
The Use of Artificial Intelligence in the Liver Histopathology Field: A Systematic Review
 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
1.1. Artificial Intelligence in Medicine
1.2. AI Applications on Histological Images
1.3. Aim
2. Methods
2.1. Search Strategy
2.2. Search Criteria
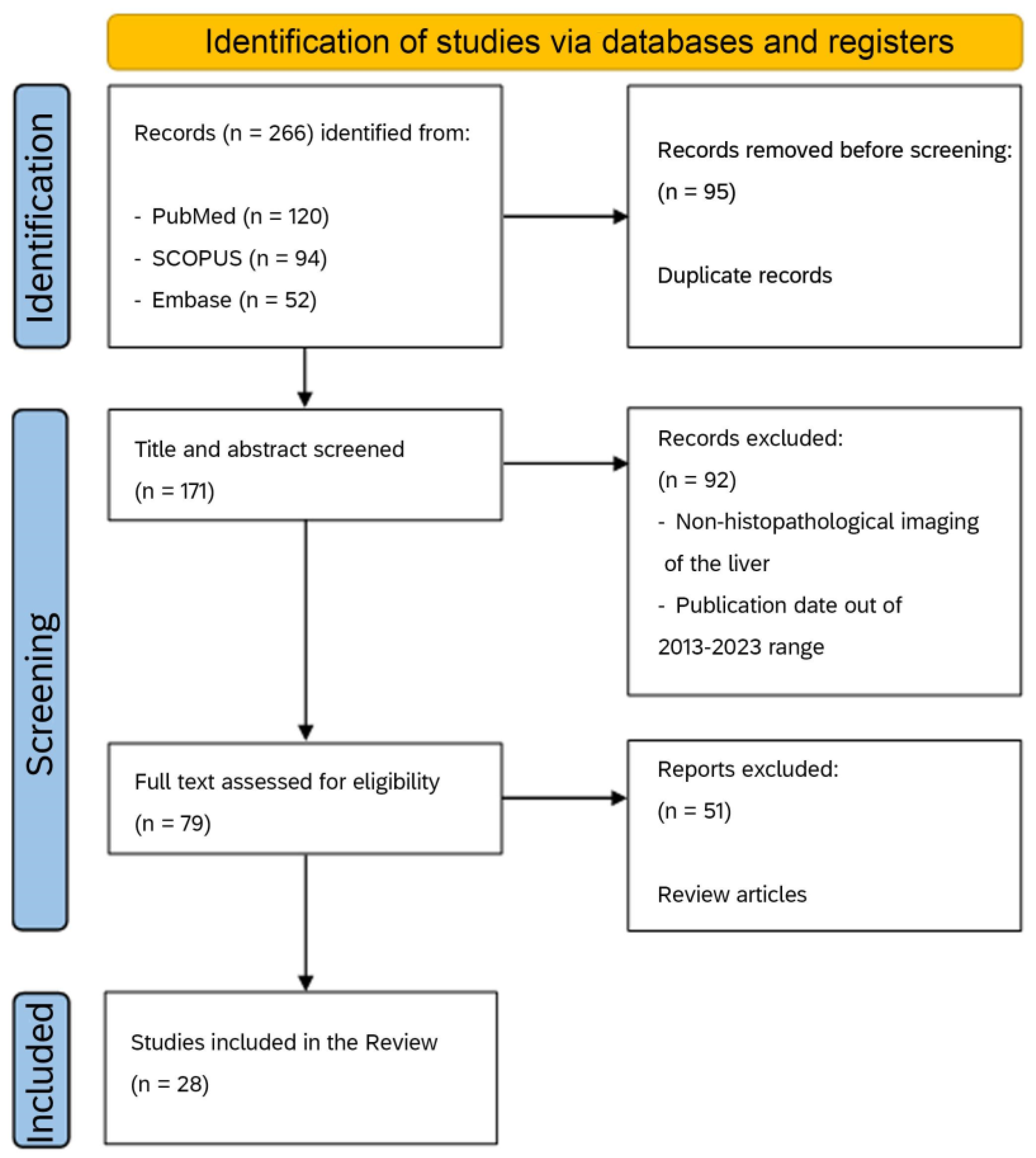
2.3. Screening and Article Selection
2.4. Data Extraction
3. Results
3.1. Search Results
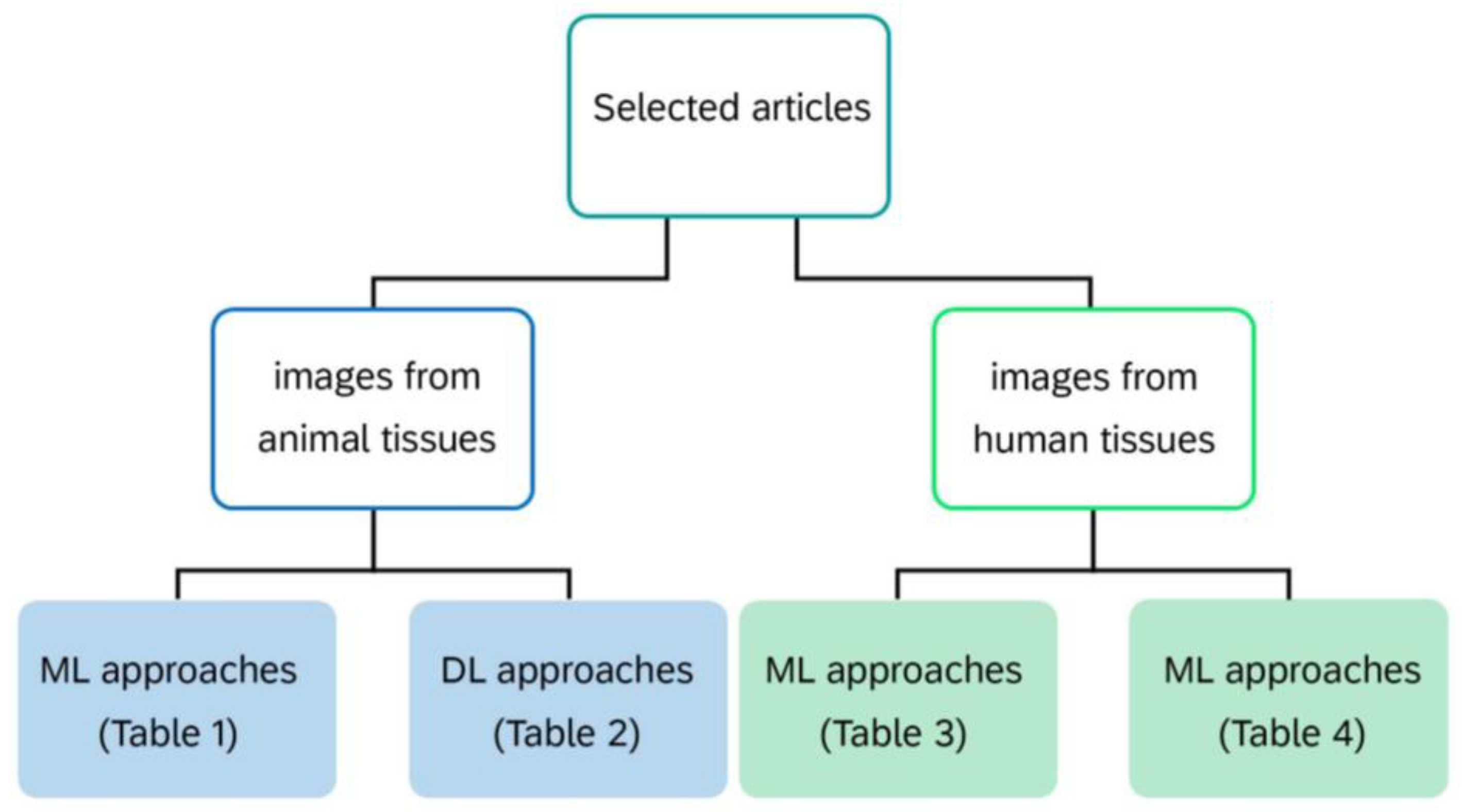
3.2. Results Organization
3.3. Studies Conducted on Animal Tissues
3.3.1. ML Approaches on Animal Tissues
3.3.2. DL Approaches on Animal Tissues
3.4. Studies Conducted on Human Tissues
3.4.1. ML Approaches on Human Tissues
3.4.2. DL Approaches on Human Tissues
4. Discussion
4.1. State-of-the-Art
4.2. Qualitative Analysis
4.3. Generalizability
4.4. Overall Bias in the Selected Articles
4.5. Limits of DP
4.6. Present Review Limitation
4.7. Future Directions of AI Approaches in Liver Diseases
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malik, P.; Pathania, M.; Rathaur, V.K. Overview of artificial intelligence in medicine. J. Fam. Med. Prim. Care 2019, 8, 2328–2331. [Google Scholar] [CrossRef]
- Kaul, V.; Enslin, S.; Gross, S.A. History of artificial intelligence in medicine. Gastrointest. Endosc. 2020, 92, 807–812. [Google Scholar] [CrossRef]
- Ramesh, A.N.; Kambhampati, C.; Monson, J.R.; Drew, P.J. Artificial intelligence in medicine. Ann. R. Coll. Surg. Engl. 2004, 86, 334–338. [Google Scholar] [CrossRef]
- Rosenfeld, A. Computer vision: Basic principles. Proc. IEEE 1988, 76, 863–868. [Google Scholar] [CrossRef]
- Qin, C.; Yao, D.; Shi, Y.; Song, Z. Computer-aided detection in chest radiography based on artificial intelligence: A survey. Biomed. Eng. Online 2018, 17, 113. [Google Scholar] [CrossRef]
- Putra, R.H.; Doi, C.; Yoda, N.; Astuti, E.R.; Sasaki, K. Current applications and development of artificial intelligence for digital dental radiography. Dentomaxillofac Radiol. 2022, 51, 20210197. [Google Scholar] [CrossRef]
- Hardy, M.; Harvey, H. Artificial intelligence in diagnostic imaging: Impact on the radiography profession. Br. J. Radiol. 2020, 93, 20190840. [Google Scholar] [CrossRef]
- Shen, Y.T.; Chen, L.; Yue, W.W.; Xu, H.X. Artificial intelligence in ultrasound. Eur. J. Radiol. 2021, 139, 109717. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, M.; Sakai, A.; Dozen, A.; Shozu, K.; Yasutomi, S.; Machino, H.; Asada, K.; Kaneko, S.; Hamamoto, R. Towards Clinical Application of Artificial Intelligence in Ultrasound Imaging. Biomedicines 2021, 9, 720. [Google Scholar] [CrossRef] [PubMed]
- Akkus, Z.; Cai, J.; Boonrod, A.; Zeinoddini, A.; Weston, A.D.; Philbrick, K.A.; Erickson, B.J. A survey of deep-learning applications in ultrasound: Artificial intelligence–powered ultrasound for improving clinical workflow. J. Am. Coll. Radiol. 2019, 16, 1318–1328. [Google Scholar] [CrossRef]
- Wang, B.; Liu, M.; Zhu, M.; Eisenbrey, J. Artificial intelligence in ultrasound imaging: Current research and applications. Dep. Radiol. Fac. Pap. 2019, 75, 53–61. [Google Scholar] [CrossRef]
- Wong, D.J.; Gandomkar, Z.; Wu, W.J.; Zhang, G.; Gao, W.; He, X.; Wang, Y.; Reed, W. Artificial intelligence and convolution neural networks assessing mammographic images: A narrative literature review. J. Med. Radiat. Sci. 2020, 67, 134–142. [Google Scholar] [CrossRef]
- Yoon, J.H.; Kim, E.K. Deep learning-based artificial intelligence for mammography. Korean J. Radiol. 2021, 22, 1225–1239. [Google Scholar] [CrossRef] [PubMed]
- Vyborny, C.J.; Giger, M.L. Computer vision and artificial intelligence in mammography. AJR Am. J. Roentgenol. 1994, 162, 699–708. [Google Scholar] [CrossRef]
- Geras, K.J.; Mann, R.M.; Moy, L. Artificial intelligence for mammography and digital breast tomosynthesis: Current concepts and future perspectives. Radiology 2019, 293, 246–259. [Google Scholar] [CrossRef] [PubMed]
- Faiella, E.; Santucci, D.; Calabrese, A.; Russo, F.; Vadalà, G.; Zobel, B.B.; Soda, P.; Iannello, G.; de Felice, C.; Denaro, V. Artificial Intelligence in Bone Metastases: An MRI and CT Imaging Review. Int. J. Environ. Res. Public Health 2022, 19, 1880. [Google Scholar] [CrossRef]
- Zhang, Z.; Seeram, E. The use of artificial intelligence in computed tomography image reconstruction-a literature review. J. Med. Imaging Radiat. Sci. 2020, 51, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.; Kolossváry, M.; Motwani, M.; Išgum, I.; Maurovich-Horvat, P.; Slomka, P.J.; Dey, D. Artificial intelligence in cardiovascular CT: Current status and future implications. J. Cardiovasc. Comput. Tomogr. 2021, 15, 462–469. [Google Scholar] [CrossRef]
- Brossard, C.; Lemasson, B.; Attyé, A.; De Busschère, J.A.; Payen, J.F.; Barbier, E.L.; Grèze, J.; Bouzat, P. Contribution of CT-scan analysis by artificial intelligence to the clinical care of TBI patients. Front. Neurol. 2021, 12, 666875. [Google Scholar] [CrossRef]
- Lin, D.J.; Johnson, P.M.; Knoll, F.; Lui, Y.W. Artificial intelligence for MR image reconstruction: An overview for clinicians. J. Magn. Reson. Imaging 2021, 53, 1015–1028. [Google Scholar] [CrossRef]
