
Autoimmune Hepatitis: A Diagnostic and Therapeutic Overview
Abstract
:1. Introduction
2. Epidemiology
Genetic Susceptibility
3. Clinical Spectrum
3.1. Asymptomatic Disease
3.2. Symptomatic Disease
4. Specific Clinical Features and Presentations
4.1. AIH and PBC
4.2. AIH and PSC
4.3. DILI and AIH
4.4. AIH and Pregnancy
4.5. Viral Hepatitis and AIH
4.6. De Novo AIH after LT
4.7. Acute Disease, Acute Liver Failure and Chronic Complications in AIH
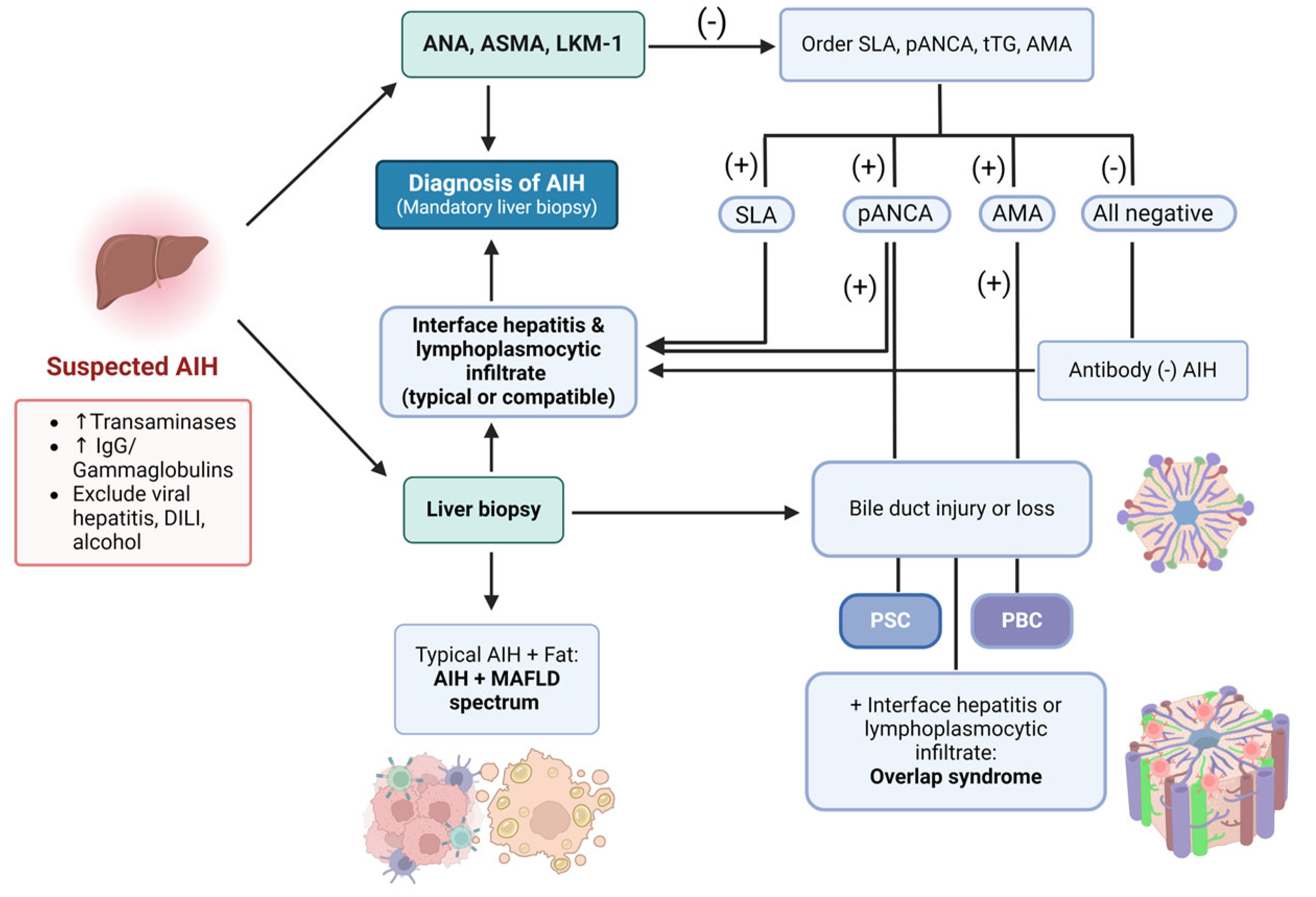
5. Diagnostic Workup
5.1. Biochemical Findings
5.2. Autoantibodies
5.3. Histology
5.4. Diagnostic Scoring Systems
5.5. Noninvasive Assessment of Hepatic Fibrosis
5.5.1. Biomarker Panels
5.5.2. Vibration-Controlled Transient Elastography (VCTE)
5.5.3. Magnetic Resonance Elastography (MRE)
5.5.4. Acoustic Radiation Force Impulse Imaging (ARFI)
6. Therapy in AIH
6.1. Pre-Treatment Considerations
6.1.1. Thiopurine Methyltransferase (TPMT)
6.1.2. Vaccination
6.1.3. HBV Reactivation Detection and Prevention
6.1.4. Osteoporosis
6.1.5. Metabolic Syndrome
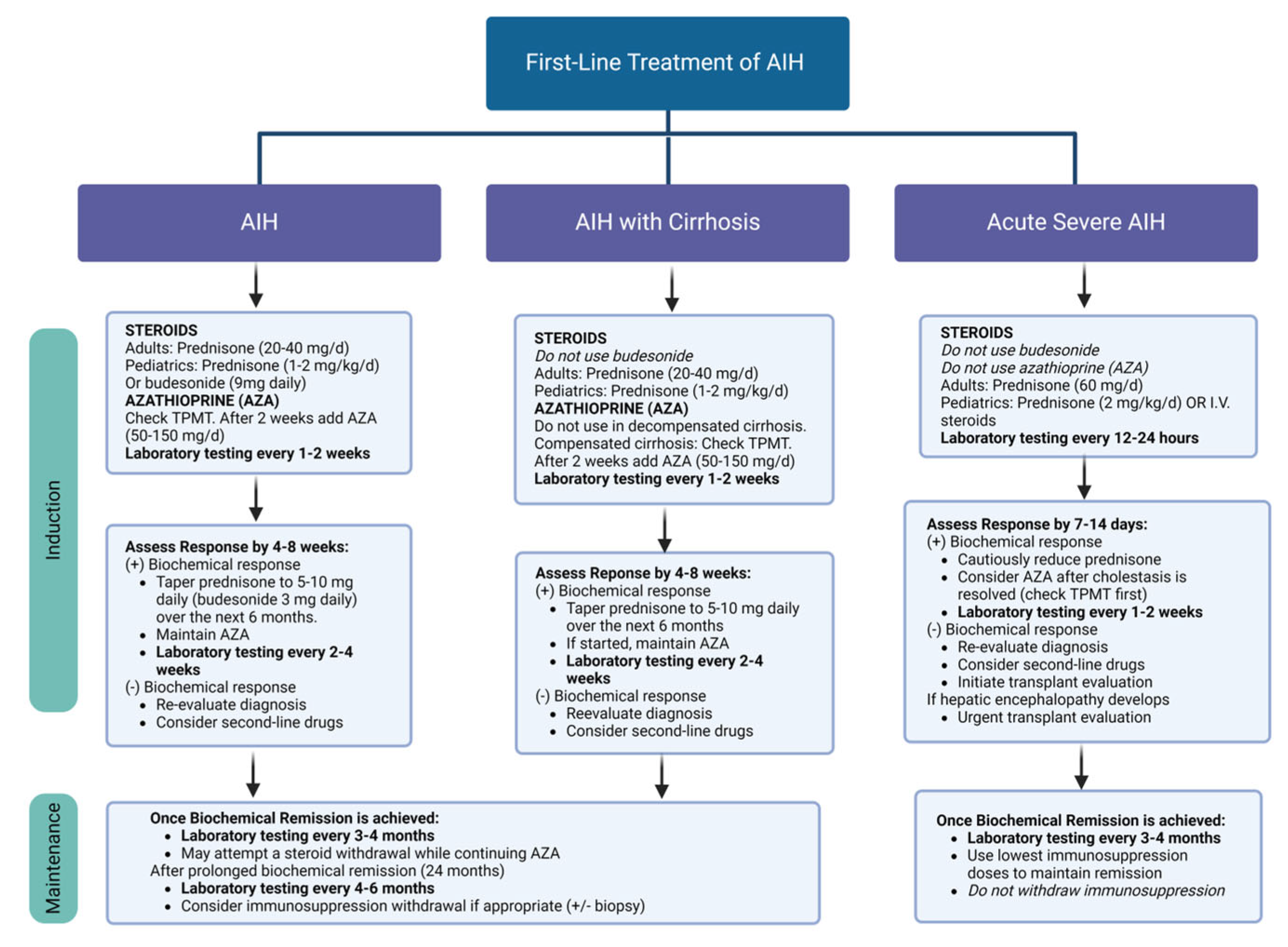
6.2. First-Line Treatment
6.2.1. AIH Induction Phase
6.2.2. AIH and Cirrhosis
6.2.3. Maintenance
6.2.4. Acute Severe AIH
6.2.5. Relapse in AIH
6.3. Second-Line Treatment
6.3.1. MMF
6.3.2. Calcineurin Inhibitors
6.3.3. Liver Transplantation in AIH
6.4. Future of Biologic Therapy in AIH
Rituximab and Infliximab
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

Appendix B

References
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, P.J.; Hirschfield, G.M. Recent advances in clinical practice: Epidemiology of autoimmune liver diseases. Gut 2021, 70, 1989–2003. [Google Scholar] [CrossRef] [PubMed]
- Mack, C.L.; Adams, D.; Assis, D.N.; Kerkar, N.; Manns, M.P.; Mayo, M.J.; Vierling, J.M.; Alsawas, M.; Murad, M.H.; Czaja, A.J. Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines from the American Association for the Study of Liver Diseases. Hepatology 2020, 72, 671–722. [Google Scholar] [CrossRef] [PubMed]
- Muratori, L.; Lohse, A.W.; Lenzi, M. Diagnosis and management of autoimmune hepatitis. BMJ 2023, 380, e070201. [Google Scholar] [CrossRef] [PubMed]
- van Gerven, N.M.; Verwer, B.J.; Witte, B.I.; van Erpecum, K.J.; van Buuren, H.R.; Maijers, I.; Visscher, A.P.; Verschuren, E.C.; van Hoek, B.; Coenraad, M.J.; et al. Epidemiology and clinical characteristics of autoimmune hepatitis in the Netherlands. Scand. J. Gastroenterol. 2014, 49, 1245–1254. [Google Scholar] [CrossRef]
- Gregorio, G.V.; Portmann, B.; Reid, F.; Donaldson, P.T.; Doherty, D.G.; McCartney, M.; Mowat, A.P.; Vergani, D.; Mieli-Vergani, G. Autoimmune hepatitis in childhood: A 20-year experience. Hepatology 1997, 25, 541–547. [Google Scholar] [CrossRef]
- Czaja, A.J. Global Disparities and Their Implications in the Occurrence and Outcome of Autoimmune Hepatitis. Dig. Dis. Sci. 2017, 62, 2277–2292. [Google Scholar] [CrossRef]
- Ngu, J.H.; Bechly, K.; Chapman, B.A.; Burt, M.J.; Barclay, M.L.; Gearry, R.B.; Stedman, C.A. Population-based epidemiology study of autoimmune hepatitis: A disease of older women? J. Gastroenterol. Hepatol. 2010, 25, 1681–1686. [Google Scholar] [CrossRef]
- Hahn, J.W.; Yang, H.R.; Moon, J.S.; Chang, J.Y.; Lee, K.; Kim, G.A.; Rahmati, M.; Koyanagi, A.; Smith, L.; Kim, M.S.; et al. Global incidence and prevalence of autoimmune hepatitis, 1970-2022: A systematic review and meta-analysis. EClinicalMedicine 2023, 65, 102280. [Google Scholar] [CrossRef]
- Bittermann, T.; Lewis, J.D.; Levy, C.; Goldberg, D.S. Sociodemographic and geographic differences in the US epidemiology of autoimmune hepatitis with and without cirrhosis. Hepatology 2023, 77, 367–378. [Google Scholar] [CrossRef]
- Minuk, G.Y.; Liu, S.; Kaita, K.; Wong, S.; Renner, E.; Rempel, J.; Uhanova, J. Autoimmune hepatitis in a North American Aboriginal/First Nations population. Autoimmune hepatitis in a North American Aboriginal/First Nations population. Can. J. Gastroenterol. 2008, 22, 829–834. [Google Scholar] [CrossRef]
- Levy, C.; Naik, J.; Giordano, C.; Mandalia, A.; O’Brien, C.; Bhamidimarri, K.R.; Schiff, E.R.; Martin, P. Hispanics with primary biliary cirrhosis are more likely to have features of autoimmune hepatitis and reduced response to ursodeoxycholic acid than non-Hispanics. Clin. Gastroenterol. Hepatol. 2014, 12, 1398–1405. [Google Scholar] [CrossRef]
- Munoz-Espinosa, L.; Alarcon, G.; Mercado-Moreira, A.; Cordero, P.; Caballero, E.; Avalos, V.; Villarreal, G.; Senties, K.; Puente, D.; Soto, J.; et al. Performance of the international classifications criteria for autoimmune hepatitis diagnosis in Mexican patients. Autoimmunity 2011, 44, 543–548. [Google Scholar] [CrossRef]
