approach for Pneumonia Detection Using Customized VGG16 Deep Learning Model. In Internet of Things and Connected Technologies; Misra, R., Kesswani, N., Rajarajan, M., Veeravalli, B., Patel, A., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 17–28. [Google Scholar]
- Yang, T.; Wang, Y.C.; Shen, C.F.; Cheng, C.M. Point-of-care RNA-based diagnostic device for COVID-19. Diagnostics 2020, 10, 165. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. arXiv 2015, arXiv:1505.04597. [Google Scholar]
- Rajpurkar, P.; Irvin, J.; Ball, R.L.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.P.; et al. Deep learning for chest radiograph diagnosis: A retrospective comparison of the CheXNeXt algorithm to practicing radiologists. PLoS Med. 2018, 15, e1002686. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, P.; Sundaram, B. Deep learning at chest radiography: Automated classification of pulmonary tuberculosis by using convolutional neural networks. Radiology 2017, 284, 574–582. [Google Scholar] [CrossRef]
- Afshar, P.; Heidarian, S.; Naderkhani, F.; Oikonomou, A.; Plataniotis, K.N.; Mohammadi, A. Covid-caps: A capsule network-based framework for identification of COVID-19 cases from X-ray images. Pattern Recognit. Lett. 2020, 138, 638–643. [Google Scholar] [CrossRef]
- Abbas, A.; Abdelsamea, M.M.; Gaber, M.M. Classification of COVID-19 in chest X-ray images using DeTraC deep convolutional neural network. Appl. Intell. 2021, 51, 854–864. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Lin, Z.Q.; Wong, A. Covid-net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci. Rep. 2020, 10, 19549. [Google Scholar] [CrossRef] [PubMed]
- Ucar, F.; Korkmaz, D. COVIDiagnosis-Net: Deep Bayes-SqueezeNet based diagnosis of the coronavirus disease 2019 (COVID-19) from X-ray images. Med. Hypotheses 2020, 140, 109761. [Google Scholar] [CrossRef]
- Khan, A.I.; Shah, J.L.; Bhat, M.M. CoroNet: A deep neural network for detection and diagnosis of COVID-19 from chest X-ray images. Comput. Methods Programs Biomed. 2020, 196, 105581. [Google Scholar] [CrossRef]
- Zammit, S.C.; Sidhu, R. Capsule Endoscopy–Recent Developments and Future Directions. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Kesim, E.; Dokur, Z.; Olmez, T. X-ray Chest Image Classification by A Small-Sized Convolutional Neural Network. In Proceedings of the 2019 Scientific Meeting on Electrical-Electronics & Biomedical Engineering and Computer Science (EBBT), Istanbul, Turkey, 24–26 April 2019; pp. 1–5. [Google Scholar]
- Demir, F.; Ismael, A.M.; Sengur, A. Classification of Lung Sounds with CNN Model Using Parallel Pooling Structure. IEEE Access 2020, 8, 105376–105383. [Google Scholar] [CrossRef]