- Zhao, X.; Ang, C.K.E.; Acharya, U.R.; Cheong, K.H. Application of Artificial Intelligence techniques for the detection of Alzheimer’s disease using structural MRI images. Biocybern. Biomed. Eng. 2021, 41, 456–473. [Google Scholar] [CrossRef]
- Ranjbarzadeh, R.; Caputo, A.; Tirkolaee, E.B.; Ghoushchi, S.J.; Bendechache, M. Brain tumor segmentation of MRI images: A comprehensive review on the application of artificial intelligence tools. Comput. Biol. Med. 2023, 152, 106405. [Google Scholar] [CrossRef]
- Grignaffini, F.; Barbuto, F.; Piazzo, L.; Troiano, M.; Simeoni, P.; Mangini, F.; Pellacani, G.; Cantisani, C.; Frezza, F. Machine Learning Approaches for Skin Cancer Classification from Dermoscopic Images: A Systematic Review. Algorithms 2022, 15, 438. [Google Scholar] [CrossRef]
- Rajpara, S.M.; Botello, A.P.; Townend, J.; Ormerod, A.D. Systematic review of dermoscopy and digital dermoscopy/artificial intelligence for the diagnosis of melanoma. Br. J. Dermatol. 2009, 161, 591–604. [Google Scholar] [CrossRef] [PubMed]
- Mishra, N.K.; Celebi, M.E. An overview of melanoma detection in dermoscopy images using image processing and machine learning. arXiv 2016, arXiv:1601.07843. [Google Scholar]
- Chen, X.; Lu, Q.; Chen, C.; Jiang, G. Recent developments in dermoscopy for dermatology. J. Cosmet. Dermatol. 2021, 20, 1611–1617. [Google Scholar] [CrossRef] [PubMed]
- Grignaffini, F.; Troiano, M.; Barbuto, F.; Simeoni, P.; Mangini, F.; D’andrea, G.; Piazzo, L.; Cantisani, C.; Musolff, N.; Ricciuti, C.; et al. Anomaly Detection for Skin Lesion Images Using Convolutional Neural Network and Injection of Handcrafted Features: A Method That Bypasses the Preprocessing of Dermoscopic Images. Algorithms 2023, 16, 466. [Google Scholar] [CrossRef]
- Spanhol, F.A.; Oliveira, L.S.; Petitjean, C.; Heutte, L. Breast cancer histopathological image classification using convolutional neural networks. In Proceedings of the 2016 International Joint Conference on Neural Networks (IJCNN), Vancouver, BC, Canada, 24–29 July 2016; pp. 2560–2567. [Google Scholar] [CrossRef]
- Kieffer, B.; Babaie, M.; Kalra, S.; Tizhoosh, H.R. Convolutional neural networks for histopathology image classification: Training vs. using pre-trained networks. In Proceedings of the 2017 Seventh International Conference on Image Processing Theory, Tools and Applications (IPTA), Montreal, QC, Canada, 28 November–1 December 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Mungle, T.; Tewary, S.; Das, D.K.; Arun, I.; Basak, B.; Agarwal, S.; Ahmed, R.; Chatterjee, S.; Chakraborty, C. MRF-ANN: A machine learning approach for automated ER scoring of breast cancer immunohistochemical images. J. Microsc. 2017, 267, 117–129. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Wang, D.; Rubadue, C.; Suster, D.; Beck, A. Deep learning assessment of tumor proliferation in breast cancer histological images. In Proceedings of the 2017 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Kansas City, MO, USA, 13–16 November 2017; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2017; pp. 600–603. [Google Scholar] [CrossRef]
- Ludovic, R.; Daniel, R.; Nicolas, L.; Maria, K.; Humayun, I.; Jacques, K.; Frédérique, C.; Catherine, G.; Gilles, L.N.; Metin, N.G. Mitosis detection in breast cancer histological images An ICPR 2012 contest. J. Pathol. Inform. 2013, 4, 8. [Google Scholar] [CrossRef]
- Kumar, M.D.; Babaie, M.; Zhu, S.; Kalra, S.; Tizhoosh, H.R. A comparative study of CNN, BoVW and LBP for classification of histopathological images. In Proceedings of the 2017 IEEE Symposium Series on Computational Intelligence (SSCI), Honolulu, HI, USA, 27 November–1 December 2017; pp. 1–7. [Google Scholar] [CrossRef]
- Nawaz, W.; Ahmed, S.; Tahir, A.; Khan, H.A. Classification of breast cancer histology images using alexnet. In Image Analysis and Recognition: 15th International Conference, ICIAR 2018, Póvoa de Varzim, Portugal, 27–29 June 2018; Proceedings 15; Springer International Publishing: Povoa de Varzim, Portugal, 2018; pp. 869–876. [Google Scholar]
- Araújo, T.; Aresta, G.; Castro, E.; Rouco, J.; Aguiar, P.; Eloy, C.; Polónia, A.; Campilho, A. Classification of breast cancer histology images using convolutional neural networks. PLoS ONE 2017, 12, e0177544. [Google Scholar] [CrossRef]
- Vesal, S.; Ravikumar, N.; Davari, A.; Ellmann, S.; Maier, A. Classification of breast cancer histology images using transfer learning. In Image Analysis and Recognition: 15th International Conference, ICIAR 2018, Póvoa de Varzim, Portugal, 27–29 June 2018; Proceedings 15; Springer International Publishing: Povoa de Varzim, Portugal, 2018; pp. 812–819. [Google Scholar]
- Chen, J.; Srinivas, C. Automatic lymphocyte detection in H&E images with deep neural networks. arXiv 2016, arXiv:1612.03217. [Google Scholar]
- Abas, F.S.; Gokozan, H.N.; Goksel, B.; Otero, J.J.; Gurcan, M.N. Intraoperative neuropathology of glioma recurrence: Cell detection and classification. In Proceedings of the International Society for Optics and Photonics (SPIE) Conference on Medical Imaging, San Diego, CA, USA, 27 February–3 March 2016; p. 979109. [Google Scholar] [CrossRef]