- Verma, S.; Torbenson, M.; Thuluvath, P.J. The impact of ethnicity on the natural history of autoimmune hepatitis. Hepatology 2007, 46, 1828–1835. [Google Scholar] [CrossRef]
- Gronbaek, L.; Vilstrup, H.; Jepsen, P. Autoimmune hepatitis in Denmark: Incidence, prevalence, prognosis, and causes of death. A nationwide registry-based cohort study. J. Hepatol. 2014, 60, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J.; Donaldson, P.T. Genetic susceptibilities for immune expression and liver cell injury in autoimmune hepatitis. Immunol. Rev. 2000, 174, 250–259. [Google Scholar] [CrossRef]
- Pando, M.; Larriba, J.; Fernandez, G.C.; Fainboim, H.; Ciocca, M.; Ramonet, M.; Badia, I.; Daruich, J.; Findor, J.; Tanno, H.; et al. Pediatric and adult forms of type I autoimmune hepatitis in Argentina: Evidence for differential genetic predisposition. Hepatology 1999, 30, 1374–1380. [Google Scholar] [CrossRef]
- Donaldson, P.T.; Doherty, D.G.; Hayllar, K.M.; McFarlane, I.G.; Johnson, P.J.; Williams, R. Susceptibility to autoimmune chronic active hepatitis: Human leukocyte antigens DR4 and A1-B8-DR3 are independent risk factors. Hepatology 1991, 13, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Kogan, J.; Safadi, R.; Ashur, Y.; Shouval, D.; Ilan, Y. Prognosis of Symptomatic Versus Asymptomatic Autoimmune Hepatitis_A Study of 68 Patients. J. Clin. Gastroenterol. 2002, 35, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J. Features and consequences of untreated type 1 autoimmune hepatitis. Liver Int. 2009, 29, 816–823. [Google Scholar] [CrossRef]
- Werner, M.; Prytz, H.; Ohlsson, B.; Almer, S.; Bjornsson, E.; Bergquist, A.; Wallerstedt, S.; Sandberg-Gertzen, H.; Hultcrantz, R.; Sangfelt, P.; et al. Epidemiology and the initial presentation of autoimmune hepatitis in Sweden: A nationwide study. Scand. J. Gastroenterol. 2008, 43, 1232–1240. [Google Scholar] [CrossRef]
- Schramm, C.; Wahl, I.; Weiler-Normann, C.; Voigt, K.; Wiegard, C.; Glaubke, C.; Brahler, E.; Lowe, B.; Lohse, A.W.; Rose, M. Health-related quality of life, depression, and anxiety in patients with autoimmune hepatitis. J. Hepatol. 2014, 60, 618–624. [Google Scholar] [CrossRef]
- Nikias, G.A.; Batts, K.P.; Czaja, A.J. The nature and prognostic implications of autoimmune hepatitis with an acute presentation. J. Hepatol. 1994, 21, 866–871. [Google Scholar] [CrossRef]
- Enke, T.; Livingston, S.; Rule, J.; Stravitz, T.; Rakela, J.; Bass, N.; Reuben, A.; Tujios, S.; Larson, A.; Sussman, N.; et al. Autoimmune hepatitis presenting as acute liver failure: A 20-year retrospective review of North America. Liver Transpl. 2023, 29, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, E.M.; Zondervan, P.E.; van Buuren, H.R. Paris criteria are effective in diagnosis of primary biliary cirrhosis and autoimmune hepatitis overlap syndrome. Clin. Gastroenterol. Hepatol. 2010, 8, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Chazouilleres, O.; Wendum, D.; Serfaty, L.; Montembault, S.; Rosmorduc, O.; Poupon, R. Primary biliary cirrhosis-autoimmune hepatitis overlap syndrome: Clinical features and response to therapy. Hepatology 1998, 28, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Boberg, K.M.; Chapman, R.W.; Hirschfield, G.M.; Lohse, A.W.; Manns, M.P.; Schrumpf, E.; International Autoimmune Hepatitis, G. Overlap syndromes: The International Autoimmune Hepatitis Group (IAIHG) position statement on a controversial issue. J. Hepatol. 2011, 54, 374–385. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of cholestatic liver diseases. J. Hepatol. 2009, 51, 237–267. [Google Scholar] [CrossRef] [PubMed]
- Gregorio, G.V.; Portmann, B.; Karani, J.; Harrison, P.; Donaldson, P.T.; Vergani, D.; Mieli-Vergani, G. Autoimmune hepatitis/sclerosing cholangitis overlap syndrome in childhood: A 16-year prospective study. Hepatology 2001, 33, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Rojas, C.P.; Bodicharla, R.; Campuzano-Zuluaga, G.; Hernandez, L.; Rodriguez, M.M. Autoimmune hepatitis and primary sclerosing cholangitis in children and adolescents. Fetal Pediatr. Pathol. 2014, 33, 202–209. [Google Scholar] [CrossRef]
- Czaja, A.J. Cholestatic phenotypes of autoimmune hepatitis. Clin. Gastroenterol. Hepatol. 2014, 12, 1430–1438. [Google Scholar] [CrossRef]
- Mieli-Vergani, G.; Heller, S.; Jara, P.; Vergani, D.; Chang, M.H.; Fujisawa, T.; González-Peralta, R.P.; Kelly, D.; Mohan, N.; Shah, U.; et al. Autoimmune hepatitis. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Perdigoto, R.; Carpenter, H.A.; Czaja, A.J. Frequency and significance of chronic ulcerative colitis in severe corticosteroid-treated autoimmune hepatitis. J. Hepatol. 1992, 14, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Mieli-Vergani, G.; Vergani, D.; Baumann, U.; Czubkowski, P.; Debray, D.; Dezsofi, A.; Fischler, B.; Gupte, G.; Hierro, L.; Indolfi, G.; et al. Diagnosis and Management of Pediatric Autoimmune Liver Disease: ESPGHAN Hepatology Committee Position Statement. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 345–360. [Google Scholar] [CrossRef]