- Park, S.; Kim, G.; Oh, Y.; Seo, J.B.; Lee, S.M.; Kim, J.H.; Moon, S.; Lim, J.K.; Ye, J.C. Multi-task vision transformer using low-level chest X-ray feature corpus for COVID-19 diagnosis and severity quantification. Med. Image Anal. 2022, 75, 102299. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Lu, S.; Wang, S.H.; Yu, X.; Wang, S.J.; Yao, L.; Pan, Y.; Zhang, Y.D. Diagnosis of COVID-19 Pneumonia via a Novel Deep Learning Architecture. J. Comput. Sci. Technol. 2022, 37, 330–343. [Google Scholar] [CrossRef] [PubMed]
- Makris, A.; Kontopoulos, I.; Tserpes, K. COVID-19 detection from chest X-ray images using Deep Learning and Convolutional Neural Networks. In Proceedings of the 11th Hellenic Conference on Artificial Intelligence, Athens, Greece, 2–4 September 2020; pp. 60–66. [Google Scholar]
- Pereira, R.M.; Bertolini, D.; Teixeira, L.O.; Silla, C.N., Jr.; Costa, Y.M.G. COVID-19 identification in chest X-ray images on flat and hierarchical classification scenarios. Comput. Methods Programs Biomed. 2020, 194, 105532. [Google Scholar] [CrossRef] [PubMed]
- Dey, A.; Chattopadhyay, S.; Singh, P.K.; Ahmadian, A.; Ferrara, M.; Senu, N.; Sarkar, R. MRFGRO: A hybrid meta-heuristic feature selection method for screening COVID-19 using deep features. Sci. Rep. 2021, 11, 24065. [Google Scholar] [CrossRef]
- Basha, S.H.; Farazuddin, M.; Pulabaigari, V.; Dubey, S.R.; Mukherjee, S. Deep Model Compression Based on the Training History. arXiv 2021, arXiv:2102.00160. [Google Scholar] [CrossRef]
- Geng, L.; Zhang, S.; Tong, J.; Xiao, Z. Lung Segmentation Method with Dilated Convolution Based on VGG-16 Network. Comput. Assist. Surg. 2019, 24, 27–33. [Google Scholar] [CrossRef]
- Bagaskara, A.; Suryanegara, M. Evaluation of VGG-16 and VGG-19 Deep Learning Architecture for Classifying Dementia People. In Proceedings of the 2021 4th International Conference of Computer and Informatics Engineering (IC2IE), Depok, Indonesia, 14–15 September 2021; pp. 1–4. [Google Scholar]
- Mohammadi, R.; Salehi, M.; Ghaffari, H.; Reiazi, R. Transfer Learning-Based Automatic Detection of Coronavirus Disease 2019 (COVID-19) from Chest X-ray Images. J. Biomed. Phys. Eng. 2020, 10, 559. [Google Scholar] [CrossRef]
- Alom, M.Z.; Taha, T.M.; Yakopcic, C.; Westberg, S.; Sidike, P.; Nasrin, M.S.; Van Esesn, B.C.; Awwal, A.A.S.; Asari, V.K. The history began from alexnet: A comprehensive survey on deep learning approaches. arXiv 2018, arXiv:1803.01164. [Google Scholar]
- Reddy, A.S.B.; Juliet, D.S. Transfer Learning with ResNet-50 for Malaria Cell-Image Classification. In Proceedings of the 2019 International Conference on Communication and Signal Processing (ICCSP), Chennai, India, 4–6 April 2019; pp. 0945–0949. [Google Scholar]
- Al-Haija, Q.A.; Adebanjo, A. Breast Cancer Diagnosis in Histopathological Images Using ResNet-50 Convolutional Neural Network. In Proceedings of the 2020 IEEE International IOT, Electronics and Mechatronics Conference (IEMTRONICS), Vancouver, BC, Canada, 9–12 September 2020; pp. 1–7. [Google Scholar]