- Khosravi, P.; Kazemi, E.; Imielinski, M.; Elemento, O.; Hajirasouliha, I. Deep Convolutional Neural Networks Enable Discrimination of Heterogeneous Digital Pathology Images. EBioMedicine 2018, 27, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.E.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, CVPR, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar] [CrossRef]
- Kainz, P.; Pfeiffer, M.; Urschler, M. Segmentation and classification of colon glands with deep convolutional neural networks and total variation regularization. PeerJ 2017, 5, e3874. [Google Scholar] [CrossRef] [PubMed]
- Stanitsas, P.; Cherian, A.; Li, X.; Truskinovsky, A.; Morellas, V.; Papanikolopoulos, N. Evaluation of feature descriptors for cancerous tissue recognition. In Proceedings of the 23rd International Conference on Pattern Recognition, Cancun, Mexico, 4–8 December 2016; pp. 1490–1495. [Google Scholar] [CrossRef]
- Malon, C.; Brachtel, E.; Cosatto, E.; Graf, H.P.; Kurata, A.; Kuroda, M.; Meyer, J.S.; Saito, A.; Wu, S.; Yagi, Y. Mitotic figure recognition: Agreement among pathologists and computerized detector. Anal. Cell Pathol. 2012, 35, 97–100. [Google Scholar] [CrossRef]
- Budak, Ü.; Cömert, Z.; Rashid, Z.N.; Şengür, A.; Çıbuk, M. Computer-aided diagnosis system combining FCN and Bi-LSTM model for efficient breast cancer detection from histopathological images. Appl. Soft Comput. 2019, 85, 105765. [Google Scholar] [CrossRef]
- Jiang, Y.; Yang, M.; Wang, S.; Li, X.; Sun, Y. Emerging role of deep learning-based artificial intelligence in tumor pathology. Cancer Commun. 2020, 40, 154–166. [Google Scholar] [CrossRef]
- Bellocq, J.P.; Anger, E.; Camparo, P.; Capron, F.; Chenard, M.P.; Chetritt, J.; Chigot, J.P.; Cochand-Priollet, B.; Coindre, J.M.; Copin, M.C.; et al. Sécuriser le diagnostic en anatomie et cytologie pathologiques en 2011. L’erreur diagnostique: Entre discours et réalité. Ann Pathol. 2011, 31, S92–S94. [Google Scholar] [CrossRef]
- Baxi, V.; Edwards, R.; Montalto, M.; Saha, S. Digital pathology and artificial intelligence in translational medicine and clinical practice. Mod. Pathol. 2022, 35, 23–32. [Google Scholar] [CrossRef]
- Kaushal, C.; Bhat, S.; Koundal, D.; Singla, A. Recent trends in computer assisted diagnosis (CAD) system for breast cancer diagnosis using histopathological images. IRBM 2019, 40, 211–227. [Google Scholar] [CrossRef]
- Niazi, M.K.K.; Parwani, A.V.; Gurcan, M.N. Digital pathology and artificial intelligence. Lancet Oncol. 2019, 20, e253–e261. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.; Nitschke, G. Improving deep learning with generic data augmentation. In Proceedings of the 2018 IEEE Symposium Series on Computational Intelligence (SSCI), Bangalore, India, 18–21 November 2018; pp. 1542–1547. [Google Scholar] [CrossRef]
- Perez, L.; Wang, J. The effectiveness of data augmentation in image classification using deep learning. arXiv 2017, arXiv:1712.04621. [Google Scholar]
- Wong, S.C.; Gatt, A.; Stamatescu, V.; McDonnell, M.D. Understanding data augmentation for classification: When to warp? In Proceedings of the 2016 International Conference on Digital Image Computing: Techniques and Applications (DICTA), Gold Coast, Australia, 30 November–2 December 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Shorten, C.; Khoshgoftaar, T.M. A survey on image data augmentation for deep learning. J. Big Data 2019, 6, 60. [Google Scholar] [CrossRef]
- Balsano, C.; Alisi, A.; Brunetto, M.R.; Invernizzi, P.; Burra, P.; Piscaglia, F.; Special Interest Group (SIG) Artificial Intelligence and Liver Diseases; Italian Association for the Study of the Liver (AISF). The application of artificial intelligence in hepatology: A systematic review. Dig. Liver Dis. 2022, 54, 299–308. [Google Scholar] [CrossRef]
- Hardie, A.D.; Chamberlin, J.H.; Boyum, J.H.; Sharbidre, K.G.; Petrocelli, R.; Flemming, B.P.; Zahid, M.; Venkatesh, S.K.; Mruthyunjayappa, S.; Hajdu, C.H.; et al. Multi-Center Follow-up Study to Develop a Classification System Which Differentiates Mucinous Cystic Neoplasm of the Liver and Benign Hepatic Cyst Using Machine Learning. Acad. Radiol. 2022, 29, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Woznicki, P.; Siedek, F.; van Gastel, M.D.; Dos Santos, D.P.; Arjune, S.; Karner, L.A.; Meyer, F.; Caldeira, L.L.; Persigehl, T.; Gansevoort, R.T.; et al. Automated Kidney and Liver Segmentation in MR Images in Patients with Autosomal Dominant Polycystic Kidney Disease: A Multicenter Study. Kidney360 2022, 3, 2048–2058. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.H.; Lim, M.; Han, G.; Park, H.; Kim, Y.B.; Park, J.; Jun, S.Y.; Lee, J.; Cho, J.W. Preparing pathological data to develop an artificial intelligence model in the nonclinical study. Sci. Rep. 2023, 13, 3896. [Google Scholar] [CrossRef]
- Nowak, S.; Mesropyan, N.; Faron, A.; Block, W.; Reuter, M.; Attenberger, U.I.; Luetkens, J.A.; Sprinkart, A.M. Detection of liver cirrhosis in standard T2-weighted MRI using deep transfer learning. Eur. Radiol. 2021, 31, 8807–8815. [Google Scholar] [CrossRef]