- Lüth, S.; Kanzler, S.; Frenzel, C.; Kasper, H.U.; Dienes, H.P.; Schramm, C.; Galle, P.R.; Herkel, J.; Lohse, A.W. Characteristics and long-term prognosis of the autoimmune hepatitis/primary sclerosing cholangitis overlap syndrome. J. Clin. Gastroenterol. 2009, 43, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Bjornsson, E.; Talwalkar, J.; Treeprasertsuk, S.; Kamath, P.S.; Takahashi, N.; Sanderson, S.; Neuhauser, M.; Lindor, K. Drug-induced autoimmune hepatitis: Clinical characteristics and prognosis. Hepatology 2010, 51, 2040–2048. [Google Scholar] [CrossRef] [PubMed]
- Castiella, A.; Lucena, M.I.; Zapata, E.M.; Otazua, P.; Andrade, R.J. Drug-induced autoimmune-like hepatitis: A diagnostic challenge. Dig. Dis. Sci. 2011, 56, 2501–2502; author reply 2502–2503. [Google Scholar] [CrossRef] [PubMed]
- Appleyard, S.; Saraswati, R.; Gorard, D.A. Autoimmune hepatitis triggered by nitrofurantoin: A case series. J. Med. Case Rep. 2010, 4, 311. [Google Scholar] [CrossRef]
- Gough, A.; Chapman, S.; Wagstaff, K.; Emery, P.; Elias, E. Minocycline induced autoimmune hepatitis and systemic lupus erythematosus-like syndrome. BMJ 1996, 312, 169–172. [Google Scholar] [CrossRef]
- Germano, V.; Picchianti Diamanti, A.; Baccano, G.; Natale, E.; Onetti Muda, A.; Priori, R.; Valesini, G. Autoimmune hepatitis associated with infliximab in a patient with psoriatic arthritis. Ann. Rheum. Dis. 2005, 64, 1519–1520. [Google Scholar] [CrossRef]
- Watkins, P.B.; Seeff, L.B. Drug-induced liver injury: Summary of a single topic clinical research conference. Hepatology 2006, 43, 618–631. [Google Scholar] [CrossRef]
- Chalasani, N.; Bonkovsky, H.L.; Fontana, R.; Lee, W.; Stolz, A.; Talwalkar, J.; Reddy, K.R.; Watkins, P.B.; Navarro, V.; Barnhart, H.; et al. Features and Outcomes of 899 Patients with Drug-Induced Liver Injury: The DILIN Prospective Study. Gastroenterology 2015, 148, 1340–1352.e1347. [Google Scholar] [CrossRef]
- deLemos, A.S.; Foureau, D.M.; Jacobs, C.; Ahrens, W.; Russo, M.W.; Bonkovsky, H.L. Drug-induced liver injury with autoimmune features. Semin. Liver Dis. 2014, 34, 194–204. [Google Scholar] [CrossRef]
- de Boer, Y.S.; Kosinski, A.S.; Urban, T.J.; Zhao, Z.; Long, N.; Chalasani, N.; Kleiner, D.E.; Hoofnagle, J.H.; Drug-Induced Liver Injury, N. Features of Autoimmune Hepatitis in Patients with Drug-induced Liver Injury. Clin. Gastroenterol. Hepatol. 2017, 15, 103–112.e102. [Google Scholar] [CrossRef]
- Ramachandran, R.; Kakar, S. Histological patterns in drug-induced liver disease. J. Clin. Pathol. 2009, 62, 481–492. [Google Scholar] [CrossRef]
- Heurgue, A.; Vitry, F.; Diebold, M.D.; Yaziji, N.; Bernard-Chabert, B.; Pennaforte, J.L.; Picot, R.; Louvet, H.; Fremond, L.; Geoffroy, P.; et al. Overlap syndrome of primary biliary cirrhosis and autoimmune hepatitis: A retrospective study of 115 cases of autoimmune liver disease. Gastroenterol. Clin. Biol. 2007, 31, 17–25. [Google Scholar] [CrossRef]
- Buchel, E.; Van Steenbergen, W.; Nevens, F.; Fevery, J. Improvement of autoimmune hepatitis during pregnancy followed by flare-up after delivery. Am. J. Gastroenterol. 2002, 97, 3160–3165. [Google Scholar] [CrossRef]
- Westbrook, R.H.; Yeoman, A.D.; Kriese, S.; Heneghan, M.A. Outcomes of pregnancy in women with autoimmune hepatitis. J. Autoimmun. 2012, 38, J239–J244. [Google Scholar] [CrossRef]
- Schramm, C.; Herkel, J.; Beuers, U.; Kanzler, S.; Galle, P.R.; Lohse, A.W. Pregnancy in autoimmune hepatitis: Outcome and risk factors. Am. J. Gastroenterol. 2006, 101, 556–560. [Google Scholar] [CrossRef]
- Worns, M.A.; Teufel, A.; Kanzler, S.; Shrestha, A.; Victor, A.; Otto, G.; Lohse, A.W.; Galle, P.R.; Hohler, T. Incidence of HAV and HBV infections and vaccination rates in patients with autoimmune liver diseases. Am. J. Gastroenterol. 2008, 103, 138–146. [Google Scholar] [CrossRef]
- Muratori, L.; Lenzi, M.; Cataleta, M.; Giostra, F.; Cassani, F.; Ballardini, G.; Zauli, D.; Bianchi, F.B. Interferon therapy in liver/kidney microsomal antibody type 1-positive patients with chronic hepatitis C. J. Hepatol. 1994, 21, 199–203. [Google Scholar] [CrossRef]
- Dalekos, G.N.; Wedemeyer, H.; Obermayer-Straub, P.; Kayser, A.; Barut, A.; Frank, H.; Manns, M.P. Epitope mapping of cytochrome P4502D6 autoantigen in patients with chronic hepatitis C during alpha-interferon treatment. J. Hepatol. 1999, 30, 366–375. [Google Scholar] [CrossRef]