- Anand, R.; Shanthi, T.; Nithish, M.S.; Lakshman, S. Face Recognition and Classification Using GoogleNET Architecture. In Soft Computing for Problem Solving; Springer: Berlin/Heidelberg, Germany, 2020; pp. 261–269. [Google Scholar]
- Foo, P.H.; Ng, G.W. High-level information fusion: An overview. J. Adv. Inf. Fusion 2013, 8, 33–72. [Google Scholar]
- Mohandes, M.; Deriche, M.; Aliyu, S.O. Classifiers combination techniques: A comprehensive review. IEEE Access 2018, 6, 19626–19639. [Google Scholar] [CrossRef]
- Gu, Q.; Han, J. Clustered support vector machines. In Proceedings of the 16th International Conference on Artificial Intelligence and Statistics (AISTATS), Scottsdale, AZ, USA, 29 April–1 May 2013; pp. 307–315. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No | Papers | Deep Learning Classifier | Diseases | Accuracy % |
|---|---|---|---|---|
| 1 | Asmaa Abbas [22] | DeTraC (Decompose, Transfer and Compose) | COVID-19 | 95.12% |
| 2 | Kesim and Dokur [27] | New CNN model | COVID-19 | 86% |
| 3 | Aras. M. Ismael [28] | Resnet-18, Resnet-50, Resnet-101, VGG-16, VGG-19 | COVID-19 and Normal | 94% |
| 4 | Yujin Oh [29] | New CNN Model based on ResNet -18 | Normal, Pneumonia, COVID-19 | 76.9% |
| 5 | Zhang [30] | Resnet-18 | COVID-19 and non-COVID-19 | 95.18% |
| Rounds | Classes | Training | Total Training | Testing | Total Testing | Training + Testing | Total Images |
|---|---|---|---|---|---|---|---|
| Round-1 | COVID-19 Normal SARS Abnormal | 113 1073 7 1103 | 2296 | 28 268 1 275 | 572 | 141 1341 8 1378 | 2868 |
| Round-2 | COVID-19 Normal SARS Abnormal | 113 1073 7 1103 | 2296 | 28 268 1 275 | 572 | 141 1341 8 1378 | 2868 |
| Round-3 | COVID-19 Normal SARS Abnormal | 113 1073 7 1103 | 2296 | 28 268 1 275 | 572 | 141 1341 8 1378 | 2868 |
| Round-4 | COVID-19 Normal SARS Abnormal | 113 1073 7 1103 | 2296 | 28 268 1 275 | 572 | 141 1341 8 1378 | 2868 |
| Round-5 | COVID-19 Normal SARS Abnormal | 113 1073 7 1103 | 2296 | 28 268 1 275 | 572 | 141 1341 8 1378 | 2868 |
| Rounds | Classes | Training | Total Training | Testing | Total Testing | Training + Testing | Total Images |
|---|---|---|---|---|---|---|---|
| Round-1 | COVID-19 Normal SARS Abnormal | 1243 1073 1267 1103 | 4686 | 28 268 1 275 | 572 | 1271 1341 1268 1378 | 5258 |
| Round-2 | COVID-19 Normal SARS Abnormal | 1243 1073 1267 1103 | 4686 | 28 268 1 275 | 572 | 1271 1341 1268 1378 | 5258 |
| Round-3 | COVID-19 Normal SARS Abnormal | 1243 1073 1267 1103 | 4686 | 28 268 1 275 | 572 | 1271 1341 1268 1378 | 5258 |
| Round-4 | COVID-19 Normal SARS Abnormal | 1243 1073 1267 1103 | 4686 | 28 268 1 275 | 572 | 1271 1341 1268 1378 | 5258 |
| Round-5 | COVID-19 Normal SARS Abnormal | 1243 1073 1267 1103 | 4686 | 28 268 1 275 | 572 | 1271 1341 1268 1378 | 5258 |
| Models | Size (M) | Layers | Model Description |
|---|---|---|---|
| VGG 16 | 520 | 16 | 13 conv + 3 fc layers |
| VGG 19 | 560 | 19 | 16 conv + 3 fc layers |
| ResNet 50 | 235 | 50 | 49 conv + 1 fc layers |
| GoogleNet | 40 | 22 | 21 conv + 1 fc layers |