- Luetkens, J.A.; Nowak, S.; Mesropyan, N.; Block, W.; Praktiknjo, M.; Chang, J.; Bauckhage, C.; Sifa, R.; Sprinkart, A.M.; Faron, A.; et al. Deep learning supports the differentiation of alcoholic and other-than-alcoholic cirrhosis based on MRI. Sci. Rep. 2022, 12, 8297. [Google Scholar] [CrossRef]
- Konerman, M.A.; Zhang, Y.; Zhu, J.; Higgins, P.D.; Lok, A.S.; Waljee, A.K. Improvement of predictive models of risk of disease progression in chronic hepatitis C by incorporating longitudinal data. Hepatology 2015, 61, 1832–1841. [Google Scholar] [CrossRef]
- Ma, H.; Xu, C.F.; Shen, Z.; Yu, C.H.; Li, Y.M. Application of machine learning techniques for clinical predictive modeling: A cross-sectional study on nonalcoholic fatty liver disease in China. Biomed. Res. Int. 2018, 2018, 4304376. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Mehta, R.; Moris, D.; Sahara, K.; Bagante, F.; Paredes, A.Z.; Farooq, A.; Ratti, F.; Marques, H.P.; Silva, S.; et al. Utilizing machine learning for pre-and postoperative assessment of patients undergoing resection for BCLC-0, A and B hepatocellular carcinoma: Implications for resection beyond the BCLC guidelines. Ann. Surg. Oncol. 2020, 27, 866–874. [Google Scholar] [CrossRef]
- Li, J.; Wu, Q.Q.; Zhu, R.H.; Lv, X.; Wang, W.Q.; Wang, J.L.; Liang, B.Y.; Huang, Z.Y.; Zhang, E.L. Machine learning predicts portal vein thrombosis after splenectomy in patients with portal hypertension: Comparative analysis of three practical models. World J. Gastroenterol. 2022, 28, 4681–4697. [Google Scholar] [CrossRef]
- Singh, Y.; Jons, W.A.; Eaton, J.E.; Vesterhus, M.; Karlsen, T.; Bjoerk, I.; Abildgaard, A.; Jorgensen, K.K.; Folseraas, T.; Little, D. Algebraic topology-based machine learning using MRI predicts outcomes in primary sclerosing cholangitis. Eur. Radiol. Exp. 2022, 6, 58. [Google Scholar] [CrossRef]
- Ji, G.W.; Zhu, F.P.; Xu, Q.; Wang, K.; Wu, M.Y.; Tang, W.W.; Li, X.C.; Wang, X.H. Machine-learning analysis of contrast-enhanced CT radiomics predicts recurrence of hepatocellular carcinoma after resection: A multi-institutional study. EBioMedicine 2019, 50, 156–165. [Google Scholar] [CrossRef]
- Wang, J.; Zheng, T.; Liao, Y.; Geng, S.; Li, J.; Zhang, Z.; Shang, D.; Liu, C.; Yu, P.; Huang, Y.; et al. Machine learning prediction model for post-hepatectomy liver failure in hepatocellular carcinoma: A multicenter study. Front. Oncol. 2022, 12, 986867. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Homeyer, A.; Schenk, A.; Arlt, J.; Dahmen, U.; Dirsch, O.; Hahn, H.K. Fast and accurate identification of fat droplets in histological images. Comput. Methods Programs Biomed. 2015, 121, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Saitou, T.; Takanezawa, S.; Ninomiya, H.; Watanabe, T.; Yamamoto, S.; Hiasa, Y.; Imamura, T. Tissue intrinsic fluorescence spectra-based digital pathology of liver fibrosis by marker-controlled segmentation. Front. Med. 2018, 5, 350. [Google Scholar] [CrossRef] [PubMed]
- Yarbakht, M.; Pradhan, P.; Köse-Vogel, N.; Bae, H.; Stengel, S.; Meyer, T.; Schmitt, M.; Stallmach, A.; Popp, J.; Bocklitz, T.W.; et al. Nonlinear Multimodal Imaging Characteristics of Early Septic Liver Injury in a Mouse Model of Peritonitis. Anal. Chem. 2019, 91, 11116–11121. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.X.; Jin, R.; Li, X.H.; Yang, Q.; Teng, X.; Liu, F.F.; Wu, N.; Rao, H.Y.; Liu, F. Collagen co-localized with macrovesicular steatosis better differentiates fibrosis progression in non-alcoholic fatty liver disease mouse models. Front. Med. 2023, 10, 1172058. [Google Scholar] [CrossRef] [PubMed]
- Puri, M. Automated machine learning diagnostic support system as a computational biomarker for detecting drug-induced liver injury patterns in whole slide liver pathology images. Assay. Drug Dev. Technol. 2020, 18, 1–10. [Google Scholar] [CrossRef]
- Ramot, Y.; Zandani, G.; Madar, Z.; Deshmukh, S.; Nyska, A. Utilization of a deep learning algorithm for microscope-based fatty vacuole quantification in a fatty liver model in mice. Toxicol. Pathol. 2020, 48, 702–707. [Google Scholar] [CrossRef]
- Ramot, Y.; Deshpande, A.; Morello, V.; Michieli, P.; Shlomov, T.; Nyska, A. Microscope-based automated quantification of liver fibrosis in mice using a deep learning algorithm. Toxicol. Pathol. 2021, 49, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Pischon, H.; Mason, D.; Lawrenz, B.; Blanck, O.; Frisk, A.L.; Schorsch, F.; Bertani, V. Artificial intelligence in toxicologic pathology: Quantitative evaluation of compound-induced hepatocellular hypertrophy in rats. Toxicol. Pathol. 2021, 49, 928–937. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, T.; Deshpande, A.; Hajra, A.; Thomas, T.; Muta, K.; Yamada, N.; Yasui, Y.; Shoda, T. Deep learning-based image-analysis algorithm for classification and quantification of multiple histopathological lesions in rat liver. J. Toxicol. Pathol. 2022, 35, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Baek, E.B.; Hwang, J.H.; Park, H.; Lee, B.S.; Son, H.Y.; Kim, Y.B.; Jun, S.Y.; Her, J.; Lee, J.; Cho, J.W. Artificial intelligence-assisted image analysis of acetaminophen-induced acute hepatic injury in Sprague-Dawley rats. Diagnostics 2022, 12, 1478. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Baek, E.B.; Hwang, J.H.; Lim, M.; Jung, W.H.; Bae, M.A.; Son, H.Y.; Cho, J.W. Application of convolutional neural network for analyzing hepatic fibrosis in mice. J. Toxicol. Pathol. 2023, 3, 21–30. [Google Scholar] [CrossRef]