- Montano-Loza, A.J.; Vargas-Vorackova, F.; Ma, M.; Bain, V.G.; Burak, K.; Kumar, T.; Mason, A.L. Incidence and risk factors associated with de novo autoimmune hepatitis after liver transplantation. Liver Int. 2012, 32, 1426–1433. [Google Scholar] [CrossRef]
- Kerkar, N.; Vergani, D. De novo autoimmune hepatitis—Is this different in adults compared to children? J. Autoimmun. 2018, 95, 26–33. [Google Scholar] [CrossRef]
- Kerkar, N.; Hadzic, N.; Davies, E.T.; Portmann, B.; Donaldson, P.T.; Rela, M.; Heaton, N.D.; Vergani, D.; Mieli-Vergani, G. De-novo autoimmune hepatitis after liver transplantation. Lancet 1998, 351, 409–413. [Google Scholar] [CrossRef]
- Jones, D.E.; James, O.F.; Portmann, B.; Burt, A.D.; Williams, R.; Hudson, M. Development of autoimmune hepatitis following liver transplantation for primary biliary cirrhosis. Hepatology 1999, 30, 53–57. [Google Scholar] [CrossRef]
- Aguilera, I.; Wichmann, I.; Sousa, J.M.; Bernardos, A.; Franco, E.; Garcia-Lozano, J.R.; Nunez-Roldan, A. Antibodies against glutathione S-transferase T1 (GSTT1) in patients with de novo immune hepatitis following liver transplantation. Clin. Exp. Immunol. 2001, 126, 535–539. [Google Scholar] [CrossRef]
- Stravitz, R.T.; Lefkowitch, J.H.; Fontana, R.J.; Gershwin, M.E.; Leung, P.S.; Sterling, R.K.; Manns, M.P.; Norman, G.L.; Lee, W.M.; Acute Liver Failure Study, G. Autoimmune acute liver failure: Proposed clinical and histological criteria. Hepatology 2011, 53, 517–526. [Google Scholar] [CrossRef]
- Aljumah, A.A.; Al-Ashgar, H.; Fallatah, H.; Albenmousa, A. Acute onset autoimmune hepatitis: Clinical presentation and treatment outcomes. Ann. Hepatol. 2019, 18, 439–444. [Google Scholar] [CrossRef]
- Fujiwara, K.; Fukuda, Y.; Yokosuka, O. Precise histological evaluation of liver biopsy specimen is indispensable for diagnosis and treatment of acute-onset autoimmune hepatitis. J. Gastroenterol. 2008, 43, 951–958. [Google Scholar] [CrossRef]
- Muratori, P.; Granito, A.; Lenzi, M.; Muratori, L. Limitation of the simplified scoring system for the diagnosis of autoimmune Hepatitis with acute onset. Liver Int. 2021, 41, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Yasui, S.; Fujiwara, K.; Okitsu, K.; Yonemitsu, Y.; Ito, H.; Yokosuka, O. Importance of computed tomography imaging features for the diagnosis of autoimmune acute liver failure. Hepatol. Res. 2012, 42, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Teufel, A.; Weinmann, A.; Centner, C.; Piendl, A.; Lohse, A.W.; Galle, P.R.; Kanzler, S. Hepatocellular carcinoma in patients with autoimmune hepatitis. World J. Gastroenterol. 2009, 15, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Ngu, J.H.; Gearry, R.B.; Frampton, C.M.; Stedman, C.A. Mortality and the risk of malignancy in autoimmune liver diseases: A population-based study in Canterbury, New Zealand. Hepatology 2012, 55, 522–529. [Google Scholar] [CrossRef]
- Czaja, A.J. Hepatocellular carcinoma and other malignancies in autoimmune hepatitis. Dig. Dis. Sci. 2013, 58, 1459–1476. [Google Scholar] [CrossRef]
- Zachou, K.; Muratori, P.; Koukoulis, G.K.; Granito, A.; Gatselis, N.; Fabbri, A.; Dalekos, G.N.; Muratori, L. Review article: Autoimmune hepatitis–current management and challenges. Aliment. Pharmacol. Ther. 2013, 38, 887–913. [Google Scholar] [CrossRef]
- Alvarez, F.; Berg, P.A.; Bianchi, F.B.; Bianchi, L.; Burroughs, A.K.; Cancado, E.L.; Chapman, R.W.; Cooksley, W.G.; Czaja, A.J.; Desmet, V.J.; et al. International Autoimmune Hepatitis Group Report: Review of criteria for diagnosis of autoimmune hepatitis. J. Hepatol. 1999, 31, 929–938. [Google Scholar] [CrossRef]
- Muratori, P.; Granito, A.; Quarneti, C.; Ferri, S.; Menichella, R.; Cassani, F.; Pappas, G.; Bianchi, F.B.; Lenzi, M.; Muratori, L. Autoimmune hepatitis in Italy: The Bologna experience. J. Hepatol. 2009, 50, 1210–1218. [Google Scholar] [CrossRef] [PubMed]
- Zachou, K.; Gatselis, N.; Papadamou, G.; Rigopoulou, E.I.; Dalekos, G.N. Mycophenolate for the treatment of autoimmune hepatitis: Prospective assessment of its efficacy and safety for induction and maintenance of remission in a large cohort of treatment-naive patients. J. Hepatol. 2011, 55, 636–646. [Google Scholar] [CrossRef]
- Hennes, E.M.; Zeniya, M.; Czaja, A.J.; Pares, A.; Dalekos, G.N.; Krawitt, E.L.; Bittencourt, P.L.; Porta, G.; Boberg, K.M.; Hofer, H.; et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology 2008, 48, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Manns, M.P.; Czaja, A.J.; Gorham, J.D.; Krawitt, E.L.; Mieli-Vergani, G.; Vergani, D.; Vierling, J.M.; American Association for the Study of Liver, D. Diagnosis and management of autoimmune hepatitis. Hepatology 2010, 51, 2193–2213. [Google Scholar] [CrossRef]