| AlexNet | 238 | 8 | 5 conv + 3 fc layers |
| Metric | Fold | VGG16 | VGG19 | AlexNet | ResNet50 | GoogleNet |
|---|---|---|---|---|---|---|
| Accuracy (%) | 1 | 90.5 | 92.3 | 91.0 | 95.2 | 94.8 |
| 2 | 89.7 | 91.8 | 90.4 | 94.6 | 94.1 | |
| 3 | 90.2 | 92.1 | 91.2 | 95.4 | 94.5 | |
| 4 | 89.9 | 91.5 | 90.7 | 94.9 | 94.3 | |
| 5 | 90.0 | 92.0 | 90.9 | 95.1 | 94.4 | |
| Precision (%) | 1 | 87.6 | 89.9 | 88.4 | 92.7 | 91.9 |
| 2 | 86.8 | 89.4 | 87.9 | 92.2 | 91.5 | |
| 3 | 87.2 | 89.7 | 88.1 | 92.9 | 91.8 | |
| 4 | 87.0 | 89.2 | 88.0 | 92.6 | 91.6 | |
| 5 | 87.1 | 89.6 | 88.2 | 92.8 | 91.7 | |
| Recall (%) | 1 | 86.5 | 88.7 | 87.3 | 91.8 | 91.1 |
| 2 | 85.7 | 88.2 | 86.8 | 91.3 | 90.7 | |
| 3 | 86.1 | 88.5 | 87.0 | 91.6 | 91.0 | |
| 4 | 85.9 | 88.0 | 86.9 | 91.4 | 90.8 | |
| 5 | 86.0 | 88.4 | 87.1 | 91.5 | 90.9 | |
| F1-Score (%) | 1 | 87.0 | 89.3 | 87.8 | 92.2 | 91.5 |
| 2 | 86.2 | 88.8 | 87.3 | 91.7 | 91.1 | |
| 3 | 86.6 | 89.1 | 87.5 | 92.2 | 91.4 | |
| 4 | 86.4 | 88.6 | 87.4 | 92.0 | 91.2 | |
| 5 | 86.5 | 89.0 | 87.6 | 92.1 | 91.3 |
| Model | Round 1 | Round 2 | Round 3 | Round 4 | Round 5 | Avg. |
|---|---|---|---|---|---|---|
| VGG 16 | 86.12 | 88.12 | 84.1 | 87.12 | 78.1 | 84.71 |
| VGG19 | 97.72 | 98 | 97.1 | 97.4 | 97.57 | 97.55 |
| AlexNet | 98.01 | 97.32 | 96.48 | 97.8 | 97.92 | 97.5 |
| ResNet50 | 99.7 | 98.82 | 99.04 | 98.68 | 98.95 | 99.03 |
| GoogleNet | 98.84 | 98.18 | 98.95 | 98.02 | 98.08 | 98.41 |
| Model | Round 1 | Round 2 | Round 3 | Round 4 | Round 5 | Avg. |
|---|---|---|---|---|---|---|
| VGG16 | 92.81 | 93.73 | 93.24 | 94.34 | 93.9 | 93.60 |
| VGG19 | 94.41 | 94.58 | 94.37 | 95.33 | 94.9 | 94.71 |
| AlexNet | 92.92 | 94.44 | 94.87 | 95.1 | 94.72 | 94.40 |
| ResNet50 | 99.14 | 99.66 | 98.3 | 99.25 | 99.15 | 99.10 |
| GoogleNet | 99.35 | 99.58 | 99.33 | 99.11 | 99.79 | 99.43 |
| Model | Round 1 | Round 2 | Round 3 | Round 4 | Round 5 | Avg. |
|---|---|---|---|---|---|---|
| VGG 16 | 0.4164 | 0.4974 | 0.5742 | 0.5612 | 0.5774 | 0.5253 |
| VGG19 | 0.1163 | 0.1118 | 0.1276 | 0.1164 | 0.1194 | 0.1183 |
| AlexNet | 0.183 | 0.1566 | 0.149 | 0.1436 | 0.1511 | 0.1566 |
| ResNet50 | 0.0182 | 0.106 | 0.0392 | 0.069 | 0.035 | 0.08624 |
| GoogleNet | 0.084 | 0.089 | 0.0478 | 0.0492 | 0.0227 | 0.05854 |
| Model | Round 1 | Round 2 | Round 3 | Round 4 | Round 5 | Avg. |
|---|---|---|---|---|---|---|
| VGG 16 | 0.1861 | 0.1785 | 0.1828 | 0.1717 | 0.1476 | 0.1733 |
| VGG19 | 0.1557 | 0.1527 | 0.154 | 0.1336 | 0.1448 | 0.1481 |
| AlexNet | 0.1839 | 0.1557 | 0.149 | 0.1436 | 0.1442 | 0.1552 |
| ResNet50 | 0.0117 | 0.0016 | 0.0104 | 0.035 | 0.0284 | 0.0174 |
| GoogleNet | 0.0162 | 0.0557 | 0.049 | 0.0386 | 0.0391 | 0.0397 |
| Model | Round 1 | Round 2 | Round 3 | Round 4 | Round 5 | Avg. |
|---|---|---|---|---|---|---|
| VGG 16 | 87.45 | 88.02 | 84.03 | 87.02 | 83.03 | 85.91 |
| VGG19 | 95.2 | 93.2 | 94.8 | 93.91 | 92.88 | 93.99 |
| AlexNet | 95.9 | 95.27 | 94.75 | 73.21 | 94.01 | 90.62 |