- Shi, J.; Li, Y.; Zhu, J.; Sun, H.; Cai, Y. Joint sparse coding based spatial pyramid matching for classification of color medical image. Comput. Med. Imaging Graph. 2015, 41, 61–66. [Google Scholar] [CrossRef]
- Liu, C.; Huang, Y.; Ozolek, J.A.; Hanna, M.G.; Singh, R.; Rohde, G.K. SetSVM: An approach to set classification in nuclei-based cancer detection. IEEE J. Biomed. Health Inf. 2019, 23, 351–361. [Google Scholar] [CrossRef]
- Gawrieh, S.; Sethunath, D.; Cummings, O.W.; Kleiner, D.E.; Vuppalanchi, R.; Chalasani, N.; Tuceryan, M. Automated quantification and architectural pattern detection of hepatic fibrosis in NAFLD. Ann. Diagn. Pathol. 2020, 47, 151518. [Google Scholar] [CrossRef]
- Pérez-Sanz, F.; Riquelme-Pérez, M.; Martínez-Barba, E.; de la Peña-Moral, J.; Salazar Nicolás, A.; Carpes-Ruiz, M.; Esteban-Gil, A.; Legaz-García, M.D.C.; Parreño-González, M.A.; Ramírez, P.; et al. Efficiency of machine learning algorithms for the determination of macrovesicular steatosis in frozen sections stained with sudan to evaluate the quality of the graft in liver transplantation. Sensors 2021, 21, 1993. [Google Scholar] [CrossRef]
- Astbury, S.; Grove, J.I.; Dorward, D.A.; Guha, I.N.; Fallowfield, J.A.; Kendall, T.J. Reliable computational quantification of liver fibrosis is compromised by inherent staining variation. J. Pathol. Clin. Res. 2021, 7, 471–481. [Google Scholar] [CrossRef]
- Wan, J.; Dong, Y.; Xue, J.H.; Lin, L.; Du, S.; Dong, J.; Yao, Y.; Li, C.; Ma, H. Polarization-based probabilistic discriminative model for quantitative characterization of cancer cells. Biomed. Opt. Express 2022, 13, 3339–3354. [Google Scholar] [CrossRef]
- Lin, H.; Wei, C.; Wang, G.; Chen, H.; Lin, L.; Ni, M.; Chen, J.; Zhuo, S. Automated classification of hepatocellular carcinoma differentiation using multiphoton microscopy and deep learning. J. Biophotonics 2019, 12, e201800435. [Google Scholar] [CrossRef]
- Guo, X.; Wang, F.; Teodoro, G.; Farris, A.B.; Kong, J. Liver steatosis segmentation with deep learning methods. Proc. IEEE Int. Symp. Biomed. Imaging 2019, 2019, 24–27. [Google Scholar] [CrossRef]
- Roy, M.; Wang, F.; Vo, H.; Teng, D.; Teodoro, G.; Farris, A.B.; Castillo-Leon, E.; Vos, M.B.; Kong, J. Deep-learning-based accurate hepatic steatosis quantification for histological assessment of liver biopsies. Lab. Investig. 2020, 100, 1367–1383. [Google Scholar] [CrossRef]
- Levy, J.J.; Salas, L.A.; Christensen, B.C.; Sriharan, A.; Vaickus, L.J. PathFlowAI: A high-throughput workflow for preprocessing, deep learning and interpretation in digital pathology. In Proceedings of the Pacific Symposium on Biocomputing 2020, Kohala Coast, HI, USA, 3–7 January 2020; pp. 403–414. [Google Scholar] [CrossRef]
- Levy, J.J.; Azizgolshani, N.; Andersen, M.J., Jr.; Suriawinata, A.; Liu, X.; Lisovsky, M.; Ren, B.; Bobak, C.A.; Christensen, B.C.; Vaickus, L.J. A large-scale internal validation study of unsupervised virtual trichrome staining technologies on nonalcoholic steatohepatitis liver biopsies. Mod. Pathol. 2021, 34, 808–822. [Google Scholar] [CrossRef]
- Wang, Z.; Saoud, C.; Wangsiricharoen, S.; James, A.W.; Popel, A.S.; Sulam, J. Label cleaning multiple instance learning: Refining coarse annotations on single whole-slide images. IEEE Trans. Med. Imaging 2022, 41, 3952–3968. [Google Scholar] [CrossRef]
- Cinar, U.; Cetin Atalay, R.; Cetin, Y.Y. Human Hepatocellular Carcinoma Classification from H&E Stained Histopathology Images with 3D Convolutional Neural Networks and Focal Loss Function. J. Imaging 2023, 9, 25. [Google Scholar] [CrossRef]
- Dievernich, A.; Stegmaier, J.; Achenbach, P.; Warkentin, S.; Braunschweig, T.; Neumann, U.P.; Klinge, U.A. Deep-Learning-Computed Cancer Score for the Identification of Human Hepatocellular Carcinoma Area Based on a Six-Colour Multiplex Immunofluorescence Panel. Cells 2023, 12, 1074. [Google Scholar] [CrossRef]
- Zhan, H.; Chen, S.; Gao, F.; Wang, G.; Chen, S.D.; Xi, G.; Yuan, H.Y.; Li, X.; Liu, W.Y.; Byrne, C.D.; et al. AutoFibroNet: A deep learning and multi-photon microscopy-derived automated network for liver fibrosis quantification in MAFLD. Aliment. Pharmacol. Ther. 2023, 58, 573–584. [Google Scholar] [CrossRef]
- Wei, S.; Si, L.; Huang, T.; Du, S.; Yao, Y.; Dong, Y.; Ma, H. Deep-learning-based cross-modality translation from Stokes image to bright-field contrast. J. Biomed. Opt. 2023, 28, 102911. [Google Scholar] [CrossRef]
- Becker, L.; Lu, C.E.; Montes-Mojarro, I.A.; Layland, S.L.; Khalil, S.; Nsair, A.; Duffy, G.P.; Fend, F.; Marzi, J.; Schenke-Layland, K. Raman microspectroscopy identifies fibrotic tissues in collagen-related disorders via deconvoluted collagen type I spectra. Acta Biomater. 2023, 162, 278–291. [Google Scholar] [CrossRef]