- Czaja, A.J. Performance parameters of the conventional serological markers for autoimmune hepatitis. Dig. Dis. Sci. 2011, 56, 545–554. [Google Scholar] [CrossRef]
- Czaja, A.J.; Carpenter, H.A.; Manns, M.P. Antibodies to soluble liver antigen, P450IID6, and mitochondrial complexes in chronic hepatitis. Gastroenterology 1993, 105, 1522–1528. [Google Scholar] [CrossRef]
- Baeres, M.; Herkel, J.; Czaja, A.J.; Wies, I.; Kanzler, S.; Cancado, E.L.; Porta, G.; Nishioka, M.; Simon, T.; Daehnrich, C.; et al. Establishment of standardised SLA/LP immunoassays: Specificity for autoimmune hepatitis, worldwide occurrence, and clinical characteristics. Gut 2002, 51, 259–264. [Google Scholar] [CrossRef]
- Efe, C.; Ozaslan, E.; Wahlin, S.; Purnak, T.; Muratori, L.; Quarneti, C.; Yuksel, O.; Muratori, P. Antibodies to soluble liver antigen in patients with various liver diseases: A multicentre study. Liver Int. 2013, 33, 190–196. [Google Scholar] [CrossRef]
- Targan, S.R.; Landers, C.; Vidrich, A.; Czaja, A.J. High-titer antineutrophil cytoplasmic antibodies in type-1 autoimmune hepatitis. Gastroenterology 1995, 108, 1159–1166. [Google Scholar] [CrossRef] [PubMed]
- Terjung, B.; Sohne, J.; Lechtenberg, B.; Gottwein, J.; Muennich, M.; Herzog, V.; Mahler, M.; Sauerbruch, T.; Spengler, U. p-ANCAs in autoimmune liver disorders recognise human beta-tubulin isotype 5 and cross-react with microbial protein FtsZ. Gut 2010, 59, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J.; Cassani, F.; Cataleta, M.; Valentini, P.; Bianchi, F.B. Frequency and significance of antibodies to actin in type 1 autoimmune hepatitis. Hepatology 1996, 24, 1068–1073. [Google Scholar] [CrossRef] [PubMed]
- Frenzel, C.; Herkel, J.; Luth, S.; Galle, P.R.; Schramm, C.; Lohse, A.W. Evaluation of F-actin ELISA for the diagnosis of autoimmune hepatitis. Am. J. Gastroenterol. 2006, 101, 2731–2736. [Google Scholar] [CrossRef] [PubMed]
- Granito, A.; Muratori, L.; Muratori, P.; Pappas, G.; Guidi, M.; Cassani, F.; Volta, U.; Ferri, A.; Lenzi, M.; Bianchi, F.B. Antibodies to filamentous actin (F-actin) in type 1 autoimmune hepatitis. J. Clin. Pathol. 2006, 59, 280–284. [Google Scholar] [CrossRef]
- Gueguen, P.; Dalekos, G.; Nousbaum, J.B.; Zachou, K.; Putterman, C.; Youinou, P.; Renaudineau, Y. Double reactivity against actin and alpha-actinin defines a severe form of autoimmune hepatitis type 1. J. Clin. Immunol. 2006, 26, 495–505. [Google Scholar] [CrossRef]
- Bachrich, T.; Thalhammer, T.; Jager, W.; Haslmayer, P.; Alihodzic, B.; Bakos, S.; Hitchman, E.; Senderowicz, A.M.; Penner, E. Characterization of autoantibodies against uridine-diphosphate glucuronosyltransferase in patients with inflammatory liver diseases. Hepatology 2001, 33, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Martini, E.; Abuaf, N.; Cavalli, F.; Durand, V.; Johanet, C.; Homberg, J.C. Antibody to liver cytosol (anti-LC1) in patients with autoimmune chronic active hepatitis type 2. Hepatology 1988, 8, 1662–1666. [Google Scholar] [CrossRef] [PubMed]
- Vergani, D.; Alvarez, F.; Bianchi, F.B.; Cancado, E.L.; Mackay, I.R.; Manns, M.P.; Nishioka, M.; Penner, E.; International Autoimmune Hepatitis, G. Liver autoimmune serology: A consensus statement from the committee for autoimmune serology of the International Autoimmune Hepatitis Group. J. Hepatol. 2004, 41, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Bogdanos, D.P.; Invernizzi, P.; Mackay, I.R.; Vergani, D. Autoimmune liver serology: Current diagnostic and clinical challenges. World J. Gastroenterol. 2008, 14, 3374–3387. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J.; Carpenter, H.A. Sensitivity, specificity, and predictability of biopsy interpretations in chronic hepatitis. Gastroenterology 1993, 105, 1824–1832. [Google Scholar] [CrossRef] [PubMed]
- Misdraji, J.; Thiim, M.; Graeme-Cook, F.M. Autoimmune hepatitis with centrilobular necrosis. Am. J. Surg. Pathol. 2004, 28, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Miyake, Y.; Iwasaki, Y.; Terada, R.; Onishi, T.; Okamoto, R.; Takaguchi, K.; Ikeda, H.; Makino, Y.; Kobashi, H.; Sakaguchi, K.; et al. Clinical features of Japanese type 1 autoimmune hepatitis patients with zone III necrosis. Hepatol. Res. 2007, 37, 801–805. [Google Scholar] [CrossRef]
- Balitzer, D.; Shafizadeh, N.; Peters, M.G.; Ferrell, L.D.; Alshak, N.; Kakar, S. Autoimmune hepatitis: Review of histologic features included in the simplified criteria proposed by the international autoimmune hepatitis group and proposal for new histologic criteria. Mod. Pathol. 2017, 30, 773–783. [Google Scholar] [CrossRef]