| ResNet50 | 97.19 | 95.07 | 96.67 | 96.42 | 94.00 | 95.87 |
| GoogleNet | 94.62 | 95.01 | 92.6 | 94.43 | 91.41 | 93.61 |
| Model | Round 1 | Round 2 | Round 3 | Round 4 | Round 5 | Avg. |
|---|---|---|---|---|---|---|
| VGG16 | 91.61 | 91.26 | 92.31 | 89.69 | 88.19 | 90.61 |
| VGG19 | 93.3 | 92.83 | 92.13 | 90.21 | 90.73 | 91.84 |
| AlexNet | 91.96 | 92.3 | 92.23 | 95.1 | 89.03 | 92.12 |
| ResNet50 | 97.7 | 97.2 | 97.3 | 94.32 | 94.23 | 96.15 |
| GoogleNet | 95.8 | 96.31 | 95.6 | 95.32 | 94.27 | 95.46 |
| Model | Round 1 | Round 2 | Round 3 | Round 4 | Round 5 | Avg. |
|---|---|---|---|---|---|---|
| VGG16 | 0.3028 | 0.3951 | 0.4044 | 0.3951 | 0.3951 | 0.3787 |
| VGG 19 | 0.1476 | 0.1412 | 0.1872 | 0.1923 | 0.2363 | 0.1809 |
| AlexNet | 0.5273 | 0.6644 | 0.6786 | 0.895 | 0.6612 | 0.6853 |
| ResNet50 | 0.1567 | 0.1196 | 0.279 | 0.202 | 0.2895 | 0.2093 |
| GoogleNet | 0.198 | 0.2211 | 0.3821 | 0.222 | 0.483 | 0.3014 |
| Model | Round 1 | Round 2 | Round 3 | Round 4 | Round 5 | Avg. |
|---|---|---|---|---|---|---|
| VGG16 | 0.2382 | 0.223 | 0.2532 | 0.2901 | 0.2576 | 0.2524 |
| VGG 19 | 0.2016 | 0.2053 | 0.2025 | 0.2401 | 0.2579 | 0.2214 |
| AlexNet | 0.2294 | 0.2016 | 0.2011 | 0.2501 | 0.2579 | 0.228 |
| ResNet50 | 0.1424 | 0.1196 | 0.1869 | 0.3795 | 0.2895 | 0.2235 |
| GoogleNet | 0.2101 | 0.2216 | 0.2991 | 0.3101 | 0.713 | 0.3507 |
| Models | Recall (%) | Specificity (%) | Precision (%) | F1-Score (%) |
|---|---|---|---|---|
| VGG 16 | 87.05 | 92.02 | 91.11 | 92.60 |
| VGG 19 | 94.11 | 95.05 | 96.51 | 97.20 |
| AlexNet | 93.12 | 89.32 | 94.10 | 89.02 |
| ResNet50 | 97.34 | 90.73 | 98.20 | 94.40 |
| GoogleNet | 98.34 | 99.01 | 99.51 | 99.21 |
| Models | Recall (%) | Specificity (%) | Precision (%) | F1-Score (%) |
|---|---|---|---|---|
| VGG 16 | 84.02 | 86.1 | 86.02 | 84.7 |
| VGG 19 | 95.12 | 96.02 | 97.41 | 95.61 |
| AlexNet | 94.08 | 85.8 | 90.12 | 83.12 |
| ResNet50 | 95.04 | 81.02 | 88.92 | 85.14 |
| GoogleNet | 94.02 | 96.33 | 94.71 | 93.89 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, C.-T.; Kumar, R.; Wen, Z.-H.; Wang, C.-H.; Chang, C.-Y.; Shiue, Y.-L. Improving Respiratory Infection Diagnosis with Deep Learning and Combinatorial Fusion: A Two-Stage Approach Using Chest X-ray Imaging. Diagnostics 2024, 14, 500. https://doi.org/10.3390/diagnostics14050500
Pan C-T, Kumar R, Wen Z-H, Wang C-H, Chang C-Y, Shiue Y-L. Improving Respiratory Infection Diagnosis with Deep Learning and Combinatorial Fusion: A Two-Stage Approach Using Chest X-ray Imaging. Diagnostics. 2024; 14(5):500. https://doi.org/10.3390/diagnostics14050500
Chicago/Turabian StylePan, Cheng-Tang, Rahul Kumar, Zhi-Hong Wen, Chih-Hsuan Wang, Chun-Yung Chang, and Yow-Ling Shiue. 2024. "Improving Respiratory Infection Diagnosis with Deep Learning and Combinatorial Fusion: A Two-Stage Approach Using Chest X-ray Imaging" Diagnostics 14, no. 5: 500. https://doi.org/10.3390/diagnostics14050500