- Olveres, J.; González, G.; Torres, F.; Moreno-Tagle, J.C.; Carbajal-Degante, E.; Valencia-Rodríguez, A.; Méndez-Sánchez, N.; Escalante-Ramírez, B. What is new in computer vision and artificial intelligence in medical image analysis applications. Quant. Imaging Med. Surg. 2021, 11, 3830–3853. [Google Scholar] [CrossRef]
- de Matos, J.; Ataky, S.T.M.; de Souza Britto, A., Jr.; Soares de Oliveira, L.E.; Lameiras Koerich, A. Machine learning methods for histopathological image analysis: A review. Electronics 2021, 10, 562. [Google Scholar] [CrossRef]
- Allaume, P.; Rabilloud, N.; Turlin, B.; Bardou-Jacquet, E.; Loréal, O.; Calderaro, J.; Khene, Z.E.; Acosta, O.; De Crevoisier, R.; Rioux-Leclercq, N.; et al. Artificial Intelligence-Based Opportunities in Liver Pathology-A Systematic Review. Diagnostics 2023, 13, 1799. [Google Scholar] [CrossRef]
- Sounderajah, V.; Ashrafian, H.; Rose, S.; Shah, N.H.; Ghassemi, M.; Golub, R.; Kahn, C.E., Jr.; Esteva, A.; Karthikesalingam, A.; Mateen, B.; et al. A quality assessment tool for artificial intelligence-centered diagnostic test accuracy studies: QUADAS-AI. Nat. Med. 2021, 27, 1663–1665. [Google Scholar] [CrossRef]
- Rana, M.; Bhushan, M. Machine learning and deep learning approach for medical image analysis: Diagnosis to detection. Multimed. Tools Appl. 2023, 82, 26731–26769. [Google Scholar] [CrossRef]
- Jahn, S.W.; Plass, M.; Moinfar, F. Digital Pathology: Advantages, Limitations and Emerging Perspectives. J. Clin. Med. 2020, 9, 3697. [Google Scholar] [CrossRef]
- Komura, D.; Ishikawa, S. Machine learning approaches for pathologic diagnosis. Virchows Arch. 2019, 475, 131–138. [Google Scholar] [CrossRef]
- Shmatko, A.; Ghaffari Laleh, N.; Gerstung, M.; Kather, J.N. Artificial intelligence in histopathology: Enhancing cancer research and clinical oncology. Nat. Cancer 2022, 3, 1026–1038. [Google Scholar] [CrossRef]
- Acs, B.; Rantalainen, M.; Hartman, J. Artificial intelligence as the next step towards precision pathology. J. Intern. Med. 2020, 288, 62–81. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas (TGCA). Available online: https://tcga-data.nci.nih.gov/tcga/ (accessed on 25 September 2017).
- Lonsdale, J.; Thomas, J.; Salvatore, M.; Phillips, R.; Lo, E.; Shad, S.; Hasz, R.; Walters, G.; Garcia, F.; Young, N.; et al. The Genotype-Tissue Expression (GTEx) project. Nat. Genet. 2013, 45, 580–585. [Google Scholar] [CrossRef]
- Marinelli, R.J.; Montgomery, K.; Liu, C.L.; Shah, N.H.; Prapong, W.; Nitzberg, M.; Zachariah, Z.K.; Sherlock, G.J.; Natkunam, Y.; West, R.B.; et al. The Stanford Tissue Microarray Database. Nucleic Acids Res. 2008, 36, D871–D877. [Google Scholar] [CrossRef]
- Komura, D.; Ishikawa, S. Machine learning methods for histopathological image analysis. Comput. Struct. Biotechnol. J. 2018, 16, 34–42. [Google Scholar] [CrossRef]
- Thakur, N.; Yoon, H.; Chong, Y. Current trends of artificial intelligence for colorectal cancer pathology image analysis: A systematic review. Cancers 2020, 12, 1884. [Google Scholar] [CrossRef]
- Abdelsamea, M.M.; Zidan, U.; Senousy, Z.; Gaber, M.M.; Rakha, E.; Ilyas, M. A survey on artificial intelligence in histopathology image analysis. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2022, 12, e1474. [Google Scholar] [CrossRef]
- Wang, S.; Yang, D.M.; Rong, R.; Zhan, X.; Fujimoto, J.; Liu, H.; Minna, J.; Wistuba, I.I.; Xie, Y.; Xiao, G. Artificial intelligence in lung cancer pathology image analysis. Cancers 2019, 11, 1673. [Google Scholar] [CrossRef]
- Jain, D.; Torres, R.; Celli, R.; Koelmel, J.; Charkoftaki, G.; Vasiliou, V. Evolution of the liver biopsy and its future. Transl. Gastroenterol. Hepatol. 2021, 6, 20. [Google Scholar] [CrossRef]
- Sanyal, A.J.; Jha, P.; Kleiner, D.E. Digital pathology for nonalcoholic steatohepatitis assessment. Nat. Rev. Gastroenterol. Hepatol. 2023, 21, 57–69. [Google Scholar] [CrossRef]
- Briganti, G.; Le Moine, O. Artificial intelligence in medicine: Today and tomorrow. Front. Med. 2020, 7, 27. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tool Used | Study Aim | Model of Animals | Data Augmentation | Results | Author and Year |
|---|---|---|---|---|---|
| RF | Fat droplet identification for rapid and accurate quantification of hepatic steatosis | NAFLD in rats with methionine-choline-deficient plus high-fat diet | - | SE SFD: 0.91 ± 0.02; SE CFD: 0.90 ± 0.02; SP: 0.92 ± 0.01; ACC: 0.91 ± 0.01 | Homeyer et al., 2015 [68] |
| K-means and BoF framework | Analysis of fibrosis states via the quantification of spectral–spatial features | Carbon Tetrachloride-induced hepatic fibrosis in mice | - | ACC: 0.90–0.95 | Saitou et al., 2018 [69] |
| LDA | Analysis of sepsis-induced liver damage | Polymicrobial abdominal infection in mice | - | SHG AUC: 0.49; TPEF AUC: 0.83; CARS AUC: 0.93; SHG/TPEF/CARS AUC: 0.85 | Yarbakht et al., 2019 [70] |
| Classification and Regression Trees | Analysis of steatosis and fibrosis states using label-free microscopy | Mice model of diet-induced NAFLD | - | Steatosis AUC: [0.81–1] Fibrosis AUC: [0.73–1] | Wang et al., 2023 [71] |
| Tool Used | Study Aim | Model of Animals | Data Augmentation | Results | Author and Year |