- Feld, J.J.; Dinh, H.; Arenovich, T.; Marcus, V.A.; Wanless, I.R.; Heathcote, E.J. Autoimmune hepatitis: Effect of symptoms and cirrhosis on natural history and outcome. Hepatology 2005, 42, 53–62. [Google Scholar] [CrossRef]
- Yada, N.; Kudo, M.; Chung, H.; Watanabe, T. Autoimmune hepatitis and immunoglobulin G4-associated autoimmune hepatitis. Dig. Dis. 2013, 31, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A.; Arinaga-Hino, T.; Ohira, H.; Abe, K.; Torimura, T.; Zeniya, M.; Abe, M.; Yoshizawa, K.; Takaki, A.; Suzuki, Y.; et al. Non-alcoholic fatty liver disease in patients with autoimmune hepatitis. JGH Open 2018, 2, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Lohse, A.W.; Sebode, M.; Bhathal, P.S.; Clouston, A.D.; Dienes, H.P.; Jain, D.; Gouw, A.S.H.; Guindi, M.; Kakar, S.; Kleiner, D.E.; et al. Consensus recommendations for histological criteria of autoimmune hepatitis from the International AIH Pathology Group: Results of a workshop on AIH histology hosted by the European Reference Network on Hepatological Diseases and the European Society of Pathology: Results of a workshop on AIH histology hosted by the European Reference Network on Hepatological Diseases and the European Society of Pathology. Liver Int. 2022, 42, 1058–1069. [Google Scholar] [CrossRef]
- Johnson, P.J.; McFarlane, I.G. Meeting report: International Autoimmune Hepatitis Group. Hepatology 1993, 18, 998–1005. [Google Scholar] [CrossRef]
- Czaja, A.J. Performance parameters of the diagnostic scoring systems for autoimmune hepatitis. Hepatology 2008, 48, 1540–1548. [Google Scholar] [CrossRef]
- Gatselis, N.K.; Zachou, K.; Papamichalis, P.; Koukoulis, G.K.; Gabeta, S.; Dalekos, G.N.; Rigopoulou, E.I. Comparison of simplified score with the revised original score for the diagnosis of autoimmune hepatitis: A new or a complementary diagnostic score? Dig. Liver Dis. 2010, 42, 807–812. [Google Scholar] [CrossRef]
- Qiu, D.; Wang, Q.; Wang, H.; Xie, Q.; Zang, G.; Jiang, H.; Tu, C.; Guo, J.; Zhang, S.; Wang, J.; et al. Validation of the simplified criteria for diagnosis of autoimmune hepatitis in Chinese patients. J. Hepatol. 2011, 54, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Muratori, P.; Granito, A.; Pappas, G.; Muratori, L. Validation of simplified diagnostic criteria for autoimmune hepatitis in Italian patients. Hepatology 2009, 49, 1782–1783; author reply 1783. [Google Scholar] [CrossRef]
- Czaja, A.; Carpenter, H.A. Validation of scoring system for diagnosis of autoimmune hepatitis. Dig. Dis. Sci. 1996, 41, 305–314. [Google Scholar] [CrossRef]
- Yeoman, A.D.; Westbrook, R.H.; Al-Chalabi, T.; Carey, I.; Heaton, N.D.; Portmann, B.C.; Heneghan, M.A. Diagnostic value and utility of the simplified International Autoimmune Hepatitis Group (IAIHG) criteria in acute and chronic liver disease. Hepatology 2009, 50, 538–545. [Google Scholar] [CrossRef]
- Galaski, J.; Weiler-Normann, C.; Schakat, M.; Zachou, K.; Muratori, P.; Lampalzer, S.; Haag, F.; Schramm, C.; Lenzi, M.; Dalekos, G.N.; et al. Update of the simplified criteria for autoimmune hepatitis: Evaluation of the methodology for immunoserological testing. J. Hepatol. 2021, 74, 312–320. [Google Scholar] [CrossRef]
- Flikshteyn, B.; Amer, K.; Tafesh, Z.; Pyrsopoulos, N.T. Diagnosis of Autoimmune Hepatitis. Clin. Liver Dis. 2024, 28, 37–50. [Google Scholar] [CrossRef]
- Shah, A.G.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J.; Nash Clinical Research, N. Comparison of noninvasive markers of fibrosis in patients with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef]
- Poynard, T.; Ngo, Y.; Perazzo, H.; Munteanu, M.; Lebray, P.; Moussalli, J.; Thabut, D.; Benhamou, Y.; Ratziu, V. Prognostic value of liver fibrosis biomarkers: A meta-analysis. Gastroenterol. Hepatol. 2011, 7, 445–454. [Google Scholar]
- Poynard, T.; de Ledinghen, V.; Zarski, J.P.; Stanciu, C.; Munteanu, M.; Vergniol, J.; France, J.; Trifan, A.; Le Naour, G.; Vaillant, J.C.; et al. Relative performances of FibroTest, Fibroscan, and biopsy for the assessment of the stage of liver fibrosis in patients with chronic hepatitis C: A step toward the truth in the absence of a gold standard. J. Hepatol. 2012, 56, 541–548. [Google Scholar] [CrossRef]
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Hartl, J.; Denzer, U.; Ehlken, H.; Zenouzi, R.; Peiseler, M.; Sebode, M.; Hubener, S.; Pannicke, N.; Weiler-Normann, C.; Quaas, A.; et al. Transient elastography in autoimmune hepatitis: Timing determines the impact of inflammation and fibrosis. J. Hepatol. 2016, 65, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Talwalkar, J.A.; Yin, M.; Venkatesh, S.; Rossman, P.J.; Grimm, R.C.; Manduca, A.; Romano, A.; Kamath, P.S.; Ehman, R.L. Feasibility of in vivo MR elastographic splenic stiffness measurements in the assessment of portal hypertension. AJR Am. J. Roentgenol. 2009, 193, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Malik, N.; Yin, M.; Smyrk, T.C.; Czaja, A.J.; Ehman, R.L.; Venkatesh, S.K. Magnetic resonance elastography is accurate in detecting advanced fibrosis in autoimmune hepatitis. World J. Gastroenterol. 2017, 23, 859–868. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J. Review article: The prevention and reversal of hepatic fibrosis in autoimmune hepatitis. Aliment. Pharmacol. Ther. 2014, 39, 385–406. [Google Scholar] [CrossRef] [PubMed]
- Piscaglia, F.; Salvatore, V.; Di Donato, R.; D’Onofrio, M.; Gualandi, S.; Gallotti, A.; Peri, E.; Borghi, A.; Conti, F.; Fattovich, G.; et al. Accuracy of VirtualTouch Acoustic Radiation Force Impulse (ARFI) imaging for the diagnosis of cirrhosis during liver ultrasonography. Ultraschall Med. 2011, 32, 167–175. [Google Scholar] [CrossRef]
- Karlas, T.F.; Pfrepper, C.; Rosendahl, J.; Benckert, C.; Wittekind, C.; Jonas, S.; Moessner, J.; Troltzsch, M.; Tillmann, H.L.; Berg, T.; et al. Acoustic radiation force impulse (ARFI) elastography in acute liver failure: Necrosis mimics cirrhosis. Z. Gastroenterol. 2011, 49, 443–448. [Google Scholar] [CrossRef]
- Ben Ari, Z.; Mehta, A.; Lennard, L.; Burroughs, A.K. Azathioprine-induced myelosuppression due to thiopurine methyltransferase deficiency in a patient with autoimmune hepatitis. J. Hepatol. 1995, 23, 351–354. [Google Scholar] [CrossRef]
- Czaja, A.J.; Carpenter, H.A. Thiopurine methyltransferase deficiency and azathioprine intolerance in autoimmune hepatitis. Dig. Dis. Sci. 2006, 51, 968–975. [Google Scholar] [CrossRef] [PubMed]
- Langley, P.G.; Underhill, J.; Tredger, J.M.; Norris, S.; McFarlane, I.G. Thiopurine methyltransferase phenotype and genotype in relation to azathioprine therapy in autoimmune hepatitis. J. Hepatol. 2002, 37, 441–447. [Google Scholar] [CrossRef]
- Loomba, R.; Liang, T.J. Hepatitis B Reactivation Associated with Immune Suppressive and Biological Modifier Therapies: Current Concepts, Management Strategies, and Future Directions. Gastroenterology 2017, 152, 1297–1309. [Google Scholar] [CrossRef] [PubMed]
- Kornbluth, A.; Hayes, M.; Feldman, S.; Hunt, M.; Fried-Boxt, E.; Lichtiger, S.; Legnani, P.; George, J.; Young, J. Do guidelines matter? Implementation of the ACG and AGA osteoporosis screening guidelines in inflammatory bowel disease (IBD) patients who meet the guidelines’ criteria. Am. J. Gastroenterol. 2006, 101, 1546–1550. [Google Scholar] [CrossRef] [PubMed]
- American Gastroenterological, A. American Gastroenterological Association medical position statement: Osteoporosis in hepatic disorders. Gastroenterology 2003, 125, 937–940. [Google Scholar] [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Rochlani, Y.; Pothineni, N.V.; Kovelamudi, S.; Mehta, J.L. Metabolic syndrome: Pathophysiology, management, and modulation by natural compounds. Ther. Adv. Cardiovasc. Dis. 2017, 11, 215–225. [Google Scholar] [CrossRef]
- Montano-Loza, A.J.; Carpenter, H.A.; Czaja, A.J. Improving the end point of corticosteroid therapy in type 1 autoimmune hepatitis to reduce the frequency of relapse. Am. J. Gastroenterol. 2007, 102, 1005–1012. [Google Scholar] [CrossRef]
- Zachou, K.; Gatselis, N.K.; Arvaniti, P.; Gabeta, S.; Rigopoulou, E.I.; Koukoulis, G.K.; Dalekos, G.N. A real-world study focused on the long-term efficacy of mycophenolate mofetil as first-line treatment of autoimmune hepatitis. Aliment. Pharmacol. Ther. 2016, 43, 1035–1047. [Google Scholar] [CrossRef]
- Geier, A.; Gartung, C.; Dietrich, C.G.; Wasmuth, H.E.; Reinartz, P.; Matern, S. Side effects of budesonide in liver cirrhosis due to chronic autoimmune hepatitis: Influence of hepatic metabolism versus portosystemic shunts on a patient complicated with HCC. World J. Gastroenterol. 2003, 9, 2681–2685. [Google Scholar] [CrossRef]
- Hempfling, W.; Grunhage, F.; Dilger, K.; Reichel, C.; Beuers, U.; Sauerbruch, T. Pharmacokinetics and pharmacodynamic action of budesonide in early- and late-stage primary biliary cirrhosis. Hepatology 2003, 38, 196–202. [Google Scholar] [CrossRef]