|---|---|---|---|---|---|
| Google’s AutoML Visionbeta | Detection and classification of DILI | DILI induced with different drugs in rats | - | PR: 0.93; REC: 0.93; ACC: 0.93 | Puri 2020 [72] |
| AIRA Matrix | Quantification of fat vacuoles | NAFLD in mice by a high-fat diet or high-cholesterol-cholate diet | - | r = 0.87; p < 0.001 | Ramot et al., 2020 [73] |
| U-Net-like custom encoder–decoder architecture | Quantification of fibrosis | Carbon tetrachloride-induced hepatic fibrosis | Random affine transformations and color variations on each training tile | IoU: 0.80; F1: 0.98 | Ramot et al., 2021 [74] |
| U-Net22 | Evaluation of hepatocellular hypertrophy | Hepatocellular hypertrophy induced via treatment with Phenobarbital for 7 and 14 days in rats | Rotation, flipping of labeled tissue regions, and changes in brightness and contrast | Model 1—study 1: r = 0.874; study 2: r = 0.705. Model 2—study 2: r = 0.80 | Pischon et al., 2021 [75] |
| U-Net | Simultaneous classification and quantification of different histopathological findings | Hepatocellular damage induced via treatment with different drugs in rats | Chromatic (changes in saturation and hue) and geometric (rotation at multiple 90° angles and horizontal/vertical flips) increments | Lesion detection task—AUC: 0.89; REC: 0.85; SP: 0.82; PR: 0.67; ACC: 0.83; F1: 0.73 | Shimazaki et al., 2022 [76] |
| Mask R-CNN | DILI prediction | DILI induced via treatment with acetaminophen in rats | Reversing, rotating, and changing brightness (8 repetitions) | Portal triad Av PR: 0.95; R2: 0.94. Necrosis Av PR: 1.00; R2: 0.955. Inflammation Av PR: 0.96. Infiltration Av PR: 0.94. Total Av PR: 0.96 | Baek et al., 2022 [77] |
| Xception | To determine whether an AI algorithm can help the classification of liver fibrosis lesions | Liver lesions induced via treatment with HFD combined with CCl4 (HFDC) in mice and treatment with elafibranor in HFDC mice | - | ACC test: 1.00. Single slide PR: 0.85; REC: 0.96; F1: 0.90. Model vs. pathologists: r = 0.91. Model vs. annotations: r = 0.83 | Kim et al., 2023 [78] |
| Tool Used | Study Aim | Disease | Data Augmentation | Results | Author and Year |
|---|---|---|---|---|---|
| JScSPM method + SVM | Demonstrate the loss of color information related to the conversion of medical images to grayscale | HCC | - | Multiclass HIK-SVM ACC: 0.92 ± 0.0129; SE: 0.92 ± 0.0134; SP: 0.96 ± 0.0068. Multiclass CSK-SVM ACC: 0.92 ± 0.0136; SE: 0.91 ± 0.0134; SP: 0.96 ± 0.0067. Binary HIK-SVM ACC: 0.96 ± 0.083; SE: 0.9 ± 0.0213; SP: 0.99 ± 0.0122; AUC: 0.981. Binary CSK-SVM ACC: 0.96 ± 0.0166; SE: 0.89 ± 0.0261; SP: 0.996 ± 0.0099; AUC: 0.98 | Shi et al., 2015 [79] |
| SetSVM | Differentiation of malignant HCC from focal nodular hyperplasia | HCC | - | (1) ACC: 0.91; PR: 0.93; REC: 0.82; AUC: 0.93. (2) ACC: 0.85; PR: 0.86; REC: 0.71; AUC: 0.91. (3) ACC: 0.86; PR: 0.92; REC: 0.71; AUC: 0.87. | Liu et al., 2019 [80] |
| SVM with linear kernels | Detection and quantification of liver fibrosis | NAFLD | - | CPA R2: 0.67 and 0.86. Detection task—Av PR: 0.81; Av REC: 0.85; Av AUC: 0.88 | Gawrieh et al., 2020 [81] |
| KNN, SVM, RF, NB, simple ANN, and ANNs with TensorFlow and Keras | Determination of macrovesicular steatosis | NAFLD | - | KNN ACC: 0.996; SE: 0.84; SP: 0.999; PR: 0.96. SVM ACC: 0.996; SE: 0.96; SP: 0.997; PR: 0.89. RF ACC: 0.996; SE: 0.96; SP: 0.997; PR: 0.89. NB ACC: 0.997; SE: 0.91; SP: 0.999; PR: 0.97. ANN ACC: 0.997; SE: 0.96; SP: 0.998; PR: 0.91. Keras ACC: 0.995; SE: 0.97; SP: 0.996; PR: 0.96 | Pérez-Sanz et al., 2021 [82] |
| WEKA | Quantification of scarring in liver sections and study of the effect of staining variation | Cirrhosis from different etiologies | - | WEKA individuals rinter = 0.24, rintra = 0.24; WEKA combined (1) rinter = 0.29, rintra = 0.31; WEKA combined (2) rinter = 0.37, rintra = 0.53 | Astbury et al., 2021 [83] |
| L0 regularized LR | Quantitative characterization of cancer cells | Liver cancer | - | P-PDM ACC: 0.85; REC: 0.88; PR: 0.88 | Wan et al., 2022 [84] |
| Tool Used | Study Aim | Disease | Data Augmentation | Results | Author and Year |
|---|---|---|---|---|---|
| Pre-trained VGG-16 | Classification of HCC differentiation | HCC | Horizontal or vertical rotation and flipping | G1 vs. G2G3 AUC: 0.92; Av ACC: 0.94 (0.913–0.968). G2 vs. G1G3 AUC: 0.89; Av ACC: 0.86 (0.807–0.910). G3 vs. G1G2 AUC: 0.91; Av ACC: 0.81 (0.756–0.868) | Lin et al., 2019 [85] |
| Pre-trained Mask R-CNN with a ResNet50 backbone | Steatosis segmentation | NAFLD | Random affine transformation, random flipping, and Gaussian blurring | Av PR: 0.76; REC: 0.61; F1: 0.66; Jaccard index: 0.77 | Guo et al., 2019 [86] |
| DeEp LearnINg steatosis sEgmentation (DELINEATE) architecture: dil-U-Net + HNN + FCN-8s | Quantification of hepatic steatosis drops | NAFLD | Region module: horizontal flip, vertical flip, rotation in 4-degree angles, and re-scaling by 0.5 scales. Boundary module: rotation and flipping at 16 different angles | Identification task PR: 0.98 ± 0.01; REC: 0.91 ± 0.06; F1: 0.94 ± 0.03; Object wise Dice Index: 0.9492; Object wise Hausdorff Distance: 3.4591 | Roy et al., 2020 [87] |