- Czaja, A.J. Safety issues in the management of autoimmune hepatitis. Expert. Opin. Drug Saf. 2008, 7, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Heneghan, M.A.; Allan, M.L.; Bornstein, J.D.; Muir, A.J.; Tendler, D.A. Utility of thiopurine methyltransferase genotyping and phenotyping, and measurement of azathioprine metabolites in the management of patients with autoimmune hepatitis. J. Hepatol. 2006, 45, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J.; Menon, K.V.; Carpenter, H.A. Sustained remission after corticosteroid therapy for type 1 autoimmune hepatitis: A retrospective analysis. Hepatology 2002, 35, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Selvarajah, V.; Montano-Loza, A.J.; Czaja, A.J. Systematic review: Managing suboptimal treatment responses in autoimmune hepatitis with conventional and nonstandard drugs. Aliment. Pharmacol. Ther. 2012, 36, 691–707. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J. Rapidity of treatment response and outcome in type 1 autoimmune hepatitis. J. Hepatol. 2009, 51, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Santiago, P.; Schwartz, I.; Tamariz, L.; Levy, C. Systematic review with meta-analysis: Mycophenolate mofetil as a second-line therapy for autoimmune hepatitis. Aliment. Pharmacol. Ther. 2019, 49, 830–839. [Google Scholar] [CrossRef] [PubMed]
- De Lemos-Bonotto, M.; Valle-Tovo, C.; Costabeber, A.M.; Mattos, A.A.; Azeredo-da-Silva, A.L.F. A systematic review and meta-analysis of second-line immunosuppressants for autoimmune hepatitis treatment. Eur. J. Gastroenterol. Hepatol. 2018, 30, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, A.J.; Roberts, S.K.; Lim, R.; Mitchell, J.; Weltman, M.; George, J.; Wigg, A.; Stuart, K.; Gow, P.; MacQuillan, G.; et al. Beneficial response to mycophenolate mofetil by patients with autoimmune hepatitis who have failed standard therapy, is predicted by older age and lower immunoglobulin G and INR levels. Aliment. Pharmacol. Ther. 2019, 49, 1314–1322. [Google Scholar] [CrossRef] [PubMed]
- Efe, C.; Hagstrom, H.; Ytting, H.; Bhanji, R.A.; Muller, N.F.; Wang, Q.; Purnak, T.; Muratori, L.; Werner, M.; Marschall, H.U.; et al. Efficacy and Safety of Mycophenolate Mofetil and Tacrolimus as Second-line Therapy for Patients with Autoimmune Hepatitis. Clin. Gastroenterol. Hepatol. 2017, 15, 1950–1956.e1951. [Google Scholar] [CrossRef] [PubMed]
- Carbone, M.; Neuberger, J.M. Autoimmune liver disease, autoimmunity and liver transplantation. J. Hepatol. 2014, 60, 210–223. [Google Scholar] [CrossRef]
- Mendes, F.; Couto, C.A.; Levy, C. Recurrent and de novo autoimmune liver diseases. Clin. Liver Dis. 2011, 15, 859–878. [Google Scholar] [CrossRef]
- Hayashi, M.; Keeffe, E.B.; Krams, S.M.; Martinez, O.M.; Ojogho, O.N.; So, S.K.; Garcia, G.; Imperial, J.C.; Esquivel, C.O. Allograft rejection after liver transplantation for autoimmune liver diseases. Liver Transpl. Surg. 1998, 4, 208–214. [Google Scholar] [CrossRef]
- Milkiewicz, P.; Gunson, B.; Saksena, S.; Hathaway, M.; Hubscher, S.G.; Elias, E. Increased incidence of chronic rejection in adult patients transplanted for autoimmune hepatitis: Assessment of risk factors. Transplantation 2000, 70, 477–480. [Google Scholar] [CrossRef]
- Czaja, A.J. Advancing Biologic Therapy for Refractory Autoimmune Hepatitis. Dig. Dis. Sci. 2022, 67, 4979–5005. [Google Scholar] [CrossRef]
- Than, N.N.; Hodson, J.; Schmidt-Martin, D.; Taubert, R.; Wawman, R.E.; Botter, M.; Gautam, N.; Bock, K.; Jones, R.; Appanna, G.D.; et al. Efficacy of rituximab in difficult-to-manage autoimmune hepatitis: Results from the International Autoimmune Hepatitis Group. JHEP Rep. 2019, 1, 437–445. [Google Scholar] [CrossRef]
- Weiler-Normann, C.; Schramm, C.; Quaas, A.; Wiegard, C.; Glaubke, C.; Pannicke, N.; Moller, S.; Lohse, A.W. Infliximab as a rescue treatment in difficult-to-treat autoimmune hepatitis. J. Hepatol. 2013, 58, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Bjornsson, E.S.; Gunnarsson, B.I.; Grondal, G.; Jonasson, J.G.; Einarsdottir, R.; Ludviksson, B.R.; Gudbjornsson, B.; Olafsson, S. Risk of drug-induced liver injury from tumor necrosis factor antagonists. Clin. Gastroenterol. Hepatol. 2015, 13, 602–608. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Score |
|---|---|
| 1. ANA or SMA/F-actin | |
| ≥1:40 | +1 |
| ≥1:80 or | +2 |
| LKM ≥ 1:40 or | +2 |
| SLA (+) | +2 |
| 2. Serum IgG | |
| > Upper limit of normality | +1 |
| >1.1 × upper limit of normality | +2 |
| 3. Histologic findings | |
| Compatible with AIH | +1 |
| Typical AIH | +2 |
| 4. Negative hepatitis viral markers | +2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mercado, L.A.; Gil-Lopez, F.; Chirila, R.M.; Harnois, D.M. Autoimmune Hepatitis: A Diagnostic and Therapeutic Overview. Diagnostics 2024, 14, 382. https://doi.org/10.3390/diagnostics14040382
Mercado LA, Gil-Lopez F, Chirila RM, Harnois DM. Autoimmune Hepatitis: A Diagnostic and Therapeutic Overview. Diagnostics. 2024; 14(4):382. https://doi.org/10.3390/diagnostics14040382
Chicago/Turabian StyleMercado, Lydia A., Fernando Gil-Lopez, Razvan M. Chirila, and Denise M. Harnois. 2024. "Autoimmune Hepatitis: A Diagnostic and Therapeutic Overview" Diagnostics 14, no. 4: 382. https://doi.org/10.3390/diagnostics14040382