| U-Net and ResNet34 | Assessment of steatohepatitis pattern | Steatohepatitis from undescribed etiology | - | Av SE: 0.71; Av AUC: 0.78 | Levy et al., 2020 [88] |
| CycleGAN | Conversion of staining of digital WSIs from H&E to trichrome using a GAN | NASH | - | r = 0.86; 95% CI: 0.84–0.88 | Levy et al., 2021 [89] |
| LC-MIL | Refinement of coarse annotation of cancerous regions in WSIs | HCC | - | LC-MIL-atten F1—S-I: 0.91 ± 0.098; S-II: 0.83 ± 0.128; S-III: 0.83 ± 0.163. LC-MIL-miNet F1—S-I: 0.88 ± 0.156; S-II: 0.84 ± 0.119; S-III: 0.83 ± 0.167 | Wang et al., 2022 [90] |
| 3D CNN | Classification of HCC | HCC | - | Gamma = 2, and alpha = 0.5: ACC: 0.97; PR: 0.999; REC: 0.97; F1: 0.98; MCC: 0.86 | Cinar et al., 2023 [91] |
| U-Net | Identification of cancer area by cancer score | HCC | - | ACC: 0.75 | Dievernich et al., 2023 [92] |
| AutoFibroNet | Classification of fibrosis grades in MAFLD patients | NAFLD/MAFLD | - | AUC G0,G1,G2,G3/4—first cohort: 0.99, 0.83, 0.80, 0.90; second cohort: 1.00, 0.83, 0.80, 0.94 | Zhan et al., 2023 [93] |
| CycleGAN | Development of a system to support the analysis of the properties of histological specimens | Liver samples from patients of undescribed etiology | - | Stokes images: 45 degrees—SSIM: 0.694; RMSE: 0.099; JSD: 0.181; EMD: 8.935. 135 degrees—SSIM: 0.710; RMSE: 0.104; JSD: 0.203; EMD: 11.515. R—SSIM: 0.732; RMSE: 0.099; JSD: 0.178; EMD: 9.353. L—SSIM: 0.713; RMSE: 0.101; JSD: 0.186; EMD: 9.077. E1—SSIM: 0.706; RMSE: 0.102; JSD: 0.209; EMD: 11.093. E2—SSIM: 0.7518; RMSE: 0.093; JSD: 0.178; EMD: 8.467 | Wei et al., 2023 [94] |
| Approach | Tissue | Results | Author and Year |
|---|---|---|---|
| SetSVM (ML) | Thyroid tissue sections stained with the Feulgen technique, and melanoma tissue sections stained using H&E | Thyroid cancer: Differentiation of follicular adenoma of the thyroid (FA) from nodular goiter (NG) [AUC: 0.83, 0.84, 0.80]; differentiation of follicular variant of papillary thyroid carcinoma (FVPC) from NG [AUC: 0.87, 0.91, 0.92]. Melanoma: Differentiation of malignant melanoma from dysplastic nevi [AUC: 0.75, 0.75, 0.78]. | Liu et al., 2019 [78] |
| L0 regularized LR (ML) | Breast cancer pathological tissues stained with H&E | P-PDM ACC: 0.87; REC: 0.87; PR: 0.88. | Wan et al., 2022 [82] |
| LC-MIL (DL) | Breast cancer lymph node metastasis tissues stained with H&E and colorectal cancer tissues stained with H&E | Breast cancer: LC-MIL-atten F1—S-I: 0.88 ± 0.068; S-II: 0.85 ± 0.084; S-III: 0.85 ± 0.096. LC-MIL-miNet F1—S-I: 0.87 ± 0.104; S-II: 0.84 ± 0.091; S-III: 0.84 ± 0.096. Colorectal cancer: LC-MIL-atten F1—S-I: 0.82 ± 0.167; S-II: 0.72 ± 0.138; S-III: 0.86 ± 0.077. LC-MIL-miNet F1—S-I: 0.81 ± 0.181; S-II: 0.79 ± 0.106; S-III: 0.87 ± 0.081. | Wang et al., 2022 [88] |
| CycleGAN (DL) | Breast tissues pathological slices with H&E staining, and lung tissues with two types of immunohistochemistry staining, i.e., thyroid transcription factor-1 and Ki-67 | Breast cancer: Stokes images: 45 degrees—SSIM: 0.727; RMSE: 0.130; JSD: 0.200; EMD: 9.761. 135 degrees—SSIM: 0.742; RMSE: 0.126; JSD: 0.191; EMD: 9.296. R—SSIM: 0.742; RMSE: 0.139; JSD: 0.202; EMD: 11.955. L—SSIM: 0.752; RMSE: 0.134; JSD: 0.226; EMD: 11.711. E1—SSIM: 0.760; RMSE: 0.126; JSD: 0.202; EMD: 9.796. E2—SSIM: 0.755; RMSE: 0.124; JSD: 0.192; EMD: 9.460. Lung cancer: Ki-67: Stokes images: 45 degrees—SSIM: 0.929; RMSE: 0.078; JSD: 0.237; EMD: 7.520. 135 degrees—SSIM: 0.923; RMSE: 0.075; JSD: 0.229; EMD: 6.870. R—SSIM: 0.917; RMSE: 0.083; JSD: 0.248; EMD: 7.914. L—SSIM: 0.911; RMSE: 0.081; JSD: 0.237; EMD: 7.322. E1—SSIM: 0.920; RMSE: 0.082; JSD: 0.240; EMD: 7.738. E2—SSIM: 0.908; RMSE: 0.093; JSD: 0.23; EMD: 7.693. TTF-1: Stokes images: 45 degrees—SSIM: 0.915; RMSE: 0.087; JSD: 0.246; EMD: 6.698. 135 degrees—SSIM: 0.904; RMSE: 0.101; JSD: 0.277; EMD: 8.384. R—SSIM: 0.917; RMSE: 0.092; JSD: 0.267; EMD: 7.360. L—SSIM: 0.925; RMSE: 0.092; JSD: 0.261; EMD: 7.519. E1—SSIM: 0.9214; RMSE: 0.097; JSD: 0.263; EMD: 7.998. E2—SSIM: 0.914; RMSE: 0.091; JSD: 0.253; EMD: 7.194. | Wei et al., 2023 [92] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grignaffini, F.; Barbuto, F.; Troiano, M.; Piazzo, L.; Simeoni, P.; Mangini, F.; De Stefanis, C.; Onetti Muda, A.; Frezza, F.; Alisi, A. The Use of Artificial Intelligence in the Liver Histopathology Field: A Systematic Review. Diagnostics 2024, 14, 388. https://doi.org/10.3390/diagnostics14040388
Grignaffini F, Barbuto F, Troiano M, Piazzo L, Simeoni P, Mangini F, De Stefanis C, Onetti Muda A, Frezza F, Alisi A. The Use of Artificial Intelligence in the Liver Histopathology Field: A Systematic Review. Diagnostics. 2024; 14(4):388. https://doi.org/10.3390/diagnostics14040388
Chicago/Turabian StyleGrignaffini, Flavia, Francesco Barbuto, Maurizio Troiano, Lorenzo Piazzo, Patrizio Simeoni, Fabio Mangini, Cristiano De Stefanis, Andrea Onetti Muda, Fabrizio Frezza, and Anna Alisi. 2024. "The Use of Artificial Intelligence in the Liver Histopathology Field: A Systematic Review" Diagnostics 14, no. 4: 388. https://doi.org/10.3390/diagnostics14040388